Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Gastrointestinal Problems in Chinese Children with Autism Spectrum Disorder
Authors Lai KYC ![]() , Leung PWL
, Leung PWL ![]() , Hung SF, Shea CKS, Mo F, Che KKI, Tse CY
, Hung SF, Shea CKS, Mo F, Che KKI, Tse CY ![]() , Lau FLF, Ma SL
, Lau FLF, Ma SL ![]() , Wu JCY, So S, Dadds MR
, Wu JCY, So S, Dadds MR
Received 6 May 2020
Accepted for publication 6 July 2020
Published 24 July 2020 Volume 2020:16 Pages 1807—1815
DOI https://doi.org/10.2147/NDT.S260654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Kelly YC Lai,1 Patrick WL Leung,2 Se Fong Hung,1 Caroline KS Shea,3 Flora Mo,3 Kiti KI Che,3 Chun-Yu Tse,2 Fanny LF Lau,1 Suk Ling Ma,1 Justin CY Wu,4 Suzanne So,2 Mark R Dadds5
1Department of Psychiatry, Chinese University of Hong Kong, Shatin, Hong Kong; 2Department of Psychology, Chinese University of Hong Kong, Shatin, Hong Kong; 3Department of Psychiatry, Alice Ho Miu Ling Nethersole Hospital, Tai Po, Hong Kong; 4Department of Medicine, Chinese University of Hong Kong, Shatin, Hong Kong; 5School of Psychology, University of Sydney, Sydney, Australia
Correspondence: Kelly YC Lai
Department of Psychiatry, Chinese University of Hong Kong, Shatin, Hong Kong
Tel +852 26076025
Fax +852 26671255
Email [email protected]
Purpose: Gastrointestinal symptoms in individuals with autism spectrum disorder may constitute a subgroup with complex gut-brain interactions underlying the pathogenesis. This study examined the prevalence of gastrointestinal symptoms in a sample of Chinese children with autism spectrum disorder, as well as the factors related to them.
Participants and Methods: The participants included a clinic sample of 107 children with autism spectrum disorder and 249 gender- and age-matched typically developing community children.
Results: Results found children with autism spectrum disorder to be twice as likely to suffer from gastrointestinal symptoms, reporting increased rates of constipation, abdominal migraine and aerophagia. Autism spectrum disorder diagnosis remained a significant predictor of gastrointestinal symptoms after taking into account the potential confounders that included comorbid psychopathologies, diets, and parental anxiety and depression.
Conclusion: Our results suggest that autism spectrum disorder with gastrointestinal symptoms may constitute a subgroup within the autism spectrum disorder population that warrants further investigation.
Keywords: autism spectrum disorder, gastrointestinal symptoms, subgroup, children, Chinese
Introduction
Autism spectrum disorder (ASD) is a complex neurodevelopmental disorder that begins in childhood and characterized by deficits in social and communication skills together with repetitive stereotyped behaviors. It is a disorder with a wide range of psychiatric and physical comorbidities.1,2
In recent years, there has been a growing interest in the co-occurrence of gastrointestinal (GI) symptoms and ASD. Studies have confirmed an increase in the prevalence of GI symptoms in children with ASD compared to children with other developmental disorders, or those who are typically developing, including sibling pairs. However, the actual reported prevalence rates differ widely across studies, ranging from 9% to 91%, with a mean of approximately 44%.3 In a meta-analysis, McElhanon et al concluded that children with ASD were 2–4 times more likely to suffer from functional GI symptoms, and the most commonly reported were constipation, diarrhea, and abdominal pain.4
Yet, factors associated with the increased prevalence of GI symptoms are poorly understood. Some studies found GI symptoms to be associated with more severe autism symptoms,5–7 but others did not find such an association.8–11 The relationship with intellectual level is also inconclusive, with studies finding either those without intellectual disability to be more likely to present with GI symptoms, or there was no difference in intellectual levels between those with and without GI symptoms.8,9,11,12 Eating behaviors, and dietary factors such as those stemming from food selectivity and use of special diets, which are common among children with ASD,13 can have an impact on nutritional intake, but have not been found to be associated with GI symptoms.6,8,10,14 On the other hand, an emerging theme, and one where the findings appear more consistent, is the association with emotional symptoms. Studies spanning different age ranges, developmental levels and intellectual abilities have reported that children with ASD and GI symptoms have more irritability, anxiety, and affective symptoms than those without GI symptoms.12,15-18 However, this should not be too surprising given the well-established relationship between GI symptoms and emotional symptoms,19 as well as between ASD and emotional symptoms.20
In summary, while the increase in prevalence of GI symptoms among children with ASD is recognized, reasons for the increase remain unclear. Factors such as severity of autism symptoms, intellectual levels, diets, and emotional symptoms can all, on their own or in combination, explain the increased rates of GI symptoms in children with ASD. Methodological differences among studies, such as how GI symptoms were assessed (eg, instruments used, lifetime or current symptoms, etc.), or the characteristics of participants recruited (eg, with or without comorbid intellectual disability and/or emotional symptoms, etc.) can all contribute to the inconsistent results. One major limitation of past studies is their lack of control for all these potential confounders. Indeed, it is unclear whether the diagnosis of ASD itself remains an independent predictor of GI symptoms after controlling for these confounders. It is therefore the aim of this study to test the above hypothesis, including potential confounders such as dietary pattern and comorbid psychopathologies. Because the main informants of this study will be parents, the possibility of biased reporting secondary to parental levels of anxiety and depression will also be examined as confounders.
Participants and Methods
Participants
Participants were two groups of Chinese children from Hong Kong – a group with a diagnosis of ASD and a typically developing community comparison group. The ASD group was randomly selected from children aged 4–18 attending the child and adolescent psychiatric clinic of a university teaching hospital. Their diagnosis was made by child psychiatrists according to DSM-5 criteria21 after obtaining a detailed developmental history from the parents and observing the children’s behaviors in the clinic. They also had to be studying in local mainstream schools for children without intellectual disability. Children were excluded if they had 1) intellectual disability, 2) organic illnesses that affected their GI function, such as Hirschsprung’s disease, spina bifida, and hypothyroidism, or 3) severe mental disorders such as psychoses or affective disorders. They were also excluded if the parents could not understand Chinese. The comorbidities of the ASD participants were assessed by a questionnaire – the Strengths and Difficulties Questionnaire (SDQ) – which covers emotional symptoms, conduct problems and hyperactivity.22 Detailed explanation about the study was given to the parents of the eligible children with subsequent written consent obtained from them.
The typically developing community comparison group was recruited by inviting several local mainstream schools from the same district as the clinic to participate. As noted, these local mainstream schools in Hong Kong are for children without intellectual disability. The research team first visited the interested schools to explain the aims and purpose of the study to the school personnel, who in turn conveyed the study invitation to parents of their students to participate on a voluntary basis. For interested parents, detailed explanation about the study was given to them by the research team and written consent subsequently obtained. The same set of exclusion criteria that was applied to the ASD group was similarly applied to the comparison group. In addition, children in the comparison group whose parents reported a diagnosis of ASD or whose score on the Autism Spectrum Quotient (AQ-child/AQ-adolescent)23,24 were above cutoff were excluded.
This study received ethical approval from the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (Ref no. CRE-2013.425).
Procedure
Parents of all participants, whether they be clinical or typically developing, were asked to complete 1) The Questionnaire on Pediatric Gastrointestinal Symptoms – Rome III Version (QPGS-III),25 2) Strengths and Difficulties Questionnaire – Parent version (SDQ-P),22 3) a diet questionnaire, 4) Hospital Anxiety and Depression Scale (HADS)26 for parents’ anxiety and depressive symptoms, and 5) a questionnaire on demographics. Parents of the comparison group were additionally asked to complete the Autism Spectrum Quotient – Child version (AQ-Child) for children between 4 and 11 years old and adolescent version (AQ-Adol) for adolescents 12–18 years old.23,24 The parents of the clinical sample completed the questionnaires when they brought their children to the clinic for follow-up and a research assistant was on hand to answer any questions. Parents of the comparison group were given the questionnaires by the school personnel coordinating the study, who also helped to collect the completed questionnaires one week later. The parents were given envelopes to put in their completed questionnaires before handing back to the school coordinators. The telephone contact of the research team was given to the parents in case they had any queries. The questionnaires took just under an hour to complete.
Measures
The Questionnaire on Pediatric Gastrointestinal Symptoms – Rome III Version (QPGS-III)
The QPGS-III is a 71-item questionnaire that assesses GI symptoms in the pediatric population and provides a standardized algorithm for the classification of functional GI disorders.25 The parent version, which is for children aged four and above, was used in this study. Responses to this questionnaire are scored on a 5-point scale to measure frequency, severity, and duration of GI symptoms. Functional GI disorders are classified according to Rome-III criteria. A Chinese translated version is available from the Rome Foundation. As this was originally translated for use among Mandarin-speaking Chinese population in Mainland China, slight modification in the language of the items had to be made to adjust for its use in Hong Kong, which speaks the Cantonese instead of Mandarin dialect. Approval was granted by the Rome Committee for this modification.
Strengths and Difficulties Questionnaire – Parent Version (SDQ-P)
The SDQ-P is a brief behavioral screening questionnaire completed by parents of children aged 4–18.22 It consists of 25 attributes that are scored on a three-point scale. The attributes are divided across five subscales, namely, emotional symptoms, conduct problems, hyperactivity, peer relationship problems and prosocial behavior. All subscales except prosocial behavior are summed to generate a total difficulties score. The SDQ has been translated into Chinese. Its reliability and validity were affirmed with clinic and community children in Hong Kong.27,28
Dietary Pattern
Dietary information was collected from a dietary questionnaire developed by the Department of Health, Hong Kong SAR Government. It was used in its 2005–2006 child health survey. In this questionnaire, parents were asked to provide information on children’s eating behaviors and dietary habits. For the purpose of this study, information on the intake of i) nutrients (ie, the average number of portions of protein and carbohydrates taken per meal in the past 7 days), ii) fibers (the average amount of fruits and vegetables taken each day in the past 7 days), and iii) unhealthy food (the amount of soft drinks, fried food, junk food, and the number of times s/he ate in fast food restaurants in the past 7 days, and whether fats from meat were removed) was extracted for analysis. There were altogether 6 items on nutrients intake, 2 items on fibre intake, and 5 questions on unhealthy food.
Hospital Anxiety Depression Scale (HADS)
HADS measures the presence and severity of anxiety and depressive symptoms in the preceding week using a 4-point scale, ranging from 0 to 3 (0: absence of symptoms, 3: severe symptoms). A Chinese translation is available and found to have good internal consistency (0.86) and external validity (AUC = 0.83), with a favorable sensitivity (0.8) and specificity (0.8) for use in Hong Kong.29
The Chinese Autism Spectrum Quotient-Child Version (AQ-Child) and -Adolescent Version (AQ-Adol)
The Child and Adolescent versions of the Autism Spectrum Quotient are derived from the original Adult version for completion by parents or main caretakers to quantify autistic traits among children and adolescents with normal intelligence. Items cover behaviors across five domains: communication, social skills, attention switching, imagination, and attention to detail. The AQ-Child is for children aged 4–11 years, and the AQ-Adol for adolescents 12–18 year olds. Psychometric studies have attested to their sound validity and test-retest reliability.23,24 Both the AQ-Child and AQ-Adol have been translated from the original English version into Chinese and have been tested to exhibit satisfactory validity and reliability with ASD and typically developing children in Hong Kong (unpublished Masters theses).
Data Analysis
The objectives of the study were to compare the prevalence of GI symptoms in children with ASD and typically developing controls, and to examine associated factors. Statistical analyses were carried out using SPSS version 22.0. Group comparisons of categorical variables were made using Chi-square test, but where the expected frequencies were fewer than 5, Fisher’s Exact test was used. Comparisons of dimensional data were made using independent t-tests when the data were normally distributed, and Mann–Whitney’s U-test when the data were not normally distributed. Correlations with GI symptoms were examined by using Spearman’s Rank-order correlation when the variables were categorical, and Pearson’s correlation when variables were dimensional. A series of multiple regression were then run to assess whether the diagnosis of ASD could still independently predict GI symptoms after comorbid emotional and behavioral symptoms, dietary pattern, and parental anxiety and depression were controlled.
Results
Sample Characteristics (TABLE 1)
The clinic sample consisted of 107 children with a clinical diagnosis of ASD. A gender- and age-matched community comparison group consisting of 249 children was established by correspondingly selecting from 633 eligible comparison participants. Sociodemographic characteristics of the two groups are listed in Table 1. The mean age of the 107 children with ASD was 9.2 years (s.d. 3.3), while that of the 249 community subjects 9.8 years (s.d. 3.5). The majority were boys, and this was expected given the predominance of male sex in individuals with ASD. The two groups did not differ in terms of sibling status, parental age, and household income. Parents were the informants for all of the ASD group and 95% of the community group.
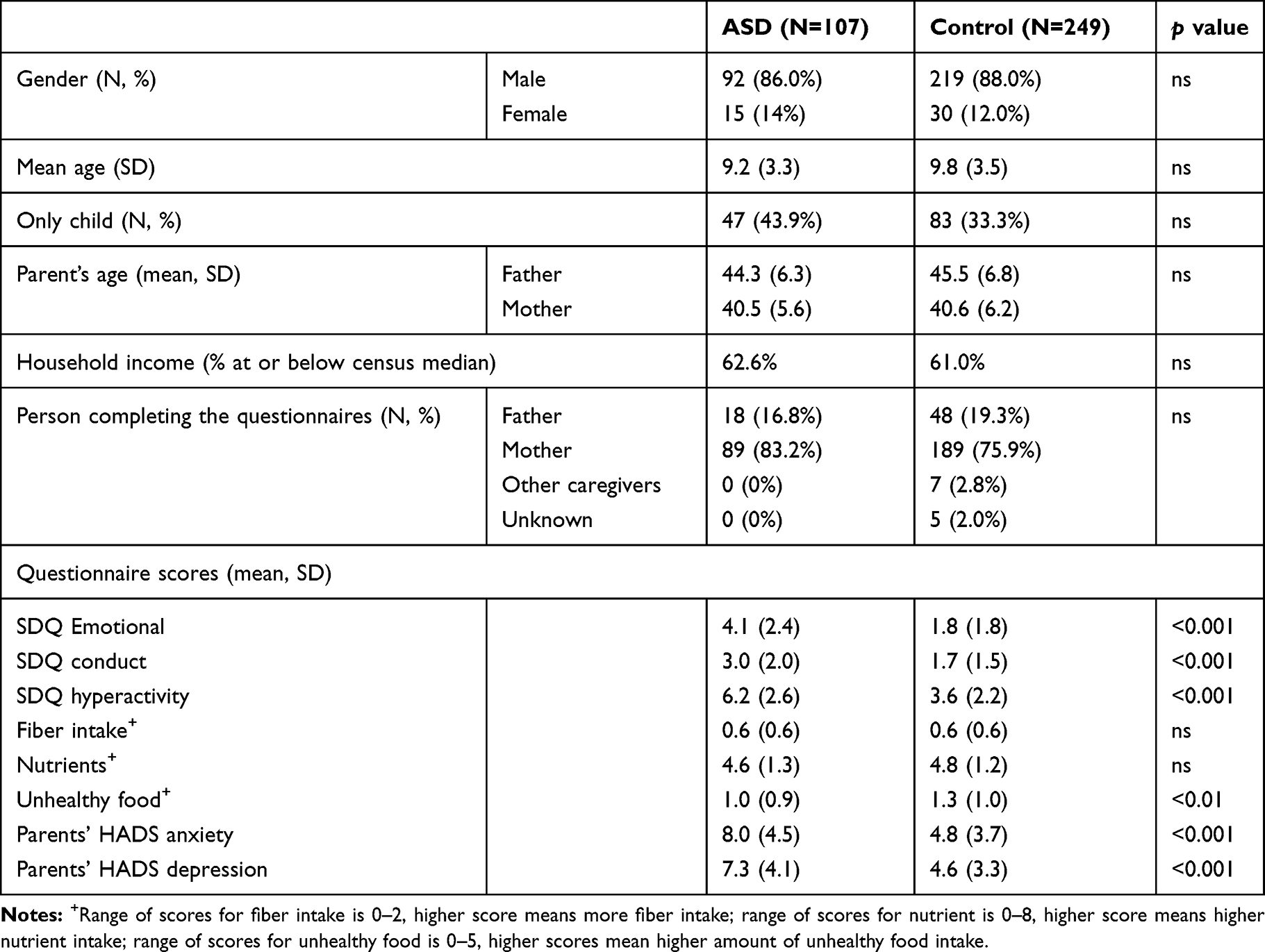 |
Table 1 Characteristics of Study Participants |
Rates and Types of GI Symptoms (TABLE 2)
The rates of different types of GI symptoms are tabulated in Table 2. Overall, 26.2% of children with ASD were reported by their parents to have GI symptoms according to QPRS, as compared to 10.4% of children in the comparison group, and the difference was statistically significant (χ2=14.384, p<0.001). GI symptoms that were significantly elevated in the ASD group were functional constipation (12.9% in ASD group, 4.8% in comparison group, χ2=5.574, p<0.05), abdominal migraine (9.4% in ASD group, 2.0% in comparison group, χ2=9.702, p=0.002), and aerophagia (6.3% in ASD group, 0.4% in comparison group, Fisher’s Exact test p<0.01).
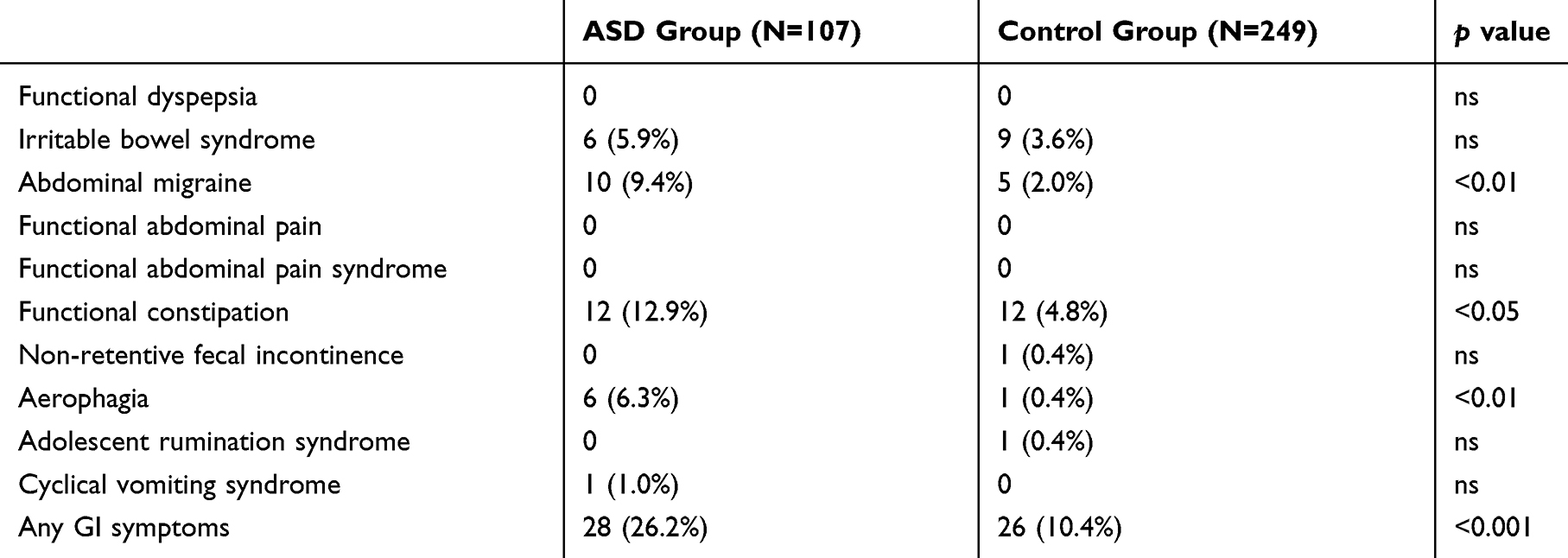 |
Table 2 Prevalence of Gastrointestinal Symptoms |
Factors Associated with GI Symptoms
QPGS-III assesses separate, individual GI symptoms which do not necessarily constitute parts of a unitary, single disorder. Each symptom should be considered on its own. The above analysis identified three GI symptoms, namely, functional constipation, abdominal migraine and aerophagia, the frequencies of which were significantly raised in children with ASD. Originally, each GI symptom is a categorical variable, absent (scored “0”) or present (scored “1”). We adopted a simple method of forming a dimensional scale out of the above three identified GI symptoms by adding up their scores so that the new scale would have a score ranging from “0” to “3”.30 This would give us a dimensional dependent variable – GI symptoms – to be predicted by various independent variables, including the diagnosis of ASD. In the subsequent analysis, when we mention GI symptoms, we are referring to this dimensional scale composed of the three GI symptoms identified to be raised in frequency in our clinical sample.
To examine factors associated with the presence of GI symptoms, correlational analyses were first conducted (see Table 3). Results showed that the presence of GI symptoms was significantly correlated with ASD diagnosis, child psychopathologies, and parental HADS scores. None of the dietary factors was significantly correlated with GI symptoms.
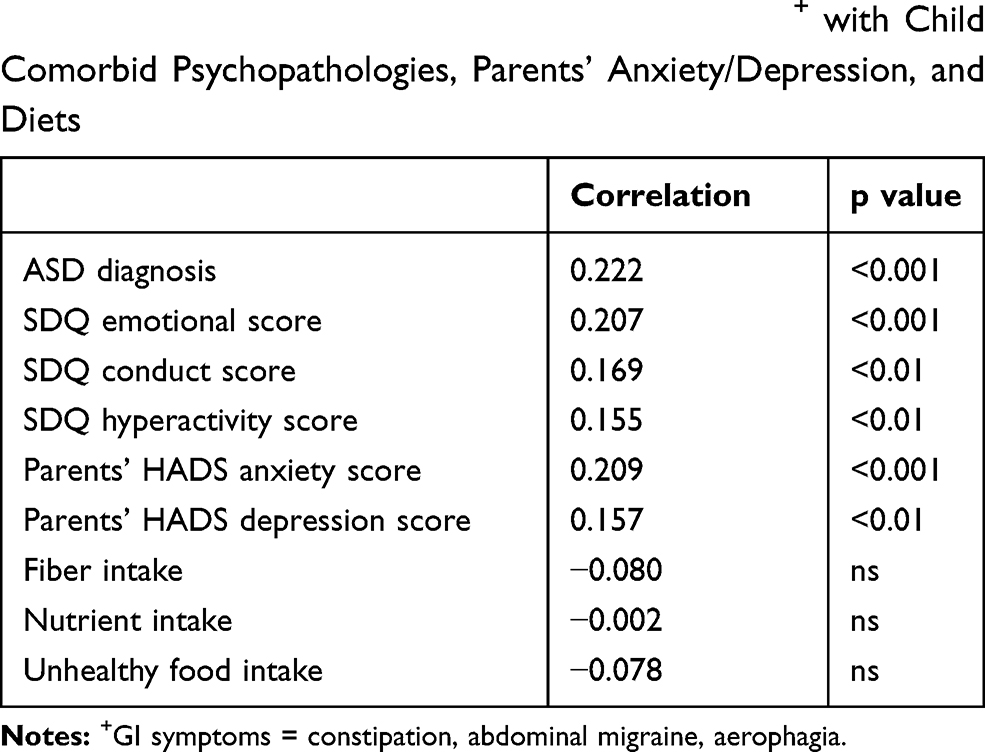 |
Table 3 Correlation of Gastrointestinal Symptoms+ with Child Comorbid Psychopathologies, Parents’ Anxiety/Depression, and Diets |
Next, to explore the unique contribution of each of these significant factors in predicting GI symptoms, they were entered into a multiple linear regression analysis as independent variables, and GI symptoms were the dependent variable. Results are tabulated in Table 4. A significant regression equation was found (F(6339)=4.744, p<0.001, R2 = 0.077), with ASD diagnosis (Beta = 0.118, p<0.05) emerged as the only significant predictor. Other comorbid psychopathologies, such as emotional symptoms, and parental anxiety were no longer significant predictors.
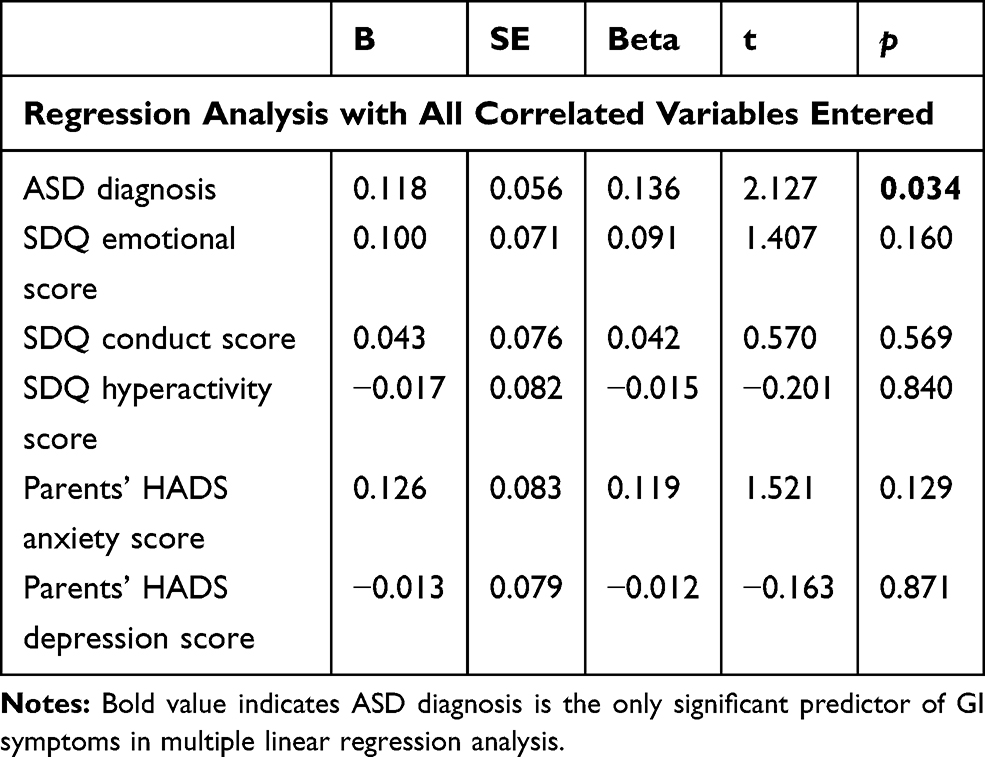 |
Table 4 Results of Multiple Linear Regression Analysis |
Discussion
Our results show that 26.2% of Chinese children with ASD have GI symptoms. This rate is more than twice that found in the typically developing comparison group (10.4%). The types of symptoms identified to be significantly raised are those of constipation, abdominal migraine, and aerophagia. After controlling for comorbid emotional symptoms, hyperactivity, conduct problems, diet, and parental anxiety and depression, the diagnosis of ASD remains the only significant predictor of GI symptoms.
Comparing our findings with those of previous studies, our results are similar in that children with ASD are at least twice as likely to suffer from GI symptoms as children who are typically developing. However, our prevalence of 26.2% is at the lower end of the range reported, which is estimated to average 44%, with a range of 9–91%.3 One possible reason for the lower prevalence in our study can be due to methodological differences such as how GI symptoms are measured. We utilize QPGS-III, which is a standardized instrument based on Rome III criteria, and which assesses a range of GI symptoms within a stipulated time frame of the past year or 2 months, depending on the symptoms enquired. This is in contrast to many previous studies which use a variety of chart reviews, medical history interview, or investigator-designed questionnaires to chart GI symptoms over various durations ranging from six months to whole life. However, compared to a recent US study which also utilized the QPGS-III, our prevalence is still relatively low.31 This may reflect the overall variability of the rates of functional gastro-intestinal symptoms in children across different ethnic and socio-economic groups.32,33
The types of GI symptoms with elevated prevalence found in this study include constipation (12.9%), abdominal pain (9.4%), and aerophagia (6.3%). The former two symptoms are well known to be increased in children with ASD. Aerophagia is less often mentioned in the literature, but previous studies have reported excessive gaseousness, abdominal bloatedness and flatulence.34 Previous studies also found elevated prevalence of diarrhoea.34 However, because the ROME III criteria for children do not have diarrhea as a stand-alone symptom, we do not have the prevalence of diarrhea to compare against earlier findings. Under ROME III, diarrhoea is subsumed under symptoms of Irritable Bowel Syndrome (IBS), and our findings do not find a statistically significant elevation in the prevalence of IBS in children with ASD.
Our finding that ASD remains the only significant predictor of GI symptoms after deliberately controlling for known correlates has not been reported in the past. It should be noted that emotional symptoms are correlated with GI symptoms on a one-to-one basis, but they are no longer a significant predictor of GI symptoms in the regression analysis alongside other correlates. This result suggests that emotional symptoms as a comorbid or correlated condition in our ASD group are not as powerful as ASD diagnosis itself in predicting GI symptoms. We also did not find an association between dietary factors and GI symptoms, which is similar to findings from previous studies. In sum, our study confirms that the association between ASD and GI symptoms is not spurious and cannot be explained away by the associated emotional symptoms or dietary problems found in children with ASD.
Our result lends support to the notion that children with ASD and GI symptoms constitute an ASD subtype.35 Identifying ASD subtypes may pave the way for further etiological explorations. There is a burgeoning literature speculating that complex gut-brain interactions may be one possible pathogenic pathway for ASD. In support of such speculation are findings that subsets of individuals with ASD have altered intestinal microbiota,36 and that such dysbiosis can affect brain development by modulating intestinal and blood-brain barrier permeability and immune dysregulation.37–39 The microbiota-gut-brain interaction can also modulate the stress reactivity of the hypothalamic-pituitary-adrenal (HPA) axis,40 and contribute to the presence of GI symptoms. Psychophysiological studies have found that children with ASD have atypical autonomic responses to anxiety,41 and this relationship between altered autonomic nervous system functioning, stress responses and GI symptoms may be another potential mechanism underlying an ASD-GI subgroup.31 These different potential mechanisms may, in turn, be related to the genetic causes underlying ASD, such as the involvement of the c-MET,42,43 CHD8,44,45 and Serotonin (5HT) systems,11,46,47 all of which have wide ranging effects on biological processes ranging from intestinal functions, immune functions, and brain development, and are related to complex behavior such as emotional reactivity, anxiety and depressive behavior as well as cognition.48 Children with ASD and GI symptoms may therefore be a subgroup to focus on for further etiological exploration.
One of the strengths of this study is the inclusion of variables that may confound the relationship between ASD and GI symptoms. These potential confounders have not been properly controlled in previous studies, leading to uncertainties regarding the unique contribution of ASD to GI symptoms. Towards this end, our study recruited participants from local mainstream schools which are for children without intellectual disability. This procedure helps to eliminate the impact of intellectual disability or lack of verbal communication skills on GI symptoms,3,6 although the downside is that we have not actually tested them as potential confounders. We assess the associated psychopathologies in ASD, particularly emotional symptoms, as potential confounders. By including parents’ anxiety and depression in the analyses, the possibility of biased reporting due to parental psychopathology can also be examined. The inclusion of a diet questionnaire helps to examine whether any particular dietary habits contribute to the presence of GI symptoms. Another strength of our study is to have adopted a systematic assessment of GI symptoms by using a widely recognized pediatric GI questionnaire that is based on ROME III criteria. The ROME-III criteria are standardized, and can help with the large variance observed in the review by Buie.3
Nevertheless, we must note some limitations of the study. First, although all the clinical participants received a diagnosis of ASD made by child psychiatrists according to DSM-5, the assessment of comorbid problems, eg, emotional symptoms or hyperactivity, was instead conducted by a questionnaire – SDQ. Yet, it is a well-established and valid measure of childhood and adolescent psychopathologies, and has been re-validated for use locally.27,28 Second, this study did not include children with other neurodevelopmental disorders so that we cannot answer the question whether elevated rates of GI problems are also found in those groups of children, as suggested by some previous studies.17,49 Third, the actual number of children identified to have GI symptoms in both the ASD and comparison groups was small. This small sample size does not allow further analyses of whether there are specific predictors for each type of GI symptoms, namely, constipation, abdominal migraine, and aerophagia. Lastly, although the lack of association between diets and GI symptoms is in keeping with previous findings, we have only studied a limited number of dietary factors (nutrients, fibers, and unhealthy food). More extensive dietary assessment may be needed to further explore the relationship between diets and GI symptoms and reconfirm our current findings.
Conclusion
Our study finds that ASD diagnosis remains a significant predictor of GI symptoms after controlling for a range of potential confounders, including comorbid psychopathologies, diets and parents’ anxiety and depression. Children with ASD and GI symptoms may constitute an ASD subtype. Further studies of this subtype may shed light on some specific etiological pathways for ASD. From a clinical perspective, an awareness of the increased prevalence of GI problems in children with ASD should remind clinicians to routinely enquire into the former and manage accordingly.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study received ethical approval from the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (Ref no. CRE-2013.425). All procedures were performed in compliance with the Declaration of Helsinki. Parents signed written informed consent on behalf of their participating children.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflict of interest in this work.
References
1. Lai M-C, Kassee C, Besney R, et al. Prevalence of co-occurring mental health diagnoses in the autism population: a systemic review and meta-analysis. Lancet Psychiatr. 2019;6:819–829. doi:10.1016/S2215-0366(19)30289-5
2. Bauman ML. Medical comorbidities in autism: challenges to diagnosis and treatment. Neurotherapeutics. 2010;7:320–327. doi:10.1016/j.nurt.2010.06.001
3. Buie T, Campbell DB, Fuchs GJIII, et al. Evaluation, diagnosis, and treatment of gastrointestinal disorders in individuals with ASDs: a consensus report. Pediatr. 2010;125(Supplement 1):S1–18. doi:10.1542/peds.2009-1878C
4. McElhanon BO, McCracken C, Karpen S, Sharp WG. Gastrointestinal symptoms in autism spectrum disorder: a meta-analysis. Pediatr. 2014;133:872–883. doi:10.1542/peds.2013-3995
5. Wang LW, Tancredi DJ, Thomas DW. The prevalence of gastrointestinal problems in children across the United States with autism spectrum disorders from families with multiple affected members. J Dev Behav Pediatr. 2011;32:351–360. doi:10.1097/DBP.0b013e31821bd06a
6. Gorrindo P, Williams KC, Lee EB, Walker LS, McGrew SG, Levitt P. Gastrointestinal dysfunction in autism: parental report, clinical evaluation, and associated factors. Autism Res. 2012;5:101–108. doi:10.1002/aur.237
7. Adams JB, Johansen LJ, Powell LD, Quig D, Rubin RA. Gastrointestinal flora and gastrointestinal status in children with autism – comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011;11:22. doi:10.1186/1471-230X-11-22
8. Chandler S, Carcani-Rathwell I, Charman T, et al. Parent-reported gastrointestinal symptoms in children with autism spectrum disorders. J Autism Dev Disord. 2013;43:2737–2747. doi:10.1007/s10803-013-1768-0
9. Mazefsky CA, Schreiber DR, Olino TM, Minshew NJ. The association between emotional and behavioral problems and gastrointestinal symptoms among children with high-functioning autism. Autism. 2014;18(5):493–501. doi:10.1177/1362361313485164
10. Son JS, Zheng LJ, Rowehl LM, et al. Comparison of fecal microbiota in children with autism spectrum disorders and neurotypical siblings in the Simons simplex collection. PLoS One. 2015;10:e0137725. doi:10.1371/journal.pone.0137725
11. Marler S, Ferguson BJ, Lee EB, et al. Brief report: whole blood serotonin levels and gastrointestinal symptoms in autism spectrum disorder. J Autism Dev Disord. 2016;46:1124–1130. doi:10.1007/s10803-015-2646-8
12. Mannion A, Leader G. An analysis of the predictors of comorbid psychopathology, gastrointestinal symptoms and epilepsy in children and adolescents with autism spectrum disorder. Res Autism Spectr Disord. 2013;7:1663–1671. doi:10.1016/j.rasd.2013.10.002
13. Vissoker RE, Latzer Y, Gal E. Eating and feeding problems and gastrointestinal dysfunction in autism spectrum disorder. Res Autism Spectr Disord. 2015;12:10–21. doi:10.1016/j.rasd.2014.12.010
14. Ferguson BJ, Dovgan K, Severns D, et al. Lack of associations between dietary intake and gastrointestinal symptoms in autism spectrum disorder. Front Psychiatry. 2019;10:528. doi:10.3389/fpsyt.2019.00528
15. Nikolov RN, Bearss KE, Lettinga J, et al. Gastrointestinal symptoms in a sample of children with pervasive developmental disorders. J Autism Dev Disord. 2009;39:405–413. doi:10.1007/s10803-008-0637-8
16. Williams KC, Christofi FL, Clemmons T, Rosenberg D, Fuchs GJ. 342 chronic GI symptoms in children with autism spectrum disorders are associated with clinical anxiety. Gastroenterology. 2012;142(Suppl 5):S79–80. doi:10.1016/S0016-5085(12)60303-5
17. Chaidez V, Hansen RL, Hertz-Picciotto I. Gastrointestinal problems in children with autism, developmental delays or typical development. J Autism Dev Disord. 2014;44:1117–1127. doi:10.1007/s10803-013-1973-x
18. Ferguson BJ, Dovgan K, Takahashi N, Beversdorf DQ. The relationship among gastrointestinal symptoms, problem behaviors, and internalizing symptoms in children and adolescents with autism spectrum disorder. Front Psychiatry. 2019;10:194. doi:10.3389/fpsyt.2019.00194
19. Waters AM, Schilpzand E, Bell C, Walker LS, Baber K. Functional gastrointestinal symptoms in children with anxiety disorders. J Abnorm Child Psychol. 2013;41:151–163. doi:10.1007/s10802-012-9657-0
20. van Steensel FJA, Bögels SM, Perrin S. Anxiety disorders in children and adolescents with autistic spectrum disorders: a meta-analysis. Clin Child Fam Psychol Rev. 2011;14:302–317. doi:10.1007/s10567-011-0097-0
21. American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders.
22. Goodman R. Psychometric properties of the strengths and difficulties questionnaire (SDQ). JAACAP. 2001;40:1337–1345.
23. Auyeung B, Baron-Cohen S, Wheelwright S, Allison C. The autism spectrum quotient: children’s version (AQ-child). J Autism Dev Disord. 2008;38(7):1230–1240. doi:10.1007/s10803-007-0504-z
24. Baron-Cohen S, Hoekstra RA, Knickmeyer R, Wheelwright S. The autism spectrum quotient (AQ)—adolescent version. J Autism Dev Disord. 2006;36(3):343–350. doi:10.1007/s10803-006-0073-6
25. Walker LS, Caplan-Dover A, Rasquin-Weber A. Manual for the Questionnaire on Pediatric Gastrointestinal Symptoms. Nashville, TN: Department of Pediatrics, Vanderbilt University Medical Center; 2006.
26. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
27. Lai KYC, Luk ESL, Leung PW, Wong A, Law L, Ho K. Validation of the Chinese version of the strengths and difficulties questionnaire in Hong Kong. Soc Psychiatry Psychiatr Epidemiol. 2010;45:1179–1186. doi:10.1007/s00127-009-0152-z
28. Lai KYC, Luk ESL, Leung PW, Wong A. Use of the extended strengths and difficulties questionnaire (SDQ) to predict psychiatric caseness in Hong Kong. Child Psychiatry Hum Dev. 2014;45:703–711. doi:10.1007/s10578-014-0439-5
29. Leung CM, Ho S, Kan CS, Hung CH, Chen CN. Evaluation of the Chinese version of the hospital anxiety and depression scale: a cross-cultural perspective. Int J Psychosom. 1993;40:29–34.
30. Leung PWL, Luk SL, Ho TP, Taylor E, Lieh-Mak F, Bacon-Shone J. The diagnosis and prevalence of hyperactivity in Chinese schoolboys. Br J Psychiatry. 1996;168:486–496. doi:10.1192/bjp.168.4.486
31. Ferguson BJ, Marler S, Altstein AA, et al. Psychophysiological associations with gastrointestinal symptomatology and autism spectrum disorder. Autism Res. 2017;10:276–288. doi:10.1002/aur.1646
32. Korterink JJ, Diederen K, Benninga MA, Tabbers MM, Zhang L. Epidemiology of pediatric functional abdominal pain disorders: a meta-analysis. PLoS One. 2015;10(5):e0126982. doi:10.1371/journal.pone.0126982
33. Mugie SM, Benninga MA, Di Lorenzo C. Epidemiology of constipation in children and adults: a systemic review. Best Pract Res Clin Gastroenterol. 2011;25:3–18. doi:10.1016/j.bpg.2010.12.010
34. Holingue C, Newill C, Lee L-C, Pasricha PJ, Fallin MD. Gastrointestinal symptoms in autism spectrum disorder: a review of the literature on ascertainment and prevalence. Autism Res. 2018;11:24–36. doi:10.1002/aur.1854
35. Hsiao EY. Gastrointestinal issues in autism spectrum disorder. Harv Rev Psychiatry. 2014;22:104–111. doi:10.1097/HRP.0000000000000029
36. Liu F, Li J, Wu F, Sheng H, Peng Q, Zhou H. Altered composition and function of intestinal microbiota in autism spectrum disorders: a systematic review. Transl Psychiatry. 2019;9:43. doi:10.1038/s41398-019-0389-6
37. Vuong HE, Hsiao EY. Emerging roles or the gut microbiome in autism spectrum disorder. Biol Psychiatry. 2017;81:411–423. doi:10.1016/j.biopsych.2016.08.024
38. Azhari A, Azizan F, Esposito G. A systematic review of gut-immune-brain mechanisms in autism spectrum disorder. Dev Psychobiol. 2018;61(5):752–771.
39. Rose DR, Yang H, Serena G, et al. Differential immune responses and microbiota profiles in children with autism spectrum disorder and co-morbid gastrointestinal symptoms. Brain Behav Immun. 2018;70:354–368. doi:10.1016/j.bbi.2018.03.025
40. Carabotti M, Scirocco A, Maselli MA, Severi C. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Annal Gastroenterol. 2015;28:203–209.
41. Kushki A, Brian J, Dupuis A, Anagnostou E. Functional autonomic nervous system profile in children with autism spectrum disorder. Molecular Autism. 2013;5:39. doi:10.1186/2040-2392-5-39
42. Eagleson KL, Xie Z, Levitt P. The pleiotropic MET receptor network: circuit development and the neural-medical interface of autism. Biol Psychiatry. 2017;81:424–433. doi:10.1016/j.biopsych.2016.08.035
43. Campbell DB, Buie TM, Winter H, et al. Distinct genetic risk based on association of MET in families with co-occurring autism and gastrointestinal conditions. Pediatrics. 2009;123:1018–1024. doi:10.1542/peds.2008-0819
44. Bernier R, Golzio G, Xiong B, et al. Disruptive CHD8 mutations define a subtype of autism early in development. Cell. 2014;158:263–276. doi:10.1016/j.cell.2014.06.017
45. Wilkinson B, Grepo N, Thompson BL, et al. The autism-associated gene chromodomain helicase DNA-binding protein 8 (CHD8) regulates noncoding RNAs and autism-related genes. Transl Psychiatry. 2015;5(5):e568. doi:10.1038/tp.2015.62
46. Abdelrahman HM, Sherief LM, Alghobashy AA, et al. Association of 5-HT2A receptor gene polymorphisms with gastrointestinal disorders in Egyptian children with autistic disorder. Res Dev Disabil. 2015;36:485–490. doi:10.1016/j.ridd.2014.10.023
47. Sutcliffe JS, Delahanty RJ, Prasad HC, et al. Allelic heterogeneity at the serotonin transporter locus (SLC6A4) confers susceptibility to autism and rigid-compulsive behaviors. Am J Hum Genet. 2005;77:265–279. doi:10.1086/432648
48. Mayer EA, Knight R, Mazmanian SK, Cryan JF, Tillisch K. Gut microbes and the brain: paradigm shift in neuroscience. J Neurosci. 2014;34(46):15490–15496. doi:10.1523/JNEUROSCI.3299-14.2014
49. Bresnahan M, Horning M, Schultz AF, et al. Association of maternal report of infant and toddler gastrointestinal symptoms with autism – evidence from a prospective birth cohort. JAMA Psychiatr. 2015;72(5):466–474. doi:10.1001/jamapsychiatry.2014.3034
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.