Back to Journals » Patient Preference and Adherence » Volume 20
Gender Difference in Satisfaction with Nursing Home Services Among Disabled Elderly Inpatients Across Disease Categories: A Multi-Center Study
Authors Zhang J, Yu C, Han B ![]() , Li A, Huang X, Wang Y
, Li A, Huang X, Wang Y ![]()
Received 12 February 2026
Accepted for publication 30 May 2026
Published 11 June 2026 Volume 2026:20 602613
DOI https://doi.org/10.2147/PPA.S602613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Jing Zhang,1 Cong Yu,2 Biyuan Han,3 Aidong Li,4 Xiaoping Huang,5 Yulong Wang1
1Department of Rehabilitation, Shenzhen Second People’s Hospital, The First Affiliated Hospital of Shenzhen University, Shenzhen, Guangdong, 518035, People’s Republic of China; 2Department of Nursing, Shenzhen Second People’s Hospital, The First Affiliated Hospital of Shenzhen University, Shenzhen, Guangdong, 518035, People’s Republic of China; 3Department of Nursing, Shenzhen Dapeng New District Nan’ao People’s Hospital, Shenzhen, Guangdong, 518121, People’s Republic of China; 4Department of Rehabilitation,The Second People’s Hospital of Futian District Shenzhen, Guangdong, 518049, People’s Republic of China; 5Department of Nursing, Shenzhen Baihe Hospital, Shenzhen, Guangdong, 518112, People’s Republic of China
Correspondence: Yulong Wang, Department of Rehabilitation, Shenzhen Second People’s Hospital, The First Affiliated Hospital of Shenzhen University, Shenzhen, Guangdong, 518035, People’s Republic of China, Email [email protected]
Objective: This study aimed to investigate the independent effect of gender on patient satisfaction among disabled inpatients across various disease types and to identify the key factors influencing these satisfaction levels.
Methods: A cross-sectional, multi-center study recruited 1,157 disabled inpatients from seven institutions. The measurements encompassed general characteristics (age, gender, height, weight, disease diagnosis, and functional impairment). Data were analyzed using multivariable logistic regression to identify factors associated with patient satisfaction, supplemented by stratified subgroup analyses across disease categories. Receiver Operating Characteristic (ROC) curves were used to evaluate the predictive value of gender-specific factors.
Results: This study investigated gender differences in satisfaction among disabled elderly inpatients with prevalent comorbidities, including neurologic (75.8%) and cardiovascular (75.3%) diseases. Multivariate logistic regression revealed that males were significantly less likely to report satisfaction compared to females (OR = 0.465, p = 0.018), a trend consistent across subgroup analyses for cardiovascular diseases (OR = 0.452, p = 0.042) and chronic geriatric diseases (OR = 0.389, p = 0.047). Neurologic disease subgroups showed marginal significance (OR = 0.536, p = 0.083).
Conclusion: Gender is a significant determinant of satisfaction among disabled elderly residents, with males reporting lower satisfaction, particularly in cardiovascular and chronic geriatric departments. These findings underscore the necessity of transitioning from a “one-size-fits-all” model to gender-sensitive care. Implementing gender-tailored intervention strategies is essential to address psychosocial disparities and optimize patient-centered outcomes in long-term disability care.
Keywords: gender difference, disease, satisfaction, disability, inpatients
Introduction
Patient satisfaction serves as a critical indicator of healthcare service quality, directly influencing treatment adherence and health outcomes.1 In the context of globally aging populations, the satisfaction of disabled elderly inpatients has emerged as a vital metric for evaluating care systems, yet it remains insufficiently explored across diverse clinical profiles.2 Previous studies suggest that gender shapes healthcare perceptions through its influence on health behaviors, psychological status, and social support systems.3 Evidence further indicates that men and women face unique challenges in accessing quality inpatient care depending on their specific disease types.4 Consequently, as personalized medicine advances, understanding gender-based disparities in healthcare experiences has gained increasing academic and clinical attention.5
For disabled elderly inpatients—a population facing prolonged hospitalizations and complex care needs—satisfaction is a multi-dimensional construct that transcends simple clinician-patient interaction. In this study, we evaluated satisfaction across seven key domains: service quality, staff attitude, humanistic care, needs fulfillment, living environment, service pricing, and health improvement outcomes. The inclusion of these diverse domains is essential for a holistic evaluation because, for this population, the facility serves as a primary living space. Thus, environmental comfort, financial burden (pricing), and functional recovery (health outcomes) are as central to their care experience as the technical quality of medical services.
Existing literature regarding gender-based satisfaction, however, remains conflicting. Some studies indicate that female or older patients generally report higher satisfaction than male patients, potentially attributed to their greater propensity for emotional expression and social support-seeking.6 This contrasts with a German analysis of physician rating websites where male patients tended to rate more positively.7 Furthermore, research has shown that patients with internal medical or chronic conditions (e.g., cardiovascular diseases and diabetes) exhibit reduced satisfaction levels, with female patients occasionally showing significantly greater dissatisfaction than their male counterparts.8 Other data suggest that while a higher proportion of males may be extremely satisfied compared to females, the differences are not always statistically significant.9 Notably, studies on rural care reveal that gender disparities can become even more pronounced in specific geographical contexts.10
These discrepancies highlight that the influence of gender remains unclear, primarily due to the lack of systematic analysis across diverse disease categories. Although prior studies have examined gender differences in satisfaction, most have focused on single-disease cohorts or specific populations, failing to account for the clinical complexity of disabled inpatients. Clarifying the distinct needs of male and female patients is essential for targeted care management and the improvement of overall care quality. However, no previous studies have systematically investigated whether gender disparities in patient satisfaction exist across various types of diseases among disabled inpatient populations in China. To address this gap, the present study accounts for participants’ functional status while systematically investigating gender differences in satisfaction across various disease categories. This study aims to investigate gender differences in satisfaction with nursing home services among disabled elderly inpatients across different disease categories, thereby providing an empirical basis for optimizing individualized care strategies and improving long-term health outcomes.
Materials and Methods
Study Design
This study employed a multi-center cross-sectional design to collect satisfaction data regarding institutional caregiver services through a structured questionnaire survey. To ensure objectivity, the survey targeted either the inpatients or their primary family caregivers. Under the coordination of head nurses, the survey was administered to a comprehensive sample, covering no less than 80% of the eligible respondents currently in the wards. All eligible patients within the assessment window were recruited between August 2022 and May 2023 (ChiCTR2100045187). Informed consent was acquired online from all participants prior to enrollment; in cases where a patient was unable to provide consent due to cognitive or physical incapacity, informed consent was obtained from their legally authorized representative.
Participants and Sampling
A multistage stratified sampling method was employed to recruit a representative sample of disabled elderly residents from nursing home institutions. To ensure sufficient statistical power for multidimensional satisfaction analysis, a priori power analysis was performed to determine the required sample size. As shown in the participant selection flowchart (Figure 1), 1,275 residents were initially screened. After excluding individuals who did not meet the inclusion criteria or had incomplete records, the final analytical sample comprised 1,157 participants. This sample size provides ample power for the subsequent gender-based comparisons and logistic regression models, ensuring the stability and reliability of the estimated parameters.
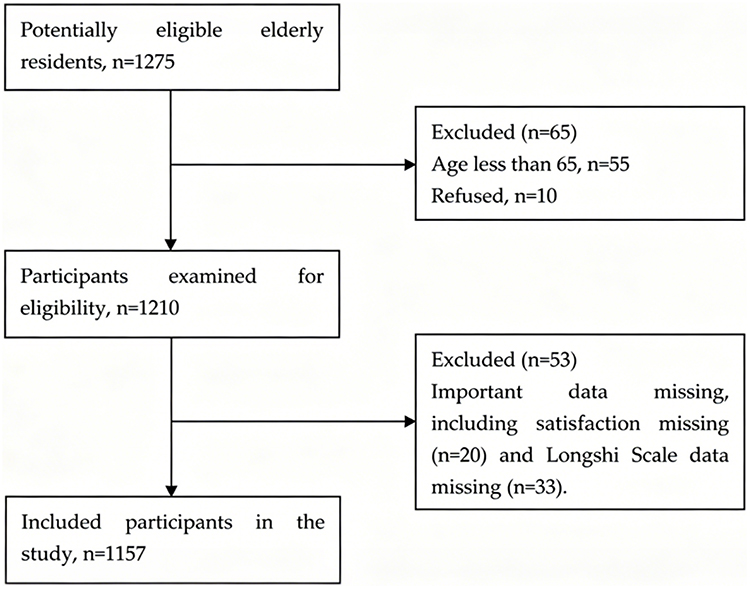 |
Figure 1 The participant selection flowchart. |
Sampling Strategy
A multistage stratified sampling method was employed to ensure a representative distribution.
In the first stage, nursing home institutions in the first-tier cities of China were selected as primary sampling units based on the following criteria: (1) high consistency in clinical pathways, standardized nursing/rehabilitation protocols, and service pricing; (2) routine integration of the Longshi Scale for disability assessment into daily care; and (3) enhanced representativeness to ensure generalizability rather than convenience sampling.
In the second stage, a systematic sampling approach was utilized within various units of the selected institutions to recruit eligible disabled inpatients, thereby minimizing selection bias.
Inclusion and Exclusion Criteria
The inclusion criteria for participants were as follows: (1) complete assessment data on satisfaction measurement were available; (2) they were identified as disabled according to the Longshi scale; (3) they were inpatients; (4) they could complete all evaluation procedures; and (5) they provided informed consent to participate in the study.
The exclusion criteria were as follows: (1) presence of severe organ dysfunction (eg., severe decompensation of the heart, liver, or kidneys); (2) history of severe mental disorders or related diseases.
Measurement
General Information Questionnaire
A self-compiled questionnaire was used to collect demographic and health-related information, including name, gender, age, telephone number, height, weight, BMI, smoking status, drinking status, disease information, and patient satisfaction.
Longshi Scale
The Longshi Scale (LS) demonstrates Cronbach’s α coefficients ranging from 0.589 to 0.875, indicating acceptable internal consistency.11–13 We selected the LS because it was independently developed for the Chinese institutional context, and was officially adopted as the National Standard of China in 2018 (GB/T37103-2018). The scale comprises three dimensions—bedside, room, and outdoor activities—with a total score of 20 points. Based on the total score, the disability level is categorized as follows: 0 points indicate bedridden (complete dependency); 1–6 points indicate severe disability; 7–13 points indicate moderate disability (indoor activities); and 14–20 points indicate mild disability or functional independence (outdoor activities). This framework provides an accurate categorization of the disabled population based on functional mobility, specifically their ability to transition from being bedbound to moving outdoors.
Satisfaction Questionnaire
Patient satisfaction was evaluated using a self-developed 7-item scale (English and Chinese versions are provided in Supplementary Figures S1 and S2, respectively). The seven domains (service quality, staff attitude, humanistic care, needs fulfillment, living environment, service pricing, and health improvement) were based on national Chinese elderly care service standards (GB/T 35796–2017, GB/T 37276–2018, MZ/T 133–2019). Each domain was assessed using a single item. All items were rated on a 5-point Likert scale (1 = very dissatisfied, 5 = very satisfied). The overall satisfaction score was calculated as the arithmetic mean of the seven domain scores. Given the high overall satisfaction rate (95.76%) in this cohort, the outcome was dichotomized into Satisfied (mean score ≥ 4.0) and Not Satisfied (mean score < 4.0) using the Top-Two Box method, a standard approach for analyzing skewed satisfaction data. In our sample, the scale demonstrated acceptable internal consistency (Cronbach’s α = 0.862).
Data Collection
Data were collected from seven representative long-term care institutions in first-tier cities, including Shanghai, Guangzhou, and Shenzhen (eg., Baihe, Nanao, Caring Home, Longcheng, and Shenzhen Facilities). The database collected information on general information, disease information, and patients satisfaction through face-to-face interviews. The degree of disability was assessed using the Longshi Scale, while patient satisfaction was evaluated via a standardized questionnaire. Patient satisfaction was dichotomized into “satisfied” and “not satisfied” using the Top-Two Box method as described in the Measurement section.
Statistical Analysis
Descriptive statistics were used to summarize baseline characteristics, with categorical variables presented as frequencies (%) and continuous variables as mean ± SD. Detailed assignment and coding of all study variables are explicitly provided in Table 1. Multivariable logistic regression analyses were performed to evaluate factors associated with patient satisfaction. The base model was adjusted for age, smoking status, drinking status, combined dysfunction, and Longshi Scale score to control for potential confounding. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to quantify associations. Stratified subgroup analyses by major disease categories (neurologic, cardiovascular, and chronic geriatric diseases) were performed to investigate gender-specific disparities in patient satisfaction. Detailed disease classifications and categories are presented in Supplementary Table S1. Stratified logistic regression models were used to assess heterogeneity in gender-related effects across disease subgroups, while Receiver Operating Characteristic (ROC) curves were constructed to evaluate the clinical predictive value of gender for satisfaction levels. The discriminatory performance of the ROC curves was interpreted using the following standard thresholds: Poor discrimination: AUC = 0.50–0.69; Acceptable discrimination: AUC = 0.70–0.79; Excellent discrimination: AUC ≥ 0.80. All statistical analyses were conducted in R version 4.4.3 (R Foundation for Statistical Computing, Vienna, Austria), utilizing the ggplot2 and pROC packages for visualization and model validation.
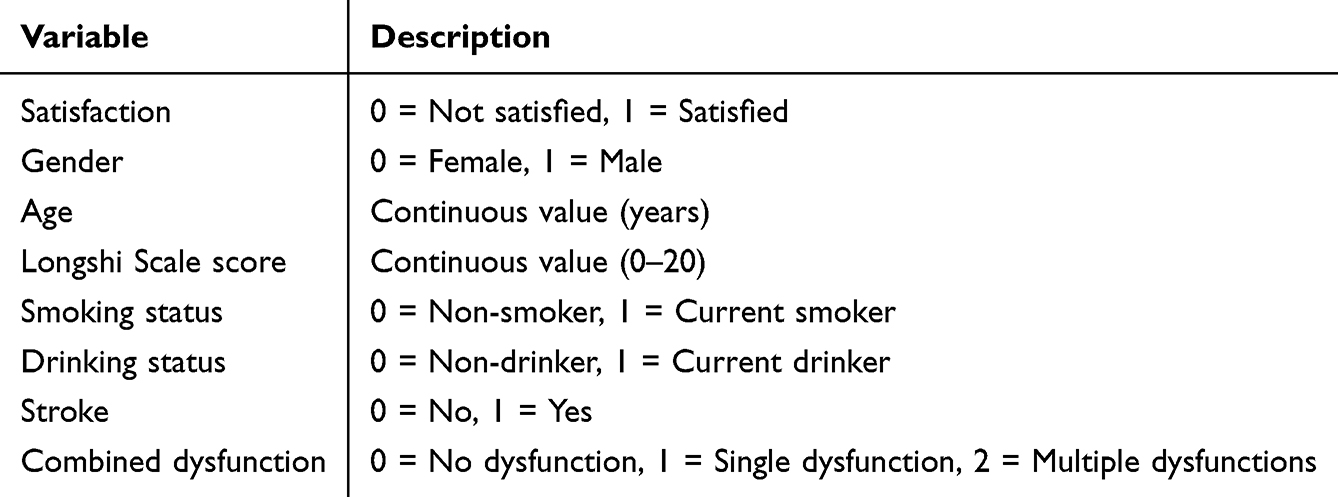 |
Table 1 Variable Assignment |
Results
Variable Description
Detailed variable assignments are presented in Table 1, with categorical variables coded as binary indicators, continuous variables retained on their original scales, and combined dysfunction treated as an ordinal variable (0, 1, 2) in the regression analysis.
General Characteristics of Participants
Out of 1,157 participants, overall satisfaction was relatively high (95.76%), and the gender distribution of the sample was balanced (50.99% female, 49.01% male). Participants could report multiple diagnoses, with neurologic (75.80%) and cardiovascular (75.37%) diseases being the most prevalent comorbidities. Specifically, 36.13% of the participants were diagnosed with chronic geriatric diseases, while 20.31% were diagnosed with other diseases (Table 2).
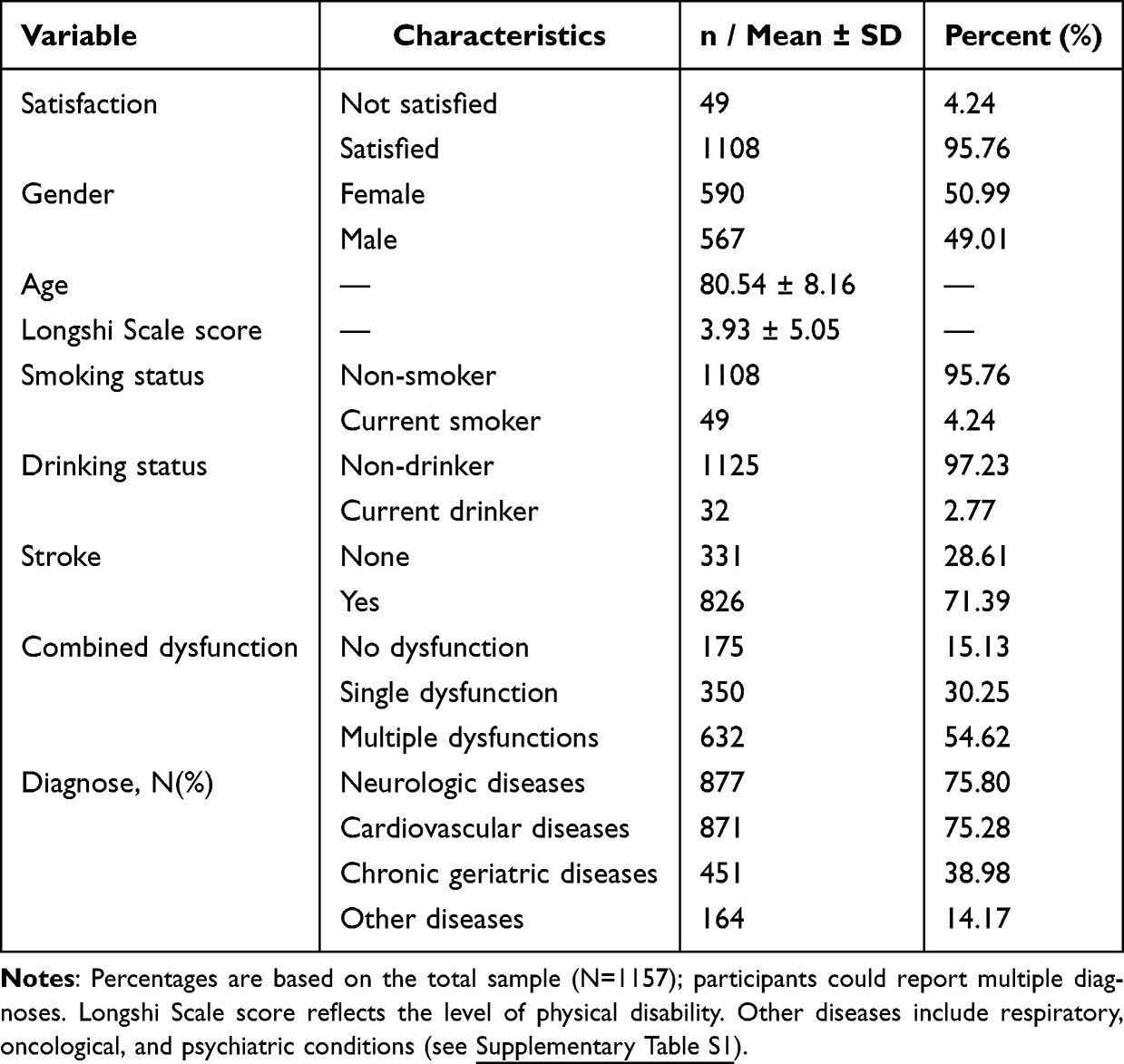 |
Table 2 Characteristics of Disabled Elderly Inpatients (N=1157) |
Gender Differences in Patient Satisfaction
Multivariable logistic regression analysis were conducted to identify factors associated with patient satisfaction, as presented in Table 3.
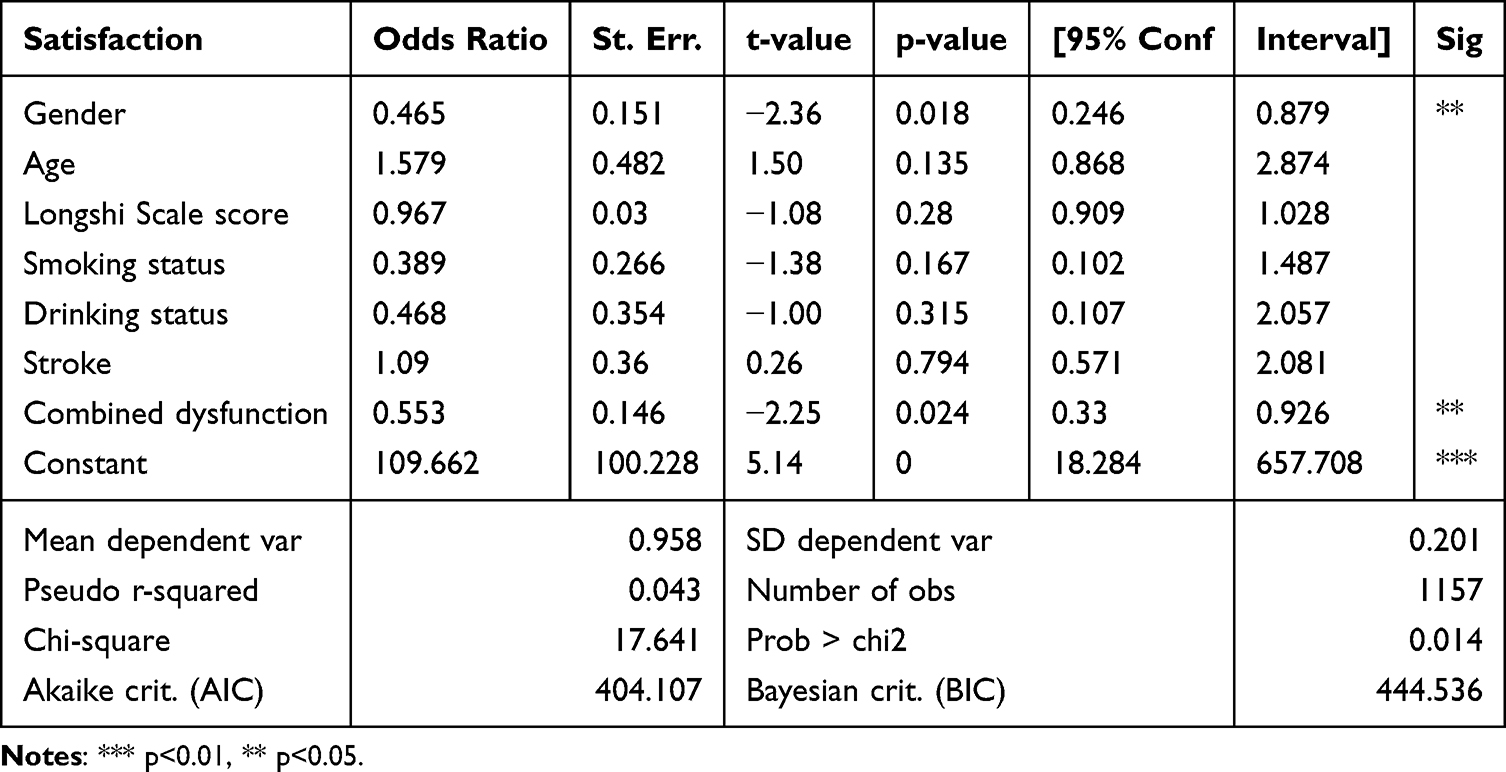 |
Table 3 Logistic Regression Analysis on Satisfaction |
The results demonstrated that gender was a significant associated variable, with males being significantly less likely to report satisfaction compared to females (OR = 0.465; 95% CI: 0.246–0.879; p = 0.018). In contrast, none of the other variables, including Smoking status, Drinking status, Combined dysfunction, Age, and Longshi Scale score were significantly associated with satisfaction (all p > 0.05). Detailed results of the adjusted model are presented in Supplementary Table S2.
Subgroup Analysis of Gender Differences by Disease Category
To assess the robustness of gender-related disparities, subgroup analyses were performed by major disease categories, including neurologic, cardiovascular, and chronic geriatric diseases (Tables 4–6). The results consistently demonstrated that female patients reported significantly higher satisfaction levels than their male counterparts across all primary categories. Specifically, gender was a significant associated variable of satisfaction in cardiovascular diseases (OR = 0.452, 95% CI [0.21, 0.973], p = 0.042; Table 5) and chronic geriatric diseases (OR = 0.389, 95% CI [0.153, 0.989], p = 0.047; Table 6). A similar, albeit marginally significant, trend was observed among patients with neurologic diseases, where males reported lower satisfaction than females (OR = 0.536, 95% CI [0.265, 1.085], p = 0.083; Table 4).
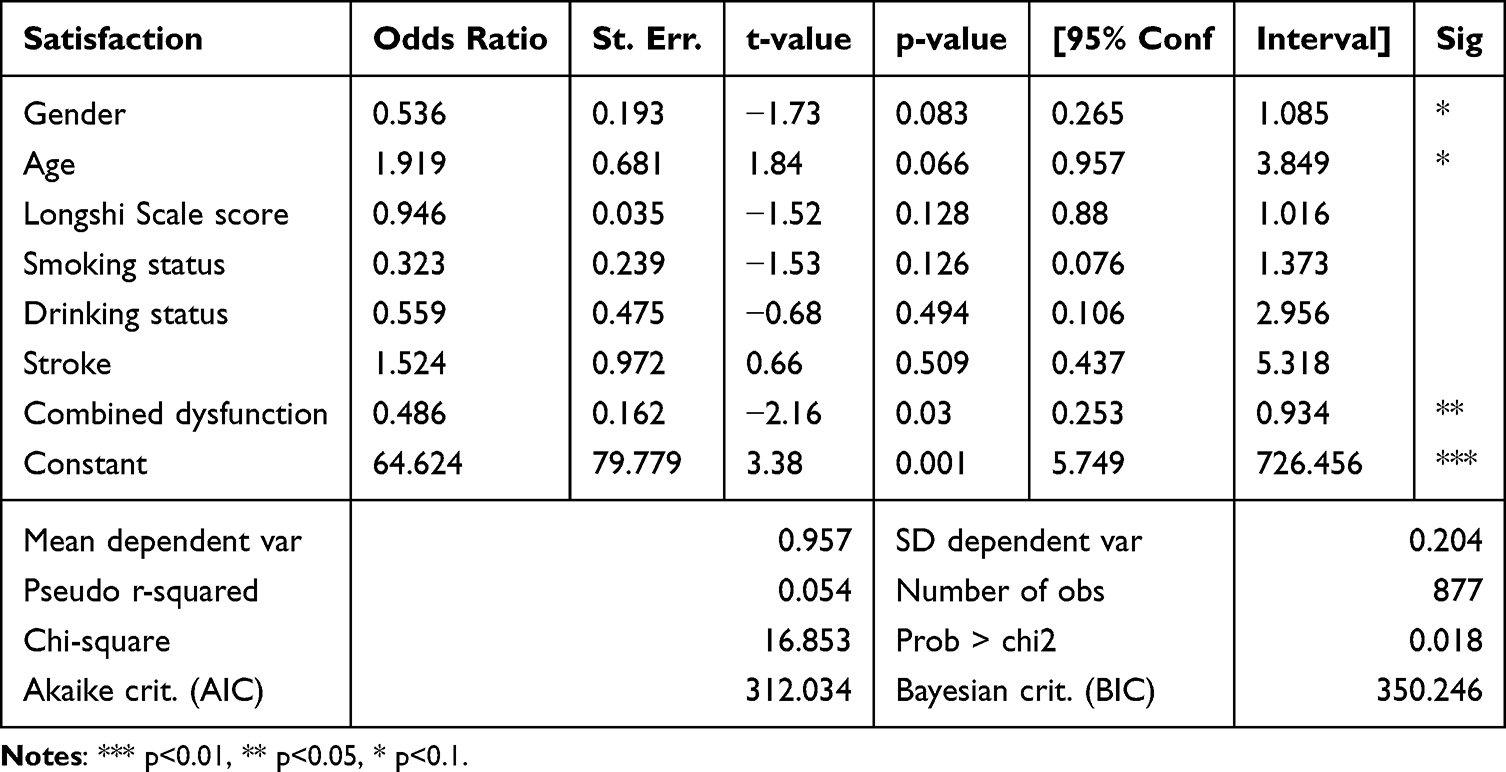 |
Table 4 Gender Differences in Satisfaction with Neurologic Diseases |
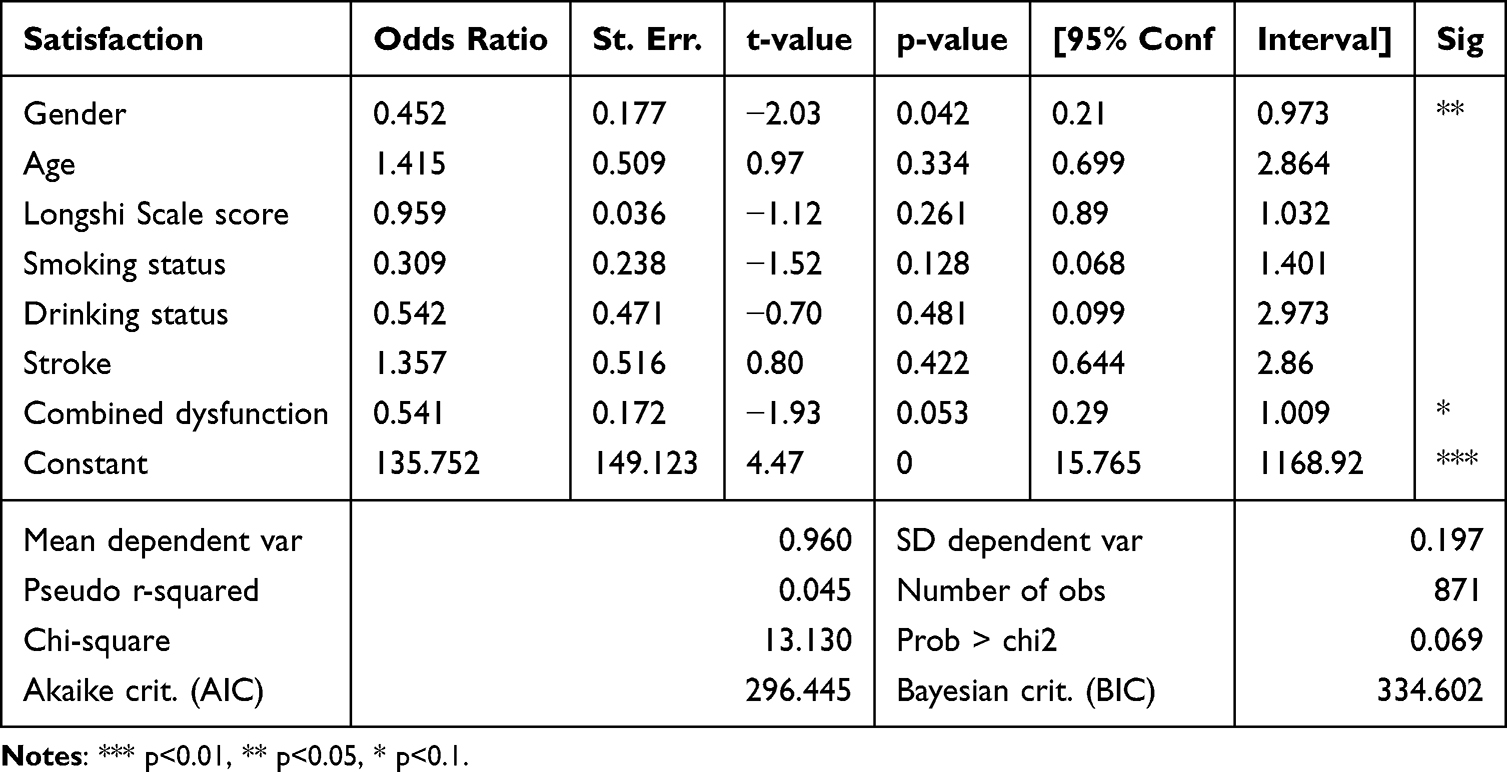 |
Table 5 Gender Differences in Satisfaction with Cardiovascular Diseases |
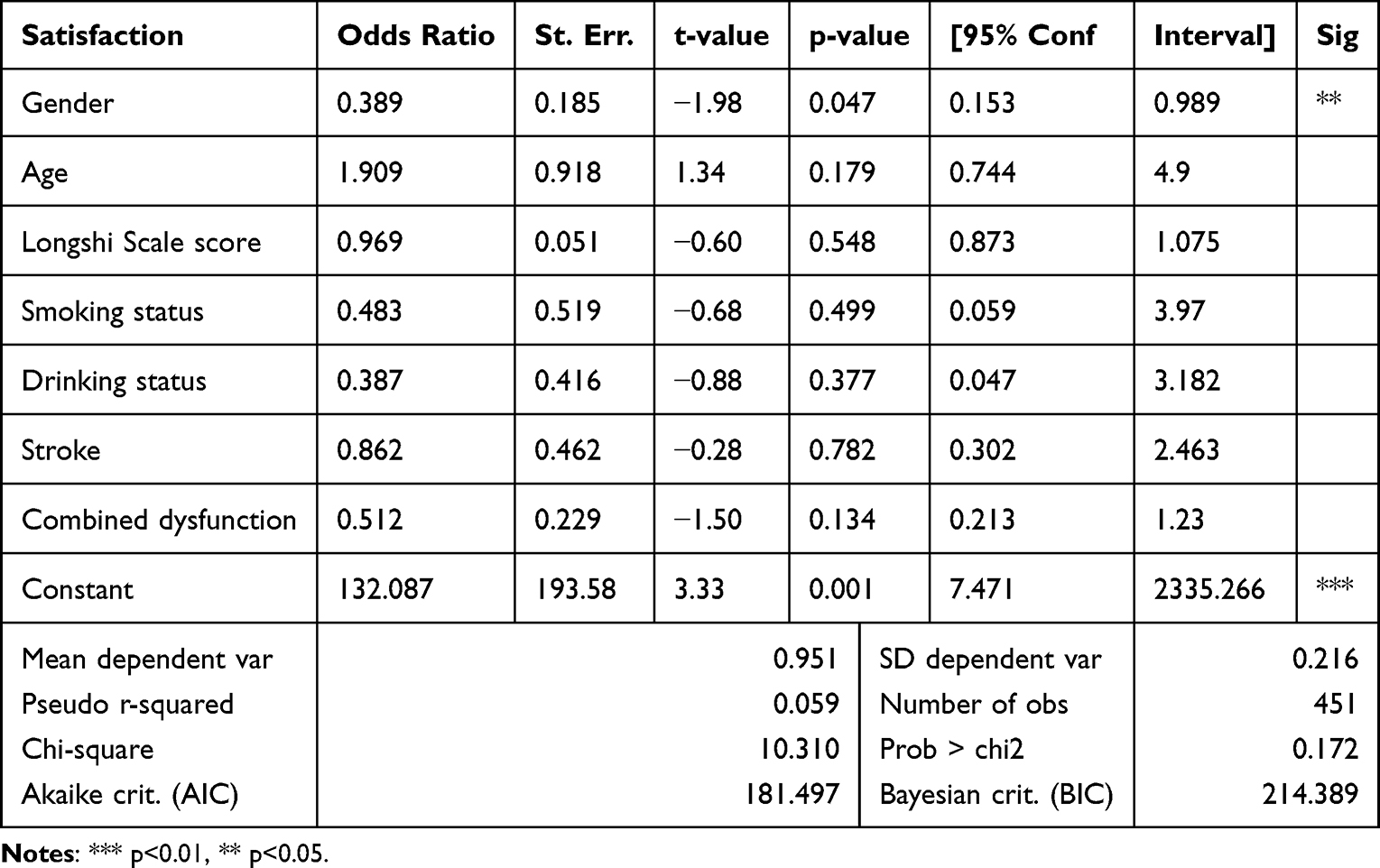 |
Table 6 Gender Differences in Satisfaction with Chronic Geriatric Diseases |
Assessment of the Predictive Value of Gender via ROC Curve Analysis
ROC curve analysis was performed to evaluate the discriminative performance of gender for patient satisfaction across different disease subgroups. The results showed that gender exhibited poor to acceptable discriminative ability, with the AUC values of 0.704 for chronic geriatric diseases, 0.702 for neurologic diseases, and 0.676 for cardiovascular diseases (Figure 2). While these values are insufficient to support gender as a standalone predictive tool, they further validate the significant association between gender and satisfaction observed in the logistic regression model, indicating that gender may serve as a stable and meaningful associated factor rather than a reliable clinical predictor.
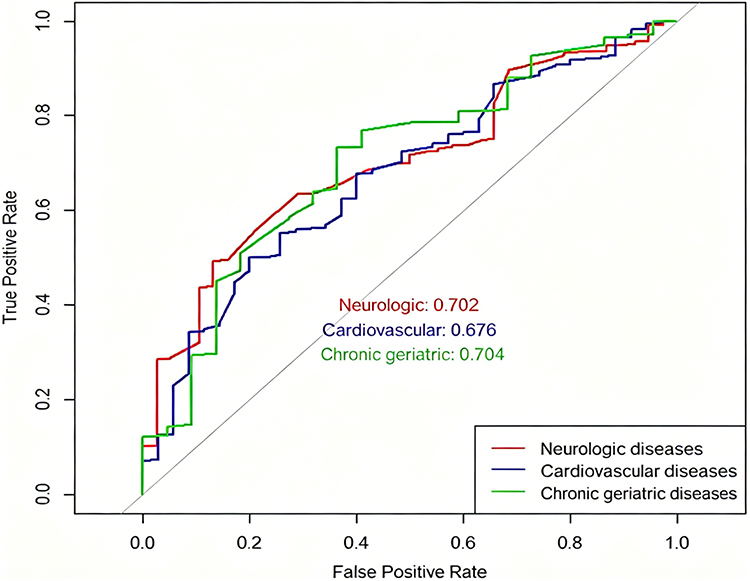 |
Figure 2 ROC curves for exploratory analysis of gender as a discriminative factor for satisfaction across disease subgroups. Figure Legend: ROC curves are shown for chronic geriatric diseases (green, AUC = 0.704), neurologic diseases (red, AUC = 0.702), and cardiovascular diseases (blue, AUC = 0.676). The diagonal line indicates a non-discriminatory model (AUC = 0.5). |
Discussion
Main Findings
This multicenter study identifies significant gender disparities in satisfaction among disabled elderly inpatients in China. Males reported consistently lower satisfaction across neurologic, cardiovascular, and chronic disease subgroups. This may be explained by two factors. First, male patients tend to hold higher expectations regarding care quality and place greater emphasis on technical competence.14 Second, the psychological distress following physical impairment may be more acute for men, as they experience greater “role strain” when transitioning from “family pillar” to “care receiver”.15 Societal expectations of “male stoicism” may further deter them from expressing unmet needs.16
In contrast, female patients reported higher satisfaction, likely reflecting their greater prioritization of empathetic communication and humanistic care.17 Women often value social connection and emotional support more than resource adequacy.18 However, this positive trend was not universal. In the “other diseases” group (eg., digestive disorders, arthritis), female inpatients reported higher dissatisfaction,19 suggesting that physical burden and pain may override the benefits of effective communication for certain conditions.
Additionally, clinicians may inadvertently neglect male psychosocial needs due to gender stereotypes.20 Lower satisfaction among males with various major disease types may stem from male patients were less likely to express unmet care needs.21,22 Evidence suggests that gender significantly shapes satisfaction with care services for disabled inpatients with low daily living ability.23 Addressing these disparities is essential for achieving equitable healthcare outcomes.
Impact of Multimorbidity Patterns on Gender-Specific Satisfaction
Disease trajectory network analysis suggests that neurologic conditions like stroke occupy a central role in comorbidity networks.24 Therefore, early intervention for hypertension or dyslipidemia is crucial, especially for female patients with complex care needs.19
Against the backdrop of China’s Diagnosis-Related Group (DRG) reforms, these disparities highlight the need for gender-sensitive policies.25 DRG-based payment systems often shorten hospital stays to improve efficiency, yet disabled male patients typically require longer adaptation periods and more complex technical nursing than females to achieve functional stability.26 This systemic pressure may be further compounded by biases in care delivery. Specifically, clinicians in resource-limited settings may unconsciously prioritize female patients due to stereotypes regarding their “higher compliance”, inadvertently neglecting the distinct psychosocial and technical needs of disabled men.27 Such a mismatch likely contributes to lower satisfaction among male inpatients in cardiovascular and chronic disease departments.
Our findings underscore that women often report higher healthcare satisfaction than men, a trend consistent with global observations regarding gender-based care perceptions.28 Given the high prevalence of multimorbidity among disabled inpatients, strengthening the understanding of gender-specific needs is essential for individualized care. Hospitals should adopt three strategies: (1) Communication training tailored to address patients’ concerns and reluctance to seek help; (2) Financial support including insurance benefits and charity programs for low-income female patients. (3) Environmental optimization balancing communal social spaces (favored by females) with quiet, functional zones (favored by males).
Tailored Resource Allocation
While gender was identified as an independent associated factor in the regression model, exploratory ROC analysis revealed only poor to acceptable discriminative ability across disease subgroups (AUC = 0.676–0.704). These findings do not support gender as a standalone clinical predictor, but confirm it as a consistent associated factor that contributes to understanding satisfaction disparities. Future studies should develop multi-factor models incorporating both clinical and service-related variables to improve predictive performance.
To maximize healthcare equity, resource allocation must transition from a “one-size-fits-all” approach to gender-sensitive strategies. Evidence suggests male patients tend to place a higher premium on “Service Level” and “Living Environment,” while females prioritize “Staff Attitude” and “Humanistic Care”.29,30 The pronounced dissatisfaction among male patients in Neurology and Cardiology departments suggests that current care models may inadequately address the technical and functional expectations.31 For female patients, complex multimorbidity patterns (eg., musculoskeletal issues) necessitate integrated clinical pathways to manage physical pain effectively.32 Aligning resource distribution with distinct satisfaction profiles can bridge gender gaps, optimize individualized care, and advance equity in disability care delivery.
Clarifying these gender differences is essential for personalizing care plans and improving services for disabled inpatients, particularly in LMICs and other resource-limited settings.
Strengths and Limitations
The results provide an empirical basis for disability care strategies. However, several limitations should be noted. Firstly, the cross-sectional design assessed satisfaction only at a single time point, precluding evaluation of changes over time. Secondly, the sample was limited to first-tier cities, which may introduce selection bias and limit generalizability to rural or home-based settings. Thirdly, the highly skewed satisfaction distribution (95.76%) and dichotomization may have led to a loss of granular information, though model robustness was supported by AIC/BIC values. This “ceiling effect” may be compounded by social desirability bias, as some surveys required caregiver assistance. Proxy-reporting could overestimate satisfaction. Fourthly, although the 7-item satisfaction measure demonstrated acceptable internal consistency, each item captures a distinct aspect of satisfaction. Thus, the use of a single item per aspect may not capture the full complexity of each domain, and future research could consider developing multi-item subscales for each satisfaction facet. Lastly, socioeconomic status and educational level, which are potential confounders of satisfaction, were not directly measured. However, the high standardization among participating first-tier city facilities suggests a relatively homogeneous sample in this regard. Notwithstanding these limitations, this study offers evidence-based guidance for optimizing individualized care for disabled elderly inpatients.
Conclusion
This study identifies significant gender disparities in satisfaction among disabled elderly inpatients in China. Males reported lower satisfaction than females, particularly within cardiovascular and chronic geriatricdisease departments. While gender was significantly associated with satisfaction, its discriminative ability was modest (AUC = 0.676–0.704), indicating that gender alone is insufficient as a standalone clinical predictor. Nonetheless, these gender-specific patterns offer valuable insights for tailoring patient-centered care, suggesting that healthcare delivery must move beyond a “one-size-fits-all” approach. Integrating gender-sensitive assessment tools and tailored intervention strategies into clinical practice may help optimize patient-centered outcomes and narrow the equity gap in long-term disability care. Future research should develop multi-factor predictive models and validate the satisfaction instrument in more diverse populations.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Statement
The questionnaire and methodology for this study were approved by the Medical Ethics Committee of Shenzhen Second People’s Hospital (approval number: 2023-226-02PJ). All study procedures involving human participants were conducted in accordance with the ethical standards of the national research committee, the Helsinki Declaration, and the WHO Ethical Standards for Health Research Involving Human Participants.
Acknowledgments
We would like to express our gratitude to the participants and trained physicians and nurses of the hospital for assisting us to perform the cross-sectional survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Sanming Project of Medicine in Shenzhen (No. SZSM202111010), and Shenzhen Medical Research Fund (C2401013).
Disclosure
The authors declare no competing interests in this work.
References
1. Aiken LH, Sermeus W, Van den Heede K, et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344(mar20 2):e1717. doi:10.1136/bmj.e1717
2. Qi X, Jia N, Hu J, et al. Analysis of the status of social frailty in Chinese older adults with cardiovascular and cerebrovascular diseases: a national cross-sectional study. Front Public Health. 2023;11:1022208. doi:10.3389/fpubh.2023.1022208
3. Sarid O, Slonim-Nevo V, Pereg A, et al. Coping strategies, satisfaction with life, and quality of life in Crohn’s disease: a gender perspective using structural equation modeling analysis. Environ Health Preventative Med. 2017;12(2):e0172779. doi:10.1265/ehpm.23-00125
4. Razmjou H, Davis AM, Jaglal SB, Holtby R, Richards RR. Disability and satisfaction after rotator cuff decompression or repair: a sex and gender analysis. BMC Musculoskeletal Disord. 2011;12(1):66. doi:10.1186/1471-2474-12-66
5. Matthias K, Honekamp I, Heinrich M, De Santis KK. Consideration of sex, gender, or age on outcomes of digital technologies for treatment and monitoring of chronic obstructive pulmonary disease: overview of systematic reviews. J Med Internet Res. 2023;25:e49639. doi:10.1371/journal.pone.0172779
6. Emmert M, Halling F, Meier F. Evaluations of dentists on a German physician rating Website: an analysis of the ratings. J Med Internet Res. 2015;17(1):e15. doi:10.2196/jmir.3830
7. Gesundheit S. Gute Noten für Ärzte und ihre Praxen. Available from: http://www.stiftung-gesundheit.de/pi-2012-02-02.
8. Park SH, Hong SH. Identification of primary medication concerns regarding thyroid hormone replacement therapy from online patient medication reviews: text mining of social network data. J Med Internet Res. 2018;20(10):e11085. doi:10.2196/11085
9. Waite LJ, Duvoisin R, Kotwal AA, Silverstein M. Social health in the national social life, health, and aging project. J Gerontol B Psychol Sci Soc Sci. 2021;76(Suppl 3):S251–11. doi:10.1093/geronb/gbab138
10. Benchimol EI, Kuenzig ME, Bernstein CN, et al. Rural and urban disparities in the care of Canadian patients with inflammatory bowel disease: a population-based study. Clin Epidemiol. 2018;10:1613–1626. doi:10.2147/clep.s178056
11. Liu X, Gao Y, Zhao J, Zhou M, Wan L. Reliability of pictorial Longshi Scale for informal caregivers to evaluate the functional Independence and disability. Nursing Open. 2023;10(3):1852–1862. doi:10.1002/nop2.1448
12. Zhang Z, Liu F, Wong J, et al. Reliability of Longshi scale with remote assessment of smartphone video calls for stroke patients’ activities of daily living. J Stroke Cerebrovascu Dis. 2023;32(3):106950. doi:10.1016/j.jstrokecerebrovasdis.2022.106950
13. Zhou J, Zha F, Liu F, et al. Reliability and validity of a graphical computerized adaptive test Longshi scale for rapid assessment of activities of daily living in stroke survivors. Sci Rep. 2024;14(1):7625. doi:10.1038/s41598-024-57671-1
14. Kitole FA, Ali Z, Song J. Exploring the gender preferences for healthcare providers and their influence on patient satisfaction. Healthcare. 2025;13(9). doi:10.3390/healthcare13091063
15. Boltz M, Resnick B, Chippendale T, Galvin J. Testing a family-centered intervention to promote functional and cognitive recovery in hospitalized older adults. J Am Geriatr Soc. 2014;62(12):2398–2407. doi:10.1111/jgs.13139
16. Woo S, Cui Y, Kim S, Choi M. Gender differences in caregiver attitudes and unmet needs for activities of daily living (ADL) assistance among older adults with disabilities. BMC Geriatrics. 2023;23(1):671. doi:10.1186/s12877-023-04383-2
17. Wagner D, Bear M. Patient satisfaction with nursing care: a concept analysis within a nursing framework. J Adv Nurs. 2009;65(3):692–701. doi:10.1111/j.1365-2648.2008.04866.x
18. Li Y, Gong W. Factors associated with outpatient satisfaction in tertiary hospitals in china: a systematic review. Int J Environ Res Public Health. 2020;17(19). doi:10.3390/ijerph17197070
19. Wang J, Xiao LD, Wang K, Luo Y, Li X. Gender Differences in Cognitive Impairment among Rural Elderly in China. Int J Environ Res Public Health. 2020;17(10). doi:10.3390/ijerph17103724
20. Wang J. Comorbidity, lifestyle factors, and sexual satisfaction among Chinese cancer survivors. BMJ Open RespiratRes. 2021;10(17):6058–6069. doi:10.1136/bmjresp-2023-001932
21. Smith CM, Lane SH, Brackney DE, Horne CE. Role expectations and workplace relations experienced by men in nursing: a qualitative study through an interpretive description lens. J Adv Nurs. 2020;76(5):1211–1220. doi:10.1111/jan.14330
22. Kusano T, Kinoshita S, Aoyagi R, Saito K, Nakamoto H, Tajima A. Treatment patterns and satisfaction in patients with type 2 diabetes newly initiating oral monotherapy with antidiabetic drugs in Japan: results from the prospective Real-world Observational Study on Patient Outcomes in Diabetes (RESPOND). Sci Rep. 2022;10(6). doi:10.1038/s41598-022-11838-w
23. Hernan AL, Giles SJ, O’Hara JK, Fuller J, Johnson JK, Dunbar JA. Developing a primary care patient measure of safety (PC PMOS): a modified Delphi process and face validity testing. BMJ Quality Safety. 2016;25(4):273–280. doi:10.1136/bmjqs-2015-004268
24. Chen J, Zhang F, Zhang Y, et al. Trajectories network analysis of chronic diseases among middle-aged and older adults: evidence from the China Health and Retirement Longitudinal Study (CHARLS). BMC public Health. 2024;24(1):559. doi:10.1186/s12889-024-17890-7
25. Rozzini R, Sleiman I, Maggi S, Noale M, Trabucchi M. Gender differences and health status in old and very old patients. J Am Med Directors Assoc. 2009;10(8):554–558. doi:10.1016/j.jamda.2009.04.005
26. Abdul Rahman H, Tengah A, Mohd Yusof Y, Slesman L, Hoon C-Y, Abdul-Mumin KH. Predictors of satisfaction with life and health status of older people in brunei: a gender comparative study. Int J Public Health. 2022;67:1605042. doi:10.3389/ijph.2022.1605042
27. Lynn MR, McMillen BJ, Sidani S. Understanding and measuring patients’ assessment of the quality of nursing care. J Adv Nurs. 2007;56(3):159–166. doi:10.1111/jan.15026
28. Lleal M, Baré M, Herranz S, et al. Trajectories of chronic multimorbidity patterns in older patients: MTOP study. BMC Geriatrics. 2024;24(1):475. doi:10.1186/s12877-024-04925-2
29. Liu P, Yang Y, Cheng J. Gender differences in medical errors among older patients and inequalities in medical compensation compared with younger adults. Front Public Health. 2022;10:883822. doi:10.3389/fpubh.2022.883822
30. Li M, Zhu W-J, Luo Q, Chen H, Duan Y, Xie H-Z. Psychological experience of humanistic care among medical staff in stroke wards: a qualitative research study conducted in China. Front Psychiatry. 2022;13:791993. doi:10.3389/fpsyt.2022.791993
31. Fradgley EA, Paul CL, Bryant J, Roos IA, Henskens FA, Paul DJ. Consumer participation in quality improvements for chronic disease care: development and evaluation of an interactive patient-centered survey to identify preferred service initiatives. J Med Internet Res. 2014;16(12):e292. doi:10.2196/jmir.3545
32. Buczak-Stec E, König HH, Feddern L, Hajek A. Long-term care preferences and sexual orientation–a systematic review and meta-analysis. J Am Med Directors Assoc. 2023;24(3):331–342.e1. doi:10.1016/j.jamda.2022.11.020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.