Back to Journals » International Medical Case Reports Journal » Volume 18
Giant Infarcted Lactating Adenoma Mimicking Inflammatory Breast Carcinoma: A First Case Report from Somalia
Authors Abdullahi IM ![]() , Ibrahim IG
, Ibrahim IG ![]()
Received 17 March 2025
Accepted for publication 15 July 2025
Published 26 July 2025 Volume 2025:18 Pages 931—936
DOI https://doi.org/10.2147/IMCRJ.S528825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xudong Zhu
Ismail Mohamud Abdullahi,1 Ismail Gedi Ibrahim2
1Mogadishu Somalia Türkiye Recep Tayyip Erdoğan Research and Training Hospital, Department of Pathology, Mogadishu, Somalia; 2Mogadishu Somalia Türkiye Recep Tayyip Erdoğan Research and Training Hospital, Department of Radiology, Mogadishu, Somalia
Correspondence: Ismail Mohamud Abdullahi, Mogadishu Somalia Türkiye Recep Tayyip Erdogan Research and Training Hospital, Department of Pathology, Mogadishu, Somalia, Email [email protected]
Abstract: A lactating adenoma is a rare and benign breast tumor that usually occurs during pregnancy or lactation period for women. These adenomas are typically small, < 3 centimeters, well circumscribed, mobile, and lobulated masses, and are most commonly witnessed in primiparous women (those having their first child) between the ages of 20 and 40 years during the third trimester of their pregnancies due to hormonal changes. In this case report, we describe an unusual variant of lactating adenoma that is characterized by the ischemic infarction of breast tissue and its giant dimensions, surpassing 16 centimeters. The case in question had poorly defined margins in addition to chronic mastitis, which can make differentiating from standard lactating adenoma presentations quite difficult clinically. Infarction associated with chronic mastitis serves to complicate the distinction, and tends to mimic inflammatory breast carcinoma. This case report emphasizes how these rare and unusual presentations of lactating adenomas can mimic a highly aggressive malignancy, leading to diagnostic confusion and potentially unnecessary interventions. Inflammatory breast carcinoma is a rapidly progressive malignancy requiring aggressive oncological management, unlike infarcted lactating adenomas, which are benign and can be effectively treated with surgical excision alone. This case adds an important dimension to the medical literature, particularly given its context of occurrence in Somalia, where resources and access to advanced diagnostic tools are limited. By detailing this unique instance, the study not only contributes to the understanding of breast pathology but also emphasizes the necessity for keen clinical acumen in achieving appropriate therapeutic interventions in diverse health-care settings.
Keywords: lactation disorders, breast, breast neoplasms
Introduction
A lactating adenoma is a rare benign breast tumor that usually occurs in pregnant or lactating women. It is a hormonally driven neoplasm usually manifesting as a well-circumscribed, mobile, and lobulated mass, with a mean diameter <3 cm.1 These tumors are usually seen in primiparous women at the age of 20–40 years in the third trimester of pregnancy.2 Although lactating adenomas are usually well-circumscribed, self-limited lumps, a few cases may present with atypical features that pose significant diagnostic challenges.3
Rapid hormonal shifts during pregnancy can promote tumor growth, and in rare cases lead to spontaneous infarction due to compromised blood supply. Infarcted adenomas may present with inflammatory signs that clinically and radiologically mimic inflammatory breast cancer (IBC), a rare but aggressive form of breast carcinoma comprising 1%–5% of all cases.2,3 Infarction within a lactating adenoma is unusual and may cause rapidly enlarging, inflamed lesions that resemble aggressive malignancies, accompanied by symptoms such as pain, erythema, and skin thickening.3 In resource-limited settings, access to advanced imaging and histopathological evaluation may be limited, further contributing to diagnostic uncertainty.4
According to a study conducted at Somalia Turkey Recep Tayyip Erdoğan Education and Research Hospital by Tahtabasi et al, breast cancer accounted for 13.1% of cancers among women and was the third–most common malignancy overall in Somalia. Challenges in diagnosis and treatment include late presentation, limited access to screening tools like mammography, and a general lack of awareness, which contribute to delayed diagnoses and poorer outcomes.5
In this report, we document the first reported case in Somalia of a lactating adenoma with spontaneous infarction masquerading as IBC. Remarkably, with regard to the presented case, considering the unusual size of the tumor (>16 cm) and its ischemic infarction, its histopathological diagnosis was uncertain. Through the description of this case, we seek to bring attention to novel presentations of lactating adenomas and emphasize the significance of clinical judgment in differentiating benign from malignant breast disorders, particularly in environments with scarce and limited diagnostic tools. Considering the potential existence of both scenarios, it is essential for their diagnosis to avoid unnecessary interventions and directed towards therapies.
Case Presentation
A 26-year-old Somali woman 2 months postpartum was brought to the clinic complaining of a large, rapidly growing, painful mass in her left breast, which was followed by swelling. She noted that the mass appeared during the first trimester of her pregnancy, and the symptoms become progressively worsened after delivery. The patient denied any history of trauma, fever, or systemic symptoms like weight loss or fatigue.
On physical examination, the left breast was grossly swollen. There was a palpable, large, tender mass occupying the upper quadrant of the left breast. The skin over the mass appeared shiny, resembling the peau d’orange appearance seen in IBC. There was axillary lymphadenopathy detected on both palpation and breast ultrasound.
The clinical presentation was highly suggestive of IBC, leading to concerns regarding a potential malignant process.
The infarcted adenoma presented as a hypoechoic mass, with areas of necrosis and heterogeneous echogenicity with poorly defined edges measuring 20×13×9 cm on breast ultrasound, potentially misinterpreted as inflammatory carcinoma. A prompt ultrasound-guided breast core needle biopsy (CNB) was done to assess for malignancy, especially in light of concerns about IBC, which can present similarly to an infection or benign conditions.
Histopathological Findings
The spontaneous infarct of the lactating adenoma revealed necrotic tissue, hemorrhage, and scarring. In line with that, only a small number of nearby areas displayed benign glandular structures that exhibited lactating characteristics, without any signs of malignancy. The ischemic infarct was probably caused by reduced blood flow within the adenoma, which had grown rapidly after delivery. Despite the explicit histopathological findings, clinicians were still concerned about the possibility of IBC, and thus a surgeon brought the patient to surgery for an excisional biopsy. Nevertheless, the histopathologic results aligned with the initial findings, validating the diagnosis of an infarct within the giant lactating adenoma (Figures 1 and 2).
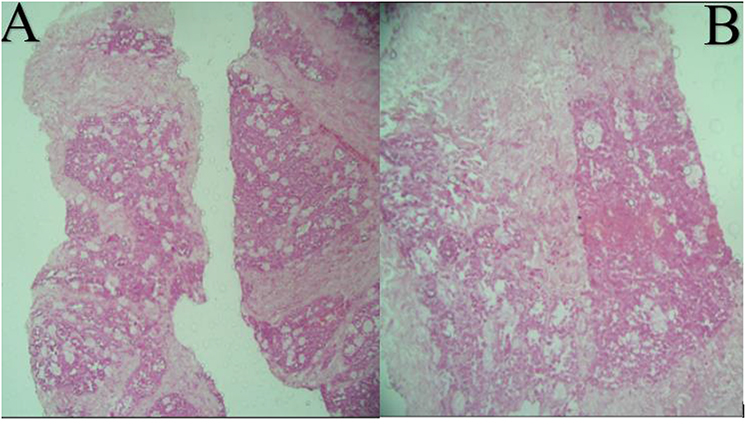 |
Figure 1 Photomicrograph of the core biopsy. (A) Lactating adenoma, closely packed and intermixed with delicate fibrous stroma (H&E, 10×). (B) Microscopic appearance of grossly chalk-like area demonstrating coagulative necrosis. Some viable acini with cytoplasmic vacuolization and lumina containing eosinophilic secretions (H&E, 20×). |
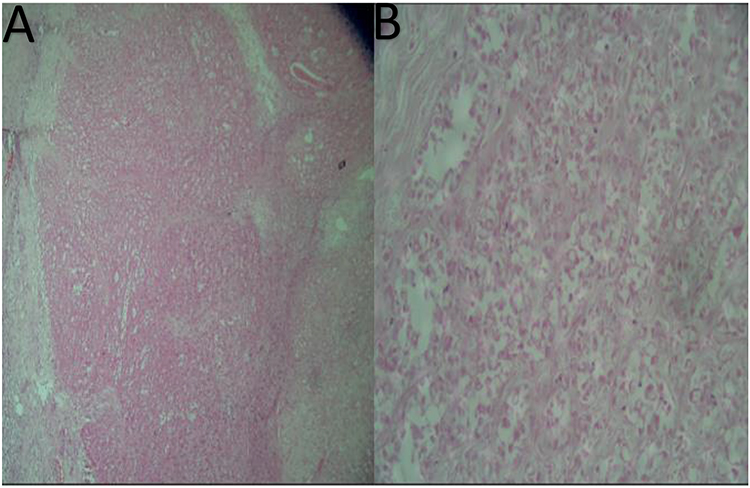 |
Figure 2 Photomicrograph of the surgical excision. (A) Lactating adenoma, closely packed and intermixed with delicate fibrous stroma. (H&E, 10×). (B) Microscopic appearance of viable acini with cytoplasmic vacuolization, prominent nuclear hobnailing with bulbous nuclear projections into the lumina, and eosinophilic secretions in the lumen (H&E, 40×). |
Clinical and radiological correlation is essential in such cases. Clinicians must be aware that lactating adenomas, particularly when undergoing infarction, can present with features that closely mimic malignancy. It is important that the pathology be carefully reviewed, as necrosis and inflammation can overlap with malignancy. However, the presence of benign glandular structures with necrosis and fibrosis can help confirm the diagnosis of a lactating adenoma.
Discussion
Lactating adenoma is a noncancerous breast tumor that is influenced by hormones and commonly develops in women during pregnancy or while breastfeeding. While the majority of lactating adenomas present as small, well-circumscribed, mobile, lobulated masses,1,3 the case presented in this report deviated from the typical clinical and radiological features in several critical aspects, emphasizing the importance of considering rare and atypical presentations in the differential diagnosis of breast masses.
This case report details a giant lactating adenoma (measuring >16 cm) that unexpectedly presented with spontaneous infarction, which is a rare phenomenon in medical literature. The infarction resulted in necrosis and hemorrhage within the adenoma, leading to unclear margins and complex imaging results that resembled IBC. The skin underwent changes, such as the development of a peau d’orange appearance and enlarged axillary lymph nodes, which increased the likelihood of malignancy (Table 1). IBC is a rare and aggressive form of breast cancer that manifests with erythema, edema, and warmth due to extensive dermal lymphatic invasion by malignant cells.6,7 Given the clinical and radiological overlap between lactating adenoma and IBC, it is imperative that clinicians maintain a high degree of clinical suspicion and utilize appropriate diagnostic tools to distinguish between the two entities.
As demonstrated by Kim et al and Han et al, both have documented cases where infarcted lactating adenomas were initially suspected to be malignant due to similar imaging findings, including heterogeneous echogenicity and poorly defined margins, which can lead to misinterpretation as inflammatory or malignant lesions.8,9
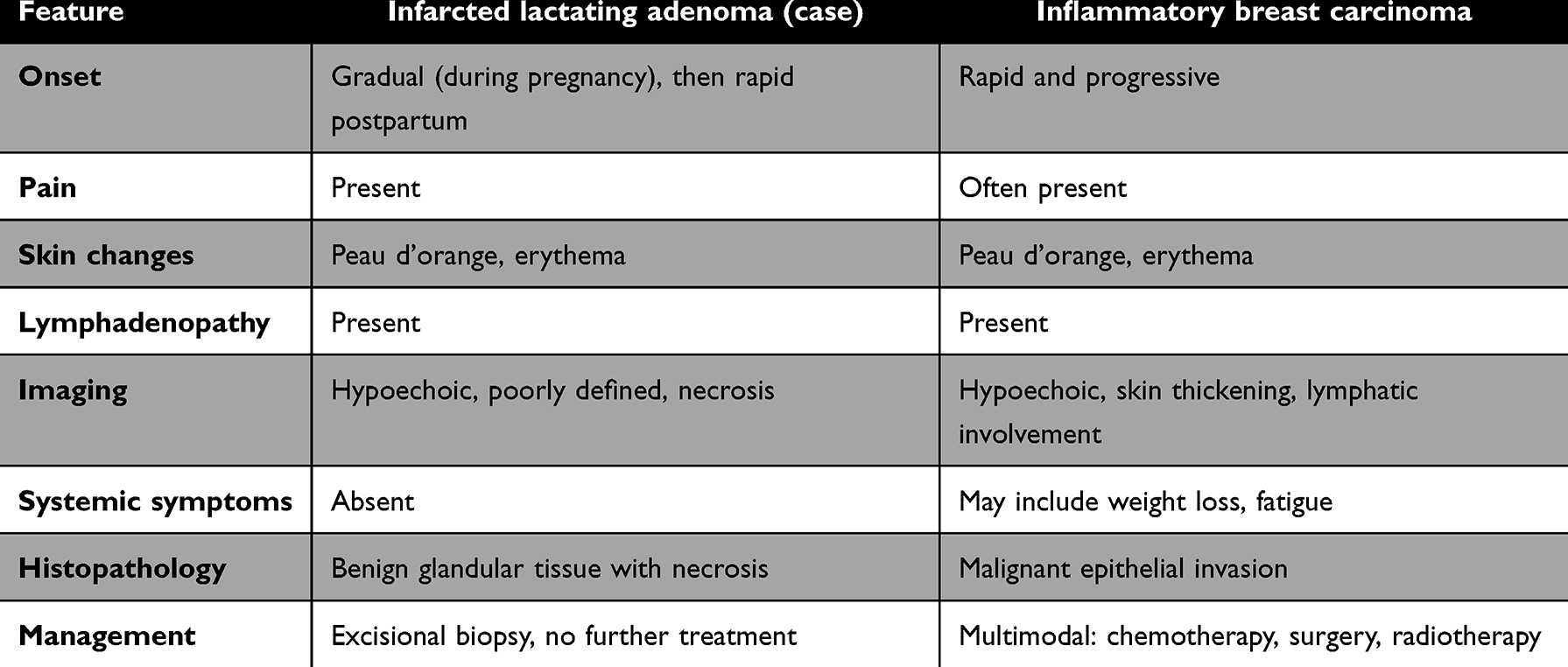 |
Table 1 Comparative features of infarcted lactating adenoma and inflammatory breast carcinoma |
IBC is an aggressive type of breast cancer that develops quickly, and its symptoms, such as breast swelling, redness, and skin changes, can resemble those of inflammatory conditions, emphasizing the importance of early and precise diagnosis. In this particular case, the patient did not experience any systemic symptoms like fever, weight loss, or fatigue, which decreased the probability of a malignancy. However, the mass’s rapid growth and inflammatory features required immediate biopsy to determine if it was cancerous, and a CNB was quickly carried out.10,11
The histopathological examination showed necrosis, hemorrhage, and fibrosis, indicating an infarcted lactating adenoma, with only small areas of viable benign glandular tissue remaining. No cancerous cells were found, providing evidence that the lesion was noncancerous. These findings emphasize the significance of correlating histopathological findings with clinical and radiological information. Since lactating adenomas can experience infarction, leading to necrosis and inflammation, these characteristics may resemble those of malignancy, including IBC.12,13 Given the overlap between benign and aggressive conditions, it is crucial to thoroughly analyze biopsy results and take into account the patient’s complete clinical picture, particularly when benign conditions can exhibit aggressive characteristics that may lead to unnecessary interventions.
One of the major challenges in diagnosing lactating adenomas with infarction is their ability to overlap clinical and radiological features with malignant lesions like IBC. These benign lesions may present with rapid enlargement, skin erythema, pain, and even axillary lymphadenopathy, features classically associated with aggressive breast malignancies. The role of imaging is pivotal in distinguishing benign from malignant lesions, yet even advanced diagnostic techniques, such as ultrasound and mammography, may not always provide definitive differentiation. In this case, ultrasound revealed a hypoechoic mass with heterogeneous echogenicity and poorly defined edges, which contributed to the concern that it might be IBC, as mammography is not available at our hospital. Nevertheless, the absence of malignant characteristics in the histopathological examination provided conclusive evidence of a giant infarcted lactating adenoma. Guirguis et al14 emphasized the need for radiologists and clinicians to remain vigilant and skeptical when evaluating breast masses, especially when the clinical presentation appears to be deceptive or misleading.
This case also highlights the diagnostic challenges faced in resource-limited settings like Somalia, where access to advanced imaging and pathology services may be scarce. Timely and precise diagnosis is of utmost importance in such circumstances to prevent unnecessary treatments and guarantee that patients receive the most suitable care. Additionally, it emphasizes the significance of clinical expertise in recognizing uncommon and unusual manifestations of benign breast conditions, which can resemble more aggressive malignancies.6,14
Delaying tissue diagnosis in the hope that an inflammatory process will resolve may risk missing an underlying malignancy, while acting too aggressively without histological confirmation may result in overtreatment. Therefore, a biopsy should not be deferred or postponed if the clinical or imaging findings raise even moderate suspicion of malignancy. In this case, the decision to perform an early CNB was crucial in avoiding unnecessary radical surgery and guiding conservative management.
Limitations
This case report presents valuable insights into an unusual presentation of a lactating adenoma with spontaneous infarction; however, several limitations should be acknowledged. First, as a single case, its findings cannot be generalized to broader populations. The rarity of such a presentation limits the ability to draw definitive conclusions about incidence, risk factors, or optimal management strategies. Second, diagnostic limitations related to resource constraints in Somalia may have influenced the diagnostic process. Advanced imaging modalities (eg, contrast-enhanced mammography) and immunohistochemical studies, which could have further characterized the lesion, were not available. These limitations may affect the diagnostic certainty and delay establishing a definitive diagnosis. Nonetheless, the patient underwent a 9-month clinical follow-up after surgical excision, during which no complications or recurrence were noted. Despite these limitations, this report contributes valuable insight as the first documented case from Somalia, highlighting an unusual presentation of a benign lesion mimicking IBC.
Conclusion
This case report brings to light a rare occurrence of spontaneous infarct of a giant lactating adenoma,that resembledIBC based on clinical and radiological features. Timely and accurate diagnosis through imaging findings and careful pathology review is crucial in the differential diagnosis of benign conditions from malignancies. We recommend an approach that prioritizes early imaging and biopsy, particularly when features mimic malignancy. Educating clinicians on the spectrum of lactating adenoma presentations; including infarcted variants, can reduce diagnostic delays, prevent unnecessary aggressive treatment, and improve patient outcomes in resource-limited environments. Despite the fact that the clinical presentation and imaging findings of this patient showed a lot of contradictions for malignancies, she was finally diagnosed with the infarction of a giant lactating adenoma through histopathological confirmation. Awareness of such rare presentations is very crucial to achieve inappropriate treatment and also to avoid overaggressive interventions. This report contributes valuable insights into the management of breast disorders in resource-constrained environments and enhances our understanding of the diverse presentations of lactating adenomas.
Data Sharing Statement
The data that support the findings of this study are available from the Mogadishu Somali Turkey Recep Tayyip Erdogan Training and Research Hospital information system. Data are, however, can be shared upon reasonable request and with permission of the education and research committee.
Ethics Approval
Mogadishu Somali Türkiye Training and Research Hospital (MSTH) does not require institutional review board (IRB) approval for case reports.
Informed Consent for Publication
Written and signed informed consent for publication from the patient is available.
Author Contributions
All authors made substantial contributions to the reported work, including conception, study design, execution, data collection, analysis, and interpretation. They participated in drafting, revising, or critically reviewing the article. Each author gave final approval to the version to be published and agreed on the journal to which the article was submitted. Furthermore, all authors take full responsibility for every aspect of the work.
Funding
The authors declare that they have not received any financial support for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Teberian I, Bhimani C, Sciotto M, Wilkes A, Germaine P. Breast masses in pregnancy and lactation. J Am Osteopath Coll Radiol. 2019;8(8):5–16.
2. Hara Y, Yano H, Yamaguchi R, Iwasaki K. Surgical excision of a lactating adenoma with rapid enlargement: a case report. Int J Surg Case Rep. 2021;89:106544. doi:10.1016/j.ijscr.2021.106544
3. Teng CY, Diego EJ. Case report of a large lactating adenoma with rapid antepartum enlargement. Int J Surg Case Rep. 2016;20:127–129. doi:10.1016/j.ijscr.2016.01.027
4. Bell H, Peters G, Lynch A, Harle R. Breast disorders during pregnancy and lactation: the differential diagnoses. J Clin Gynecol Obstet. 2013;2(2):47–50.
5. Tahtabasi M, Mohamud Abdullahi I, Kalayci M, Gedi Ibrahim I, Er S. Cancer incidence and distribution at a Tertiary Care Hospital in Somalia from 2017 to 2020: an initial report of 1306 cases. Cancer Manage Res. 2020;28:8599–8611. doi:10.2147/CMAR.S277202
6. Moulaz IR, de Oliveira FSS, da Silva EC, Machado JM, Santos MCLFS. Giant lactating adenoma. Autops Case Rep. 2021;11:e2021252. PMID: 33968827; PMCID: PMC8087397. doi:10.4322/acr.2021.252
7. O’Hara MF, Page DL. Adenomas of the breast and ectopic breast under lactational influences. Human Pathol. 1985;16(7):707–712. doi:10.1016/S0046-8177(85)80156-8
8. Kim JY, Kim KS, Lee Y, Kim JH. Spontaneous Infarction of benign breast lesion during pregnancy: ultrasonographic and pathologic findings. J Korean Soc Radiol. 2015;73(4):259–263. doi:10.3348/jksr.2015.73.4.259
9. Han B, Zhang H, Jiang P, et al. Breast infarction during pregnancy and lactation: a case report. Exp Ther Med. 2015;10(5):1888–1892. doi:10.3892/etm.2015.2756
10. Szabo J, Garcia D, Ciomek N, Margolies L. Spuriously aggressive features of a lactating adenoma prompting repeated biopsies. Radiol Case Rep. 2017;12(2):215–218. doi:10.1016/j.radcr.2017.01.019
11. Phung HT, Nguyen LT, Van Nguyen H, Van Nguyen C, Nguyen HT. Aggressive lactating adenoma mimicking breast carcinoma: a case report. Int J Surg Case Rep. 2020;70:17–19. doi:10.1016/j.ijscr.2020.03.047
12. Mlees MA, Elsaka AM. Giant lactating adenoma of the breast: safety and benefits of surgical removal. J Surg. 2017;5(3–1):56–60.
13. Elzahaby IA, Saleh S, Metwally IH, Fathi A, Atallah K. Huge lactating adenoma of the breast: case report. Breast Dis. 2017;37(1):37–42. doi:10.3233/BD-160263
14. Guirguis MS, Adrada B, Santiago L, Candelaria R, Arribas E. Mimickers of breast malignancy: imaging findings, pathologic concordance and clinical management. Insights Into Imaging. 2021;12:1–8. doi:10.1186/s13244-021-00991-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.