Back to Journals » International Medical Case Reports Journal » Volume 15
Generalized Lesions of Kyrle’s Disease: A Rare Case
Authors Dharmadji HP, Firdaus CP ![]() , Sugiri U
, Sugiri U ![]() , Sutedja EK
, Sutedja EK ![]() , Achdiat PA
, Achdiat PA ![]() , Tsaqilah L
, Tsaqilah L ![]() , Gunawan H
, Gunawan H ![]()
Received 14 January 2022
Accepted for publication 18 March 2022
Published 12 April 2022 Volume 2022:15 Pages 187—191
DOI https://doi.org/10.2147/IMCRJ.S358523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Hartati Purbo Dharmadji, Chaerani Pratiwi Firdaus, Unwati Sugiri, Eva Krishna Sutedja, Pati Aji Achdiat, Laila Tsaqilah, Hendra Gunawan
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Hartati Purbo Dharmadji, Department of Dermatology and Venereology, Faculty of Medicine Universitas Padjadjaran - Dr. Hasan Sadikin General Hospital, Jl. Pasteur No. 38, Bandung, West Java, 40161, Indonesia, Tel +62222032426 ext. 3449, Fax +62222032426, Email [email protected]
Abstract: Kyrle’s disease (KD) is a rare type of acquired perforating dermatosis (APD) associated with various systemic diseases, particularly chronic kidney disease and diabetes mellitus (DM). It most commonly occurs at the lower extremities. Generalized lesions of KD are rare. We report a case of generalized KD in a 29-year-old woman with chronic kidney disease and DM. Physical examination revealed multiple hyperkeratotic and hyperpigmented papules, plaques, and nodules with central umbilication and keratotic plugs on almost all parts of the body. Histopathological examination showed keratinized epithelial layer with acanthosis and hyperkeratosis, invagination with the formation of keratin plugs, and basophilic cell debris accompanied by parakeratosis and abnormal keratinization of epithelial cells. These histopathological findings fulfilled the Constantine and Carter criteria for KD. This condition is characterized clinically by umbilicated, round, erythematous or hyperpigmented papules and nodules with central crusts or keratotic plug, predominantly involving the extensor surfaces of the extremities and the trunk. Although uncommon, it may also involve the face or the scalp. Nevertheless, generalized lesions involving faces are rarely found in KD.
Keywords: acquired perforating dermatosis, chronic kidney disease, diabetes mellitus
Introduction
Kyrle’s disease (KD) is a rare variant of acquired perforating dermatosis (APD),1,2 which is commonly found in females between 30 and 50 years of age.3–5 It is generally associated with diabetes mellitus (DM), chronic kidney disease, and liver disorders.6 The skin lesions of KD are characterized clinically by umbilicated, round, erythematous or hyperpigmented papules and nodules with central crusts or keratotic plugs. The lesions are mainly found on the extensor surfaces of the extremities and the trunk, and may involve the face or scalp, albeit uncommon.1,7 This case report presents a rare case of generalized lesion involving the face in a patient with KD.
Case
A 29-year-old woman, who had been diagnosed with type 1 DM since 13 years ago and with end-stage renal disease (ESRD) since one year ago, presented with a 4-month history of pruritic lumps and black spots, which began in the lower extremities. The patient scratched the skin lesions, and they became thick and expanded to form hyperpigmented plaques. The skin lesions became erosions, subsequently dried into serous crusts and left hyperpigmented macules. The lesions gradually spread to the hands, chest, abdomen, and one month later, the lesions extended to almost all parts of the body. Upon physical examination, vital signs were within normal limits, but icteric sclerae and hepatomegaly were found. Dermatological examination revealed a generalized distribution of multiple lesions on almost all parts of the body except the palms and soles. The skin lesions were mostly in the form of discrete, irregular, well-defined, dry, mostly raised, hyperkeratotic and hyperpigmented papules and nodules. The skin lesions were also accompanied by umbilication and keratotic plugs, as well as hyperpigmented plaques, serous crusts, and hyperpigmented macules. In addition, Koebner phenomenon was also observed (Figure 1).
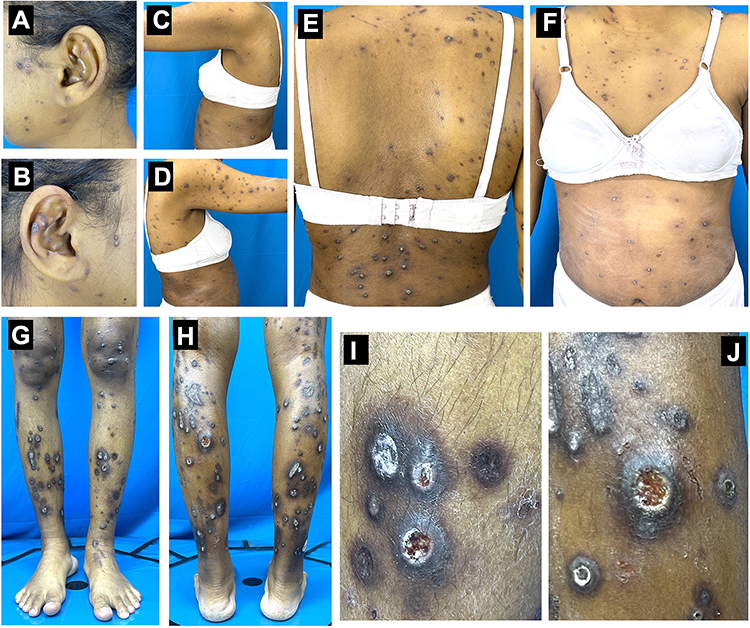 |
Figure 1 (A–H) shows the skin lesions on almost all parts of the body. (I and J) are hyperkeratotic and hyperpigmented papules and nodules with umbilication and keratotic plug lesion. |
Routine blood examination showed increased blood glucose, and the patient’s total protein and albumin levels were decreased. Histopathological examination showed that invagination is accompanied by the formation of keratin plugs. Basophilic cell debris with parakeratosis and abnormal keratinization of epithelial cells were observed (Figure 2). The histopathological features fulfilled the Constantine and Carter criteria for KD. This patient’s prognosis was poor due to the underlying diseases, which can be life-threatening. The patient died of Coronavirus disease (COVID)-19 before receiving therapy for KD.
 |
Figure 2 Histopathological findings. (A) Invagination with keratotic plug. Red arrow shows parakeratosis. Blue arrow shows abnormal keratinization; yellow arrow on picture (B) shows the invagination of basophilic cell debris. |
Discussion
In 1916, an Austrian dermatologist named Josef Kyrle first diagnosed hyperkeratosis follicularis et parafollicularis in cutem penetrans, now known as Kyrle’s Disease (KD), in a 22-year-old female with DM who complained of papules and hyperpigmented nodules measuring 5–10 mm in size with central keratotic plugs.8 A study by Kandasamy et al in 2019 at Government Rajaji Hospital India reported that KD made up for 54% of cases in 30 patients with perforating disease (PD).9 This disease occurs six times more often in females than in males, affecting individuals aged 30–50 years.7 Consistent with the epidemiological incidence of KD, the patient in this case report was a 29-year-old female.
Some types of APD, including KD, along with acquired perforating collagenosis (APC) and perforating folliculitis (PF) are generally associated with DM, chronic kidney disease, and liver disorders.1 APD, particularly KD, is usually identified in patients with DM and chronic kidney disease.1,10 Joseph et al reported 21 patients with KD, consisting of 19 patients with renal involvement in KD and 14 patients who suffered from DM for 7–10 years.10 Saray et al reported 22 cases of APD, eleven of which presented with DM.11 Kyrle’s disease usually manifests as erythematous, hyperpigmented, or skin-colored papules and nodules measuring 2–8 mm with central umbilication, crusting, or keratotic plugs with Koebner phenomenon. Pruritus is the most common subjective finding, and new lesions can arise from repeated scratching.1 The skin lesions of KD tend to be asymmetrically distributed and can be found in various parts of the body, especially the lower extremities.7 However, it does not affect the palms, soles, as well as the mucosa. Bhambri et al and Sahoo et al reported cases of KD that only occurred regionally at the extremities.7,12 Akcah et al reported cases of KD that occurred on the scalp, face, neck, and lower extremities.6 Wang et al reported that APD occurred after transient worsening of the original systemic disease.13 In this case report, physical examination revealed multiple hyperkeratotic and hyperpigmented papules, plaques, and nodules with central umbilication and keratotic plugs over almost all parts of the body. The patient had been diagnosed with DM since 13 years ago. She admitted that she rarely visited her doctor for her DM, resulting in the diagnosis of ESRD one year ago. She underwent regular hemodialysis twice a week.
The pathogenesis of KD has not yet been elucidated.1 Tappeiner et al reported that in KD, keratinization occurred faster than epidermal proliferation.14 Detmar et al reported an abnormal differentiation of the epidermis and dermoepidermal junction due to an increase in the glycosylation process in DM patients.15 Bellinato et al reported a possible physio-pathological role of advanced glycation end (AGE) product in the transepidermal elimination mechanisms involved in certain APDs.16 In patients with APD, AGE receptor expression was found to be more intense in different dermal components (ie, fibroblasts, microvascular endothelium, and inflammatory cells). Transepidermal elimination triggered by scratching or traumatic damage to the basement membrane zone can expose AGE products to keratinocytes.16 Kasaikou et al also reported improvement in KD patients who were given 300 mg clindamycin three times daily. Microorganisms are thought to play a role in the pathogenesis of KD, which is also supported by the histopathological findings of inflammatory cells infiltration in the area of the blockage.17
Kyrle’s disease must be differentiated from other disorders that cause hyperkeratotic central plugs as shown on Table 1.18 Other types of APD, such as APC, can manifest features similar to KD in the form of multiple erythematous or hyperpigmented papules, plaques, and nodules, with central umbilication and hyperkeratotic plugs. Diagnosis of KD is difficult to establish based solely on clinical examination; thus, histopathological examination is needed for diagnosis.1 Constantine and Carter formulated histopathological criteria for KD, which include keratotic plug that fills the invagination of the epithelium, parakeratosis, basophilic cell debris, and abnormal keratinization of epithelial cells.19 Histopathological examination can also distinguish KD from other types of APD, through findings of collagen blockage, which can be found in acquired reactive perforating collagenosis (ARPC), elastic tissue in acquired elastosis perforans serpiginosa (AEPS), and perforation of follicular epithelium by collagen and extracellular matrix in PF.1 Histopathological examination revealed keratinized epithelial layer with acanthosis and hyperkeratosis in our patient’s sample. Invagination with the formation of keratin plugs and basophilic cell debris accompanied by parakeratosis in all layers of the thinning epidermis and abnormal keratinization of epithelial cells were also visible. Hence, the histopathological findings met the Constantine and Carter criteria for KD.
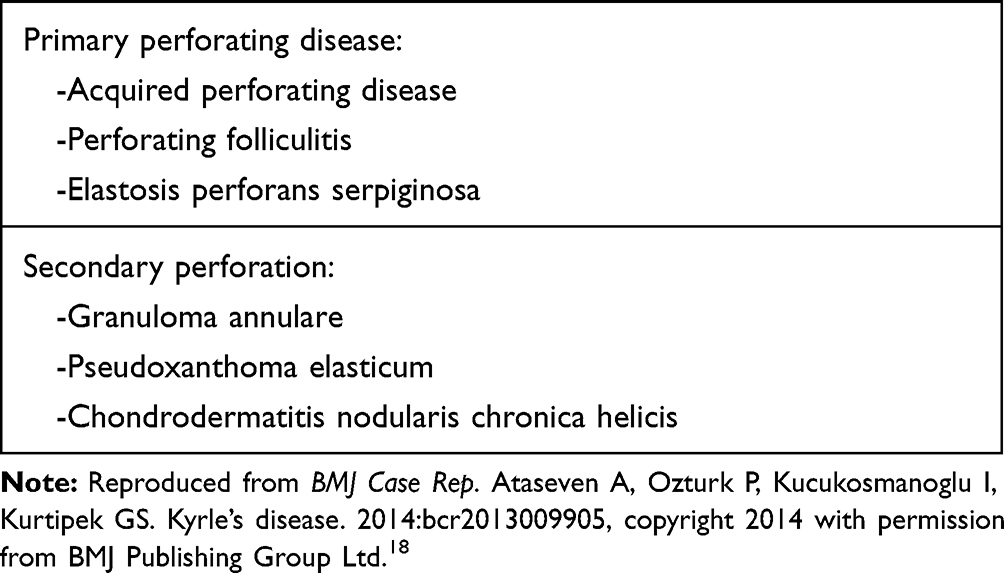 |
Table 1 Differential Diagnoses of Kyrle’s Disease |
The prognosis for this patient was poor due to the underlying diseases for APD. DM and ESRD can be particularly life-threatening. There have been reports of skin lesions resolving after the kidney condition stabilized following kidney transplantation.20
Conclusion
Kyrle’s Disease is one of the rare variants of primary PD. It is usually associated with DM, chronic kidney disease, and liver disorders. The diagnosis of KD is established based on clinical examination and histopathological examination. Lesions are usually distributed asymmetrically and can be found in various parts of the body, most commonly the lower extremities. Generalized lesions in KD occur very rarely. There is a high association between APD and systemic disorders with regard to their occurrence and lesion development.
Ethical Statement
The publications of images were included in the patient’s consent for publication of the case. Institutional approval to publish case details has been obtained.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of case details and images.
Acknowledgments
The authors would like to thank the staff of the Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Desman GT, Barnhill RT. Acquired perforating dermatosis. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, editors. Fitzpatrick’s Dermatology.
2. Shivakumar V, Okade R, Rajkumar V, et al. Familial Kyrle’s disease: a case report. Int J Dermatol. 2007;46:770–771. doi:10.1111/j.1365-4632.2007.03299.x
3. Prakken JR. Kyrle’s disease. Acta Dermatovener. 1954;34:360–367.
4. Weiner J. Kyrle’s disease in Siblings, society transactions. Arch Dermatol. 1967;95:329–332.
5. Cunningham SR, Walsh M, Matthews R, Fulton R, Burrows D. Kyrle’s disease. J Am Acad Dermatol. 1987;16:117–123. doi:10.1016/S0190-9622(87)70011-5
6. Akcah C, Baba M, Seckin D, Kayaselcuk F, Gulec T. Kyrle’s disease: a case report. J Turkish Acad Dermatol. 2007;1(4):71401c.
7. Bhambri SQJ, Rosso D, Mobini N, Janda P. Kyrle’s disease. Cosmet Dermatol. 2010;21(1):26–28.
8. Alshami MA, Mohana MJ. A case of infantile Kyrle-Flegel disease in a 6-year-old Yemeni girl. Case Rep Dermatol. 2016;8:5–9. doi:10.1159/000443824
9. Kandasamy S, Subramanian P, Gopalan G, Krishnamoorthy A. A retrospective clinicopathological study of cases of perforating dermatoses in a tertiary care centre. Int J Res Dermatol. 2019;5(4):722–727. doi:10.18203/issn.2455-4529.IntJResDermatol20194563
10. Joseph D, Papali C, Pisharody R. Kyrle’s disease: a cutaneous marker of renal disorder. Indian J Dermatol Venereol Leprol. 1996;62:222–225.
11. Saray Y, Seçkin D, Bilezikçi B. Acquired perforating dermatosis: clinicopathological features in twenty‐two cases. J EADV. 2006;20(6):679–688.
12. Sahoo AK, Rauta S. Kyrle’s disease: a rare skin manifestation of systemic diseases. J Med. 2014;15:144–145. doi:10.3329/jom.v15i2.20689
13. Wang MF, Mei XL, Wang L, Li LF. Clinical characteristics and prognosis of acquired perforating dermatosis: a case report. Exp Ther Med. 2020;19(6):3634–3640. doi:10.3892/etm.2020.8651
14. Tappeiner J, Wolff K, Schreiner E. Kyrle’s disease. Hautarzt. 1969;20:296–310.
15. Detmar M, Ruszczak Z, Imcke E, et al. Kyrle’s disease in juvenile diabetes mellitus and chronic renal failure. Z Hautkr. 1990;65:5361.
16. Bellinato F, Maurelli M, Gisondi P, Girolomoni G. Acquired perforating dermatoses show increased levels of cutaneous advanced glycation end‐products. Clin Exp Dermatol. 2022;47(1):80–85. doi:10.1111/ced.14851
17. Kasiakou SK, Peppas G, Kapaskelis AM, Falagas ME. Regression of skin lesions of Kyrle’s disease with clindamycin: implications for an infectious component in the etiology of the disease. J Infect. 2005;50(5):412–416. doi:10.1016/j.jinf.2004.06.009
18. Ataseven A, Ozturk P, Kucukosmanoglu I, Kurtipek GS. Kyrle’s disease. BMJ Case Rep. 2014;2014:bcr2013009905. doi:10.1136/bcr-2013-009905
19. Bodman M, Ehredt D, Barker R, Kirkland A, Mude P. Kyrle disease: a rare dermatologic condition associated with the diabetic foot. J Am Podiatr Med Assoc. 2015;105:451–455. doi:10.7547/14-009
20. Hemachandar R. Acquired perforating dermatosis in a diabetic patient on hemodialysis. Indian J Nephrol. 2016;26(4):304–305. doi:10.4103/0971-4065.161026
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.