Back to Journals » International Journal of Women's Health » Volume 18
Gestational Diabetes in Somali Women: Neglected Risks for Maternal and Neonatal Health
Authors Mudei NM ![]() , Adawe MMM, Ali HA, Mohamud KH
, Adawe MMM, Ali HA, Mohamud KH
Received 29 March 2026
Accepted for publication 3 June 2026
Published 8 June 2026 Volume 2026:18 612886
DOI https://doi.org/10.2147/IJWH.S612886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Nasteho Mohamud Mudei,1 Mariam Mohamed Mohamud Adawe,1 Hamdi Abdi Ali,2 Kadra Hassan Mohamud3
1Department of Obstetrics and Gynecology, Dr. Sumait Hospital, SIMAD University, Mogadishu, Banaadir, Somalia; 2Dr. Sumait Hospital, SIMAD University, Mogadishu, Banaadir, Somalia; 3Department of Pediatrics, Dr. Sumait Hospital, SIMAD University, Mogadishu, Banaadir, Somalia
Correspondence: Nasteho Mohamud Mudei, Department of Obstetrics and Gynecology, Dr. Sumait Hospital, SIMAD University, Mogadishu, Banaadir, Somalia, Tel +252615682055, Email [email protected]; [email protected]
Abstract: This commentary examines gestational diabetes mellitus (GDM) as an under-recognised contributor to adverse maternal and neonatal outcomes among Somali women and in comparable fragile settings. GDM is associated with pre-eclampsia, macrosomia, obstructed labour, stillbirth, neonatal morbidity, and later type 2 diabetes in women and offspring. Globally, hyperglycaemia in pregnancy affects approximately one in six live births, yet detection and management remain least accessible in low-resource and conflict-affected settings. Somalia has high maternal and neonatal mortality, but local GDM prevalence data are not available and routine screening is rarely embedded in antenatal care. Drawing on WHO guidance, international evidence, and literature on Somali, East African, migrant, and humanitarian populations, we argue that GDM is made invisible by overlapping clinical, social, and health-system factors: early-life undernutrition, nutritional transition, high fertility, short birth intervals, limited antenatal access, weak diagnostic supply chains, low awareness of asymptomatic “sugar disease”, and limited policy attention to pregnancy-related non-communicable diseases. These gaps convert a detectable and manageable condition into preventable complications, including obstructed labour, postpartum haemorrhage, hypertensive disorders, stillbirth, neonatal hypoglycaemia, and intergenerational diabetes risk. Practical responses include pragmatic risk-based or simplified glucose screening where oral glucose tolerance testing is not feasible, reliable access to glucometers and strips, midwife-led protocols, Somali-language education, engagement of families and community leaders while protecting women’s autonomy, postpartum follow-up linked to immunisation and child-health contacts, and inclusion of GDM indicators in maternal health information systems. Recognising and addressing GDM is essential for reducing preventable maternal and neonatal harm and for strengthening equitable women’s healthcare in fragile settings.
Keywords: gestational diabetes mellitus, maternal mortality, neonatal mortality, antenatal care, postpartum follow-up, non-communicable diseases, fragile settings
Introduction
Gestational diabetes mellitus (GDM), defined as hyperglycaemia first recognised during pregnancy that does not meet criteria for overt diabetes, is an increasingly important maternal and newborn health issue. It is associated with pre-eclampsia, fetal overgrowth, obstructed labour, postpartum haemorrhage, stillbirth, neonatal hypoglycaemia, respiratory morbidity, and later type 2 diabetes in both women and their children.1–8 These outcomes are especially consequential where antenatal screening, intrapartum monitoring, operative delivery, and neonatal supportive care are limited.
The global relevance of GDM has increased as non-communicable diseases (NCDs) intersect with maternal health. The International Diabetes Federation estimated that 23.0 million live births in women aged 20–49 years were affected by hyperglycaemia in pregnancy in 2024, equivalent to 19.7% of live births; most cases occurred in low- and middle-income countries, where access to antenatal care and diagnostic services is often constrained.1 WHO’s 2025 recommendations on diabetes during pregnancy further emphasise integrated care, glucose monitoring, individualized counselling, and postnatal follow-up as core components of quality maternity care.3
In Somalia, the limited attention to GDM is clinically and ethically important. The country continues to experience high maternal and neonatal mortality, and health-system capacity has been weakened by conflict, displacement, drought, poverty, shortages of trained staff, and uneven access to essential services.9–12 Maternal health programmes understandably prioritise acute obstetric emergencies such as haemorrhage, sepsis, hypertensive disorders, and obstructed labour. However, metabolic complications such as GDM can be upstream contributors to these same outcomes and may remain undiagnosed or undocumented.2–5
There are no robust, nationally representative local prevalence data on GDM in Somalia. This absence of data should not be interpreted as absence of disease; rather, it reflects weak surveillance, limited routine screening, and the exclusion of pregnancy-related NCD indicators from many maternal health information systems.10,12 In Somali women living in refugee camps or diaspora settings, adverse perinatal outcomes and barriers to maternity care have been described, but GDM has rarely been investigated as a possible contributor.13–17 This creates a knowledge gap at the intersection of maternal health, NCD care, humanitarian health, and reproductive justice.
This commentary examines GDM as a neglected contributor to adverse maternal and neonatal outcomes among Somali women. It synthesises WHO guidance, global evidence on hyperglycaemia in pregnancy, and literature on Somali, East African, migrant, and fragile-setting populations. It is not a systematic review and does not present primary data; instead, it offers a clinically grounded and policy-oriented analysis of why GDM remains under-recognised and how pragmatic responses could be integrated into existing maternal and newborn health services.
Evidence Base and Scope of This Commentary
To improve transparency, this article was developed as an expert commentary informed by targeted literature searching rather than systematic review methodology. The authors considered WHO and IDF guidance, peer-reviewed evidence on hyperglycaemia in pregnancy, and studies addressing maternal health, Somali women, East African or migrant populations, refugee or humanitarian contexts, NCDs, and fragile health systems. Targeted searches were undertaken in PubMed and grey literature sources, supplemented by known policy documents and reference chaining. Because the purpose was conceptual and policy-oriented, no formal search protocol, risk-of-bias assessment, statistical synthesis, or meta-analysis was performed. The article therefore uses cited evidence selectively to support a structured argument and should be interpreted as a commentary rather than an evidence synthesis.
Converging Clinical and Structural Risks for Somali Women
Early-Life Undernutrition and Developmental Programming
Conflict, drought, food insecurity, and displacement expose many Somali girls and women to undernutrition before and during their reproductive years. Developmental-origins research links early-life undernutrition followed by later nutritional transition to insulin resistance, obesity, and diabetes risk.8,18 For pregnant women, this life-course pattern can increase susceptibility to GDM. The point is not to individualise blame, but to recognise that metabolic risk is socially produced through deprivation, displacement, and limited access to preventive care.
Nutritional and Lifestyle Transition
Urbanisation, displacement, and migration can shift diets toward refined carbohydrates, sugary beverages, and energy-dense foods, while insecurity and limited safe spaces reduce physical activity.19 In Somali urban and diaspora settings, these changes coexist with poverty and food insecurity, creating a dual burden of undernutrition and overnutrition. In pregnancy, this nutritional transition can worsen insulin resistance and make dietary counselling difficult when healthy foods are unaffordable or unavailable.
High Fertility and Short Birth Intervals
Somalia has high fertility, and many women experience repeated pregnancies with limited time for metabolic recovery.11 Closely spaced pregnancies also reduce opportunities for postpartum glucose testing, counselling, and linkage to primary care after a GDM-affected pregnancy. Family planning access, respectful counselling, and preconception care are therefore relevant not only to birth spacing but also to long-term diabetes prevention.
Limited Access to Quality Antenatal and Intrapartum Care
WHO diagnostic guidance recommends testing for hyperglycaemia in pregnancy, and the 2025 WHO recommendations emphasise ongoing glucose monitoring, individualized advice on diet and physical activity, and timely pharmacological treatment when needed.2,3,20 In Somalia, routine GDM screening is rarely embedded in antenatal care outside some urban or private facilities. Screening may be optional or fee-based, and facilities may lack trained staff, laboratory capacity, glucometers, glucose strips, lancets, calibration systems, referral pathways, and reliable resupply.10,12 These supply-chain realities mean that even simple recommendations can fail at the point of care unless procurement and supervision are addressed.
Comparative Relevance to Fragile and Humanitarian Settings
The Somali case reflects a broader challenge in fragile and humanitarian settings: maternal health packages often focus on life-saving obstetric care, while pregnancy-related NCDs are treated as secondary or specialised concerns.3,10,21 Refugee settlements, internally displaced persons camps, and conflict-affected districts may lack laboratory infrastructure, continuity of care, and reliable follow-up after delivery. Therefore, the argument advanced here is locally focused but globally relevant: GDM care needs to be simplified, decentralised, and integrated into routine maternal health platforms rather than reserved for tertiary hospitals.
A Multi-Level Awareness Gap with Clinical Implications
Community Perceptions and Health Literacy
In Somali language and community discourse, diabetes may be described as “sugar disease” and commonly associated with older adults, severe thirst, weight loss, wounds, or long-term illness.11,15,16 Pregnancy-related hyperglycaemia is often asymptomatic, so women may not perceive testing as necessary when they feel well. Low literacy, limited Somali-language education materials, mistrust of health institutions, and prior marginalisation can further reduce uptake of screening and follow-up. Culturally appropriate education should therefore explain that GDM can be silent but harmful, that testing is preventive rather than punitive, and that early management protects both mother and baby.
Household and Community Decision-Making
Costs, transport, timing of visits, and decisions about investigations are often negotiated within households. Male partners, elders, and other relatives may influence whether a woman attends antenatal care, pays for glucose testing, follows dietary advice, or returns postpartum.10,15,16 Community engagement should therefore include families, elders, community health workers, and religious leaders while ensuring that women’s autonomy, confidentiality, and informed decision-making remain central.
Provider Knowledge, Tools, and Priorities
Midwives, nurses, doctors, and community health workers in fragile settings often manage high caseloads with limited supplies. Without protocols, job aids, glucose testing tools, or referral criteria, providers may focus on immediate obstetric emergencies and miss silent metabolic risk. Training should therefore be practical: who should be screened, which test is feasible, how results should be interpreted, what dietary counselling can be offered with locally available foods, when referral is needed, and how delivery and newborn monitoring should be planned.
Policy, Leadership, and Health Communication Gaps
GDM requires leadership across levels. Hospital managers can integrate glucose testing into antenatal workflows, protect stocks of glucometers and strips, and audit outcomes. District health teams can supervise implementation, track coverage, and support referral. The Ministry of Health and partners can include GDM in maternal health and NCD policies, procurement plans, training curricula, and health information systems. Clinical champions can mentor staff, adapt protocols to local constraints, and keep the issue visible in quality-improvement meetings. Without this leadership architecture, GDM remains everyone’s concern but no one’s responsibility.
Pathways From Unrecognised GDM to Adverse Outcomes
The clinical mechanisms linking untreated GDM to adverse outcomes are well established and become more dangerous when emergency obstetric and neonatal services are constrained.2–7 Figure 1 summarises the pathways through which structural vulnerabilities, health-system gaps, and awareness gaps can lead to missed screening, delayed diagnosis, maternal and neonatal complications, and intergenerational diabetes risk. Figure 1. Conceptual pathways linking unrecognised GDM to adverse maternal, neonatal, and intergenerational outcomes in Somali and comparable fragile settings.
 |
Figure 1 Pathways linking unrecognised GDM to adverse outcomes. |
Macrosomia, Obstructed Labour, and Haemorrhage
Maternal hyperglycaemia can promote fetal hyperinsulinaemia and overgrowth, increasing birthweight and shoulder circumference.2,4,5 In settings with limited ultrasound, delayed referral, and restricted access to operative delivery, macrosomia increases the risk of obstructed labour, shoulder dystocia, uterine rupture, birth trauma, asphyxia, and postpartum haemorrhage. These are not abstract complications; they overlap directly with leading causes of maternal and neonatal death in Somalia.9,10
Hypertensive Disorders and Eclampsia
GDM is associated with gestational hypertension and pre-eclampsia.5 Where blood pressure monitoring is inconsistent, magnesium sulphate access is uneven, and referral is delayed, women may present late with severe disease. Because the metabolic component is rarely documented, GDM may remain hidden behind labels such as pre-eclampsia, eclampsia, or fetal death.
Stillbirth and Early Neonatal Complications
Hyperglycaemia in pregnancy increases risks of stillbirth, preterm birth, neonatal hypoglycaemia, respiratory distress, neonatal intensive care admission, and birth injury.2,4,5 Where newborn glucose monitoring, thermal care, feeding support, resuscitation, and referral are limited, these complications more often lead to death or disability. Strengthening GDM care should therefore be viewed as part of essential newborn care, not only maternal NCD care.
Long-Term and Intergenerational Risk
Women with a history of GDM have a substantially increased risk of later type 2 diabetes, and their children are at increased risk of obesity and impaired glucose tolerance.7,8 In Somali communities already affected by infectious disease, undernutrition, trauma, and weak primary care, this intergenerational NCD burden could deepen existing inequities. Postpartum follow-up is therefore a prevention opportunity that extends beyond a single pregnancy.
Clinical and Public Health Opportunities
Implementation-oriented summary of practical barriers and feasible responses for integrating GDM screening, supplies, provider support, community education, postpartum follow-up, and data accountability into maternal health services in Somali and comparable fragile settings. Table 1
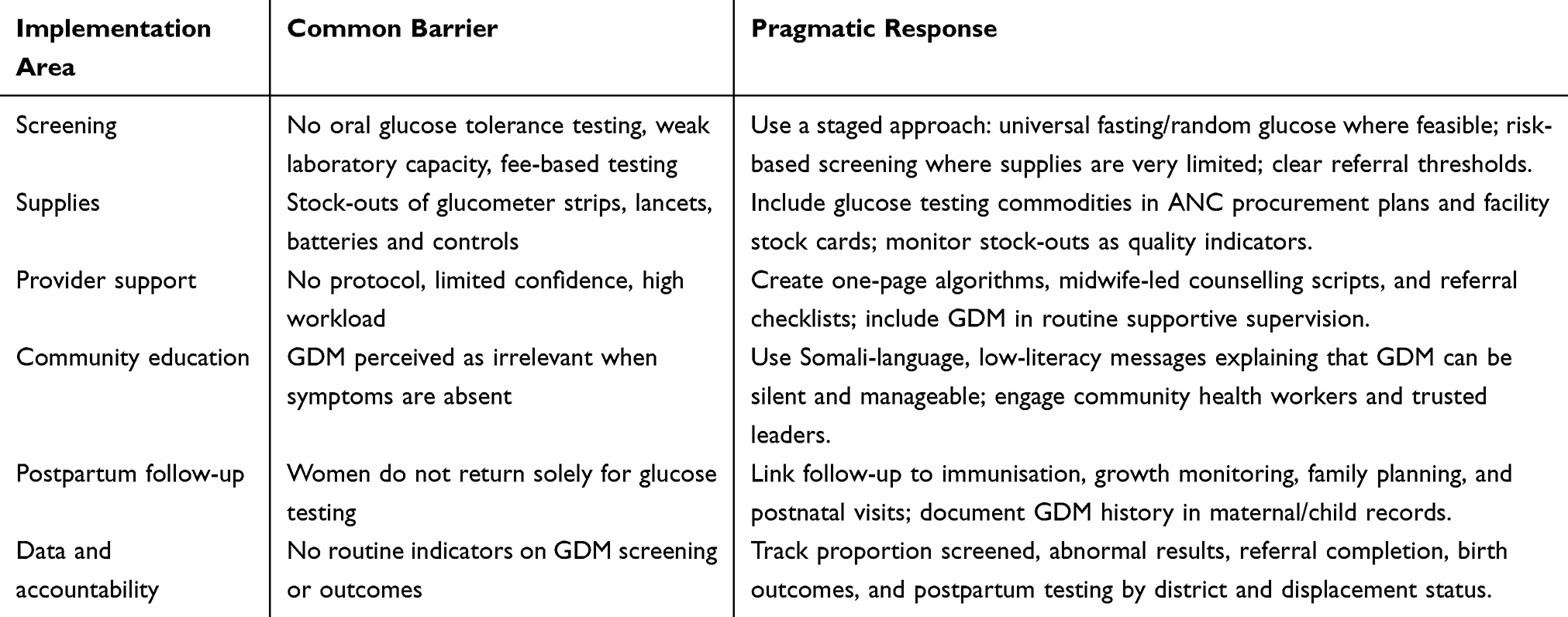 |
Table 1 Provides an Implementation-Oriented Summary of Practical Barriers and Feasible Responses |
Adapt Screening to Available Resources
The ideal approach is to implement WHO-aligned testing for hyperglycaemia in pregnancy at 24–28 weeks and earlier testing for women with risk factors.2,3,20 Where oral glucose tolerance testing is not feasible, a pragmatic phased approach may be more realistic than no screening. Facilities can start with risk-based fasting or random blood glucose testing, prioritising women with previous macrosomic baby, previous stillbirth, obesity, family history of diabetes, glycosuria, hypertension, advanced maternal age, or symptoms suggestive of hyperglycaemia. This should be framed as an interim strategy while systems build capacity for more complete testing.
Make Supplies and Referral Pathways Part of Maternal-Health Quality Improvement
Implementation depends on reliable commodities. Glucometers without strips, strips without lancets, and testing without referral pathways will not change outcomes. Facility managers and district teams should include glucose testing supplies in procurement plans, monitor stock-outs, define referral thresholds, and ensure that women with abnormal results receive counselling, follow-up testing, delivery planning, and newborn monitoring.
Provide Culturally Tailored Education
Education should use plain Somali language and low-literacy visual tools. Messages should explain that GDM may have no symptoms, can affect labour and the baby, and is often manageable through diet, physical activity where safe, glucose monitoring, and medication when needed. Advice must be realistic: recommending foods that women cannot afford or access is unlikely to be effective. Counselling should therefore focus on locally available staples, portion sizes, reducing sugary drinks, spacing meals, and safe activity within cultural and security constraints.
Link Postpartum Follow-Up to Services Women Already Use
Postpartum glucose testing is often difficult when women must travel solely for their own follow-up. Linking postpartum diabetes risk counselling and testing to immunisation, growth monitoring, postnatal care, breastfeeding support, and family planning visits could improve feasibility. A simple record of GDM history in mother-held cards or child-health records can help providers identify women needing follow-up during routine contacts.22
Generate Local Evidence and Embed GDM in Policy
Somalia needs operational evidence on the prevalence of GDM among women who attend antenatal care, feasibility of simplified screening pathways, cost and reliability of diagnostic supplies, referral completion, birth outcomes, and postpartum follow-up. Until such data are available, programme decisions should be guided by global evidence and local implementation learning. Including basic GDM indicators in health information systems would help quantify the burden, identify inequities by district or displacement status, and support resource allocation.
Limitations
This commentary has limitations. It does not present primary data from Somalia, and nationally representative GDM prevalence estimates are not currently available. The evidence cited includes global studies, WHO and IDF guidance, literature from Somali migrant populations, and health-system evidence from Somalia and comparable contexts. These sources are relevant but cannot fully substitute for local epidemiological and implementation research. The proposed actions should therefore be adapted, piloted, and evaluated in Somali facilities and communities.
Conclusion
GDM is a largely under-recognised but clinically significant contributor to adverse maternal and neonatal outcomes among Somali women. Early-life undernutrition, nutritional transition, high fertility, short birth intervals, limited antenatal access, diagnostic supply constraints, and awareness gaps create conditions in which GDM can remain undetected until complications occur.
Recognising and addressing GDM in Somali women is essential for reducing preventable maternal and neonatal deaths and breaking intergenerational cycles of ill-health. Integrating pragmatic screening, culturally tailored education, provider support, diagnostic commodities, referral pathways, postpartum follow-up, and routine data collection into maternal health services represents a feasible and urgent priority in fragile settings.
Abbreviations
ANC, antenatal care; GDM, gestational diabetes mellitus; IDF, International Diabetes Federation; NCDs, non-communicable diseases; WHO, World Health Organization.
Ethics Approval and Consent
Not applicable. This article is a commentary and did not involve human participants, patient data, or identifiable personal information.
Acknowledgments
This article was supported by SIMAD University, Somalia. The authors extend sincere appreciation to healthcare workers, including obstetricians, midwives, nurses, and allied maternal health professionals across Somalia, for their dedication and frontline service delivery, which informed the perspectives discussed in this commentary. Special thanks are extended to Dr. Sumait Hospital for fostering a supportive environment that promotes clinical inquiry and research engagement.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. World Health Organization. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. Geneva: World Health Organization; 2013.
3. World Health Organization. WHO Recommendations on Care for Women with Diabetes During Pregnancy. Geneva: World Health Organization; 2025.
4. Metzger BE, Gabbe SG, Persson B, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(7):676–8. doi:10.2337/dc10-0719
5. Farrar D, Simmonds M, Bryant M, et al. Hyperglycaemia and risk of adverse perinatal outcomes: systematic review and meta-analysis. BMJ. 2016;354:i4694. doi:10.1136/bmj.i4694
6. Sweeting A, Wong J, Murphy HR, Ross GP. A clinical update on gestational diabetes mellitus. Endocr Rev. 2022;43(5):763–793. doi:10.1210/endrev/bnac003
7. Bellamy L, Casas J-P, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009;373(9677):1773–1779. doi:10.1016/S0140-6736(09)60731-5
8. Herring SJ, Oken E. Obesity and diabetes in mothers and their children: can we stop the intergenerational cycle? Curr Diab Rep. 2011;11(1):20–27. doi:10.1007/s11892-010-0156-9
9. World Health Organization, United Nations Children’s Fund, United Nations Population Fund, World Bank Group, United Nations Department of Economic and Social Affairs Population Division. Trends in Maternal Mortality 2000-2023: Estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Geneva: World Health Organization; 2025.
10. World Health Organization Regional Office for the Eastern Mediterranean. Somalia: Reproductive, Maternal, Newborn, Child and Adolescent Health Situation Analysis. Cairo: WHO Regional Office for the Eastern Mediterranean; 2019.
11. United Nations Population Fund Somalia. Population Situation Analysis: Somalia. Nairobi: UNFPA Somalia; 2021.
12. Greene MC, Rees S, Likindikoki S, et al. Developing an integrated intervention to address intimate partner violence and psychological distress in Congolese refugee women in Tanzania. Conflict and Health. 2019;13:38. doi:10.1186/s13031-019-0222-0
13. Small R, Gagnon A, Gissler M, et al. Somali women and their pregnancy outcomes postmigration: data from six receiving countries. BJOG. 2008;115(13):1630–1640. doi:10.1111/j.1471-0528.2008.01942.x
14. Essén B, Hanson BS, Ostergren P-O, Lindquist PG, Gudmundsson S. Increased perinatal mortality among sub-Saharan immigrants in a city-population in Sweden. Acta Obstet Gynecol Scand. 2000;79(9):737–743. doi:10.1080/00016340009169187
15. Degni F, Suominen S, Essén B, El Ansari W, Vehviläinen-Julkunen K. Communication and cultural issues in providing reproductive health care to immigrant women: health care providers’ experiences in meeting somali women living in Finland. J Immigrant Minority Health. 2012;14(2):330–337. doi:10.1007/s10903-011-9465-6
16. Carroll J, Epstein R, Fiscella K, et al. Knowledge and beliefs about health promotion and preventive health care among Somali women in the United States. Health Care Women Int. 2007;28(4):360–380. doi:10.1080/07399330601179935
17. Berhe K, Kassa GM, Fekadu GA, Muche AA. Prevalence of hypertensive disorders of pregnancy in Ethiopia: a systemic review and meta-analysis. BMC Pregnancy Childbirth. 2018;18(1):34. doi:10.1186/s12884-018-1667-7
18. Fall CHD, Sachdev HS, Osmond C, et al. Association between maternal age at childbirth and child and adult outcomes in the offspring: a prospective study in five low-income and middle-income countries (COHORTS collaboration). Lancet Glob Health. 2015;3(7):e366–e377. doi:10.1016/S2214-109X(15)00038-8
19. Popkin BM. Nutrition transition and the global diabetes epidemic. Curr Diab Rep. 2015;15(9):64. doi:10.1007/s11892-015-0631-4
20. World Health Organization. Meeting of the Guideline Development Group for the Monitoring and Management of Hyperglycaemia in Pregnancy. Geneva: World Health Organization; 2025.
21. World Health Organization. Noncommunicable Diseases Country Profiles 2022. Geneva: World Health Organization; 2022.
22. World Health Organization. WHO Antenatal Care Recommendations for a Positive Pregnancy Experience. Geneva: World Health Organization; 2016.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Maternal and Newborn Health in Somalia: A Narrative Review of Health System Challenges and Public Health Priorities
Mohamoud JH, Adam MH, Mohamed AMS, Garba B, Mahamud MA, Asowe HA
International Journal of Women's Health 2026, 18:606754
Published Date: 5 May 2026