Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 15
Germline PRDM1 Variant rs2185379 in Long-Term Recurrence-Free Survivors of Advanced Ovarian Cancer
Authors Mitamura T ![]() , Zhai T
, Zhai T ![]() , Hatanaka KC, Hatanaka Y, Amano T, Wang L, Tanaka S, Watari H
, Hatanaka KC, Hatanaka Y, Amano T, Wang L, Tanaka S, Watari H
Received 25 August 2022
Accepted for publication 18 November 2022
Published 29 November 2022 Volume 2022:15 Pages 977—984
DOI https://doi.org/10.2147/PGPM.S387120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Takashi Mitamura,1 Tianyue Zhai,1 Kanako C Hatanaka,2 Yutaka Hatanaka,2,3 Toraji Amano,4 Lei Wang,5,6 Shinya Tanaka,5,6 Hidemichi Watari1
1Department of Obstetrics and Gynecology, Hokkaido University Faculty of Medicine, Hokkaido University, Sapporo, Hokkaido, Japan; 2Center for Development of Advanced Diagnostics, Hokkaido University Hospital, Sapporo, Hokkaido, Japan; 3Research Division of Genome Companion Diagnostics, Hokkaido University Hospital, Sapporo, Hokkaido, Japan; 4Clinical Research and Medical Innovation Center, Hokkaido University Hospital, Sapporo, Japan; 5Institute for Chemical Reaction Design and Discovery, Hokkaido University, Sapporo, Hokkaido, Japan; 6Department of Cancer Pathology, Faculty of Medicine, Hokkaido University, Sapporo, Hokkaido, Japan
Correspondence: Takashi Mitamura, Department of Obstetrics and Gynecology, Hokkaido University Faculty of Medicine, Hokkaido University, North15, West 7, Kita-Ku, Sapporo, 0608638, Hokkaido, Japan, Tel +81 11 706 5941, Fax +81 11 706 7711, Email [email protected]
Purpose: To identify the germline genetic characteristics of long-term recurrence-free survivors that can be applied to establishing a new strategy for curing advanced cancer, we investigated the whole-genome single nucleotide variants of ovarian cancer patients.
Patients and Methods: DNA specimens were obtained from rare long-term recurrence-free survivors with FIGO stage III–IV ovarian cancer with no recurrence for 8– 23 years after primary treatments for a whole-genome analysis of approximately 660,000 single nucleotide variants. We then established a mouse model with a notable gene alteration by CRISPR/Cas9 to confirm the biological role.
Results: The long-term recurrence-free survivors more frequently had germline heterozygous variant rs2185379 of the PRDM1 gene exon than patients with early recurrence (6.8-fold, P=0.013) and the general population. In the mouse model, primary intraperitoneal disseminated tumors of allograft ID8 were significantly smaller in the germline heterozygous rs2185379 group than in the wild-type group (57.4% decrease, P=0.008). Immunohistochemistry showed that the area of distribution of infiltrating T lymphocytes with positive CD8 staining was significantly increased in the germline heterozygous rs2185379 group in comparison to the wild-type group.
Conclusion: Germline heterozygous rs2185379 in PRDM1 is correlated with an excellent prognosis and can be used to establish a new strategy for treating advanced ovarian cancer.
Keywords: ovarian cancer, long-term survivors, rs2185379, PRDM1
Introduction
Most cancer research does not result in clinical practices because experimental treatments do not show expected effects or patients experience unexpected adverse events. When we try to overcome this inefficiency, understanding the difference in innate genetic background between patients and simulating ideal conditions of patients with a good prognosis is critical. Although patients with advanced ovarian cancer once achieve remission with combination therapy consisting of maximal debulking surgery and chemotherapy, recurrence mainly occurs within three years, and 10-year disease-free survival is under 10–30%.1–4 On the other hand, some patients with advanced disease, who seem to have a poor prognosis, never experience recurrence and achieve long-term disease-free survival without extended maintenance chemotherapy or other sophisticated treatments. This fact suggests that survivors have innate high sensitivity to chemotherapy or anticancer immunity that cures microscopic-recurrence before it grows large enough to be detected by standard imaging tests. To find the germline genetic characteristics of long-term recurrence-free survivors that can be applied to establishing a new strategy for the curative treatment of advanced cancer, we investigated the whole-genome single nucleotide variants of ovarian cancer patients.
Materials and Methods
Ovarian Cancer Patients and Whole-Genome Single Nucleotide Variant (SNV) Analysis
This research was carried out according to the principles set out in the 1964 Declaration of Helsinki. The Institutional Review Board of Hokkaido University approved all of the experiments on the human genome for this study (registration ID: 17–017). We obtained white blood cell specimens that contained DNA of germline origin from patients with ovarian cancer who understood the purpose of this study, agreed to provide samples, and gave us their written informed consent. Patients treated at Hokkaido University Hospital between 1990 and 2018 were eligible for inclusion. We defined “long-term recurrence-free survivor” as a patient without recurrence at five years after the end of the initial treatment for newly diagnosed advanced (International Federation of Gynecology and Obstetrics [FIGO] stage III or IV, 2014 FIGO classification5) ovarian cancer, primary peritoneal cancer, or fallopian tube cancer. We also defined “early recurrence” as the development of recurrent disease within five years after the end of the initial treatment.
We used the DNA specimens to perform a whole-genome SNV analysis (Asian Screening Array assay;6 Genesis Healthcare, Tokyo, Japan) specified to East Asian populations, with the iScan System (Illumina, San Diego, CA, USA). Briefly, this analysis can comprehensively analyze approximately 660,000 SNVs. To compare the variant frequency with a large general population, we used the SNV array data provided by the Tohoku Medical Megabank Organization.7
CRISPR/Cas9-Mediated Genome Engineering
The Institutional Review Board of Hokkaido University approved all of the animal protocols in this study (registration ID: 20–0161). We performed all animal experiments according to the protocol approved by the Institutional Animal Care and Use Committee at the Hokkaido University Graduate School of Medicine. We used CRISPR/Cas9-mediated genome editing to construct a C57BL/6 mouse model (Cyagen Biosciences Inc) with a heterozygous point mutation (G72S) at the mouse germline prdm1 on chromosome 10 (GenBank accession number: NM_007548.4; Ensembl: ENSMUSG00000038151).
The guideRNA for the mouse prdm1 gene, the donor oligo containing G72S (GGT to AGT) mutation sites, and Cas9 mRNA were co-injected into fertilized mouse eggs to generate targeted knock-in offspring. We confirmed the genotypes by in-house PCR with the following primers:
prdm1(G72S)-F-GTCTAGCTCCGGCTCCGTGAAG
prdm1(G72S)-R-GCTGCCAGTTAGCTTTCCCAAGAC
To obtain offspring with the germline heterozygous variant and wild type for the following experiment, we crossbred male and female mice with the germline heterozygous variant and checked the genotypes with DNA extracted from their tails.
Allogenic Transplantation of Ovarian Cancer Cells
We injected ID8 mouse ovarian surface epithelial cancer cells (3 x 106) in 200μL cell culture media into the peritoneal cavities of mice (age: 8 to 12 weeks) using a 27G needle and a 1 mL disposable syringe. After injection, we checked the general condition according to humane endpoint guidelines for all mice. At 80 days after transplantation, we sacrificed the mice by cervical dislocation.
Statistical Analyses
For in vitro studies, we compared normally distributed-continuous variables using Student’s t-test. To test the difference in the proportions of single nucleotide variants (SNVs) according to the prognosis and the proportions of immunostaining positivity by genotype, we used Pearson’s χ2 test. All statistical analyses were performed using the JMP® Pro software program, ver. 14.0.0 (SAS Institute, Cary, NC, USA). All statistical tests were two-sided, and P-values less than 0.05 were considered statistically significant.
Biospecimen Collection, Cell Culture, and Immunohistochemistry
The details of these methods are shown in Supplementary Information.
Results
We obtained DNA samples from 24 patients: 13 long-term recurrence-free survivors and 11 patients with early recurrence (Table 1). All long-term recurrence-free survivors underwent adjuvant chemotherapy after primary debulking surgery or neoadjuvant chemotherapy followed by interval debulking surgery with a combination of cytotoxic anticancer agents. The anticancer agents included paclitaxel, docetaxel, carboplatin, cisplatin, cyclophosphamide, and doxorubicin. Only one of 13 (7.7%) long-term recurrence-free survivors underwent molecular-targeted therapy with bevacizumab, while 6 of 11 (54.5%) patients with early recurrence underwent treatment with either bevacizumab or olaparib. We did not check copy number variations or large exon deletions of germline BRCA1 and BRCA2. On the other hand, we examined the representative single nucleotide variants and indels, and 2 of 13 (15.4%) long-term recurrence-free survivors and 2 of 9 (18.2%) of patients with early recurrence were found to have germline BRCA1 pathogenic variant rs80357086, c.188T>A (p.Leu63Ter). The proportion of high-grade serous carcinoma was 53.9% and 63.6% in the survivors without recurrence and patients with early recurrence, respectively, and did not seem to influence the patients’ prognoses (P=0.63). When we defined optimal surgery as cases with gross residual lesions < 2 cm in size, 1 patient was deemed inoperable, and another underwent suboptimal surgery among the patients with early recurrence. All other patients underwent optimal surgery by primary or interval debulking surgery after neoadjuvant chemotherapy. Gross residual disease was not correlated with recurrence in our series (P=0.20).
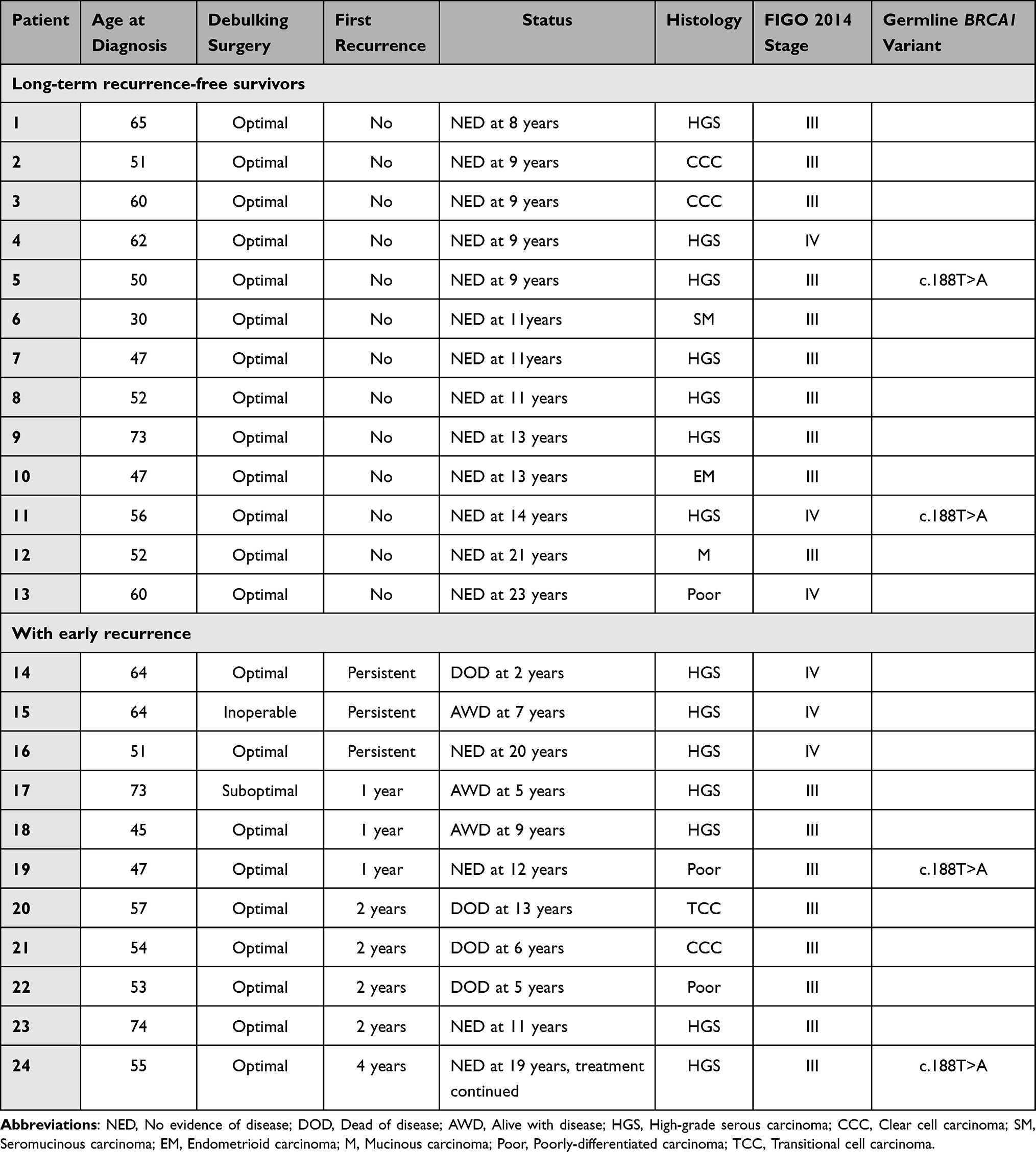 |
Table 1 Clinical Characteristics of the Ovarian Cancer Patients |
Genome sequencing showed that the various gene alterations appeared more frequently in the good prognosis group than in the worse group. Among those alterations, we took notice of SNVs in exons because they can be missense variants for a gain of anticancer function, and it should be relatively easy—from a biotechnological viewpoint—to reproduce these SNVs in mouse models. We compared the allele frequency of all SNVs and narrowed the candidates to four that were associated with the most significant change in the prognosis (Table 2). The frequency of all four SNVs was 6.8-fold that in patients with early recurrence (P=0.013). To compensate for the small number of control subjects in our study, we also referred to the mega-database of the general Japanese population. The allele frequency of PRDM1 rs2185379 in the general population and that in the patients with early recurrence in this study were similar, while the frequency of the other three SNVs was relatively high in the general population. These data suggested that—among the four SNVs—rs2185379 of PRDM1 was most specific to the long-term recurrence-free survivors without recurrence. This germline missense variant replaces the 220th base, guanine, of PRDM1 (NM_001198.4) with adenine and alters the 74th amino acid, glycine, to serine (NP_001189.2). Because the human PRDM1 is almost identical to mouse prdm1 (eg, NP_031574.2), it seemed that genome editing of the corresponding mouse nucleotide made sense to reproduce this human SNV (Supplementary Figure S1A).
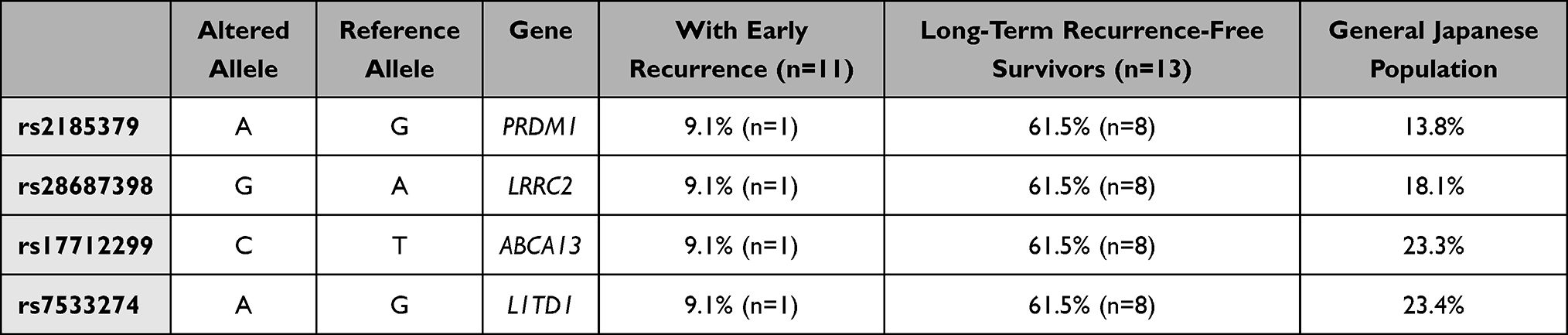 |
Table 2 Representative Single Nucleotide Variants in Exons |
Then, we established knock-in mice with germline heterozygous allele alteration equivalent to human rs2185379 (germline heterozygous rs2185379) by CRISPR/Cas9 without any virus infection. The confirmatory sequencing demonstrated that the corresponding guanine changed to adenine in mouse prdm1 (Supplementary Figure S1B). Next, we crossbred the second-generation mice with germline heterozygous rs2185379 and obtained third and fourth-generation wild type (n=10) and germline heterozygous rs2185379 (n=11) for allogeneic transplant of ID8. The intraperitoneal disseminated tumors were significantly smaller in the germline heterozygous rs2185379 than in the wild type (mean 42.3 g vs 99.2 g, P=0.008, Figure 1). Immunohistochemistry showed that the area of distribution of infiltrating CD8-positive T lymphocytes in high-power fields exceeded one-quarter in 87.5% of the germline heterozygous rs2185379 group and 40.0% of the wild type group (P=0.04, Figure 2). On the other hand, the distribution of tumor-infiltrating B lymphocytes was similar between heterozygous rs2185379 and wild type (P=0.18 for CD4 and no staining of B220 in all specimens, Figure 2).
 |
Figure 1 Intraperitoneal disseminated ID8 tumors were decreased in mice with germline heterozygous PRDM1 rs2185379. The upper bar graph shows the sum of the tumor weights, and data are shown as the mean±SD. The bottom images show representative images of the abdominal cavity in wild type and germline heterozygous rs2185379 mice (white border, representative tumors in the wild type mouse). *Indicates statistical significance (P<0.05). |
 |
Figure 2 T lymphocyte infiltration to allograft ID8 tumors was increased in mice with germline heterozygous PRDM1 rs2185379. (A) The bar graph shows proportions of mice in which the area of distribution of each type of tumor-infiltrating lymphocytes in high-power fields (x100) exceeded 25%. (B) The images show representative immunohistochemical staining of CD8 in wild type and germline heterozygous rs2185379 (black border, lymphocyte infiltration area, x 100). Three mice in which the tumors were too small to evaluate were excluded from the germline heterozygous rs2185379 group. *Indicates statistical significance (P<0.05). Abbreviations: WT, wild type; Hetero, germline heterozygous rs2185379. |
Discussion
To our knowledge, the present study is the first to demonstrate an anticancer role of rs2185379 of PRDM1. Because the allele frequency of rs2185379 is consistently low, regardless of region (approximately 3.55% in the global population8), it is noteworthy that more than 60% of the long-term recurrence-free survivors had this variant. In addition, our experiment suggested that PRDM1 rs2185379 was involved in anticancer T lymphocyte immunity. The previous finding that tumor-infiltrating T lymphocytes can improve the long-term outcomes of patients with advanced ovarian cancer is interesting.9
In terms of mechanisms, previous studies also showed that PRDM1 regulates the differentiation and exhaustion of T lymphocytes in the early phase, and the maintenance of memory T lymphocytes in the late phase of immunological reaction.10 Of these functions, our experiments suggested that PRDM1 rs2185379 could induce the initial differentiation of anticancer T lymphocytes in the early phase because the primary lesions without any treatment were partially decreased in mice with heterozygous rs2185379 in comparison to the wild type. On the other hand, it remains unknown whether PRDM1 rs2185379 can regulate the exhaustion of sensitized T lymphocytes and promote memory T cell differentiation to eliminate micro-residual or recurrent lesions and survive for a long time. To answer these points, we should next find tumor antigens that are targeted by T lymphocytes with rs2185379. It would also be interesting to confirm the correlation between the expressions of those antigens and several known immune checkpoint molecules, including PD-l and PD-L1, to elucidate the mechanism of strong anticancer immunity.
Immunotherapy with immune checkpoint inhibitors (ICIs) has been progressing in both primary treatments11 and recurrent treatments12 for various types of cancer, and a large number of clinical trials with a combination of different types of immunotherapies are progressing. For ovarian cancer patients, the TCGA data suggested that a part of ovarian cancer demonstrated an immunoreactive nature.13 However, the development of immunotherapy for advanced ovarian cancer is considerably limited. One of the reasons may be the low expression of a neoantigen that can serve as a biomarker for ICIs. In a recent clinical trial that investigated the efficacy of pembrolizumab, an anti-PD-1 antibody, in tumor mutational burden (TMB)-high cases, no patients with ovarian cancer were registered.14 These facts suggest that ovarian cancer is immunologically cold and unsuitable for existing strategies. Therefore, we expect that this study will contribute to providing new evidence to support the application of immunotherapy in ovarian cancer. Recently, clinical interest in the combination of ICIs and PARP inhibitors arose, and several trials are presently assessing the efficacy and safety of treatment with chemotherapy plus pembrolizumab and maintenance olaparib (NCT03740165) or treatment with rucaparib and nivolumab as maintenance treatment following response to front-line therapy (NCT03522246).
The long-term recurrence-free survivors in this study had not received any long-term maintenance therapy. If newly diagnosed patients show similar anticancer immunity to long-term recurrence-free survivors with germline rs2185379, we can expect the establishment of highly cost-effective and less harmful primary treatment, for example, by the technical application of iPS cells to generate genetically engineered allogeneic human T lymphocytes.15
Conclusion
The germline heterozygous rs2185379 in PRDM1 is correlated with an excellent prognosis in patients with advanced ovarian cancer. Germline genetic findings may support approaches to treatments for advanced cancer and the establishment of a new treatment strategy.
Data Sharing Statement
The datasets generated during and during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
TM was supported by the Takeda Science Foundation (Japan), SEI Group CSR Foundation (Japan), Shiro Nozawa Memorial Research Grant (Japan), and Women’s Health Integrative Network of Doctors (Japan).
Disclosure
Dr Yutaka Hatanaka reports personal fees from AstraZeneca K.K, Novartis Pharma K.K, Eli Lilly Japan K.K.; grants from Roche Diagnostics K.K., Sysmex Corp., Thermo Fisher Scientific K.K., outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Piccart MJ, Floquet A, Scarfone G., et al. Intraperitoneal cisplatin versus no further treatment: 8-year results of EORTC 55875, a randomized Phase III study in ovarian cancer patients with a pathologically complete remission after platinum-based intravenous chemotherapy. Int J Gynecol Cancer. 2003;13(Suppl 2):196–203. doi:10.1136/ijgc-00009577-200311001-00012
2. Sorbe B; Swedish-Norgewian Ovarian Cancer Study G. Consolidation treatment of advanced (FIGO stage III) ovarian carcinoma in complete surgical remission after induction chemotherapy: a randomized, controlled, clinical trial comparing whole abdominal radiotherapy, chemotherapy, and no further treatment. Int J Gynecol Cancer. 2003;13(3):278–286. doi:10.1046/j.1525-1438.2003.13193.x
3. Nicoletto MO, Tumolo S, Sorio R, et al. Long-term survival in a randomized study of nonplatinum therapy versus platinum in advanced epithelial ovarian cancer. Int J Gynecol Cancer. 2007;17(5):986–992. doi:10.1111/j.1525-1438.2007.00862.x
4. Kim SR, Kotsopoulos J, Sun P, et al. The impacts of neoadjuvant chemotherapy and of cytoreductive surgery on 10-year survival from advanced ovarian cancer. Int J Gynaecol Obstet. 2021;153(3):417–423. doi:10.1002/ijgo.13542
5. Berek JS, Kehoe ST, Kumar L, Friedlander M. Cancer of the ovary, fallopian tube, and peritoneum. Int J Gynaecol Obstet. 2018;143(Suppl 2):59–78. doi:10.1002/ijgo.12614
6. Jinam TA, Kawai Y, Saitou N. Modern human DNA analyses with special reference to the inner dual-structure model of Yaponesian. Anthropological Science. 2021;129(1):3–11. doi:10.1537/ase.201217
7. Kawai Y, Mimori T, Kojima K, et al. Japonica array: improved genotype imputation by designing a population-specific SNP array with 1070 Japanese individuals. J Hum Genet. 2015;60(10):581–587. doi:10.1038/jhg.2015.68
8. Phan Y, Jin H, Zhang W, et al; ALFA: Allele Frequency Aggregator. National Center for Biotechnology Information, U.S. National Library of Medicine. Available from: www.ncbi.nlm.nih.gov/snp/docs/gsr/alfa/.
9. Zhang L, Conejo-Garcia JR, Katsaros D, et al. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N Engl J Med. 2003;348(3):203–213. doi:10.1056/NEJMoa020177
10. Ciucci T, Vacchio MS, Chen T, et al. Dependence on Bcl6 and Blimp1 drive distinct differentiation of murine memory and follicular helper CD4+ T cells. J Exp Med. 2022;219(1). doi:10.1084/jem.20202343.
11. Kelly RJ, Ajani JA, Kuzdzal J, et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N Engl J Med. 2021;384(13):1191–1203. doi:10.1056/NEJMoa2032125
12. Makker V, Taylor MH, Aghajanian C, et al. Lenvatinib Plus Pembrolizumab in Patients With Advanced Endometrial Cancer. J Clin Oncol. 2020;38(26):2981–2992. doi:10.1200/JCO.19.02627
13. Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian carcinoma. Nature. 2011;474(7353):609–615. doi:10.1038/nature10166
14. Marabelle A, Fakih M, Lopez J, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, Phase 2 KEYNOTE-158 study. Lancet Oncol. 2020;21(10):1353–1365. doi:10.1016/S1470-2045(20)30445-9
15. Iriguchi S, Yasui Y, Kawai Y, et al. A clinically applicable and scalable method to regenerate T-cells from iPSCs for off-the-shelf T-cell immunotherapy. Nat Commun. 2021;12(1):430. doi:10.1038/s41467-020-20658-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.