Back to Journals » Patient Preference and Adherence » Volume 13
Gender Based Cognitive Determinants Of Medication Adherence In Older Adults With Chronic Conditions
Authors Mahmoodi H ![]() , Jalalizad Nahand F, Shaghaghi A
, Jalalizad Nahand F, Shaghaghi A ![]() , Shooshtari S
, Shooshtari S ![]() , Jafarabadi MA
, Jafarabadi MA ![]() , Allahverdipour H
, Allahverdipour H
Received 12 June 2019
Accepted for publication 18 September 2019
Published 15 October 2019 Volume 2019:13 Pages 1733—1744
DOI https://doi.org/10.2147/PPA.S219193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hassan Mahmoodi,1 Fatemah Jalalizad Nahand,2 Abdolreza Shaghaghi,2 Shahin Shooshtari,3 Mohammad Asghari Jafarabadi,4 Hamid Allahverdipour2
1Social Determinants of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj, Iran; 2Department of Health Education and Health Promotion, School of Public Health, Tabriz University of Medical Sciences, Tabriz, Iran; 3Departments of Family Social Sciences and Community Health Sciences, University of Manitoba; St. Amant Research Centre, Winnipeg, Manitoba, Canada; 4Department of Epidemiology and Biostatistics, School of Public Health, School of Public Health, Tabriz University of Medical Sciences, Tabriz, Islamic Republic of Iran
Correspondence: Hamid Allahverdipour
Department of Health Education & Promotion, Faculty of Health Sciences, Tabriz University of Medical Sciences, Attar-e-Neyshabouri Street, Golgasht Street, Tabriz 5165665931, Iran
Tel +98 41 333 44 731
Email [email protected]
Background: Life course gender-role traits and social stereotypes could affect the pattern of medication adherence in old age.
Objectives: The main purpose of this study was to investigate gender based cognitive determinants of medication adherence in a sample of older adults who suffer from at least a chronic condition.
Methods: In this cross-sectional design, 455 older adults participated from five health centers in Tabriz city, Iran from June to August 2017 using a random sampling method. Next, required data about medication adherence, knowledge and beliefs about prescribed medications, perceived self-efficacy in medication adherence, illness perception, and reasons for medication non-adherence were gathered using a structured written questionnaire through face-to-face interviews with the attendees.
Results: Low medication adherence was reported by 54.5% of the study participants. Perceived self-efficacy for medication adherence (OR = 1.04; 95% CI: 1.00, 1.08) and medication adherence reason (OR = 0.96; 95% CI: 0.92, 0.99) were two identified strong predictors of medication adherence among the studied older men. Illness perception (OR = 1.02; 95% CI: 1.00, 1.02) and beliefs toward prescribed medication (OR = 0.95; 95% CI: 0.93, 0.98) were both recognized as the significant predictors of medication adherence in the older women subgroup.
Conclusion: Gender based variations were noted regarding the medication adherence in the studied sample and attributes of cognitive function were the main pinpointed elucidating parameters for the non-conformity. The explicit cognitive processes must be considered in care provision or interventional programs that target medication adherence in older adults.
Keywords: chronic disease, Iran, medication regimen adherence, older adults
Introduction
Medication adherence in older adults is very important for proper treatment or management of chronic diseases and, hence, to reduce the diseases’ complications and improve their quality of life.1 However, adherence to the long-term medication regimen of chronic diseases is a challenging endeavor facing care of older adults.2 It is estimated that on average only about 50% of older adults are fully adhering to the prescribed medications worldwide and the reported adherence rate ranged from 47% to 100% in several studies.3 Non-adherence with the medication regimen could pose unnecessary health care costs4 and increased social and economic costs,5,6 and lead to delayed recovery7 and increased mortality.8 Thorough medication adherence could yield positive health outcomes such as symptom relief, mortality9 and health care cost reduction,10 reduced hospitalizations,11 and more effective management of chronic diseases among older adults.12
Adherence to the medication regimen in the elderly is a complex phenomenon and can be influenced by several factors such as multi-medication,13 development of cognitive impairment, functional limitations, poverty, and transportation limitations.14 Evidence suggests that non-adherence with the medication regimen can also be related to patients’ beliefs and attitudes toward medication.15 Studies have also shown that factors such as medication beliefs, daily forgetfulness, easy access to medications, understanding of disease,16 self-efficacy of medication adherence,17 and knowledge about prescribed medication could impact medication regimen adherence in the older population.18
Life course gender-role traits and social stereotypes were also reported to affect medication adherence.19 While gender based differences regarding perceived barriers to medication adherence were not suggested to exist,9 important differences in the distribution of medicines, metabolism, efficacy, and side effects of prescribed medicines have been reported for both sexes, with a potential effect on medication adherence.20,21 Cognitive factors were shown to act as antecedents for perception of illness, hopefulness for being cured, and beliefs about adherence to the medication regimen but with different patterns in male and female patients.22 Robust research evidence exists to suggest cross-gender variations in understanding the illness, and feeling of the need for taking medication with considerable repercussions on medication adherence among older adults.23,24 Studies on gender-based differences of medication adherence in management of chronic diseases have reached inconsistent results. Some studies reported better medication adherence prescribed for the management of chronic conditions among men,25 and others suggested better medication adherence in older women.26
Investigation of cognitive determinants of medication adherence in older men and women can be helpful to gain a better understanding about the medication non-adherence/adherence spectrum. The min purpose of this study was to investigate gender based cognitive determinants of medication adherence in a sample of older adults with at least a chronic condition.
Methods
Participants And Procedures
The study sample in this descriptive and cross-sectional study consisted of 477 individuals at least 60 years of age. The other inclusion criteria were having at least one chronic disease, taking at least one medication for more than 3 months and absence of any chronic progressive diseases with an effect on memory (e.g. dementia and cancer). The participants were recruited using a random sampling method from five urban health care centers in Tabriz, the capital city of East Azarbaijan province, north west of Iran. A structured written questionnaire was applied to collect data in face-to-face interviews with the attendees from June to August 2017. The interview locations were selected health care centers across the study location. Among the invited old people, only 455 men and women gave their informed consent to participate and, therefore, the participation rate was 95.39% in the study.
The study was approved by the institutional level Board of Trustees on Medical Research Ethics (BoTMRE) at Tabriz University of Medical Sciences. Provision of informed written consent was requested from all of the participants after providing information about the study objectives and procedures and prior to formal commencement of the interviews.
Measures
Demographics
The demographic measures included age (as a continuous variable), sex (male/female), living alone (yes/no), marital status (single, married, widowed, deceased spouse), job status (employed, jobless), and literacy status (illiterate, literate).
Health Status And Access To Medical Services
Health status and access to medical services were assessed using a number of proxy questions, i.e. having medical insurance (yes and no), number of daily-based taken prescribed medications (1 to 4, 5 10, or more) and over-the-counter (OTC) medication use (0, 1, 2, or more). Moreover, in addition to obtaining information about the prescribed drugs, the research team evaluated older patients’ medical records in the health centers, to pinpoint any recommendation or notice representing the respondents’ need for support with medication administration (yes/no).
Medication Knowledge
The medication knowledge questionnaire which had been developed by Williford and Johnson27 was applied to assess the study participants’ knowledge on medication use. The measure consists of five questions based on a 5-point Likert-type scale. These items check individuals’ knowledge about names, frequencies and purpose(s) of use, recommended dose(s), and probable side effects of the received medications. The estimated Cronbach α coefficient for this questionnaire in this study was 0.63, which attested a reliable internal consistency.
Medication Adherence Self-Efficacy Scale (MASES-R)
The Medication Adherence Self-Efficacy Scale-R (MASES-R) was developed by Fernandez et al,28 and contains 13 items to measure patients’ confidence in their ability to take their medications in a variety of situations, e.g. “when they cause some side effects”, “when you come home late from work”, “when you do not have any symptoms”. The MASES-R has a 4-point Likert-type response format and items are scored from 1 (not at all sure) to 4 (extremely sure). The higher score indicates better medication adherence self-efficacy. The calculated Cronbach α for the purpose of this study was 0.91.
Beliefs About Medicines Questionnaire (BMQ)
The Beliefs about Medicines Questionnaire (BMQ) was developed by Horne et al,29 which measures beliefs about medications for treatment of current chronic health conditions, and in this study we used the Persian version of the BMQ.30 The BMQ questionnaire has two domains. The first comprises a five-item scale assessing patients’ beliefs about the necessity of prescribed medication for controlling their illnesses (e.g. “my health at present depends on my medicines”), and five items in the second domain asking about patients' concerns (e.g. “I sometimes worry about becoming too dependent on my medicines”). Participants indicate the degree of agreement on a 5-point scale, ranging from strongly disagree (1) to strongly agree (5). Scores from each domain are summed and, thus, total scores range from 5 to 25 for both the necessity and concern sub-scales respectively. Higher scores indicate stronger beliefs about medications. The calculated Cronbach’s α for beliefs about medications was 0.83, which indicates acceptable internal consistency for the tool.
Medication Adherence Reason Scale (MAR-Scale)
The MAR-Scale was originally developed by Vik et al to determine factors that are related to medication non-adherence in the older population.3 Unni and Farris added five other items to the MAR-Scale, resulting in the 15-item version.31 The revised version was found to be more effective in differentiating non-adherents from adherents based on a 5-point Likert-scale (1 = none of the time, 5 = all of the time) (e.g. “I did not have money to pay for this medicine”). If the respondents answered “none of the time” or “a little of the time” for all 15 items on the MAR-Scale, they were considered adherent to their medication.31 The estimated reliability coefficient for medication adherence reason was α=0.79, indicating acceptable internal consistency.
Medication Adherence
For measuring medication adherence among older adults, a researcher designed questionnaire was used. This questionnaire consists of five items with a yes/no response (e.g. “did you forget to take your pills in the last week”; “did you forget to take your pills in last month”; and “have you ever refused to take your medication based on your own decision”). An estimated reliability coefficient of 0.71 attested to the internal consistency of the medication adherence questionnaire. The total score ranged between 0 and 5, where a higher score indicates better medication adherence. For the purpose of this study, the study participants were classified into two groups (adherent and non-adherent). The non-adherent group consisted of those who scored less than 3; and the adherent group consisted of those who scored 4 and higher.
Brief Illness Perception Questionnaire (Brief IPQ)
In this study, the Farsi version of the Brief Illness Perception Questionnaire (BIPQ), which was adapted to the Persian language,32 was used to assess the cognitive and emotional representations of illnesses among the older adults. This tool was developed by Broadbent et al in 2006.33 The Brief IPQ has nine items, eight scored on a scale from 0 to 10 and one additional question. For example, one of the included items is “how much your illness affects your life?” The questionnaire also contains a question about most important factors that cause the chronic illness. The calculated Cronbach α coefficient for this questionnaire in this study was 0.71. The higher score indicates better illness perception.
Data Analysis
The Statistical Package for Social Sciences (SPSS) v. 17 for Windows (SPSS Inc., Chicago, IL, USA) was used to conduct all statistical analyses. Measures of central tendency and variability were estimated to organize the study data and provide summary measures. The significance level was considered as 0.05. In the following, data analysis was performed in six steps:
1) Normal distribution for cognitive factor scores analyzed with skewness and kurtosis.
2) Demographic characteristics of the medication “non-adherer” and “adherer” among elders analyzed using the chi-square test.
3) Factors associated with medication adherence among male and female elderly analyzed with simple linear logistic regression and univariate analysis. For the purpose of this analysis, two codes (0, 1) were allocated for non-adherence and adherence respectively.
4) Final model of predictors for drugs adherence among male and female elderly analyzed with multiple logistic regression with backward elimination.
5) Correlation between cognitive factors among the studied elderly people analyzed with the Pearson correlation test.
6) Distribution of responses across the MARS for medications among the elderly reported by percent and frequency.
Results
Mean age (SD) of older patients (n=455) was 67.95 (5.24). More than half of the participants were women 239 (52.5), and 67.9% were married. Other older patients’ characteristics are shown in Table 1.
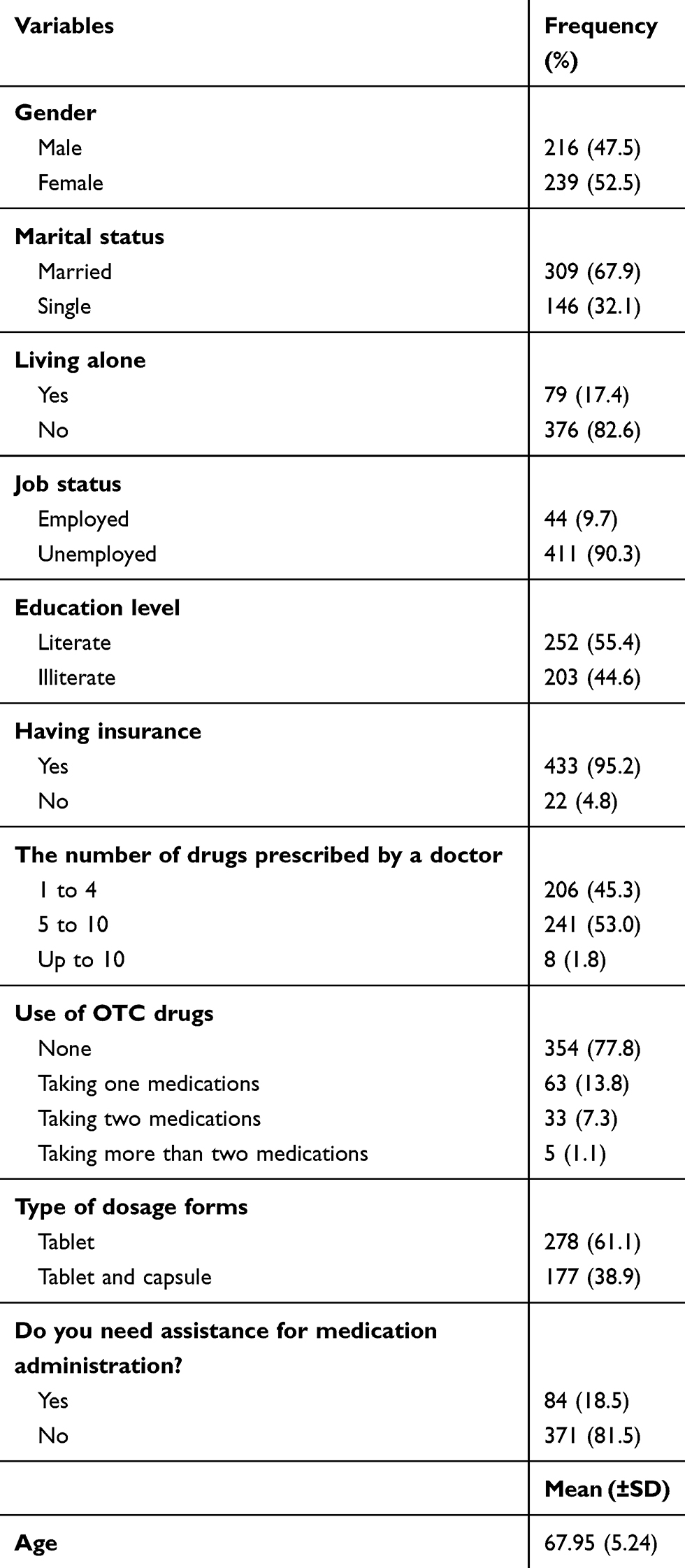 |
Table 1 Characteristics Of The Participants In The Study (n=455) |
Normal Distribution Of Cognitive Factors
The study findings revealed good distributional and psychometric properties for the applied scales. The study data indicated no considerable deviations from normality in skewness and kurtosis, and there was a very satisfactory overall internal consistency in the medication adherence, medication adherence self-efficacy, and medication knowledge, beliefs about medicines, medication adherence reason, and Illness perception (Table 2).
 |
Table 2 Normal Distribution For Cognitive Factors Scores Among Older Patients (n=455) |
Demographic Characteristics Of The Studied Medication “Non-Adherer” And “Adherer” Elder Population
According to the findings, 54.5% of the study participants had low medication adherence scores. The participants’ characteristics and their association with medication adherence, stratified according to participants’ sex, are shown in Table 3. In comparison to the single older adults, the married study attendees had significantly better medication adherence and also having medical insurance was a statistically significant precipitator of medication adherence.
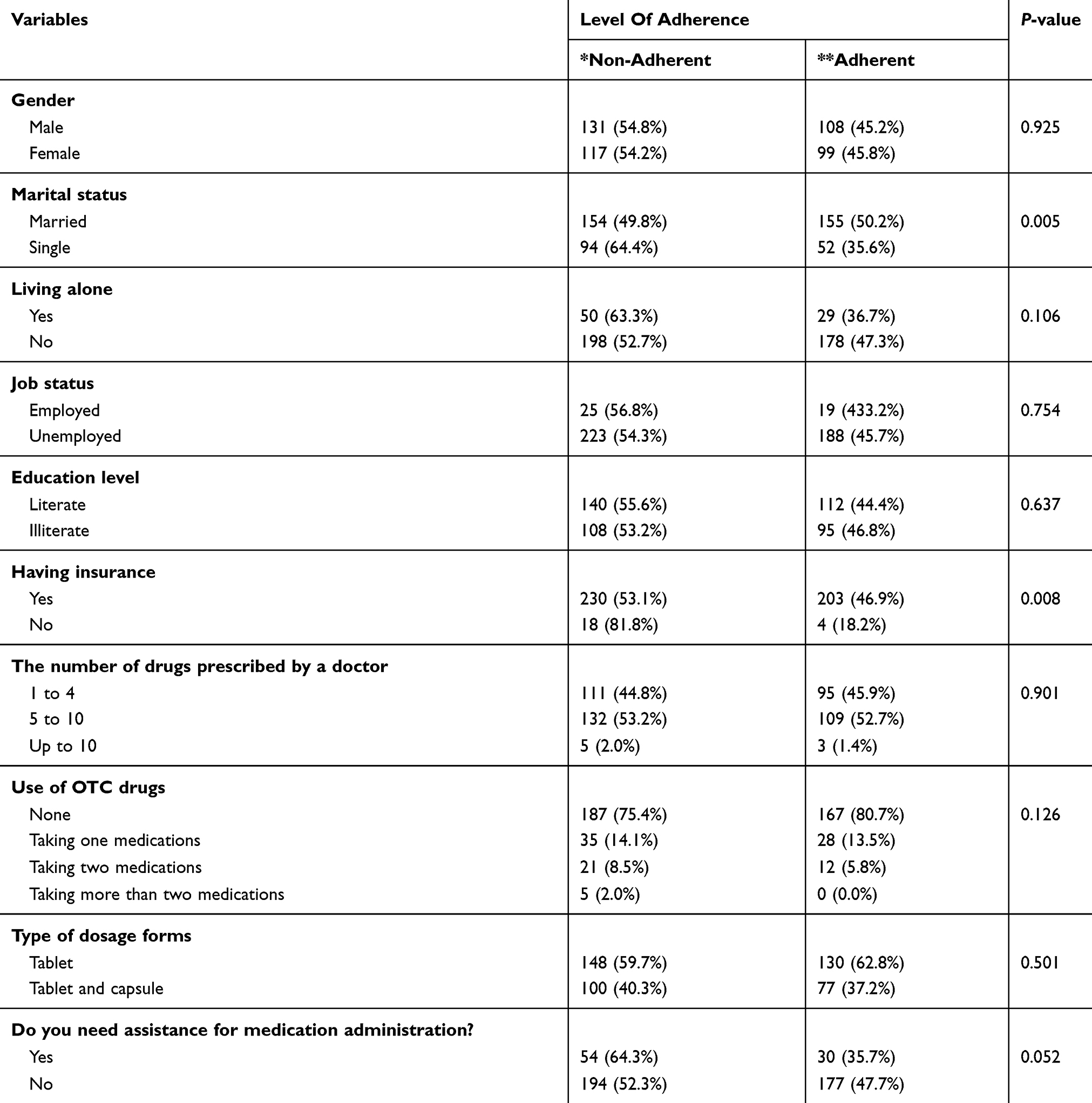 |
Table 3 Demographic Characteristics And Medication By “Non-Adherent” And “Adherent” Among Older Patients (n=455) |
Factors Associated With Drugs Adherence Among Males And Females
The applied simple logistic regression (Table 4) analysis indicated that significantly associated factors with medication adherence among males were marital status, living alone, medication adherence reason, and medication adherence self-efficacy, while among females medication adherence self-efficacy, beliefs about medicines, and medication adherence reason were factors significantly associated with drug adherence.
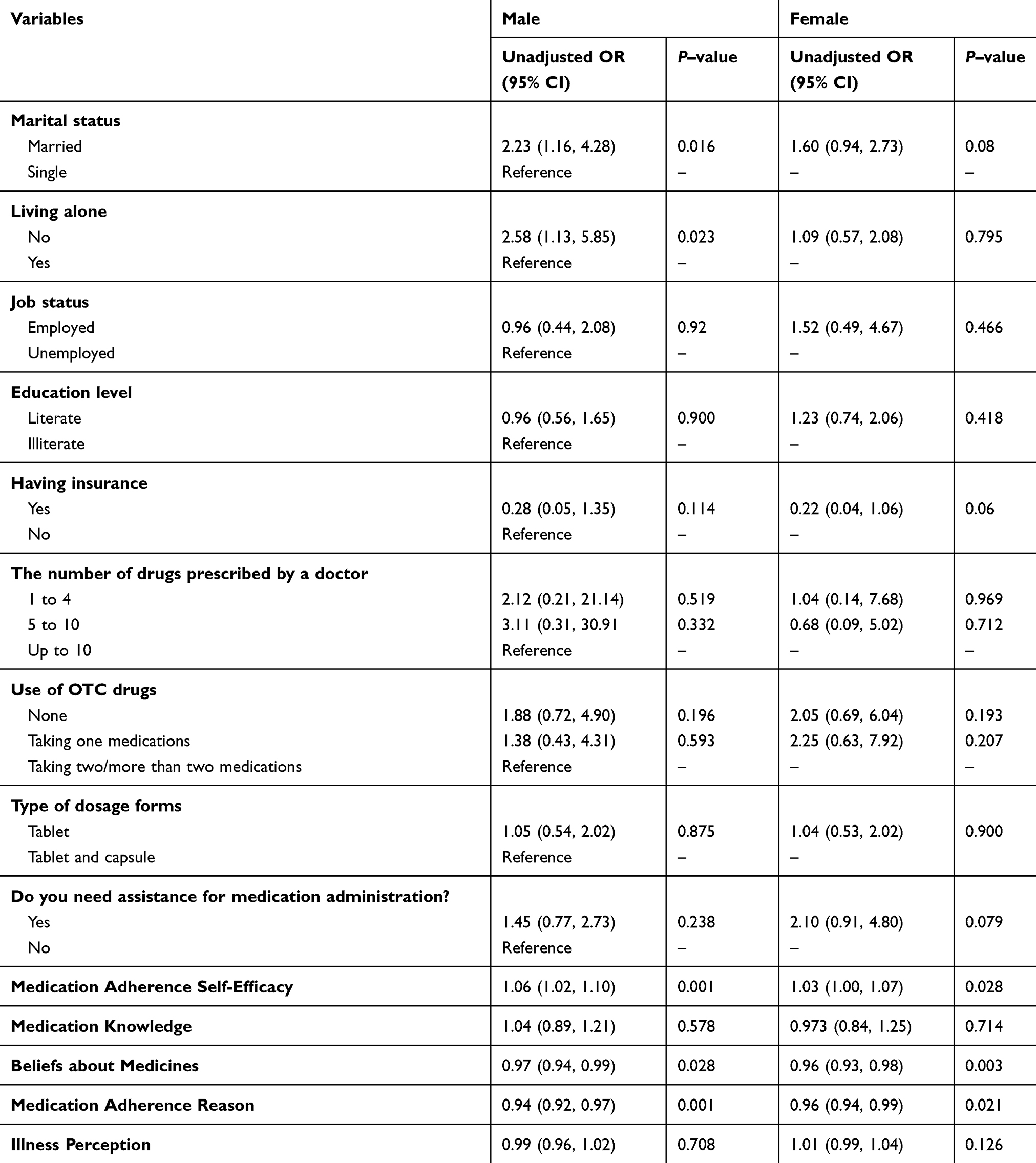 |
Table 4 Factors Associated With Drugs Adherence Among Male And Female Older Patients (n=455) |
Predictors For Drugs Adherence Among Males And Females
In multivariable models (Table 5), factors that were significantly associated with medication adherence scores in the men included marital status, medication adherence self-efficacy, and medication adherence reason. Factors that were significantly associated with medication adherence scores in the women included beliefs about prescribed medications and illness perception.
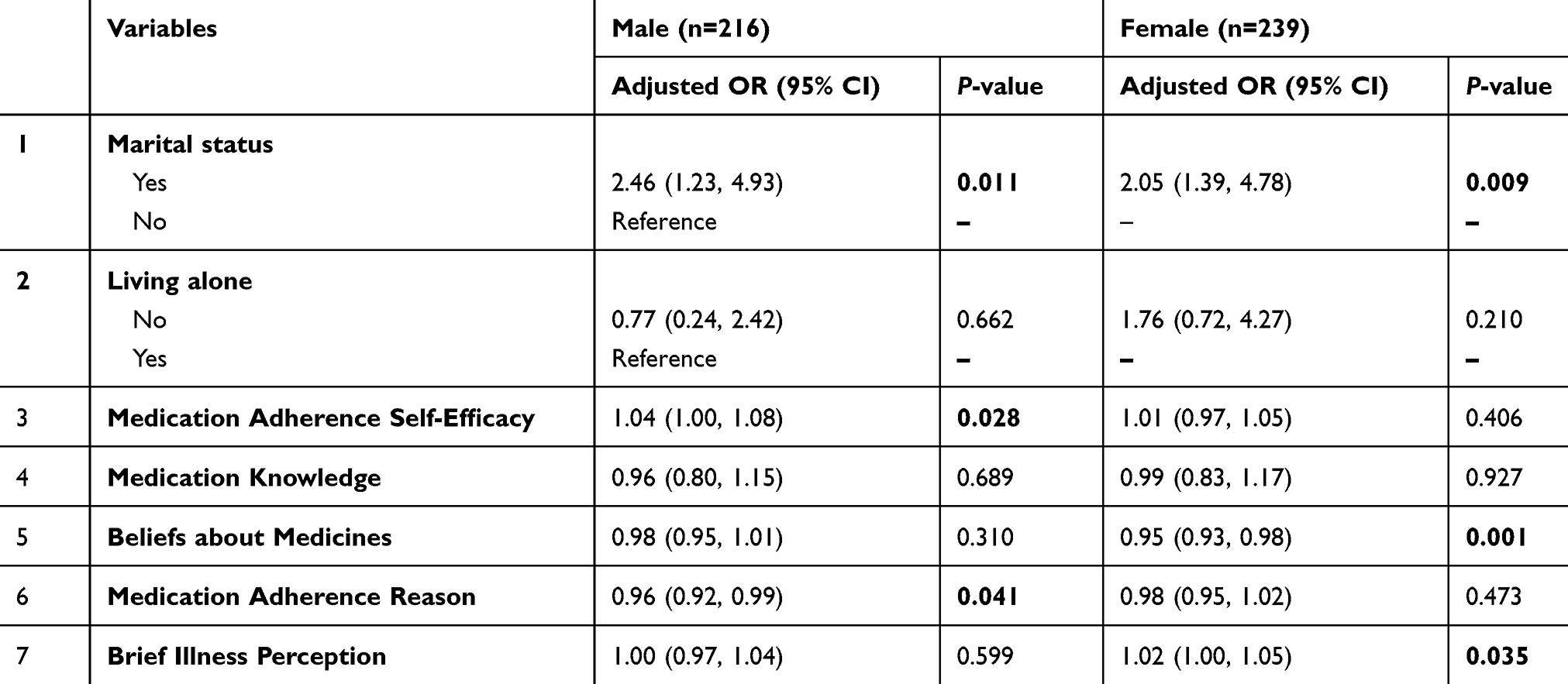 |
Table 5 Final Model Of Predictors For Drugs Adherence Among Male And Female Older Patients (n=455) |
Correlation Between Cognitive Factors
Table 6 presents the correlations among knowledge about prescribed medications, beliefs about medicines, medication adherence reason, medication adherence self-efficacy, and illness perception with medication adherence. Knowledge about prescribed medicines was negatively correlated with belief about medicine (r=−0.248, P <0.01). Additionally, medication adherence self-efficacy was positively correlated with medication adherence (r=0.369, P<0.01) and knowledge about prescribed medications (r=0.125, P<0.01). A significant positive correlation was found between beliefs about prescribed medications and medication adherence reason (r=0.370, P <0.01), and negative correlation with medication adherence self-efficacy (r −0.358, P <0.01). Beliefs about medications also had significantly negative correlation with medication adherence (r −0.248, P <0.01). (r −0.220, P <0.01). Finally, illness perception was positively correlated with beliefs about medications (r=0.274, P <0.01).
 |
Table 6 Person Correlation Between Cognitive Factors Among Older Patients (n=455) |
Distribution Of Responses Across The MARS For Medications
Reasons for medication non-adherence among the study participants were examined using the MAR-Scale. The reported reasons were: embarrassment in taking medications (72.3%), problems in opening the drugs’ containers (70.5%), difficulty swallowing (50.3%), uncertainty about proper administration of the medications (47.3%), stopping medication to see whether it is still needed (47.3%), and being in belief that medication is not needed (43.3%). All of these findings are summarized in Table 7.
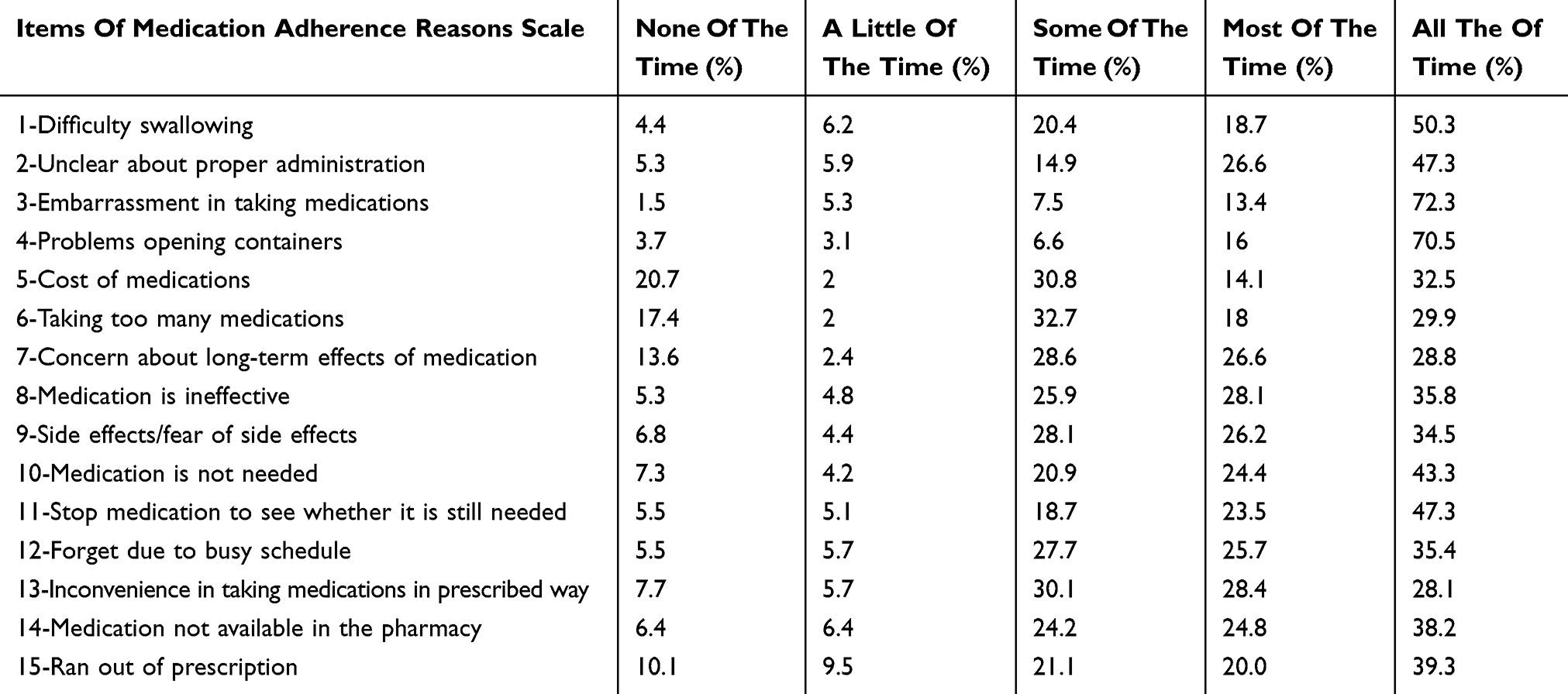 |
Table 7 Distribution Of Responses Across The MARS For Medications Among Older Patients (n=455) |
Discussion
The purpose of this study was to examine gender differences in cognitive determinants of medication adherence among the older population with a history of chronic diseases. The findings showed that two thirds of participants did not have proper medication adherence.
In line with these results, Pasina et al showed that 55.1% and 69.6% of the older studied population had a low adherence rate in the initial follow-ups and 3 months after discharge from the hospital respectively.34 Spiers et al also reported that the rate of non-adherence with the medication regimen among older adults varied between 40 and 75%.35
The main identified factors contributing to the reduced medication adherence among older adults were: forgetfulness, chronic nature of the diseases and consequently taking prescribed medication for a long time, as well as the reduction of the relationship between the old adults and their health care providers.1,36
Chronicity of the diseases among the older population was also suggested to affect the medication adherence rate, i.e. it was indicated that adherence to the medication regimen in patients with acute conditions is better than in those with chronic conditions.37 Moreover, adherence decline in the elderly due to the emergence of early symptoms of cognitive impairment was another reported factor to have a relation with medication non-adherence in the elderly.38 The low level of medication adherence in the older population needs special attention, as older adults not only suffer from several chronic diseases, but they are also more vulnerable to the consequences of medication non-adherence compared to the younger population.
Cross gender, differences in medication adherence were also suggested to be influenced by age, i.e. while in younger adolescents no differences were observed regarding medication adherence, young women indicated much better adherence than young men.39
In this study we did not find significant difference between women and men who had cognitive limitations in terms of medication adherence, which is in line with the results of a number of previous studies.34 Meanwhile, in some studies, medication adherence in older women with chronic conditions was reported to be lower compared to the men who had the same conditions.25,40 Gender based differences of medication adherence are not still conclusive, but it is reported that among women consumption of multiple medications and non-compliance with the recommendations of health care providers are influential factors on women’s decision to not comply with the prescribed medications.25 However, some studies have shown that women are more likely to seek preventive care and treatment than men.41
It is also worthwhile to note that the observed sex-related differences in effects of some medications used by the older population could stem from differences in medication adherence. It was reported for instance that the effect anti-hypertension pills could cast on the sexual function of older men may lead to their low or non-adherence compared to the hypertensive older women.9
Gender based difference in medication adherence could also be related to type of disease amongst men and women. Findings of a study show that women were consistently less likely than men to be adherent with their diabetes and cardiovascular medications.25 This difference may be explained by the fact that women experience more drug side effects than men.42 Therefore, factors associated with adherence to medication can be relatively gender‐specific.
Variations in cognitive pathways between the studied older women and men regarding medication adherence was another finding of the study. Beliefs about use of prescribed medications and understanding of the disease were important predictors of medication adherence in older women. In line with these results, a study by Molloy et al in women showed that people with a better understanding of the disease had a better medication adherence.43 Chen et al also showed that cognitive factors such as understanding of the disease could be a predictor of medication adherence.44 These results may be due to the fact that women mainly are more concerned about the diseases’ threat and thus have a better understanding of their illnesses.45 Patients’ understanding of chronic disease can enhance their ability to manage the disease and, consequently, follow the medication regimen, because illness perception or understanding the current disease is one of the important behavioral determinants of medication adherence.27 Level of understanding about existing disease can also be due to a perceived threat in patients with chronic illness, as studies have shown that people who have a high understanding of illness also have a high perceived threat and, consequently, a better medication adherence profile.46 Appropriate understanding of current chronic illness can also be a useful framework to decide on disease management including medication adherence.47
It was also recommended that understanding of the current disease could lead to active participation of patients in care, acquisition of health behaviors and their medication adherence, better emotional responses to the disease, and appropriate coping strategies with the disease.48
This study's results showed that beliefs related to medication use in older women could predict medication regimen adherence. In line with these results, in the study by Sleath et al, women who had higher scores on drug-related beliefs had a better medication adherence.49 A significant relationship was reported between medication adherence and drug-related beliefs in older adults suffering from chronic diseases in other studies.15,50
Based on the self-regulation and self-management theory a higher level of a disease threat could affect beliefs about medications and thus probability of medication adherence.51 Therefore, it is advisable to improve understanding about a disease threat and thus change patients’ baseline beliefs about prescribed regimens in those educational programs that target older adults with chronic illnesses for an enhanced medication adherence.
Self-efficacy of medication regimen adherence was found in this study to predict medication adherence behaviors both in older men and women. Findings of the study by Sleath et al were also consistent with these findings.49 Self-efficacy as a key factor in self-management of chronic diseases52 was addressed in several studies because patients will not be able to decide consummately even if they have the necessary knowledge and skills in the absence of self-efficacy.53 Self-efficacy as an essential element for initiating and maintaining health-related behaviors and therefore must be considered in interventional programs targeting medication adherence.54 Self-efficacy assessment of the health care clients, especially those older adults suffering from a chronic disease, must be incorporated into routine health care provision planned for the older population.
The perceived reasons for medication non-adherence in older men was another predictive factor that we found in this study while there is little information as well as consensus about determinants of non-adherence specially based on gender type to explain why perceived reasons for medication non-adherence was the predictor of non-adherence among men in this study. In this regard, Unni reported that prescribed medication and adherence to the medication regimen were related to how patients perceive the need for medication.16 However, findings of this study were not consistent with the results of the findings of Thunander et al.55 This inconsistency could be related to the various types of non-adherence behaviors and the reasons for non-adherence amongst men and women. Therefore, older women and men can be having different patterns for their non-adherence behaviors. It seems the inconsistencies across studies’ findings may be attributable to the perception of adherent and non-adherent in the different communities and how to measure the adherence and non-adherence behaviors.
This study has also some limitations. First, a key limitation of the study is the use of self-reported data to measure medication adherence. Second, the cross-sectional study design limited us to examine the association between the study factors and the outcomes of interest. Due to the cross-sectional nature of the data used, examination of a causal relationship was not possible. Future studies based on longitudinal data will be needed to explore medication adherence and related factors among the older population.
Conclusion
Complexity of the cognitive pathways identified in this study among older men and women in their decision to adhere prescribed medication warrant further scrutiny. The observed difference must be considered in routine health care provision for older adults. Such a distinct cognitive route for decision making among old men and women must also be highlighted in educational curriculums for training allied health care professionals, especially those who are training for elderly health care and geriatric care provision. Additionally, because of differences between women and men in their intensity of medication use, adherence to medications, and different received guidance for taking medications, more patient-specific medication protocols and therapeutic management would be needed to enrich better clinical outcomes.
Ethics Approval And Informed Consent
The Ethics Board of the institution Tabriz University of Medical Sciences granted ethical approval of the study (approval number: 58225).
Acknowledgments
This study was part of a MSc. thesis supported by Tabriz University of Medical Sciences. The authors would like to acknowledge all of the older adults who participated in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hsu YH, Mao CL, Wey M. Antihypertensive medication adherence among elderly Chinese Americans. J Transcult Nurs. 2010;21(4):297–305. doi:10.1177/1043659609360707
2. Gautério-Abreu DP, Santos SSC, da Silva BT, Gomes GC, Cruz VD, Tier CG. Prevalence of medication therapy adherence in the elderly and related factors. Rev Bras Enferm. 2016;69(2):335–342. doi:10.1590/0034-7167.2016690217i
3. Vik SA, Maxwell CJ, Hogan DB. Measurement, correlates, and health outcomes of medication adherence among seniors. Ann Pharmacother. 2004;38(2):303–312. doi:10.1345/aph.1D252
4. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
5. Hovstadius B, Petersson G. Non-adherence to drug therapy and drug acquisition costs in a national population - a patient-based register study. BMC Health Serv Res. 2011;11(1):326. doi:10.1186/1472-6963-11-326
6. Krigsman K, Melander A, Carlsten A, Ekedahl A, Nilsson JLG. Refill non-adherence to repeat prescriptions leads to treatment gaps or to high extra costs. Pharm World Sci. 2007;29(1):19–24. doi:10.1007/s11096-005-4797-8
7. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35.
8. Al-Lawati S. A Report on Patient Non-adherence in Ireland. Dublin: Pfizer; 2014.
9. Holt E, Joyce C, Dornelles A, et al. Sex differences in barriers to antihypertensive medication adherence: findings from the cohort study of medication adherence among older adults. J Am Geriatr Soc. 2013;61(4):558–564. doi:10.1111/jgs.12171
10. Lopert R, Shoemaker JS, Davidoff A, et al. Medication adherence and medicare expenditure among beneficiaries with heart failure. Am J Manag Care. 2012;18(9):556–563.
11. Braithwaite S, Shirkhorshidian I, Jones K, Johnsrud M. The role of medication adherence in the US healthcare system. Avalare United States Am. 2013.
12. Cherry SB, Benner JS, Hussein MA, Tang SSK, Nichol MB. The clinical and economic burden of nonadherence with antihypertensive and lipid-lowering therapy in hypertensive patients. Value Health. 2009;12(4):489–497. doi:10.1111/j.1524-4733.2008.00447.x
13. Marcum ZA, Gellad WF. Medication adherence to multi-drug regimens. Clin Geriatr Med. 2012;28(2):287–300. doi:10.1016/j.cger.2012.01.008
14. Gellad WF, Grenard J, McGlynn EA. A Review of Barriers to Medication Adherence: A Framework for Driving Policy Options. CA: RAND Santa Monica; 2009.
15. Horne R, Chapman SCE, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
16. Unni EJ. Development of Models to Predict Medication Non-adherence Based on a New Typology. The University of Iowa; 2008.
17. Son Y, Won MH. Depression and medication adherence among older Korean patients with hypertension: mediating role of self‐efficacy. Int J Nurs Pract. 2017;23:3. doi:10.1111/ijn.12569
18. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
19. Courtenay WH. Constructions of masculinity and their influence on men’s well-being: a theory of gender and health. Soc Sci Med. 2000;50(10):1385–1401. doi:10.1016/S0277-9536(99)00390-1
20. Anderson GD. Gender differences in pharmacological response. Int Rev Neurobiol. 2008;83:1–10.
21. Soldin OP, Mattison DR. Sex differences in pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. 2009;48(3):143–157. doi:10.2165/00003088-200948030-00001
22. Leventhal H, Brissette I, Leventhal EA. The common-sense model of self-regulation of health and illness. Self-Regul Health Illn Behav. 2003;1:42–65.
23. Emilsson M, Berndtsson I, Lötvall J, et al. The influence of personality traits and beliefs about medicines on adherence to asthma treatment. Prim Care Respir J. 2011;20(2):141. doi:10.4104/pcrj.2011.00005
24. Rajpura JR, Nayak R. Role of illness perceptions and medication beliefs on medication compliance of elderly hypertensive cohorts. J Pharm Pract. 2014;27(1):19–24. doi:10.1177/0897190013493806
25. Manteuffel M, Williams S, Chen W, Verbrugge RR, Pittman DG, Steinkellner A. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J Womens Heal. 2014;23(2):112–119. doi:10.1089/jwh.2012.3972
26. Jahanpour F, Rafiei Z, Ravanipour M, Motamed N. Assessment of medication adherence in elderly patients with cardiovascular diseases based on demographic factors in Bushehr City in the year 2013. Jundishapur J Chron Dis Care. 2015;4(3). doi:10.5812/jjcdc
27. Williford SL, Johnson DF. Impact of pharmacist counseling on medication knowledge and compliance. Mil Med. 1995;160(11):561–564.
28. Fernandez S, Chaplin W, Schoenthaler AM, Ogedegbe G. Revision and validation of the medication adherence self-efficacy scale (MASES) in hypertensive African Americans. J Behav Med. 2008;31(6):453–462. doi:10.1007/s10865-008-9170-7
29. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
30. Mostafavi F, Najimi A, Sharifirad G, Golshiri P. Beliefs about medicines in patients with hypertension: the instrument validity and reliability in Iran. Mater Sociomed. 2016;28(4):298. doi:10.5455/msm.2016.28.298-302
31. Unni EJ, Farris KB. Development of a new scale to measure self-reported medication nonadherence. Res Soc Adm Pharm. 2015;11(3):e133–43. doi:10.1016/j.sapharm.2009.06.005
32. Bazzazian S, Besharat MA. Reliability and validity of a Farsi version of the brief illness perception questionnaire. Procedia-Social Behav Sci. 2010;5:962–965. doi:10.1016/j.sbspro.2010.07.217
33. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
34. Pasina L, Brucato AL, Falcone C, et al. Medication non-adherence among elderly patients newly discharged and receiving polypharmacy. Drugs Aging. 2014;31(4):283–289. doi:10.1007/s40266-014-0163-7
35. Spiers MV, Kutzik DM, Lamar M. Variation in medication understanding among the elderly. Am J Health Pharm. 2004;61(4):373–380. doi:10.1093/ajhp/61.4.373
36. Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. 2011;26(3):155. doi:10.5001/omj.2011.38
37. Slejko JF, Ho M, Anderson HD, Nair KV, Sullivan PW, Campbell JD. Adherence to statins in primary prevention: yearly adherence changes and outcomes. J Manag Care Pharm. 2014;20(1):51–57.
38. Austin J, Klein K, Mattek N, Kaye J. Variability in medication taking is associated with cognitive performance in nondemented older adults. Alzheimer’s Dement Diagn Assess Dis Monit. 2017;6:210–213.
39. Boucquemont J, Pai ALH, Dharnidharka VR, Hebert D, Furth SL, Foster BJ. Gender differences in medication adherence among adolescent and young adult kidney transplant recipients. Transplantation [Internet]. 2019;103(4). Available from: https://journals.lww.com/transplantjournal/Fulltext/2019/04000/Gender_Differences_in_Medication_Adherence_Among.31.aspx.
40. Segarra I, Modamio P, Fernandez C, Marino EL. Sex-divergent clinical outcomes and precision medicine: an important new role for institutional review boards and research ethics committees. Front Pharmacol. 2017;8:488. doi:10.3389/Fphar.2017.00488
41. Vaidya V, Partha G, Karmakar M. Gender differences in utilization of preventive care services in the United States. J Women’s Health. 2012;21(2):140–145. doi:10.1089/jwh.2011.2876
42. Zopf Y, Rabe C, Neubert A, et al. Women encounter ADRs more often than do men. Eur J Clin Pharmacol. 2008;64(10):999. doi:10.1007/s00228-008-0494-6
43. Molloy GJ, Gao C, Johnston DW, et al. Adherence to angiotensin-converting-enzyme inhibitors and illness beliefs in older heart failure patients. Eur J Heart Fail. 2009;11(7):715–720. doi:10.1093/eurjhf/hfp059
44. Chen SL, Tsai JC, Lee WL. The impact of illness perception on adherence to therapeutic regimens of patients with hypertension in Taiwan. J Clin Nurs. 2009;18(15):2234–2244. doi:10.1111/j.1365-2702.2008.02706.x
45. Weinman J, Petrie KJ. Illness Perceptions: A New Paradigm for Psychosomatics? Elsevier; 1997.
46. Unni E, Shiyanbola OO. Clustering medication adherence behavior based on beliefs in medicines and illness perceptions in patients taking asthma maintenance medications. Curr Med Res Opin. 2016;32(1):113–121. doi:10.1185/03007995.2015.1105204
47. Vélez‐Vélez E, Bosch RJ. Illness perception, coping and adherence to treatment among patients with chronic kidney disease. J Adv Nurs. 2016;72(4):849–863. doi:10.1111/jan.2016.72.issue-4
48. Woith WM, Rappleyea ML. Emotional representation of tuberculosis with stigma, treatment delay, and medication adherence in Russia. J Health Psychol. 2016;21(5):770–780. doi:10.1177/1359105315569620
49. Sleath B, Carpenter DM, Blalock SJ, et al. Development of a new diabetes medication self-efficacy scale and its association with both reported problems in using diabetes medications and self-reported adherence. Patient Prefer Adherence. 2016;10:1003. doi:10.2147/PPA.S101349
50. Jamous RM, Sweileh WM, Taha ASE-DA, Zyoud SH. Beliefs about medicines and self-reported adherence among patients with chronic illness: a study in Palestine. J Fam Med Prim Care. 2014;3(3):224. doi:10.4103/2249-4863.141615
51. Horne R, Weinman J. Self-regulation and self-management in asthma: exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol Health. 2002;17(1):17–32. doi:10.1080/08870440290001502
52. Du S, Yuan C. Evaluation of patient self-management outcomes in health care: a systematic review. Int Nurs Rev. 2010;57(2):159–167. doi:10.1111/j.1466-7657.2009.00794.x
53. Bandura A. Perceived self-efficacy in cognitive-development and functioning. Educ Psychol. 1993;28(2):117–148. doi:10.1207/s15326985ep2802_3
54. Tussing L, Chapman-Novakofski K. Osteoporosis prevention education: behavior theories and calcium intake. J Am Diet Assoc. 2005;105(1):92–97. doi:10.1016/j.jada.2004.12.006
55. Thunander Sundbom L, Bingefors K. Women and men report different behaviours in, and reasons for medication non-adherence: a nationwide Swedish survey. Pharm Pract (Granada) [Internet]. 2012;10(4):207–221. doi:10.4321/S1886-36552012000400005
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.