Back to Journals » International Journal of Women's Health » Volume 18
Giant Cesarean Section Scar Endometriosis Presenting with Cyclic Pain: A Neglected Clinical Manifestation—A Case Report
Authors Tjahyadi D, Nisa AS ![]() , Bayuaji H
, Bayuaji H ![]() , Winarno GNA
, Winarno GNA ![]() , Anwar R
, Anwar R ![]()
Received 30 March 2026
Accepted for publication 28 May 2026
Published 10 June 2026 Volume 2026:18 613081
DOI https://doi.org/10.2147/IJWH.S613081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Dian Tjahyadi, Aisyah Shofiatun Nisa, Hartanto Bayuaji, Gatot Nyarumenteng Adhipurnawan Winarno, Ruswana Anwar
Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Dian Tjahyadi, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran –Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Email [email protected]
Background: Endometriosis is a chronic gynecological disorder characterized by the presence of endometrium-like tissue outside the uterine cavity. It is most commonly found in the pelvic organs but may also occur in extrapelvic sites, including the intestines, urinary bladder, abdominal wall, thoracic cavity, and other organs. Scar endometriosis is a rare subtype of abdominal wall endometriosis that develops within surgical scar tissue. Giant scar endometriosis is exceptionally uncommon, with lesions rarely exceeding 8 cm in previously reported cases.
Case Illustration: A 35-year-old woman, gravida 2 para 2 abortus 0 (P2A0), presented with cyclic pain and bleeding from a previous cesarean section scar during menstruation for the past three years. The pain was described as severe, with an intensity of 7– 8 on the pain scale, significantly interfering with daily activities. The patient also reported a progressively enlarging mass at the surgical scar site. She had a history of cesarean section with sterilization in 2020, and symptoms began two years after the procedure. Physical examination revealed a firm mass that was non-tender, non-erythematous, and showed no signs of inflammation. Ultrasonography demonstrated a hypoechoic lesion in the suprasymphyseal subcutaneous region. Total surgical excision was performed, yielding a large mass measuring approximately 8 × 8× 8 cm adherent to the fascia. Histopathological examination confirmed the diagnosis of scar endometriosis.
Conclusion: Giant scar endometriosis is a rare but clinically important condition that should be considered in women presenting with cyclic pain or bleeding at a surgical scar site. Early diagnosis and complete surgical excision are essential to prevent recurrence and improve patients’ quality of life.
Keywords: scar endometriosis, cyclic pain, endometriosis, case report
Introduction
Endometriosis is a chronic gynecological disorder characterized by the presence of endometrium-like tissue outside the uterine cavity and is associated with a high recurrence rate.1 Endometriosis most commonly affects pelvic organs; however, extrapelvic involvement may occur, including the intestines, urinary bladder, abdominal wall, and thoracic cavity.2
Scar endometriosis, also referred as iatrogenic endometriosis, is a rare subtype of abdominal wall endometriosis that develops within surgical scar tissue.2 Although its exact pathophysiology remains incompletely understood, the most widely accepted mechanism involves direct implantation of endometrial tissue during surgical procedures, particularly cesarean section. These displaced cells may subsequently survive within the wound environment and develop into hormonally responsive ectopic endometrial tissue.3
The reported incidence of scar endometriosis ranges from 0.03% to 0.45%.4 A review involving 445 cases of abdominal wall endometriosis found that 57% were associated with cesarean section, 11% with hysterectomy, 13% with other surgical procedures, and the remaining 20% occurred spontaneously without a history of surgery.2 In this case, the patient had a history of cesarean section performed two years prior to the onset of symptoms.
Scar endometriosis remains a diagnostic challenge because the lesion is located outside the pelvic organs, where endometriosis is typically expected.2 As a result, diagnosis is often delayed, which may worsen symptoms and negatively affect the patient’s quality of life. Furthermore, abdominal wall masses following cesarean section may mimic other conditions such as abscess, incisional hernia, suture granuloma, or soft tissue tumors, which can lead to misdiagnosis and inappropriate management if not carefully evaluated.5
Large scar endometriosis lesions are particularly uncommon and may further complicate clinical evaluation and surgical planning. Their atypical presentation can resemble other surgical conditions, increasing the risk of delayed diagnosis and inappropriate treatment. Therefore, this case highlights the clinical importance of recognizing atypical presentations, including large scar endometriosis, to avoid misdiagnosis and ensure appropriate management.
Case Illustration
A 35-year-old woman, gravida 2 para 2 abortus 0 (P2A0), was referred with complaints of cyclic pain and bleeding from a previous cesarean section scar for approximately three years prior to hospital admission. The pain was severe and significantly interfered with daily activities, with a visual analog scale (VAS) score of 7–8. The patient reported being unable to perform routine activities on the first and second days of menstruation and routinely used analgesics for pain relief. In addition, she noted a mass at the surgical scar site that was initially small and progressively enlarged over time. On physical examination, the mass was non-tender, non-erythematous, and not warm to palpation, with no signs of inflammation.
The patient reported regular menstrual cycles every 28–30 days, with a menstrual duration of seven days and moderate bleeding (approximately 3–4 sanitary pads per day). She denied dysmenorrhea. She denied dysmenorrhea, intermenstrual bleeding, postcoital bleeding, foul-smelling vaginal discharge, or bowel and urinary symptoms.
The patient had undergone a cesarean section with concomitant sterilization in 2020 and denied any prior history of endometriosis. Approximately two years after surgery, she began experiencing cyclic pain localized to the surgical scar during menstruation. The pain progressively worsened and increasingly interfered with daily activities. She initially sought treatment at a regional hospital, where ultrasonography demonstrated a subcutaneous suprapubic mass that was initially suspected to represent a chronic abscess. The patient subsequently underwent an incisional biopsy of the abdominal wall mass on July 1, 2025, without entry into the peritoneal cavity, and histopathological examination revealed abdominal wall endometriosis.
Following the biopsy procedure, the surgical wound remained moist, and the patient continued to experience cyclic pain and bleeding from the scar during each menstrual cycle. She denied a history of chronic illnesses such as diabetes mellitus, asthma, or heart disease, and reported no family history of malignancy. Due to persistent symptoms, she was referred to a tertiary referral hospital for further management.
Vital signs on admission were within normal limits. The patient was overweight, with a body mass index (BMI) of 29.5 kg/m2. Abdominal examination revealed an open cesarean section scar measuring approximately 3×2 × 1 cm, with the wound base exposing subcutaneous tissue and serous discharge without purulence (Figure 1A). Speculum and bimanual examinations were unremarkable. The patient underwent conservative wound care by a specialized wound care team for several weeks, resulting in gradual wound improvement (Figure 1B). Gynecologic ultrasonography demonstrated an anteflexed uterus measuring 7.62×4.84 cm with a clearly defined endometrial line, without adnexal masses or free fluid in the pouch of Douglas. Ultrasonographic examination of the abdominal wall demonstrated a hypoechoic lesion within the suprapubic subcutaneous tissue corresponding to the palpable mass (Figure 2).
 |
Figure 1 (A) Open surgical wound at the cesarean section scar site following incisional biopsy, showing exposed subcutaneous tissue and serous discharge without purulence. (B) Gradual improvement of the surgical wound after several weeks of conservative wound care. |
 |
Figure 2 Ultrasonographic examination demonstrating a hypoechoic lesion within the suprapubic subcutaneous tissue measuring 4.53×5.04 × 3.72 cm, consistent with abdominal wall endometriosis. |
The patient subsequently underwent surgical excision of the abdominal wall endometriosis mass. Intraoperatively, a well-circumscribed, mobile mass measuring approximately 8 × 8×8 cm was identified on the right side of the cesarean section scar, with the lesion adherent to the fascia (Figure 3A). Approximately 3 cc of dark brown fluid was aspirated from within the mass upon exploration. The mass was completely excised with a a 1-cm safety margin from the lesion edges. Prior to layered closure of the fascia, subcutaneous tissue, and skin, the operative field was irrigated with 0.9% sodium chloride solution. The excised specimen was sent for histopathological examination (Figure 3B).
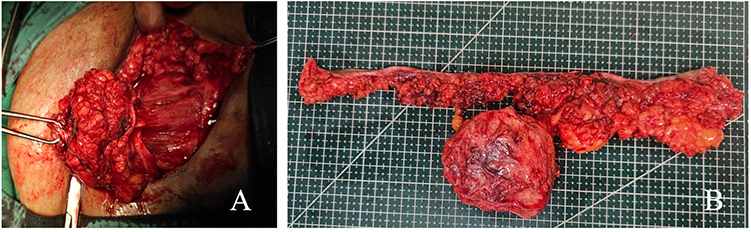 |
Figure 3 (A) Intraoperative appearance of a well-circumscribed abdominal wall endometriotic mass adherent to the fascia. (B) Gross specimen following complete surgical excision of the lesion. |
Postoperative histopathological examination confirmed the diagnosis of cesarean section scar endometriosis of the abdominal wall. As shown in Figure 4, the lesion consisted of endometrial-type glands surrounded by dense fibrocollagenous stroma. Several glands showed irregular shapes with cystic dilatation and were lined by columnar epithelium without cytological atypia. The surrounding stroma resembled endometrial stroma accompanied by lymphocytic inflammatory infiltration and vascular congestion. Hemosiderin-laden macrophages were also observed, further supporting the diagnosis of endometriosis. The patient’s postoperative course was uneventful. At follow-up, she reported complete resolution of pain and bleeding from the surgical scar, and the surgical wound had healed well.
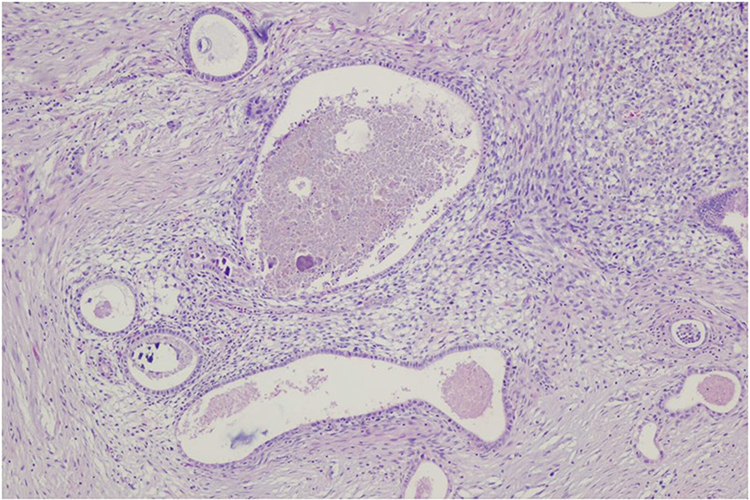 |
Figure 4 Histopathological examination of the abdominal wall lesion demonstrating endometrial-type glands surrounded by fibrocollagenous stroma, consistent with scar endometriosis. |
Discussion
Scar endometriosis is a subtype of abdominal wall endometriosis. The pathogenesis of scar endometriosis remains incompletely understood.3 Several pathogenic mechanisms have been proposed, including the theory of iatrogenic implantation, coelomic cell metaplasia, and lymphovascular dissemination. The most widely accepted mechanism is iatrogenic implantation of endometrial cells into the surgical wound during procedures such as cesarean section.3 These displaced cells may subsequently survive within the wound environment and develop into hormonally responsive ectopic endometrial tissue, leading to recurrent cyclic bleeding and pain at the scar site.6
This mechanism is consistent with the seed and soil theory, which proposes that displaced endometrial cells (seeds) can survive and proliferate within a permissive tissue environment (soil).7 Several studies suggest that inflammatory and angiogenic mechanisms contribute to the survival and proliferation of ectopic endometrial cells within postoperative scar tissue, supporting the development of scar endometriosis. Studies have demonstrated that endometrial cells in women with endometriosis exhibit higher cyclooxygenase-2 (COX-2) enzymatic activity compared to those in women without endometriosis, leading to increased production of prostaglandin E2 (PGE2). Elevated PGE2 levels promote angiogenesis through stimulation of vascular endothelial growth factor (VEGF), inhibit apoptosis, and modulate the local immune system, thereby creating a favorable environment for endometrial cell survival and proliferation. These findings support the seed and soil concept, whereby biologically active endometrial cells (seeds) are capable of surviving and implanting in tissues rich in growth and inflammatory factors (soil), such as postoperative scar tissue. Consequently, differences in biological activity and tissue microenvironment may explain why only a small proportion of patients undergoing gynecologic surgery develop scar endometriosis.8
During menstruation, hormonal withdrawal triggers inflammatory responses and shedding of endometrial tissue. When endometrial tissue implants outside the uterine cavity, such as within the abdominal wall, it may retain its hormonal responsiveness and undergo cyclic bleeding, resulting in chronic cyclic pain and local inflammation.9
These mechanisms are consistent with the findings in the present case, in which the patient experienced cyclic pain and bleeding from the surgical scar beginning two years after cesarean section. Such symptoms represent a classic manifestation of scar endometriosis and often serve as key diagnostic clues distinguishing this condition from abscesses, granulomas, or postoperative wound infections. Cyclic pain is a hallmark symptom of endometriosis, including extrapelvic forms such as scar endometriosis. A retrospective study reported cyclic pain in 92.3% of scar endometriosis cases, while another study from India reported similar findings in 90.4% of patients.10,11
Table 1 demonstrates that previously reported scar endometriosis cases generally presented with lesions measuring approximately 1–3 cm in diameter, whereas the lesion in the present case measured 8 × 8× 8 cm. This finding supports the use of the term “giant” in this case, not as a standardized classification, but as a descriptive term reflecting its size relative to those documented in the literature. In addition, symptom onset in previously reported cases ranged from 10 months to 3 years following cesarean section. Similarly, the patient in the present case developed cyclic pain approximately two years after surgery, which is consistent with findings reported by Zhang et al, who observed a mean interval of 31.6 ± 23.9 months between surgery and symptom onset.6 The unusually large size of the lesion in this case contributed to diagnostic difficulty because it clinically mimicked other surgical conditions such as abscesses, hernias, or soft tissue tumors. This highlights the importance of considering scar endometriosis in women presenting with cyclic pain, bleeding, or abdominal wall masses at previous cesarean section scars to avoid delayed diagnosis and inappropriate management.
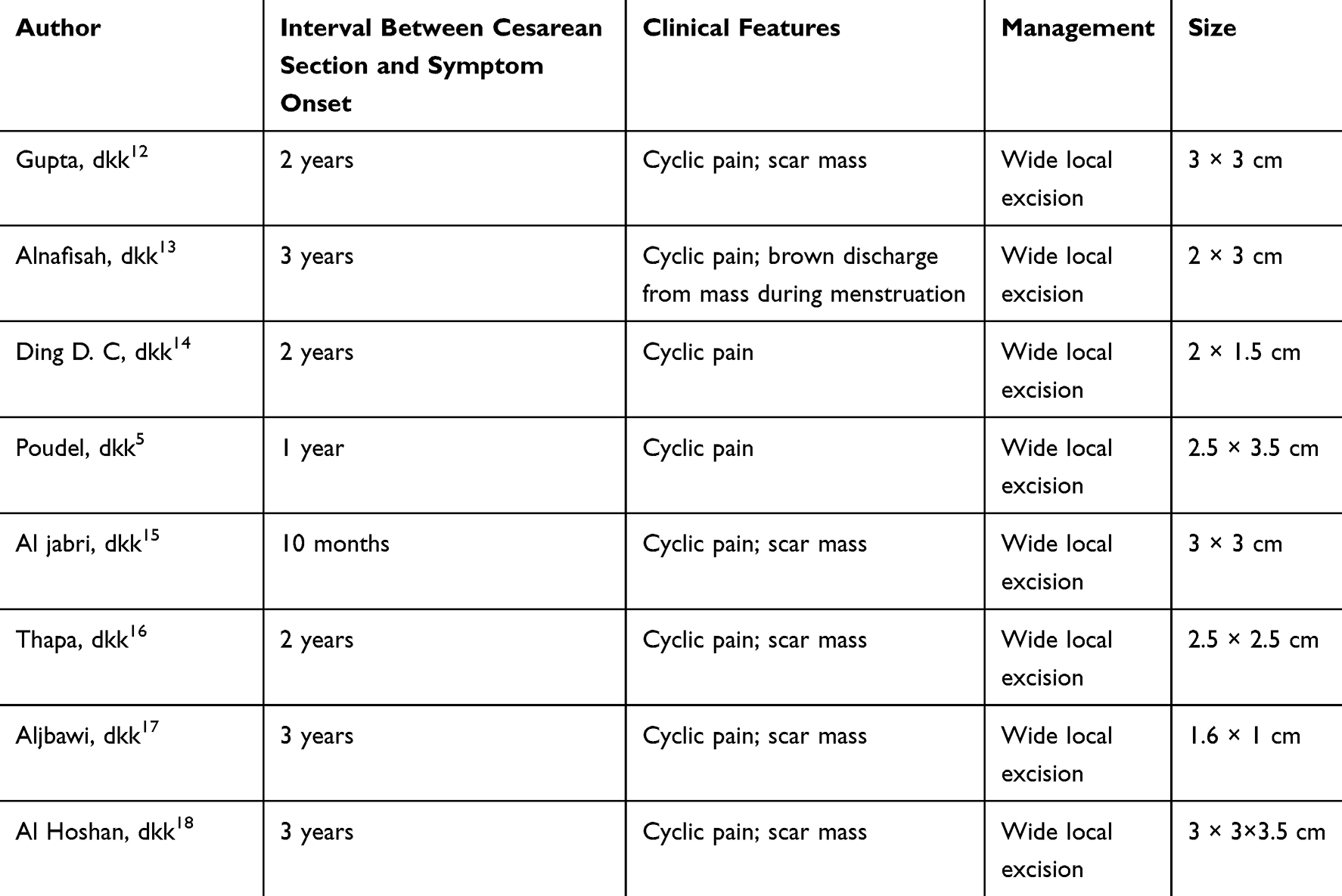 |
Table 1 Reported Cases of Cesarean Section Scar Endometriosis |
Several studies have investigated the coexistence of pelvic endometriosis with scar endometriosis. A review study reported that the incidence of concomitant pelvic endometriosis in patients with scar endometriosis ranged from 14.3% to 26%.19 Additionally, a retrospective study involving 104 patients found that 15.4% had concurrent pelvic endometriosis.10 Meanwhile, a systematic review by Gruber et al encompassing 12 studies reported a lower mean incidence of approximately 5.8%.3 Therefore, it is recommended that all patients diagnosed with scar endometriosis be evaluated for the possible presence of pelvic endometriotic lesions.19
Although scar endometriosis is rare, it can significantly impair quality of life because of chronic cyclic pain and recurrent symptoms. In addition, malignant transformation has been reported in approximately 1% of cases.20 Preventive strategies have therefore been proposed, including thorough irrigation of the surgical wound before closure, use of separate instruments for uterine and abdominal wall closure, and avoidance of contamination of the abdominal wall with endometrial tissue during cesarean section.6
One study reported that scar endometriosis most frequently occurs in the superficial layers of the abdominal wall, with approximately 70.3% of lesions located within the subcutaneous fat layer or between the fat and fascia.6 Another study demonstrated that patients with a higher body mass index (BMI) have an increased risk of developing scar endometriosis.21 In the present case, the patient had a BMI of 29.5 kg/m2, classified as overweight, which may represent a contributing risk factor. Ultrasonographic examination revealed a hypoechoic mass within the suprapubic subcutaneous layer, consistent with reports indicating that approximately 70% of abdominal wall endometriomas are located between the fat and fascial layers.
The primary management of scar endometriosis is complete surgical excision of the lesion, as this approach provides the best opportunity for definitive diagnosis and curative treatment.21 Hormonal therapies, such as gonadotropin-releasing hormone (GnRH) analogues or progestins, may be considered as adjunctive treatments.21 Recurrence may occur following inadequate excision; therefore, the fundamental surgical principle in managing scar endometriosis is wide, radical excision to ensure complete removal of endometriotic tissue.21
Wide excision with a safety margin of at least 1 cm from the lesion edges is recommended to ensure complete removal of endometriotic tissue. An appropriate surgical approach is also essential to remove all involved tissue, including any infiltration into the fascia or muscle, and to prevent further dissemination of endometrial cells during surgery.21 In the present case, the patient underwent excision of an 8 × 8×8 cm mass with a 1-cm safety margin, in accordance with the principles of radical excision. Postoperative histopathological examination confirmed the diagnosis of cesarean section scar endometriosis, and the patient reported complete resolution of symptoms without recurrence during approximately six months of postoperative follow-up. However, long-term follow-up was limited, as the patient declined further evaluation due to resolution of symptoms and financial constraints.
This study has several limitations inherent to case reports, including the inability to generalize findings. In addition, the duration of follow-up was relatively short, limited to six months, which may not be sufficient to fully assess long-term recurrence. Advanced imaging such as MRI was not performed due to limited accessibility and financial constraints, which may have restricted comprehensive evaluation of lesion extent and the possibility of concomitant pelvic endometriosis. Furthermore, postoperative hormonal therapy was not initiated, and long-term follow-up regarding medical management could not be assessed, as the patient declined further treatment due to financial limitations. Despite these limitations, this case provides important clinical insight into the diagnosis and management of large scar endometriosis.
Conclusion
Cesarean section scar endometriosis is a rare form of abdominal wall endometriosis that should be suspected in women presenting with cyclic pain, bleeding, or a mass at a previous surgical scar site. Large lesions may mimic abscesses, hernias, or soft tissue tumors, increasing the risk of diagnostic delay and misdiagnosis. Early recognition and complete surgical excision with at least a 1-cm safety margin remain essential to achieve symptom resolution and reduce recurrence risk.
Informed Consent Patient Statement
The authors confirm that written informed consent was obtained from the patient. The patient was informed about the details of the case and provided approval for the publication of the case report, including any accompanying images. All identifying information has been appropriately anonymized to ensure patient confidentiality.
Institutional Approval
Institutional approval was not required for the publication of this single-patient case report, in accordance with institutional policies and the ethical standards of the Declaration of Helsinki.
Acknowledgments
This publication charge is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnson NP, Hummelshoj L, Adamson GD, et al. World endometriosis society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315–7. doi:10.1093/humrep/dew293
2. Hirata T, Koga K, Osuga Y. Extra-pelvic endometriosis: a review. Reprod Med Biol. 2020;19(4):323–333. doi:10.1002/rmb2.12340
3. Gruber TM, Lange K, Ebeling GS, Henrich W, Mechsner S. Scar endometriosis, a form of abdominal wall endometriosis–a neglected obstetrical complication? Arch Gynecol Obstet. 2024;312(1):1–8. doi:10.1007/s00404-024-07834-2
4. Nepali R, Upadhyaya Kafle S, Pradhan T, Dhamala JN. Scar endometriosis: a rare cause of abdominal pain. Dermatopathology. 2022;9(2):158–163. doi:10.3390/dermatopathology9020020
5. Poudel D, Acharya K, Dahal S, Adhikari A. A case of scar endometriosis in cesarean scar: a rare case report. Int J Surg Case Rep. 2023;102(C):107852. doi:10.1016/j.ijscr.2022.107852
6. Zhang P, Sun Y, Zhang C, et al. Cesarean scar endometriosis: presentation of 198 cases and literature review. BMC Womens Health. 2019;19(1):14. doi:10.1186/s12905-019-0711-8
7. Go V-A, Chavez J, Robinson RD, Nicholson BJ. A seed or soil problem in early endometriosis: stromal cell origin drives cellular invasion and coupling over mesothelial cell origin. F&S Science. 2024;5(4):395–403. doi:10.1016/j.xfss.2024.08.001
8. Bulun SE. Endometriosis. N Engl J Med. 2009;360(3):268–279. doi:10.1056/NEJMra0804690
9. Maddern J, Grundy L, Castro J, Brierley SM. Pain in endometriosis. Front Cell Neurosci. 2020;14:590823. doi:10.3389/fncel.2020.590823
10. Matalliotakis M, Matalliotaki C, Zervou MI, Krithinakis K, Goulielmos GN, Kalogiannidis I. Abdominal and perineal scar endometriosis: retrospective study on 40 cases. Eur J Obstet Gynecol Reprod Biol. 2020;252:225–227. doi:10.1016/j.ejogrb.2020.06.054
11. Durairaj A, Sivamani H, Panneerselvam M. Surgical Scar endometriosis: an emerging enigma. Cureus. 2023;15(2):e35089. doi:10.7759/cureus.35089
12. Gupta P, Gupta S. Scar endometriosis: a case report with literature review. Acta Med Iran. 2015;53(12):793–795.
13. Alnafisah F, Dawa SK, Alalfy S. Skin endometriosis at the caesarean section scar: a case report and review of the literature. Cureus. 2018;10(1):e2063. doi:10.7759/cureus.2063
14. Ding D-C, Hsu S. Scar endometriosis at the site of cesarean section. Taiwanese Jo Obstetr Gynecol. 2006;45(3):247–249. doi:10.1016/S1028-4559(09)60234-5
15. Al-Jabri K. Endometriosis at caesarian section scar. Oman Med J. 2009;24(4):294. doi:10.5001/omj.2009.59
16. Thapa A, Kumar A, Gupta S. Abdominal wall endometriosis: report of a case and how much we know about it. Internet J Surg. 2007;9(2):1–2.
17. Aljbawi M, Redan L, Al-Bitar A, Saghier E. Abdominal wall endometriosis in a cesarean scar: a case report. J Med Case Reports. 2025;19(1):239. doi:10.1186/s13256-025-05301-3
18. Al Hoshan MS, Shaikh AA. A classical case of cesarean scar endometriosis in a 35-year-old woman presenting with cyclical abdominal pain: a case report. Ame J Case Reports. 2023;24:e940200–1. doi:10.12659/AJCR.940200
19. Uzunçakmak C, Güldaş A, Ozçam H, Dinç K. Scar endometriosis: a case report of this uncommon entity and review of the literature. Case Reports Obstetrics Gynecol. 2013;2013:386783. doi:10.1155/2013/386783
20. Carsote M, Terzea DC, Valea A, Gheorghisan-Galateanu -A-A. Abdominal wall endometriosis (a narrative review). Int J Med Sci. 2020;17(4):536–542. doi:10.7150/ijms.38679
21. Fernicola A, Calogero A, Peluso G, et al. Surgical reconstruction of abdominal wall endometriosis post-cesarean section: a monocentric experience of a rare pathology. J Clin Med. 2025;14(15):5416. doi:10.3390/jcm14155416
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Case Series and a Literature Review: Two Ovarian Clear Cell Carcinoma Cases with Recurrent Endometriosis

Yin D, Jiang YJ
International Journal of Women's Health 2023, 15:1611-1619
Published Date: 24 October 2023