Back to Journals » OncoTargets and Therapy » Volume 8
Genetic polymorphisms of PAI-1 and PAR-1 are associated with acute normal tissue toxicity in Chinese rectal cancer patients treated with pelvic radiotherapy
Authors Zhang H ![]() , Wang M, Shi T, Shen L, Zhu J, Sun M, Deng Y, Liang L, Li G, Wu Y, Fan M, Wei Q, Zhang Z
, Wang M, Shi T, Shen L, Zhu J, Sun M, Deng Y, Liang L, Li G, Wu Y, Fan M, Wei Q, Zhang Z
Received 28 February 2015
Accepted for publication 23 April 2015
Published 27 August 2015 Volume 2015:8 Pages 2291—2301
DOI https://doi.org/10.2147/OTT.S83723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Hui Zhang,1,5,* Mengyun Wang,2,5,* Tingyan Shi,2,5 Lijun Shen,1,5 Ji Zhu,1,5 Menghong Sun,3,5 Yun Deng,1,5 Liping Liang,1,5 Guichao Li,1,5 Yongxin Wu,1,5 Ming Fan,1,5 Qingyi Wei,2,4 Zhen Zhang1,5
1Department of Radiation Oncology, Fudan University Shanghai Cancer Center, Shanghai, People’s Republic of China; 2Cancer Institute, Fudan University Shanghai Cancer Center, Shanghai, People’s Republic of China; 3Department of Pathology, Fudan University Shanghai Cancer Center, Shanghai, People’s Republic of China; 4Duke Cancer Institute, Duke University Medical Center, Durham, NC, USA; 5Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Abstract: Plasminogen activator inhibitor type 1 (PAI-1) and protease-activated receptor-1 (PAR-1) are crucial mediators of the intestinal microenvironment and are involved in radiation-induced acute and chronic injury. To evaluate whether genetic polymorphisms of PAI-1 and PAR-1 were predictors of radiation-induced injury in patients with rectal cancer, we retrospectively evaluated 356 rectal cancer patients who had received pelvic radiotherapy and analyzed the association of genetic polymorphisms of PAI-1 and PAR-1 with acute toxicities after radiotherapy. Acute adverse events were scored, including dermatitis, fecal incontinence (anal toxicity), hematological toxicity, diarrhea, and vomiting. The patients were grouped into grade ≥2 and grade 0–1 toxicity groups to analyze the acute toxicities. Genotyping of six single nucleotide polymorphisms (SNPs) of PAI-1 and PAR-1 was performed using TaqMan assays. A logistic regression model was used to estimate the odds ratios and 95% confidence intervals. Of the 356 individuals, 264 (72.5%) had grade ≥2 total toxicities; within this group, there were 65 (18.3%) individuals who reached grade ≥3 toxicities. There were 19.5% (69/354) and 36.9% (130/352) patients that developed grade ≥2 toxicities for diarrhea and fecal incontinence, respectively. The variant genotype GG of rs1050955 in PAI-1 was found to be negatively associated with the risk of diarrhea and incontinence (P<0.05), whereas the AG and GG genotypes of rs2227631 in PAI-1 were associated with an increased risk of incontinence. The CT genotype of PAR-1 rs32934 was associated with an increased risk of total toxicity compared with the CC allele. Our results demonstrated that SNPs in the PAI-1 and PAR-1 genes were associated with acute injury in rectal cancer patients treated with pelvic irradiation. These SNPs may be useful biomarkers for predicting acute radiotoxicity in patients with rectal cancer if validated in future studies.
Keywords: rectal cancer, pelvic radiotherapy, polymorphism, acute toxicity, biomarker
Introduction
Colorectal cancer is the third most frequently diagnosed cancer in males and the second in females worldwide, with over 1.2 million new cases each year. The estimated deaths ranked fourth in males and the third in females, with over 0.6 million deaths due to colorectal cancer reported in 2008.1 Approximately half of colorectal cancers occur in the rectum, most of which are already advanced at the time of diagnosis. The treatment for rectal cancer varies according to the disease stage, and radiotherapy is a major modality. Approximately 50% of patients in early stages (stage I and stage II for tumor, lymph node, metastasis [TNM] staging) received chemotherapy alone or combined with radiotherapy; approximately 75% of patients in advanced stages (stage III and IV) were given chemotherapy or radiotherapy pre- or postsurgery in 2008 according to the National Cancer Database and the Surveillance, Epidemiology, and End Results (SEER)–Medicare linked database.2 Studies have shown that radiotherapy reduced the local recurrence rate and possibly improved the survival of rectal cancer patients, but with increased radiation-related morbidity, especially as a result of damage to the surrounding normal tissues.3–5 The injuries to normal tissue impair the patient’s quality of life and may even be life threatening.
Therefore, a major challenge has been how to decrease the damage induced by radiotherapy to the surrounding normal tissue, which is mainly observed as radiation-related intestinal injury, including acute inflammation and late fibrosis. Among the acute side effects, mucositis, vomiting, diarrhea, pain, tenesmus, bleeding, and hematological dysfunction were frequently reported.6,7 In some cases, acute toxicities occurring during or immediately after radiotherapy result in dose reduction or the complete termination of therapy. Furthermore, severe acute toxicity decreases the quality of life of rectal cancer patients and is coupled with chronic complications including irreversible fibrosis and fistulae. In addition, the toxicities vary substantially among patients, making it difficult to predict which toxicity will develop and which patients are most at risk. There is therefore an urgent need to investigate the molecular biomarkers that can identify patients who may develop severe side effects prior to radiotherapy so that therapeutic strategies can be tailored and optimized to maximize the treatment benefit and minimize the toxicities. Currently, there are a few markers for predicting these toxicities, most of which are based on the histopathological and radiophysical parameters, but these have shown limited efficacy.8,9 Furthermore, most investigations have focused on late radiation-induced injury, with fewer studies having investigated early toxicity.10,11 Therefore, we wanted to perform studies based on our interest in the early injury to normal tissue and to identify additional molecular markers for predicting acute radiation injury in rectal cancer patients.
The exact mechanisms underlying the radiation-induced intestinal injury are not fully understood. Pathologically, early radiation enteropathy is characterized by epithelial barrier breakdown and mucosal inflammation, resulting from the complex interplay among pathophysiological processes, including inflammation, epithelial regeneration, tissue remodeling, and collagen deposition, as well as the activation of the coagulation system and endothelial dysfunction.6,12,13 This complex and integrated response involves a large number of molecular pathways that can be activated by pro- or anti-inflammatory cytokines. Among these factors, transforming growth factor (TGF)-β is considered to be a key cytokine involved in radiation-induced intestinal damage.14 Radiation activates TGF-β via the generation of reactive oxygen species, and the sustained overexpression of TGF-β has been found in irradiated intestinal tissue.15 TGF-β regulates the expression of several molecules that contribute to acute and late radiation damage, among which are plasminogen activator (PA) inhibitor type 1 (PAI-1) and protease-activated receptor-1 (PAR-1). PAI-1 is a critical mediator that triggers pathways leading to acute and late normal tissue lesions after radiation.16 PAI-1, belonging to a family of serine protease inhibitors, has been widely studied in fibrotic diseases, and its role in radiation-induced acute side effects was recently observed in PAI-1 knockout mice, in which a genetic deficiency of PAI-1 was associated with decreased acute intestinal injury.17 In addition, the PAI-1 inhibitor limited the radiation-induced increase of CTGF, COL1A2, and TGF-β.18 PAR-1 is the most important member of the PAR family, which plays a central role in blood clotting, and it is also involved in radiation-induced intestinal injury.19 PAR-1 plays an important role in the tumor microenvironment through regulating monocyte migration and fibroblast chemokine production.20 PAR-1 can modulate the expression of PAI-1; in addition, both PAI-1 and PAR-1 interact with inflammatory molecules and profibrotic factors. Therefore, we hypothesized that PAI-1 and PAR-1 are important factors involved in radiation-induced injury in rectal cancer and that different expression levels or genetic polymorphisms of PAI-1 and PAR-1 may play a role in the individual difference in toxicities after radiation.
During the last 10 years, nearly 100 studies have addressed the possible associations between genetic variations and the risk of normal tissue toxicity after radiotherapy. It has been speculated that genetic polymorphisms in genes encoding drug- or radiation-related responses may influence an individuals’ response to chemoradiotherapy.21,22 The present study was designed to determine whether the different genotypes of PAI-1 and PAR-1 are predictive of acute adverse events (AEs) in patients with rectal cancer treated with pelvic radiotherapy with or without chemoradiotherapy.
Materials and methods
Study subjects
In total, there were 398 rectal cancer patients who received pelvic radiotherapy at the Fudan University Shanghai Cancer Center (Shanghai, People’s Republic of China) between January 2012 and October 2013. However, there were 42 patients whose blood samples were not collected. Thus, this study included 356 rectal cancer patients. All of the patients were histopathologically diagnosed as having rectal adenocarcinoma, and other histological types and all metastases to the rectum were excluded. All patients had a Karnofsky Performance Status score of ≥70 at the time when they received radiotherapy, and all had adequate renal and hepatic function. All of the patients were treated with pelvic radiotherapy preoperatively, postoperatively, or after pelvic recurrence, but without previous pelvic radiotherapy. A pretreatment evaluation was performed within 2 weeks before the initiation of chemoradiation, including a physical examination, blood counts, hepatic and rectal examinations, colonoscopy and biopsy, computed tomography of the thorax and abdomen, and magnetic resonance imaging. All patients were clinically staged based on the American Joint Committee on Cancer (AJCC) seventh version manual.23 Written informed consent was provided by each participant for inclusion in the study. This study was approved by the Institutional Review Board of Fudan University Shanghai Cancer Center. Detailed descriptions of the clinical and treatment characteristics of the patients are presented in Tables 1 and 2.
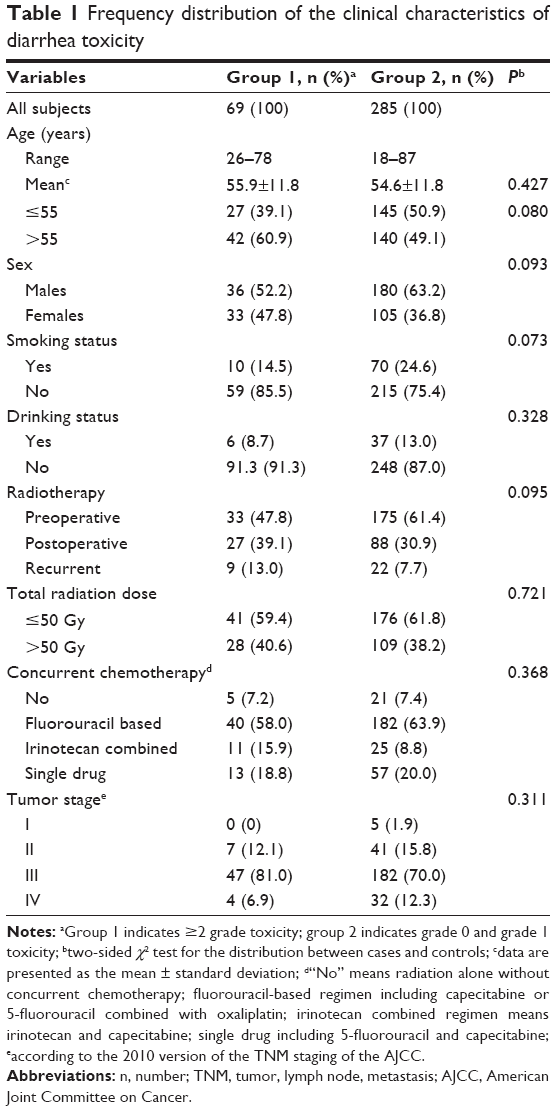 | Table 1 Frequency distribution of the clinical characteristics of diarrhea toxicity |
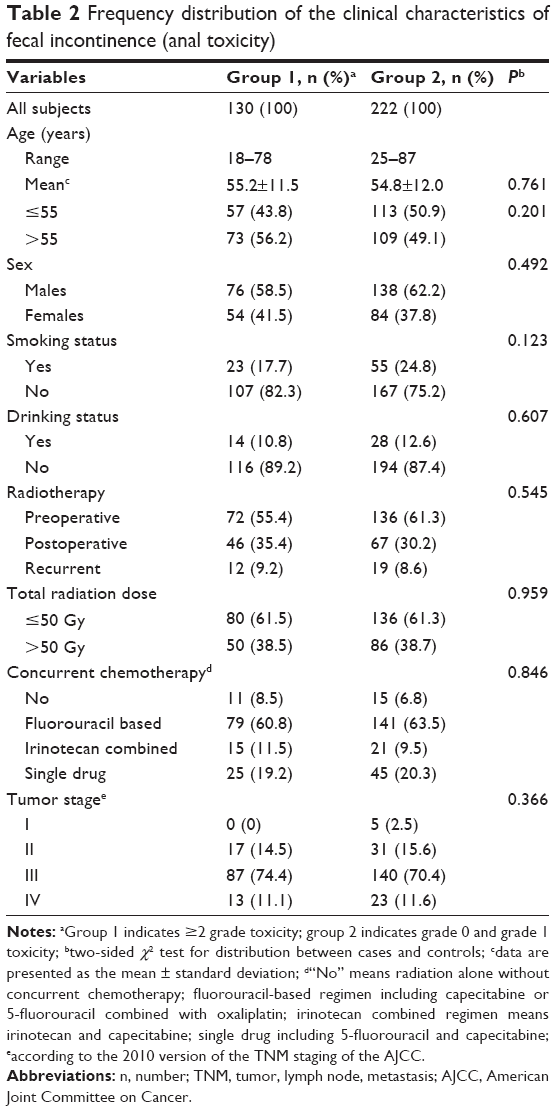 | Table 2 Frequency distribution of the clinical characteristics of fecal incontinence (anal toxicity) |
Treatment
All 356 patients received pelvic irradiation with intensity modulated radiation therapy (IMRT) using 6 MV X-rays from linear accelerators (Elekta, Stockholm, Sweden; Varian Medical Systems, Palo Alto, CA, USA). The details of delivering IMRT are described in our previously published study.24 All patients were immobilized in the prone position using a belly board and underwent planning computed tomography in the treatment position. The image data were transferred to the PINNACLE planning system (Philips Radiation Oncology Systems, Milpitas, CA, USA), and the IMRT plans were generated using the inverse planning module. The position and isocenter of each patient were verified on electronic portal imaging device films. The median total dose was 50 Gy (generally in the range of 45–54 Gy; eight patients received less than 45 Gy because of severe toxicity) with conventional fractionation, as daily fractions of 1.8–2.0 Gy, from Monday to Friday. The concurrent chemotherapy was either based on single 5-fluorouracil (5-FU)/capecitabine, or on a combination with oxaliplatin or irinotecan.
Monotherapeutic capecitabine was administered at a dose of 825 mg/m2 twice a day (bid), per os (po) 5 days per week during the course of irradiation. In the capecitabine + oxaliplatin group, patients were administered oxaliplatin at a dose of 50 mg/m2 by 2-hour intravenous infusion once a week, and capecitabine was administered po at 625 mg/m2 twice 5 days per week. In the capecitabine + irinotecan group, irinotecan was administered at 50–70 mg/m2 by intravenous infusion once a week, and capecitabine was administered po at 625 mg/m2 twice a day, 5 days per week. The administered dose of 5-FU was 1,000 mg/m2.
The total mesorectal excision (TME) is a standard surgical procedure in rectal cancer. All of the patients, who received surgery in our center, were treated by the TME procedure. During the surgery, there were no radiation-related surgical complications observed in the preoperative radiotherapy patients.
Toxicity criteria
Acute AEs, including gastrointestinal toxicities (vomiting, diarrhea, and incontinence), dermatitis, and hematologic toxicities, were evaluated weekly during the treatment using the Common Terminology Criteria (CTC) toxicity criteria version 3.0 scale according to the complaints of the patients and the recordings by one radiotherapist.25 Grade 0 indicated that there were no AEs, grade 1 indicated a mild AE, and grade 5 indicated that the patient died from toxicity-related AE, which did not happen in the present study. The patients were separated into two groups according to the CTC version 3.0 scores; patients who experienced grade ≥2 toxicities were categorized as group 1, and those with scores of 0–1 were categorized into group 2. Grade 2 was set as a cutoff, because the development of grade 2 toxicity was considered to impair the patient’s quality of life. The grade of total toxicity indicated the highest toxicity grade among the hematological toxicity, vomiting, diarrhea, fecal incontinence (anal reaction), and dermatitis.
SNP selection
We searched the National Center for Biotechnology Information dbSNP database (http://www.ncbi.nlm.nih.gov/snp) and SNPinfo (http://snpinfo.niehs.nih.gov/) for common (minor allele frequency ≥5%) and potentially functional single nucleotide polymorphisms (SNPs) in the PAI-1 and PAR-1 genes based on three criteria: 1) the SNP was located in a regulatory region, such as the 5′ end, the 3′ end, the 5′ untranslated region (UTR), or the 3′UTR; 2) there is a minor allele frequency of ≥5% in Chinese Han Beijing descendants; and 3) this frequency potentially affects these genes’ functions, such as affecting transcription factor binding site (TFBS) activity or the micro (mi)RNA binding site activity. Then, the linkage disequilibrium among several selected SNPs in a gene was evaluated pairwise using the Haploview software program (http://www.broadinstitute.org/scientific-community/science/programs/medical-and-population-genetics/haploview/haploview), with only one of the polymorphisms among several SNPs with a high linkage disequilibrium (at a stringency of r2=0.80) being chosen (Figure 1C). As a result, seven SNPs (rs1801719, rs2227744, and rs32934 in PAR-1; rs1050955, rs2227631, rs1050813, and rs11178 in PAI-1) were selected. Because the genotyping failed to use the probe for rs1050813, the final analysis included only six SNPs. The SNP rs1801719 C/T in the 3′UTR of PAR-1 is predicted to affect the expression of miRNA, rs2227744 A/G and rs32934 C/T in the gene located 5′ to PAR-1 may affect the TFBS, rs1050955 A/G and rs11178 C/T in the 3′UTR of PAI-1 may affect miRNA expression, and rs2227631 A/G in the gene located at the 5′ end to PAI-1 can potentially affect the TFBS.
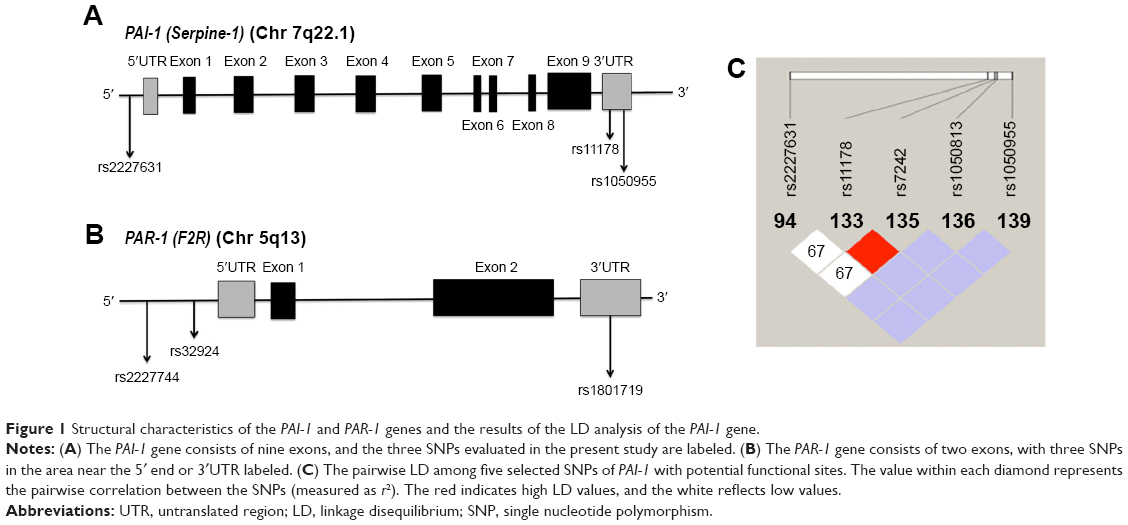 | Figure 1 Structural characteristics of the PAI-1 and PAR-1 genes and the results of the LD analysis of the PAI-1 gene. |
DNA sample preparation and genotyping
To avoid the influence of chemotherapy and radiotherapy on genotyping, the blood samples were collected within 1 week before starting the chemoradiotherapy. Genomic DNA was extracted from the white blood cells from whole blood samples. Blood samples from all patients were collected and processed by the Institutional Tissue Bank at the Shanghai Cancer Center. Genomic DNA was extracted with a Blood DNA extraction kit (PerkinElmer Inc., Waltham, MA, USA) using an automatic nucleic acid extraction system (ChemagicSTAR; Hamilton Robotics ApS, Copenhagen, Denmark). The purity and concentration of the DNA were determined by spectrophotometric measurement of the absorbance at 260 nm and 280 nm by an ultraviolet spectrophotometer (BioTek Instruments, Winooski, VT, USA). The DNA was diluted with ddH2O, and a total of 5 ng DNA was used for genotyping. The TaqMan SNP genotyping assays were ordered from Applied Biosystems/Life Technologies (Thermo Fisher Scientific, Waltham, MA, USA). All of the SNPs were genotyped using the TaqMan real-time polymerase chain reaction method with a 7900HT sequence detector system (Applied Biosystems; Thermo Fisher Scientific). To ensure high genotyping accuracy, strict quality control procedures were implemented, and four duplicate positive controls and four negative controls (ddH2O instead of DNA) were used in each of the 384-well plates, and the results were 100% concordant.
Statistical methods
The SPSS 20.0 software package was used for the statistical data analysis. The chi-squared (χ2) test was used to evaluate the differences in the frequency distributions of the clinical characteristics between group 1 (grade ≥2) and group 2 (grade 0–1), as well as to determine the differences in the frequencies of genotypes between the two groups. Univariate and multivariate logistic regression analyses were used to calculate the crude and adjusted odds ratios (ORs) for the risk of toxicities and the 95% confidence intervals (CIs). Multivariate adjustments were made for age, sex, drinking and smoking status, radiation dose, and concurrent chemotherapy. Student’s t-test was used to compare the differences in the messenger (m)RNA expression levels between the two groups. General linear modeling was used to evaluate the trends in the transcript expression levels by genotypes. A two-sided value of P<0.05 was considered to be statistically significant for all parameters.
Results
Patients’ characteristics
Analyses of 356 histopathologically-confirmed rectal cancer patients who received pelvic radiotherapy were performed for the total toxicity, hematological toxicity, diarrhea, vomiting, fecal incontinence (anal toxicity), and dermatitis. There were no significant differences (P>0.05) in the distributions of age, sex, smoking, drinking, the pattern of radiation, and the use of concomitant chemotherapy between the groups (Tables 1 and 2). More than 50% of the patients were male, over 50% of the patients received radiation before the operation, approximately 30% of patients received radiation postoperatively, and the others received radiotherapy because of local recurrence after surgery without previous pelvic radiation. Over 90% of the patients had received concurrent chemotherapy, with most patients having received two-drug regimens. The single drugs used included 5-FU and capecitabine. FU-based regimens contained capecitabine + oxaliplatin or 5-FU + oxaliplatin. The irinotecan-containing regimen refers to irinotecan + capecitabine. The patients were staged according to the TNM staging of the 2010 AJCC guidelines;23 however, there were 36 patients who could not be staged because of incomplete data.
Associations between the different genotypes and radiation-induced AEs
The influence of the different PAI-1 and PAR-1 genotypes on the occurrence of normal tissue injuries was examined. The crude ORs (95% CI), P-values, and data corrected for age, sex, radiation dose, radiation pattern, smoking, drinking, and the regimens of concurrent chemotherapy were obtained separately in terms of the total toxicity, diarrhea, fecal incontinence hematological toxicity, and dermatitis. There were no significant differences between the patients with different genotypes of the six SNPs in terms of hematological toxicity or dermatitis (data not shown). For total toxicity, positive associations were found only in a recessive model of rs2227631 (adjusted OR=1.995; 95% CI=1.166–3.415; P=0.012 for GG versus AA/AG) and for one variant allele of rs32934 (adjusted OR=1.778; 95% CI=1.034–3.059; P=0.037 for CT versus CC) (data not shown).
The associations were more obvious for diarrhea and fecal incontinence (anal toxicity). An overview of the genotype data for diarrhea is presented in Table 3. For PAI-1 rs1050955, the variant genotypes were protective against severe diarrhea (adjusted OR=0.394, 95% CI=0.181–0.858, P=0.019 for GG versus AA; and adjusted OR=0.476, 95% CI=0.247–0.916, P=0.026 for AG/GG versus AA in a dominant model [the combination of heterozygous and variant homozygous genotypes versus the wild-type genotype]). There were two SNPs that showed associations with incontinence, which were PAI-1 rs2227631 and PAI-1 rs1050955, as listed in Table 4. A positive and significant association was found between PAI-1 rs2227631 and fecal incontinence (adjusted OR=3.172, 95% CI=1.490–6.751, P=0.003 for GG versus AA; and adjusted OR=2.541, 95% CI=1.249–5.170, P=0.010 for AG/GG versus AA), and borderline significance was shown for one variant allele (adjusted OR=2.108, 95% CI=1.001–4.440, P=0.05 for AG versus AA). In a recessive model (the variant homozygous genotypes versus the variant heterozygous genotype combined with the wild-type genotype) for PAI-1 rs2227631, the variant genotypes were associated with an increased risk of fecal incontinence (adjusted OR=1.772; 95% CI=1.126–2.789; P=0.013 for GG versus AA/AG). For PAI-1 rs1050955, a protective and significant association was found with regard to the development of obvious incontinence, indicating a protective effect of this genotype (adjusted OR=0.474; 95% CI=0.248–0.922; P=0.028 for GG versus AA). In both dominant and recessive models for PAI-1 rs1050955, a protective borderline significant association with incontinence was observed (adjusted OR=0.606, 95% CI=0.342–1.075, P=0.087 for AG/GG versus AA in a dominant model, and adjusted OR=0.620, 95% CI=0.383–1.006, P=0.053 in a recessive model).
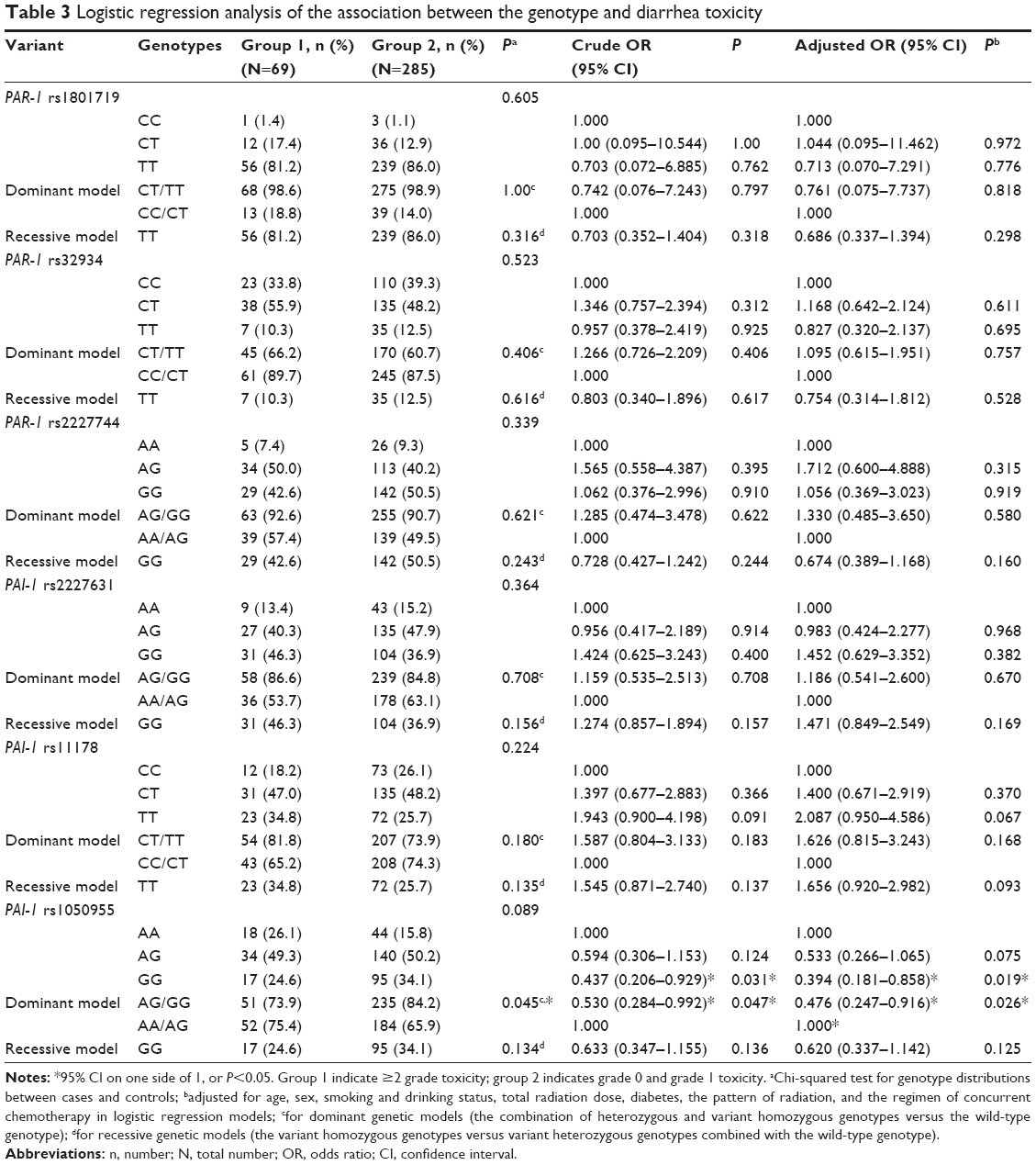 | Table 3 Logistic regression analysis of the association between the genotype and diarrhea toxicity |
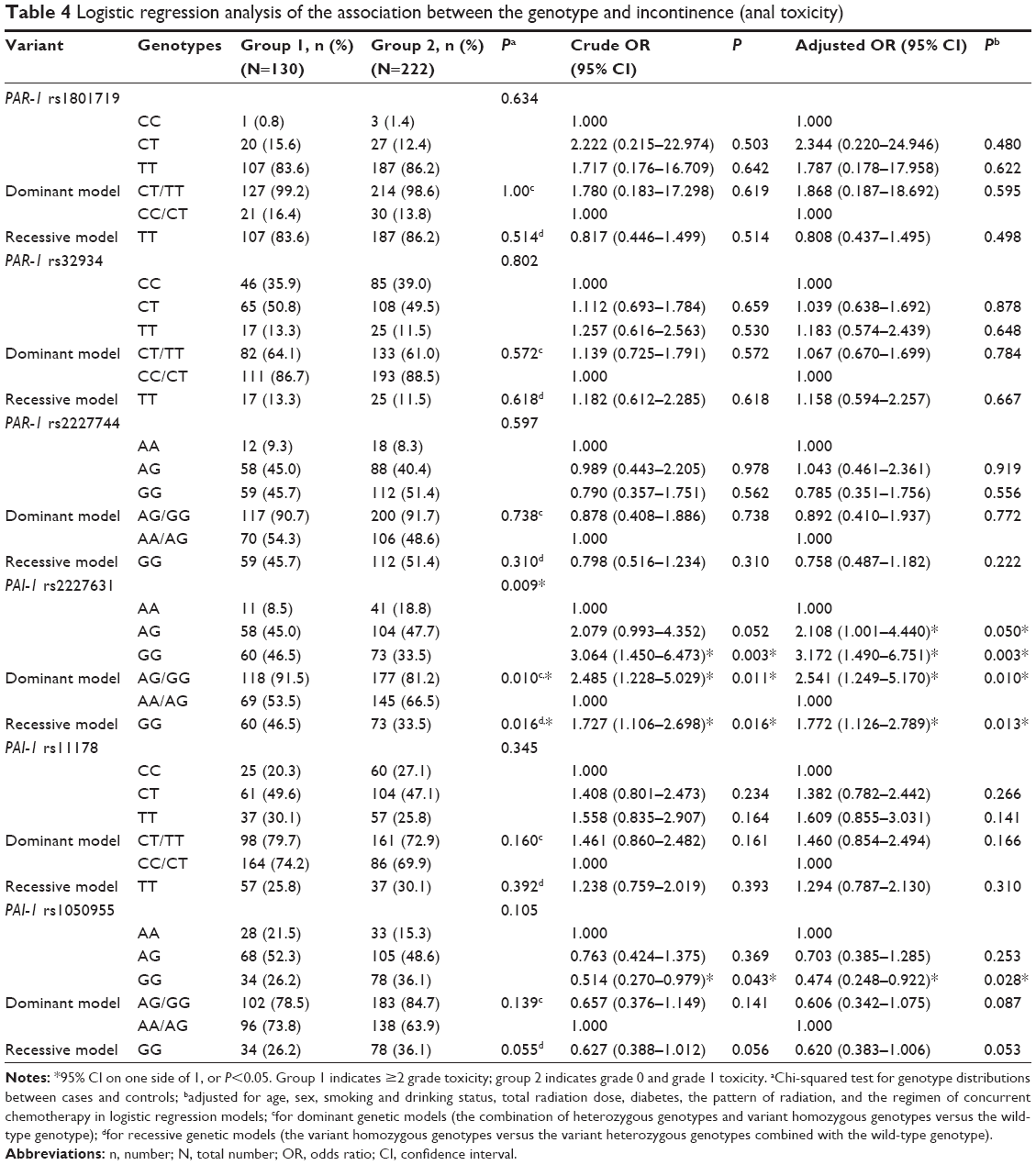 | Table 4 Logistic regression analysis of the association between the genotype and incontinence (anal toxicity) |
Although there were significant results for PAI-1 rs2227631, PAI-1 rs1050955, and PAR-1 rs32934, there were no significant associations of PAI-1 rs11178, PAR-1 rs2227744, or PAR-1 rs1801719 with the risk of severe acute toxicity.
Discussion
Genetic polymorphisms have been extensively investigated for their roles in predicting the chemosensitivity and radiosensitivity of patients. Recent studies have suggested that some polymorphisms in genes related to DNA repair, drug metabolism, cell cycle regulation, and inflammation were associated with the response to radiotherapy or chemoradiotherapy.21,22,26,27 Compared with late radiation-induced injury, there have been fewer published studies on acute injury. In the present study, we investigated the associations of six SNPs in PAI-1 and PAR-1 with radiation-induced acute normal tissue injury in rectal cancer patients treated with pelvic radiotherapy. To the best of our knowledge, this is the first report of an association between SNPs in the PAI-1/PAR-1 genes and the risk of developing severe toxicity in rectal cancer patients treated with radiotherapy.
In the present study, we considered grade ≥2 toxicity as obvious clinical toxicity, while stratifying the patients with grade 0–1 classifications into the control group, because developing grade ≥2 toxicity will strongly influence the patients’ quality of life. Our findings suggest that the SNP rs1050955 and rs2227631 in PAI-1 and rs32924 in PAR-1 are associated with the risk of developing acute injury in patients with rectal cancer receiving pelvic radiation. Thus, following validation in more individuals and/or other populations, such genetic polymorphisms could be useful biomarkers for the susceptibility to radiation-induced toxicity in rectal cancer patients who are being considered for radiotherapy.
PAI-1, as an important inhibitor of PAs and inflammation-related genes, has been mapped to chromosome 7q22, and consists of nine exons of genomic DNA (Figure 1A). The PA system plays a vital role in radiation toxicity. It has been reported that PAI-1 was more highly expressed in cancer cell lines and normal endothelial cells after radiation, and the expression was also increased in the rectal mucosa of mice and humans after radiotherapy.16,28–31 These findings suggested that PAI-1 might play a critical role in radiation-induced intestinal damage. As a target of TGF-β, PAI-1 has been widely studied in the process of fibrosis in late radiation-induced injury, and radiation-induced acute side effects were also observed using a PAI-1 knockout mouse model.16,17,32
Our present data indicate that PAI-1 variants might have an impact on the risk of acute radiation injury in patients with rectal cancer. It has been demonstrated that rs1050955 is located at an miRNA binding site of the PAI-1 gene, which may regulate the interaction between the miRNA and mRNA, thus potentially resulting in a change in the PAI-1 gene function. It is known that miRNA can genetically regulate target genes by base pairing with target mRNAs at the 3′-UTR, leading to the translational repression. The variant AG or GG genotype in PAI-1 rs1050955 was associated with a decreased risk of diarrhea and incontinence compared with the AA genotype. These results suggest that the variant allele G of rs1050955 in PAI-1 could be a biomarker for predicting the acute effects of radiation-induced normal tissue damage.
Different from PAI-1 rs1050955, PAI-1 rs2227631 showed a positive association with obvious incontinence. The rs2227631 is near the 5′ end of PAI-1 (Figure 1A) and may regulate the function of PAI-1 in a different way from rs1050955, which is located in the 3′-UTR of PAI-1. There are different forms of PAI-1 in the tissues and peripheral blood: latent and active. Only a lower level of active PAI-1 attenuates the toxicity after radiation, and a change in the expression of latent PAI-1 has no effect.18 It is likely that PAI-1 rs2227631 and rs1050955 may modulate different forms of PAI-1, and further functional studies should be performed to determine whether this is the case. The mechanisms underlying the observed PAI-1 induction after radiation remain unclear, but a p53/Smad3-dependent pathway may be one possible mechanism.16,32 Indeed, PAI-1 could be induced by both TGF-β and radiation in a manner dependent on the TP53 gene.32 In addition, PAI-1 can also be strongly induced by lipopolysaccharide, and the biological effects of PAI-1 induced by lipopolysaccharide appear to be mediated by several cytokines, such as tumor necrosis factor-α, interleukin (IL)-1, and IL-6.33 One mechanism underlying how PAI-1 is involved in radiation-induced injury may be that PAI-1 induces a strong antiapoptotic effect on endothelial cells by increasing the expression of antiapoptotic factors, such as Bcl-2 and Bcl-XL.17 Another possible mechanism may be associated with the immune reaction, since PAI-1 is a target of TGF-β, which is an important inflammatory cytokine involved in acute inflammatory reactions and the fibrotic response, including radiation-induced injury.
PAR-1, which can mediate the production of PAI-1, is abundantly expressed throughout the gastrointestinal tract and is strongly overexpressed in radiation-induced intestinal injury.34–38 Endothelial cells, epithelial cells, immune cells, and a variety of stromal cells in the intestine express PAR-1. Evidence from preclinical studies suggests that PAR-1 is involved in the pathogenesis of early and delayed radiation enteropathy.19,37 Pharmacological blockade of PAR-1 was found to reduce early radiation-induced intestinal toxicity.39 PAR-1-mediated responses include increase vascular permeability, the release of vasoactive mediators, the expression of adhesion molecules, and the production of proinflammatory cytokines. The activation of PAR-1 in the intestine induces epithelial apoptosis and a loss of barrier function.40
Our data provide evidence that the CT genotype in PAR-1 rs32934 is associated with an increased risk of total toxicity after radiation. However, its significance was not found when the separate toxicities (anal, hematological, etc) were analyzed. The rs32934 SNP is near the 5′ end of the PAR-1 gene (Figure 1B) and has a potential function as a TFBS, which may affect the transcription of PAR-1. Higher expression of PAR-1 increased the risk of radiation toxicity, and blockade of PAR-1 ameliorated early intestinal toxicity in a mouse model.19 PAR-1-mediated radiation toxicity may occur through a direct increase in the vascular permeability and modulation of cell apoptosis, including changes in endothelial cells, epithelial cells, fibroblasts, and tumor cells, and indirectly via increases in the release of active molecules, such as vasoactive mediators, adhesion molecules, and proinflammatory cytokines.37
A limitation of the present study is that only potentially functional SNPs were assessed in the analysis. Therefore, we might have overlooked SNPs, such as those in introns, which may also be associated with the risk of acute injury after radiotherapy. Introns constitute a large part of a gene, and the number of intronic SNPs is much higher than that of potentially functional SNPs, so analyzing all of the intronic SNPs is daunting work and may need to be investigated in the future following the further development of high-output technologies. The current applications of next-generation sequencing and genome-wide association studies present a comprehensive and powerful method for screening and testing new SNPs, respectively. Although genome-wide association studies have been proven to be a powerful tool to identify new loci that may affect radiosensitivity, they require a large sample size, and the identified hits must be further validated.
Another feature of the present study that could have influenced the results is the Chinese ethnicity of our study subjects. Many of the SNPs reported in Caucasian populations or Japanese subjects are not consistent with those of Chinese populations.41,42 Our findings may support the value of these SNPs in assessing the risk of radiation-induced normal tissue injury in Chinese subjects, but these findings require further validation in additional studies and/or by other investigative teams in additional patients.
Conclusion
In conclusion, our results demonstrated that SNPs in PAI-1 and PAR-1 are associated with acute injury in rectal cancer patients who received pelvic radiation. In particular, rs2227631 and rs1050955 in PAI-1 were obviously associated with diarrhea and fecal incontinence. Once validated, these SNPs may be useful biomarkers for acute toxicity in patients with rectal cancer and may be useful for identifying patients who may develop severe side effects prior to their receiving radiotherapy so that the therapeutic strategies can be individually tailored to monitor, treat, or avoid toxicity. PAI-1 and PAR-1 may represent therapeutic targets to prevent or reduce the side effects of pelvic radiotherapy. Further experiments are necessary to explore the molecular mechanisms involved in radiation-induced acute injury in patients with rectal cancer.
Acknowledgments
This study was supported by a grant from the National Natural Science Foundation of China (grant number 81372432). We would like to thank Menghong Sun of Fudan University Shanghai Cancer Center for managing the blood samples, Fei Ding of Fudan University Shanghai Cancer Center for his assistance with DNA extraction, and Hua Sheng and Shan He of Fudan University Shanghai Cancer Center for helping to record the toxicities.
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | ||
Siegel R, DeSantis C, Virgo K, et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. 2012;62(4):220–241. | ||
Zhu J, Lian P, Liu F, et al. Phase II trial of first-line chemoradiotherapy with intensity-modulated radiation therapy followed by chemotherapy for synchronous unresectable distant metastases rectal adenocarcinoma. Radiat Oncol. 2013;8:10. | ||
Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;30(16):1926–1933. | ||
Rödel C, Liersch T, Becker H, et al; German Rectal Cancer Study Group. Preoperative chemoradiotherapy and postoperative chemotherapy with fluorouracil and oxaliplatin versus fluorouracil alone in locally advanced rectal cancer: initial results of the German CAO/ARO/AIO-04 randomised phase 3 trial. Lancet Oncol. 2012;13(7):679–687. | ||
Shadad AK, Sullivan FJ, Martin JD, Egan LJ. Gastrointestinal radiation injury: symptoms, risk factors and mechanisms. World J Gastroenterol. 2013;19(2):185–198. | ||
Andreyev J. Gastrointestinal symptoms after pelvic radiotherapy: a new understanding to improve management of symptomatic patients. Lancet Oncol. 2007;8(11):1007–1017. | ||
Hovdenak N, Fajardo LF, Hauer-Jensen M. Acute radiation proctitis: a sequential clinicopathologic study during pelvic radiotherapy. Int J Radiat Oncol Biol Phys. 2000;48(4):1111–1117. | ||
Doyen J, Benezery K, Follana P, et al. Predictive factors for early and late local toxicities in anal cancer treated by radiotherapy in combination with or without chemotherapy. Dis Colon Rectum. 2013;56(10):1125–1133. | ||
Vozenin-Brotons MC, Milliat F, Linard C, et al. Gene expression profile in human late radiation enteritis obtained by high-density cDNA array hybridization. Radiat Res. 2004;161(3):299–311. | ||
Strup-Perrot C, Mathé D, Linard C, et al. Global gene expression profiles reveal an increase in mRNA levels of collagens, MMPs, and TIMPs in late radiation enteritis. Am J Physiol Gastrointest Liver Physiol. 2004;287(4):G875–G885. | ||
Ong ZY, Gibson RJ, Bowen JM, et al. Pro-inflammatory cytokines play a key role in the development of radiotherapy-induced gastrointestinal mucositis. Radiat Oncol. 2010;5:22. | ||
François A, Milliat F, Guipaud O, Benderitter M. Inflammation and immunity in radiation damage to the gut mucosa. Biomed Res Int. 2013;2013:123241. | ||
Hneino M, Francois A, Buard V, et al. The TGF-β/Smad repressor TG-interacting factor 1 (TGIF1) plays a role in radiation-induced intestinal injury independently of a Smad signaling pathway. PLoS One. 2012;7(5):e35672. | ||
Wang J, Zheng H, Sung CC, Richter KK, Hauer-Jensen M. Cellular sources of transforming growth factor-beta isoforms in early and chronic radiation enteropathy. Am J Pathol. 1998;153(5):1531–1540. | ||
Milliat F, Sabourin JC, Tarlet G, et al. Essential role of plasminogen activator inhibitor type-1 in radiation enteropathy. Am J Pathol. 2008;172(3):691–701. | ||
Abderrahmani R, François A, Buard V, et al. PAI-1-dependent endothelial cell death determines severity of radiation-induced intestinal injury. PLoS One. 2012;7(4):e35740. | ||
Abderrahmani R, François A, Buard V, et al. Effects of pharmacological inhibition and genetic deficiency of plasminogen activator inhibitor-1 in radiation-induced intestinal injury. Int J Radiat Oncol Biol Phys. 2009;74(3):942–948. | ||
Wang J, Kulkarni A, Chintala M, Fink LM, Hauer-Jensen M. Inhibition of protease-activated receptor 1 ameliorates intestinal radiation mucositis in a preclinical rat model. Int J Radiat Oncol Biol Phys. 2013;85(1):208–214. | ||
Queiroz KC, Shi K, Duitman J, et al. Protease-activated receptor-1 drives pancreatic cancer progression and chemoresistance. Int J Cancer. 2014;135(10):2294–2304. | ||
Andreassen CN, Alsner J, Overgaard M, Overgaard J. Prediction of normal tissue radiosensitivity from polymorphisms in candidate genes. Radiother Oncol. 2003;69(2):127–135. | ||
Parliament MB, Murray D. Single nucleotide polymorphisms of DNA repair genes as predictors of radioresponse. Semin Radiat Oncol. 2010;20(4):232–240. | ||
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. | ||
Zhu J, Liu F, Gu W, et al. Concomitant boost IMRT-based neoadjuvant chemoradiotherapy for clinical stage II/III rectal adenocarcinoma: results of a phase II study. Radiat Oncol. 2014;9:70. | ||
Trotti A, Colevas AD, Setser A, et al. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol. 2003;13(3):176–181. | ||
Duldulao MP, Lee W, Nelson RA, et al. Gene polymorphisms predict toxicity to neoadjuvant therapy in patients with rectal cancer. Cancer. 2013;119(5):1106–1112. | ||
Schirmer MA, Mergler CP, Rave-Fränk M, et al. Acute toxicity of radiochemotherapy in rectal cancer patients: a risk particularly for carriers of the TGFB1 Pro25 variant. Int J Radiat Oncol Biol Phys. 2012;83(1):149–157. | ||
Artman T, Schilling D, Gnann J, Molls M, Multhoff G, Bayer C. Irradiation-induced regulation of plasminogen activator inhibitor type-1 and vascular endothelial growth factor in six human squamous cell carcinoma lines of the head and neck. Int J Radiat Oncol Biol Phys. 2010;76(2):574–582. | ||
Scharpfenecker M, Kruse JJ, Sprong D, Russell NS, Ten Dijke P, Stewart FA. Ionizing radiation shifts the PAI-1/ID-1 balance and activates notch signaling in endothelial cells. Int J Radiat Oncol Biol Phys. 2009;73(2):506–513. | ||
Bayer C, Schilling D, Hoetzel J, et al. PAI-1 levels predict response to fractionated irradiation in 10 human squamous cell carcinoma lines of the head and neck. Radiother Oncol. 2008;86(3):361–368. | ||
Angenete E, Langenskiöld M, Palmgren I, Falk P, Oresland T, Ivarsson ML. uPA and PAI-1 in rectal cancer – relationship to radiotherapy and clinical outcome. J Surg Res. 2009;153(1):46–53. | ||
Niemantsverdriet M, de Jong E, Langendijk JA, Kampinga HH, Coppes RP. Synergistic induction of profibrotic PAI-1 by TGF-β and radiation depends on p53. Radiother Oncol. 2010;97(1):33–35. | ||
Fearns C, Loskutoff DJ. Induction of plasminogen activator inhibitor 1 gene expression in murine liver by lipopolysaccharide. Cellular localization and role of endogenous tumor necrosis factor-alpha. Am J Pathol. 1997;150(2):579–590. | ||
Belling F, Ribeiro A, Wörnle M, et al. PAR-1 mediates the thrombin-induced mesothelial cell overproduction of VEGF and PAI-1. Int J Artif Organs. 2013;36(2):97–104. | ||
Nylander M, Osman A, Ramström S, Aklint E, Larsson A, Lindahl TL. The role of thrombin receptors PAR1 and PAR4 for PAI-1 storage, synthesis and secretion by human platelets. Thromb Res. 2012;129(4):e51–e58. | ||
Wang J, Zheng H, Ou X, Fink LM, Hauer-Jensen M. Deficiency of microvascular thrombomodulin and up-regulation of protease-activated receptor-1 in irradiated rat intestine: possible link between endothelial dysfunction and chronic radiation fibrosis. Am J Pathol. 2002;160(6):2063–2072. | ||
Flynn AN, Buret AG. Proteinase-activated receptor 1 (PAR-1) and cell apoptosis. Apoptosis. 2004;9(6):729–737. | ||
Vergnolle N. Clinical relevance of proteinase activated receptors (pars) in the gut. Gut. 2005;54(6):867–874. | ||
Vergnolle N, Hollenberg MD, Wallace JL. Pro- and anti-inflammatory actions of thrombin: a distinct role for proteinase-activated receptor-1 (PAR1). Br J Pharmacol. 1999;126(5):1262–1268. | ||
Chin AC, Vergnolle N, MacNaughton WK, Wallace JL, Hollenberg MD, Buret AG. Proteinase-activated receptor 1 activation induces epithelial apoptosis and increases intestinal permeability. Proc Natl Acad Sci U S A. 2003;100(19):11104–11109. | ||
Takahashi H, Wilkinson GR, Caraco Y, et al. Population differences in S-warfarin metabolism between CYP2C9 genotype-matched Caucasian and Japanese patients. Clin Pharmacol Ther. 2003;73(3):253–263. | ||
Kullo IJ, Ding K. Patterns of population differentiation of candidate genes for cardiovascular disease. BMC Genet. 2007;8:48. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.