Back to Journals » Vascular Health and Risk Management » Volume 22
Gender and Age Differences in Hypertension Screening and Cardiovascular Risk Factors in Rural Kazakhstan
Authors Baglanova L, Junusbekova G, Tundybayeva M ![]() , Mukhtarkhanova D, Yegorova Y
, Mukhtarkhanova D, Yegorova Y
Received 19 October 2025
Accepted for publication 13 January 2026
Published 23 January 2026 Volume 2026:22 575431
DOI https://doi.org/10.2147/VHRM.S575431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Lyazat Baglanova,1 Gulnara Junusbekova,2 Meiramgul Tundybayeva,2 Dilyara Mukhtarkhanova,2 Yelena Yegorova1
1Cardiology Department, Kazakh-Russian Medical University, Almaty, Kazakhstan; 2Cardiology department, Asfendiyarov Kazakh National Medical University, Almaty, Kazakhstan
Correspondence: Meiramgul Tundybayeva, Department of cardiology, Asfendiyarov Kazakh National Medical University, 94 Tole Bi Street, Almaty, 050000, Kazakhstan, Email [email protected]; [email protected]
Purpose: Hypertension remains a major public health challenge with low awareness and control rates. This study aims to assess its prevalence among rural residents in Kazakhstan.
Methods: A cross-sectional study was conducted in May 2025 among adults in the Enbekshikazakh district using a validated questionnaire adapted from the May Measurement Month survey. Data on demographics, risk factors, and clinical indicators were collected. Statistical analyzes included Chi-square and t-tests, with significance set at p < 0.05.
Results: Among 1200 participants (550 males, 650 females), significant gender differences were observed across behavioral and clinical factors. Males reported higher rates of smoking, e-cigarette and alcohol use, and caffeine intake (p=0.001), while females were more engaged in healthcare and preventive medication use. Hypertension diagnosis and treatment were more frequent among females, but males showed higher measured blood pressure values (p< 0.001). Although BMI and anthropometric measures were similar, abdominal obesity was more prevalent in females (73.0% vs 40.4%, p=0.001). These findings indicate distinct gender patterns in lifestyle behaviors, cardiovascular risk factors, and health service utilization within the study population.
Conclusion: Males exhibited higher cardiovascular risk behaviors and blood pressure, while females showed greater healthcare engagement and abdominal obesity, highlighting the need for gender-specific strategies in cardiovascular disease prevention and management.
Keywords: gender differences, age differences, rural area, cardiovascular risk, hypertension, screening, Kazakhstan
Introduction
Hypertension remains a major global public health challenge, affecting approximately 1.4 billion adults aged 30–79 years worldwide in 2024, which accounts for nearly 33% of this age group. Notably, two-thirds of these individuals reside in low- and middle-income countries (LMICs), where health systems often face significant constraints. Despite being a leading contributor to premature mortality, an estimated 44% (around 600 million people) remain unaware of their hypertensive status, and only 23% achieve effective blood pressure control.1 The economic burden of hypertension is substantial across countries at all income levels, driven largely by healthcare expenditures and productivity losses. Estimates range from significant GDP impacts in middle-income countries to high per-patient costs and pronounced disparities in high-income settings.2–5
Early detection through hypertension screening is a cornerstone of cardiovascular disease prevention, particularly in resource-limited settings where delayed diagnosis contributes to avoidable complications. Screening is especially relevant in rural populations, where access to healthcare services is often fragmented and preventive care utilization remains suboptimal.6,7
Sex- and age-related differences play a critical role in hypertension detection and management. Evidence suggests that male and female differ in health-seeking behaviors, exposure to behavioral risk factors, biological susceptibility, and treatment adherence, all of which can influence hypertension awareness and control. Similarly, age-related disparities are particularly important in rural settings, where older adults may experience cumulative cardiovascular risk, limited mobility, and reduced access to routine screening, while younger adults often remain under-screened due to low perceived risk.8,9 Understanding these differences is essential for designing targeted and efficient screening strategies.
In Kazakhstan, hypertension represents a growing public health concern. Previous studies reported a prevalence of 37% in 2021, increasing to 45% in 2022–2023, accompanied by low levels of awareness and blood pressure control.10 However, existing evidence has largely focused on urban populations, leaving a critical gap in understanding hypertension burden, screening outcomes, and demographic disparities in rural areas.11 This lack of rural, sex-specific, and age-stratified data constitutes an important research gap, limiting the ability of primary healthcare (PHC) systems to tailor hypertension screening and prevention strategies to local population needs.
In this context, we focused on the rural population of the Enbekshikazakh district in the Almaty region, one of the most densely populated districts with approximately 1.5 million residents as of 2025. The district’s PHCr, located in Esik, has been designated by the WHO Regional Office for Europe as a demonstration platform for sustainable, patient-centered PHC models.10 This platform exemplifies innovative approaches to managing noncommunicable diseases, including multidisciplinary teamwork and community engagement, and serves as a training hub for health professionals and policymakers from other countries.12
The objective of this study was to conduct hypertension screening among rural residents in Enbekshikazakh district and to generate evidence-based recommendations for PHC managers to enhance current practices and inform future health policies.
Materials and Methods
A cross-sectional study was conducted using a structured questionnaire adapted from the May Measurement Month 2025 survey.13 Inclusion criteria were adults aged ≥18 years residing in the Enbekshikazakh district who were able to provide informed consent and participate in an interview and physical measurements. Exclusion criteria included pregnancy, severe acute illness at the time of screening, cognitive impairment precluding reliable responses, and refusal to participate. The questionnaire was translated into Russian and Kazakh languages for use among the local population. The translation followed a forward–backward translation procedure performed by bilingual experts, with discrepancies resolved through consensus to ensure semantic and conceptual equivalence. Content validity was reviewed by two cardiologists and one public health specialist, and the tool was pilot tested among 10 participants. The included questionnaire sections on demographic information, behavioral risk factors (smoking status, alcohol consumption, and physical activity), and clinical indicators such as body mass index (BMI), blood pressure (BP), and waist circumference. Smoking and alcohol use were evaluated using self-reported standardized questions (current, former, or never use), while physical activity was evaluated based on frequency and duration of moderate-to-vigorous activity per week. BMI was categorized as normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2).14,15 BP and heart rate were measured three times using validated automated devices (OMRON, Kyoto, Japan) by trained healthcare volunteers following standardized measurement protocols.16
The survey was conducted in four areas of the Enbekshikazakh district among participants aged 18 years and older. Informed consent was obtained from all participants prior to study participation, including an explanation of the study’s purpose, procedures, and voluntary nature. Data collection took place in May 2025, during World Hypertension Month, and each interview lasted approximately 40 minutes. Screening was carried out in four types of settings: At participants’ homes – district nurses from the PHC informed residents in advance that researchers would be visiting and obtain preliminary verbal consent; at workplaces – permission was obtained from employers to conduct screenings among staff members during working hours; at pharmacies – visitors were invited to participate in the study during their visits; in hospitals – with permission from hospital administrators, inpatients and outpatients were invited to take part. The screening was conducted by a team of five individuals, including cardiologists and PhD students from the university.
Ethical Considerations
The study was approved by the Local Ethics Committee of Kazakh-Russian Medical University, Kazakhstan (Protocol No. 18 (99), 5 January 2023). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional ethics committee and with the principles of the Declaration of Helsinki.
Statistical Analysis
Descriptive statistics were used to summarize participants’ sociodemographic characteristics, behavioral risk factors, clinical indicators, and anthropometric measurements. Comparisons between males and females, as well as across age groups, were conducted using the Chi-square (χ2) test for categorical variables and the independent-samples t-test or one-way ANOVA for continuous variables, as appropriate. A p-value < 0.05 was considered statistically significant. Anthropometric (age, BMI, waist and hip circumference) and hemodynamic (systolic and diastolic BP, pulse rate) parameters were analyzed as continuous variables and presented as mean ± standard deviation (SD). Gender differences were assessed using independent-samples t-tests.
Although a formal a priori sample size calculation was not performed, the achieved sample size exceeded 1,000 participants, which is well above the minimum sample size of approximately 384 individuals required for cross-sectional prevalence studies assuming a 95% confidence level and a 5% margin of error. Therefore, the sample size was sufficient to ensure stable estimates of hypertension prevalence and to allow meaningful comparisons across sex and age groups. Nevertheless, given the non-probability sampling approach, the findings should be interpreted with caution regarding population-wide generalizability.
Results
Sociodemographic Characteristics and Behavioral Risk Factors
Among 1200 participants (550 males, 650 females), males were more concentrated in Teskensu and more often screened at home, while females were screened mainly in hospitals (both p=0.001). Risk behaviors were significantly more prevalent among males, who demonstrated substantially higher rates of tobacco use (52.2% vs 4.2%), e-cigarette use (8.7% vs 0.8%), alcohol consumption (26.2% vs 5.8%), and frequent caffeine intake (p=0.001), Table 1.
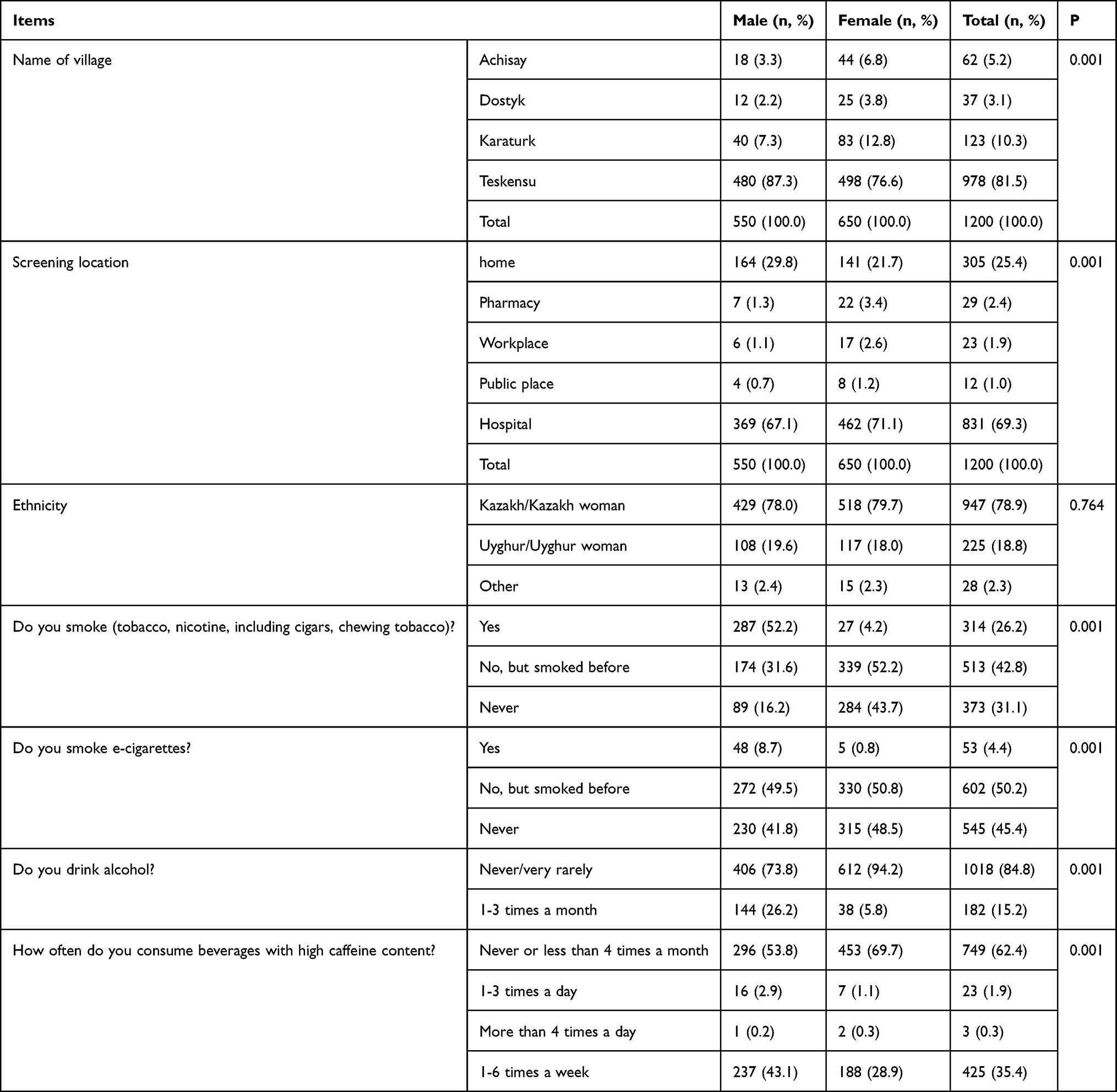 |
Table 1 Gender Differences in Sociodemographic Characteristics and Health-Related Behaviors of Study Participants |
Blood Pressure Screening, Diagnosis, and Medication Use
A higher proportion of males (49.1%) than females (43.2%) reported never having their BP measured (p=0.001), while females were more likely to have been screened within the past 12 months (30.8% vs 20.9%), indicating greater health service engagement among them. Hypertension diagnosis was more prevalent among females (17.4%) than males (11.1%) (p=0.002), and a similar pattern was seen in antihypertensive medication use (10.0% vs 4.7%, p=0.001). Females also reported higher use of preventive cardiovascular medications, including statins (2.0% vs 0.4%, p=0.011) and aspirin (7.7% vs 3.5%, p=0.002), Table 2.
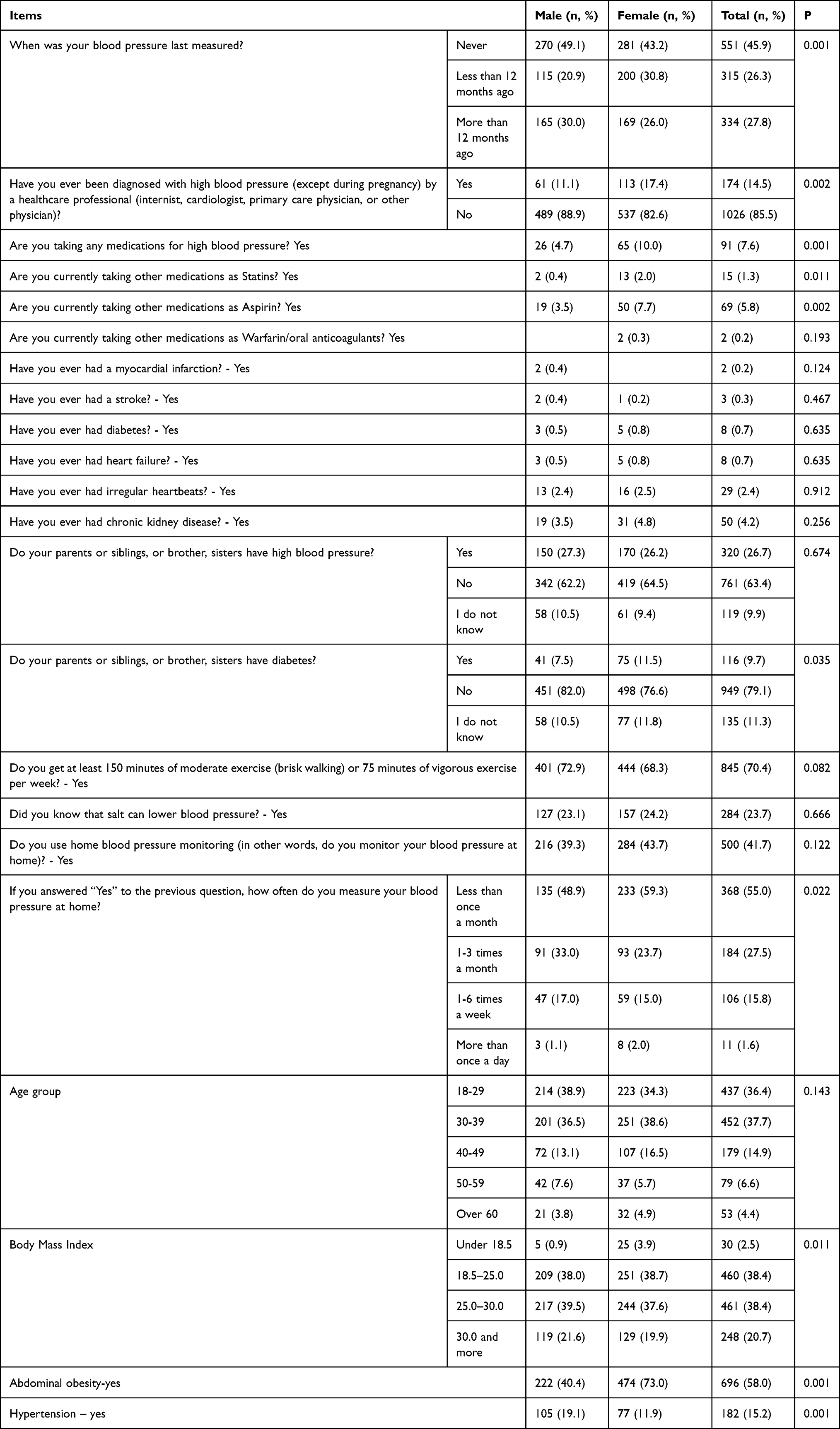 |
Table 2 Gender Differences in Blood Pressure Monitoring, Hypertension Diagnosis, and Cardiovascular Medication Use |
Histories of myocardial infarction, stroke, diabetes, heart failure, arrhythmia, and chronic kidney disease were infrequent and did not differ significantly by sex (all p > 0.05), reflecting the relatively young age of the screened population.
Anthropometric Characteristics and Blood Pressure Levels
When BMI was analyzed as a categorical variable, males were more frequently classified as overweight or obese (BMI ≥25 kg/m2), whereas underweight status was more common among females (3.9% vs 0.9%; p = 0.011) (Table 2). In contrast, mean BMI analyzed as a continuous variable did not differ significantly between sexes (27.78 ± 18.45 kg/m2 in males vs 26.77 ± 12.61 kg/m2 in females; p = 0.262) (Table 3). This indicates similar average BMI values despite differences in BMI category distribution. Abdominal obesity showed a pronounced gender disparity, being significantly more prevalent among females than males (73.0% vs 40.4%; p = 0.001). Mean age, waist circumference, and hip circumference were comparable between males and females (all p > 0.05). However, males consistently exhibited higher systolic and diastolic blood pressure values across all three measurements. The average of three readings confirmed higher SBP (121.0 ± 21.15 vs 115.9 ± 13.84 mmHg) and DBP (79.7 ± 13.55 vs 77.06 ± 9.67 mmHg) in males compared with females (both p < 0.001), while pulse rate did not differ significantly (Table 3).
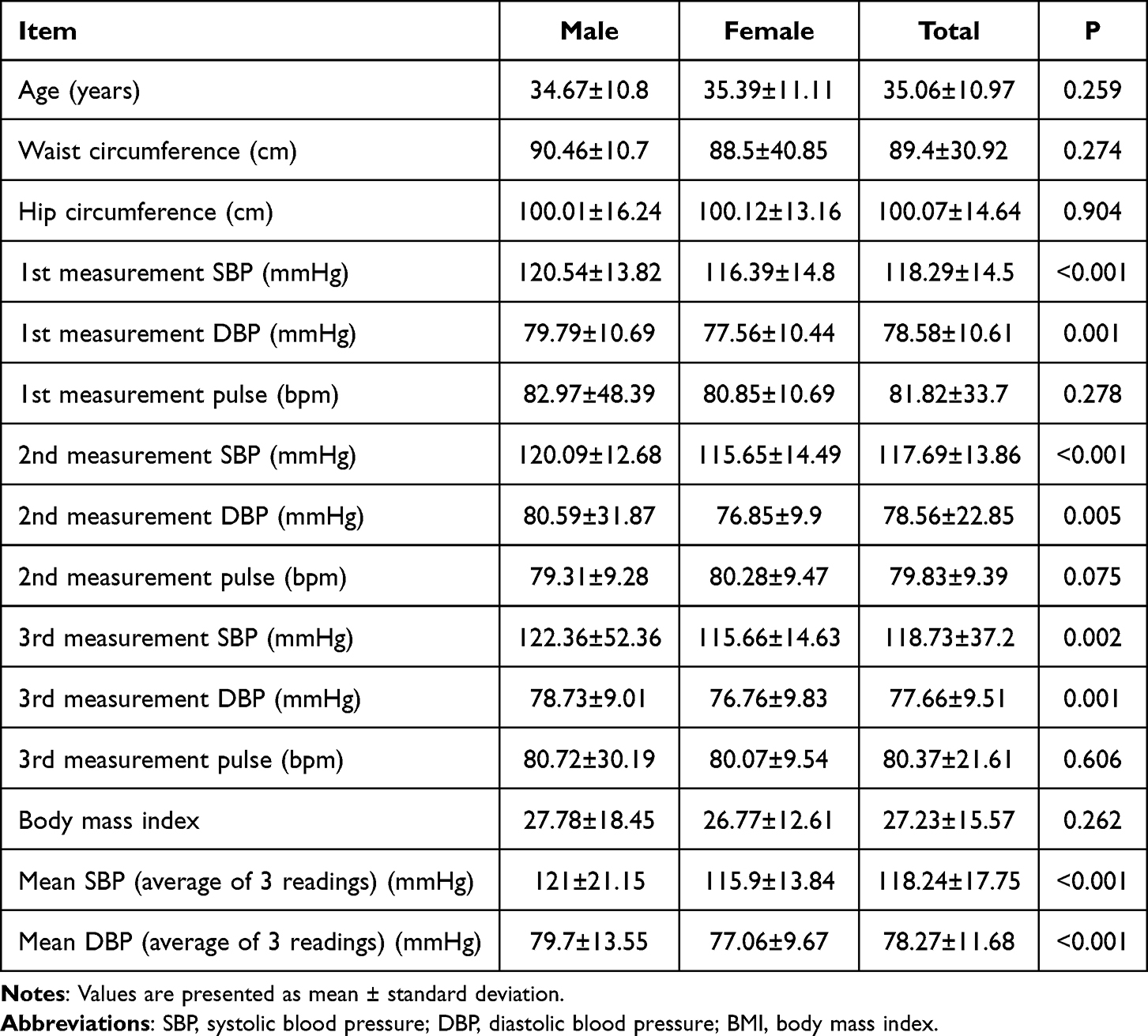 |
Table 3 Gender Differences in Anthropometric and Hemodynamic Parameters |
Age-Related Patterns
Risk behaviors such as e-cigarette use, alcohol consumption, and caffeine intake decreased significantly with age (all p = 0.001). In contrast, hypertension prevalence increased markedly with age, rising from 3.2% among participants aged 18–29 years to 49.1% among those aged ≥60 years, Table 4. Correspondingly, antihypertensive medication use increased from 1.6% to 41.5%, while statin and aspirin use also rose significantly with age (Table 5). Despite this increase, overall use of preventive cardiovascular medications remained low, particularly among younger and middle-aged adults.
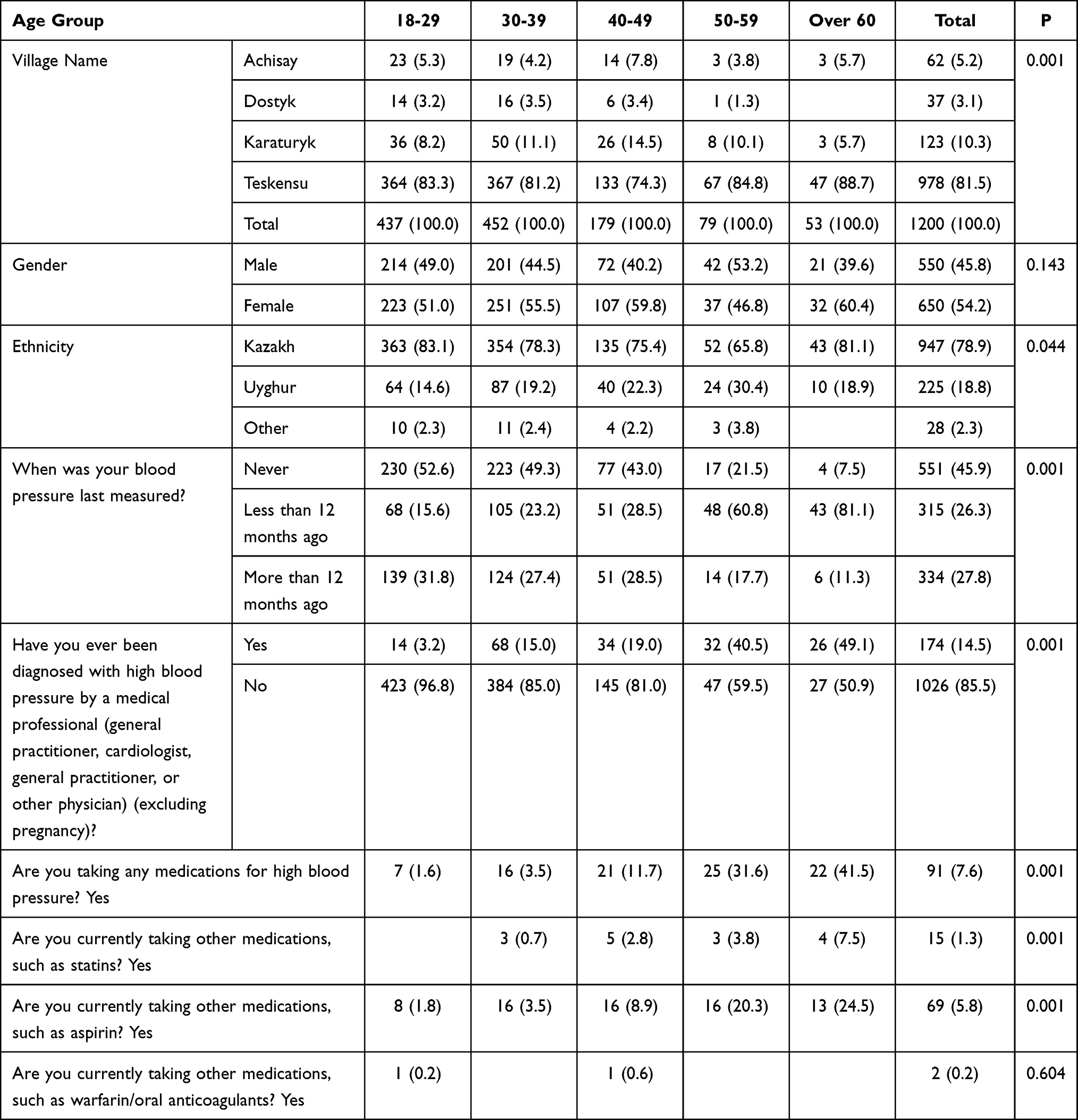 |
Table 4 Distribution of Respondents by Age, Gender, Ethnicity, and Health Indicators Related to Blood Pressure |
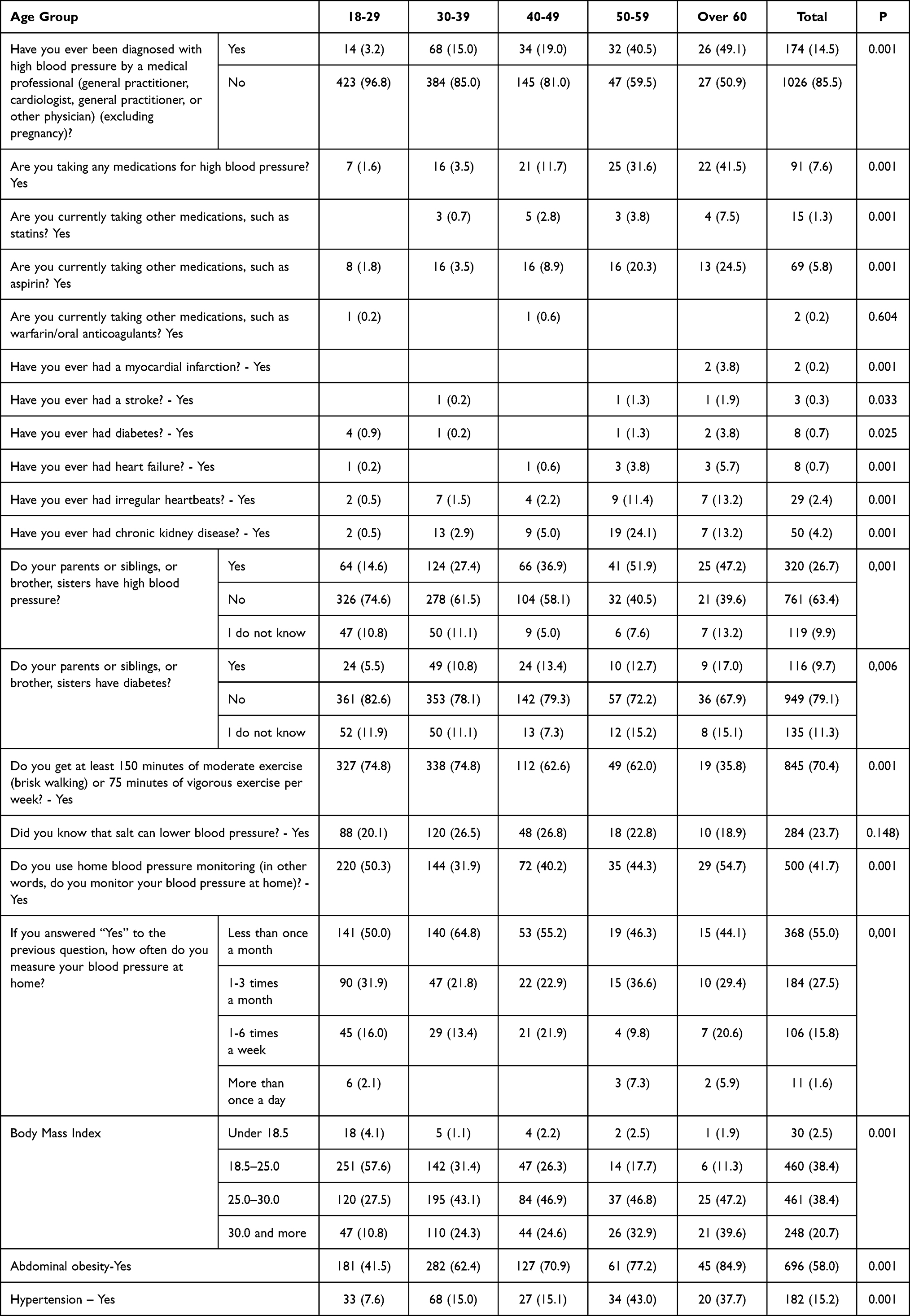 |
Table 5 Age Differences in Blood Pressure Monitoring, Hypertension Diagnosis, and Cardiovascular Medication Use |
Discussion
We found that in the rural population, males demonstrated greater engagement in unhealthy behaviors and exhibited higher systolic and diastolic BP, whereas females showed greater healthcare participation. A previous study in Kazakhstan reported similar findings, showing increasing prevalence, incidence, and mortality of hypertension, with males, older adults, and individuals of Russian or other ethnicities facing significantly higher mortality risks than females, younger individuals, and ethnic Kazakhs.17 The lower prevalence of unhealthy behaviors among females in our study may be attributed to their greater engagement with healthcare services, including more frequent BP monitoring and higher use of preventive medications. Similarly, a 10-year cohort study of 2,688 adults found that belief in heart disease preventability predicted lower CHD incidence among women (HR = 0.36, p <0.001), partly mediated by reduced smoking, underscoring the stronger protective effects of preventive health beliefs in females.18 Moreover, we revealed that vaping was primarily a behavior of younger adults. Similarly, in the US, e-cigarette use increased across most age and smoking groups, with the sharpest rise among younger adults—particularly never smokers (from 1.3% to 3.3%) and recent quitters (from 9.1% to 19.2%).19 This suggests that e-cigarettes are becoming a primary source of nicotine initiation among young people, rather than solely a tool for smoking cessation.
Findings from our screening program emphasize the need for gender-specific health interventions targeting behavioral and cardiovascular risk factors. For example, a study among male employees in British Columbia showed that although most men expressed strong interest in workplace health promotion (85–91%), many demonstrated suboptimal health behaviors—only 62% met physical activity guidelines, 29% consumed sufficient fruits and vegetables, and 14% smoked.20 Given similar patterns observed in rural Kazakhstan, primary healthcare facilities could collaborate with local employers to implement workplace-based health promotion programs aimed at improving lifestyle behaviors and reducing cardiovascular risk.
We found that although overall BMI was similar between genders, abdominal obesity was significantly more prevalent among females. Previous studies have also shown that even at the same BMI, health risks vary with visceral fat levels, as abdominal obesity increases the risk of metabolic syndromes such as hypertension, diabetes, cardiovascular disease, and fatty liver disease.21 The high prevalence of abdominal obesity among females in our study may reflect sex-specific fat distribution patterns, hormonal influences, and lifestyle factors, as well as potential differences in waist circumference sensitivity across populations. Similar patterns have been reported in other Central Asian and LMIC settings. Globally, obesity rates continue to rise—in 2021, over 42% of Americans were obese or overweight, compared with approximately 34–38% in Korea and 59% in Europe.22–24 Importantly, in our relatively young population, obesity—particularly central obesity—was already highly prevalent among adults aged 30–49 years, with approximately 40% overweight, 24% obese, and abdominal obesity affecting more than half of participants. This early accumulation of excess body weight indicates an emerging cardiovascular risk profile well before older adulthood.
The extremely low prevalence of self-reported chronic conditions such as myocardial infarction (0.2%), diabetes (0.7%), and heart failure (0.7%) likely reflects both the young age structure of the study population and potential underdiagnosis in rural settings, where access to diagnostic services and routine follow-up may be limited. This interpretation is supported by the high proportion of participants—particularly males—who reported never having had their BP measured. Consistent with this, antihypertensive and statin use remained low even among older adults. This finding likely reflects gaps in hypertension awareness, delayed diagnosis, and barriers related to healthcare access and medication affordability in rural areas, rather than a true absence of need. Similar patterns of under-treatment have been reported in rural and resource-limited settings internationally.
Both genders demonstrated limited awareness of salt reduction as a preventive measure for hypertension, indicating a critical gap in public health education. Reducing salt intake to below 5 g/day, as recommended by WHO, is proven to significantly improve cardiovascular health. Evidence from Finland, the UK, and recent studies, including a meta-analysis of 10 trials and a large-scale intervention in China, shows that behavioral and community-based salt reduction programs effectively decrease urinary sodium, increase potassium, and lower BP.25–27
The high prevalence of hypertension in Kazakhstan may be linked to rural diets that remain largely traditional and grain-based, with limited diversification due to lower income levels and restricted access to varied foods.28 Excessive salt consumption—averaging 17 g/day, nearly four times the WHO-recommended limit—poses a major health risk. In response, the government, in partnership with WHO and UNICEF, has launched a 2022–2025 nutrition roadmap aimed at reducing salt, sugar, and trans fats to lower cardiovascular disease burden.29
Finally, studies shows that young adult males demonstrated higher engagement in cardiovascular and multiple health risk behaviors, including unhealthy diets and substance use, despite greater physical activity, while females exhibited overall healthier lifestyles.8,30,31 Additionally, flourishing—high levels of hedonic and eudaimonic wellbeing—was associated with fewer risky behaviors and greater self-care among Australian emerging adults, suggesting that promoting wellbeing may help reduce unhealthy behaviors and support sustainable lifestyle improvements.32
Limitations and Future Steps
This study has several limitations. First, its cross-sectional design prevents the establishment of causal relationships between risk factors and hypertension, limiting interpretation to associations only. Second, self-reported data on behaviors such as smoking, alcohol use, diet, and medication adherence may be subject to recall and social desirability bias. Third, the study was conducted in one district (Enbekshikazakh, a rural district), which may limit the generalizability of findings to other regions of Kazakhstan with different socioeconomic or cultural contexts. Fourth, salt intake and dietary patterns were not assessed through biochemical or dietary recall methods, which would provide more accurate insights into sodium consumption and its relationship with BP. Lastly, while BP measurements were standardized and performed by trained personnel, single-visit assessments may not fully capture variability in individual BP levels.
Future policy efforts in rural Kazakhstan should prioritize community-based health education and preventive care to address hypertension and unhealthy lifestyles. Rural PHC should conduct regular BP screenings, provide nutritional counseling, and promote salt reduction awareness. Targeted health campaigns using local media and community leaders can enhance understanding of excessive salt intake risks, while gender-specific interventions should focus on reducing males’ unhealthy behaviors and integrating cardiovascular care into females’ reproductive health services. Future studies should adopt longitudinal designs, include biochemical measures such as urinary sodium, and cover diverse regions to better identify hypertension determinants and inform tailored interventions. To ensure lasting impact, national salt-reduction and nutrition strategies should be adapted for rural areas by supporting local production of fruits, vegetables, and low-sodium foods, and encouraging gradual sodium reduction in traditional dishes. Collaboration with local employers and the use of digital health tools can further improve engagement. Strengthening the role of advanced practice nurses (APNs)—introduced in primary care over the past decade, can expand preventive services. APNs can provide education, routine screenings, and follow-up monitoring for individuals with elevated BP, enhancing early detection, treatment adherence, and lifestyle modification in rural populations.
Conclusion
This study demonstrates gender- and age-related disparities in cardiovascular risk profiles and health behaviors in a rural district of Kazakhstan. While females reported higher rates of previously diagnosed hypertension and greater use of preventive medications, males exhibited higher blood pressure levels during screening and greater engagement in risk behaviors such as tobacco, alcohol, and caffeine use, suggesting a higher burden of undiagnosed or poorly controlled hypertension among male. The sharp rise in hypertension and obesity with age highlights the need for early prevention and sustained lifestyle interventions beginning in young adulthood. Given the rural context of the Enbekshikazakh district, these findings reflect population-specific healthcare access and lifestyle patterns that should inform local policy decisions. Gender-sensitive health education, targeted screening—particularly for men—and strengthened rural primary healthcare services are essential to reducing future cardiovascular disease burden.
Data Sharing Statement
The datasets and materials used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
The study was approved by the Local Ethics Committee of Kazakh-Russian Medical University, Kazakhstan (Protocol No. 18 (99), 5 January 2023).
Disclosure
The authors declare they have no competing interests in this work.
References
1. World Health Organization. Hypertension; 2025. Available from: www.who.int/news-room/fact-sheets/detail/hypertension.
2. Sorato MM, Davari M, Kebriaeezadeh A, Sarrafzadegan N, Shibru T. Societal economic burden of hypertension at selected hospitals in southern Ethiopia: a patient-level analysis. BMJ Open. 2022;12(4):e056627. doi:10.1136/bmjopen-2021-056627
3. Mennini FS, Marcellusi A, von der Schulenburg JM, et al. Cost of poor adherence to anti-hypertensive therapy in five European countries. Eur J Health Econ. 2015;16(1):65–12. doi:10.1007/s10198-013-0554-4
4. Daroudi R, AkbariSari A, Zamandi M, Shahali Z. Economic burden of hypertension in Iran: a prevalence-based cost of illness study. BMJ open. 2025;15(6):e099322. doi:10.1136/bmjopen-2025-099322
5. Wang Y, Lee JS, Pollack LM, Kumar A, Honeycutt S, Luo F. Health care expenditures and use associated with hypertension among U.S. Adults. Am J Preventive Med. 2024;67(6):820–831. doi:10.1016/j.amepre.2024.07.005
6. Noor Hassim I, Norazman MR, Diana M, Khairul Hazdi Y, Rosnah I. Cardiovascular risk assessment between urban and rural population in Malaysia. Med J Malaysia. 2016;71(6):331–337.
7. Guirguis-Blake JM, Evans CV, Webber EM, Coppola EL, Perdue LA, Weyrich MS. Screening for hypertension in adults: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;325(16):1657–1669. doi:10.1001/jama.2020.21669
8. Najman JM, Kisely S, Scott JG, et al. Gender differences in cardiovascular disease risk: adolescence to young adulthood. Nutr Metab Cardiovasc Dis. 2024;34(1):98–106. doi:10.1016/j.numecd.2023.09.024
9. GBD 2021 US Obesity Forecasting Collaborators. National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050. Lancet. 2024;404(10469):2278–2298. doi:10.1016/S0140-6736(24)01548-4
10. Mukhtarkhanova DM, Junusbekova GA, Tundybayeva MK, et al. Arterial hypertension and associated risk factors in Kazakhstan: an analysis of blood pressure screening results from May Measurement Month 2021-2023. Cardiol Ther. 2025;14(2):283–296. doi:10.1007/s40119-025-00412-w
11. Schmidt BM, Durao S, Toews I, et al. Screening strategies for hypertension. Cochrane Database Syst Rev. 2020;5(5):CD013212. doi:10.1002/14651858.CD013212.pub2
12. WHO Primary Health Care Demonstration Platform. Copenhagen: WHO Regional Office for Europe; 2022.
13. May Measurement Month. May Measurement Month 2025 (MMM25) protocol. Version 0.1. London: May Measurement Month; 2025.
14. Jensen MD, Ryan DH, Apovian CM, et al. AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation. 2014;129(suppl 2):S102–S138. doi:10.1161/01.cir.0000437739.71477.ee
15. Jones DW, Ferdinand KC, Taler SJ, et al. AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM guideline for the prevention, detection, evaluation and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;152(11):e114–e218. doi:10.1161/CIR.0000000000001356
16. Beaney T, Wang W, Schlaich MP, et al. Global blood pressure screening during the COVID-19 pandemic: results from the May Measurement Month 2021 campaign. J Hypertens. 2023;41(9):1446–1455. doi:10.1097/HJH.0000000000003488
17. Yerdessov S, Kadyrzhanuly K, Sakko Y, et al. Epidemiology of Arterial Hypertension in Kazakhstan: data from Unified Nationwide Electronic Healthcare System 2014-2019. J Cardiovasc Dev Dis. 2022;9(2):52. doi:10.3390/jcdd9020052
18. Rom Korin M, Chaplin WF, Shaffer JA, Butler MJ, Ojie MJ, Davidson KW. Men’s and women’s health beliefs differentially predict coronary heart disease incidence in a population-based sample. Health education & behavior: the official publication of the Society for Public Health. Education. 2013;40(2):231–239. doi:10.1177/1090198112449461
19. Bandi P, Cahn Z, Goding Sauer A, et al. Trends in E-Cigarette use by age group and combustible cigarette smoking histories, U.S. Adults, 2014-2018. Am J Prev Med. 2021;60(2):151–158. doi:10.1016/j.amepre.2020.07.026
20. Seaton CL, Bottorff JL, Caperchione CM, Johnson ST, Oliffe JL. The association between men’s heath behaviors and interest in workplace health promotion. Workplace Health Saf. 2020;68(5):226–235. doi:10.1177/2165079919885957
21. Cisse K, Samadoulougou S, Ouedraogo M, Kouanda S, Kirakoya-Samadoulougou F. Prevalence of abdominal obesity and its association with cardiovascular risk among the adult population in Burkina Faso: findings from a nationwide cross-sectional study. BMJ Open. 2021;11(7):e049496. doi:10.1136/bmjopen-2021-049496
22. NORC at the Universit of Chicago Obesity Prevalence & Comorbidity Map, September 2022–April 2023. Available from: https://www.norc.org/research/projects/obesity-prevalence-and-comorbidity-map.html.
23. Kim G, Woo H, Ji YA. Factors affecting abdominal obesity: analyzing national data. Healthcare. 2024;12(8):827. [Erratum in: Healthcare (Basel). 2024 Aug 26;12(17):1698. doi: 10.3390/healthcare12171698]. doi:10.3390/healthcare12080827
24. Eurostate. European Health Interview Survey Overweight and Obesity—BMI Statistics. Brussels, Belgium: EU; 2024.
25. He FJ, Campbell NRC, Woodward M, MacGregor GA. Salt reduction to prevent hypertension: the reasons of the controversy. Eur Heart J. 2021;42(25):2501–2505. doi:10.1093/eurheartj/ehab274
26. Xun R, Gao Y, Zhen S, et al. Effects of behavioral interventions for salt reduction on blood pressure and urinary sodium excretion: a systematic review and meta-analysis of randomized controlled trials. Global Heart. 2023;18(1):65. doi:10.5334/gh.1281
27. Du X, Zhu Y, Guo J, et al. Effect of salt reduction interventions in lowering blood pressure and salt intake in Zhejiang Province, China, 2017-2021: a randomized controlled trial. Nutrients. 2025;17(5):893. doi:10.3390/nu17050893
28. Jia M, Zhen L. Analysis of Food Production and Consumption Based on the Emergy Method in Kazakhstan. Foods. 2021;10(7):1520. doi:10.3390/foods10071520
29. Kazakhstan’s moves to reduce salt intake not in conflict with business interests. News release; 2023. Available from: https://www.who.int/europe/news/item/17-05-2023-kazakhstan-s-moves-to-reduce-salt-intake-not-in-conflict-with-business-interests.
30. Meher M, Pradhan S, Pradhan SR. Risk factors associated with hypertension in young adults: a systematic review. Cureus. 2023;15(4):e37467. doi:10.7759/cureus.37467
31. Kritsotakis G, Psarrou M, Vassilaki M, Androulaki Z, Philalithis AE. Gender differences in the prevalence and clustering of multiple health risk behaviours in young adults. J Adv Nurs. 2016;72(9):2098–2113. doi:10.1111/jan.12981
32. Sofija E, Harris N, Phung D, Sav A, Sebar B. Does flourishing reduce engagement in unhealthy and risky lifestyle behaviours in emerging adults? Int J Environ Res Public Health. 2020;17(24):9472. doi:10.3390/ijerph17249472
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.