Back to Journals » International Medical Case Reports Journal » Volume 19
Gastric-Type Endocervical Adenocarcinoma with Ovarian and Lymph Node Metastases: A Rare Case Study
Received 26 July 2025
Accepted for publication 25 November 2025
Published 13 January 2026 Volume 2026:19 556372
DOI https://doi.org/10.2147/IMCRJ.S556372
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Xiaofei Li, Meige Sun, Liang-Sheng Fan
Department of Obstetrics and Gynecology, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China
Correspondence: Liang-Sheng Fan, Email [email protected]
Abstract: Gastric-type endocervical adenocarcinoma (G-EAC), an uncommon HPV-negative mucinous adenocarcinoma of gastric pyloric-type epithelial differentiation, represents a significant diagnostic challenge due to its insidious etiology and vague clinical presentation. The anatomic depth of lesions within the endocervical canal frequently makes suboptimal biopsy samples both responsible for decreased diagnostic sensitivity and repeated false-negative biopsies delaying early detection. Most of the cases are diagnosed at late stages with frequent extrapelvic metastases, and these are linked with poor clinical outcomes. This case report retrospectively examines the clinicopathological characteristics, pitfalls in diagnosis, and treatment strategies for G-EAC to ensure better identification and management of this virulent neoplasm.
Keywords: non-HPV associated cervical adenocarcinoma, gastric-type endocervical adenocarcinoma
Introduction
Cervical cancer ranks as the fourth most prevalent cancer among women worldwide and one of the top causes of female cancer mortality internationally.1 The pathogenesis is principally attributed to persistent infection with high-risk human papillomavirus (HPV) genotypes. With the widespread implementation of cervical cancer screening programs and increasing adoption of HPV vaccination, a marked reduction in cervical cancer incidence has been achieved, accompanied by improved early-stage diagnosis rates. However, epidemiological data illustrate the trend of an increased incidence of cervical adenocarcinoma.2 Cervical adenocarcinoma is histologically classified into two distinct subtypes according to the International Endocervical Adenocarcinoma Criteria and Classification (IECC): HPV-associated and HPV-independent variants. Gastric-type endocervical adenocarcinoma (G-EAC), recognized as an HPV-independent histological subtype within the IECC framework, ranks as the second most frequent histomorphological entity following usual-type endocervical adenocarcinoma (UEA). Epidemiological studies estimate its prevalence at approximately 10% of all cervical adenocarcinoma cases.2 G-EAC, a distinct mucinous adenocarcinoma variant defined by gastric-type differentiation within the IECC system, demonstrates nonspecific symptomatology, anatomically occult lesions, and histologically aggressive phenotypes correlating with adverse clinical outcomes.3 This diagnostic complexity is exacerbated by the current lack of robust screening algorithms and validated molecular biomarkers for early detection. We herein present a comprehensive case report detailing the diagnostic evaluation and clinical management of a patient with G-EAC, aiming to enhance clinicians’ awareness of this diagnostically challenging entity.
Case Presentation
A 64-year-old postmenopausal female presented to the Hepatobiliary Surgery Unit of our hospital on 22 June 2022, with a history of recurring epigastric pain. Initial evaluation suggested acute cholecystitis, but contrast-enhanced abdominal CT incidentally revealed a 3.2 cm hypodense cervical mass with uterine cavity distension, raising suspicion of cervical malignancy. The patient denied postmenopausal vaginal bleeding, abnormal vaginal discharge, or other associated symptoms. Gynecological examination revealed cervical hypertrophy, with erosions at the external cervical os and contact bleeding. Tumor markers showed isolated CEA elevation (22 ng/mL). Ultrasound revealed an enlarged cervix (39 mm anteroposterior diameter) containing a heterogeneous solid mass (18×16×19 mm) with ill-defined margins and abundant vascularity on Doppler imaging. MRI revealed a 3.1*2.5*4.9 cm cervical mass with left parametrial invasion and endometrial nodules, consistent with stage IIB cervical carcinoma and suspected metastatic implants (Figure 1). Cervical HPV testing was negative, while Thinprep Cytology Test (TCT) revealed adenocarcinoma with a high-grade squamous intraepithelial lesion (HSIL). Colposcopy-guided biopsy confirmed invasive adenocarcinoma with HSIL (CIN II) at 3 o’clock and lymphovascular space invasion (LVSI). Immunohistochemistry was ER(−), PR(−), p16+ (diffuse), Ki-67 60% (hotspots), p40+, and PAX8(−). PET-CT identified a hypermetabolic cervical mass (3.8 cm) with invasion into vaginal fornix and endometrial implants, without nodal and distant metastases. Both parametria are free of tumor involvement (Figure 2). Despite imaging findings of left parametrial infiltration (suspicious FIGO Stage IIB) in MRI, pelvic examination demonstrated a definite demarcation between the cervix and pelvic wall with maintained mobility. Following careful evaluation, the final clinical stage was diagnosed as FIGO stage IIA2 (FIGO 2018) cervical adenocarcinoma. Due to the tumor’s substantial volume, three cycles of neoadjuvant chemotherapy (NACT) were administered before definitive surgical management. Post-NACT MRI showed tumor regression (25×22 mm). On September 6, 2022, the patient underwent a radical hysterectomy with bilateral salpingo-oophorectomy and pelvic lymphadenectomy. Final histopathology revealed moderately differentiated cervical adenocarcinoma (Silva pattern C), favoring HPV-independent G-EAC (Figure 3). The carcinoma circumferentially involves the endocervical canal and invades into the outer third of the cervical wall (depth of invasion approximately 1.0 cm). The carcinoma invades the cervico-uterine junction, endometrium, and superficial myometrium. Carcinoma involving both cornual regions is present. Focal lymphovascular and Perineural invasion is present. The left ovary has metastatic adenocarcinoma, the right ovary is free of carcinoma. Metastatic involvement was identified in bilateral internal iliac lymph nodes, while bilateral obturator, deep inguinal, common iliac, and external iliac lymph nodes were free of malignancy. The tumor cells show immunohistochemistry: ER(-), PAX-8(-), PR(-), P16(+), GATA-3(-), TTF-1(-), NapsinA(-), P53 (>95% strong positive, indicative of TP53 gene mutation), Special Stains: Mucicarmine (focal positive), Alcian Blue-PAS (AB-PAS) (focal positive) (Figure 4). The patient was diagnosed with stage IIIC1 (p) non-HPV-related G-EAC. She underwent adjuvant chemoradiation, consisting of 4 cycles of platinum-paclitaxel (TC) and 25 fractions of radiotherapy. Despite initial disease control, surveillance PET-CT in February 2024 revealed pulmonary and sacral metastases. The patient declined salvage chemoimmunotherapy.
 |
Figure 1 Pelvic contrast-enhanced MRI indicates a cervical mass measuring 31×25×49 mm. It is markedly hyperintense on DWI with corresponding low ADC, demonstrating heterogeneous marked enhancement after contrast. The mass invades the left cervical stroma, extending to the left vaginal fornix and parametrium. The red arrows show cervical lesion. (A) T1-weighted: Transverse view (B) T2-weighted: Sagittal view (C) mDIXON Water-phase image: Sagittal view (D) mDIXON Water-phase image: Coronal View. |
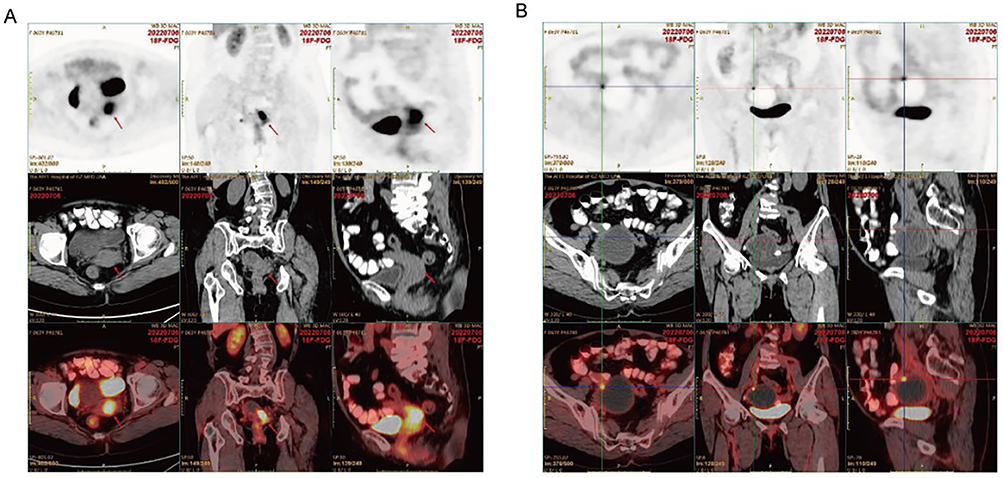 |
Figure 2 PET-CT (A) The imaging indicate cervical hypermetabolic mass (2.5×2.8×3.8 cm) invading left vaginal fornix, focal endometrial thickening with mild uptake. The red arrows show cervical lesion. (B) The center of the cross is intensely hypermetabolic nodule (0.7 cm) at the right anterosuperior uterine margin. |
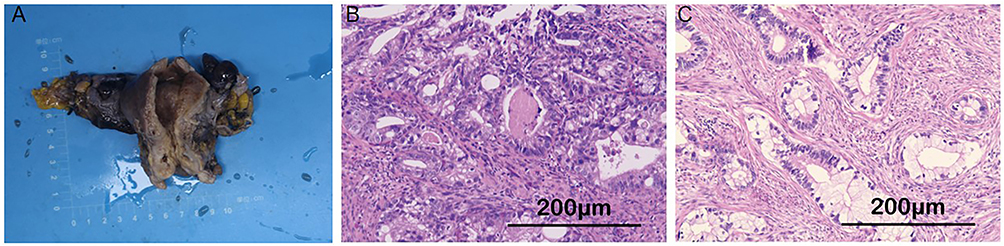 |
Figure 3 Histological finding in the patient of G-EAC. (A) Gross specimen. (B) Focal aggregates of foamy histiocytes with punctate calcification and minor tumor cells with clear cytoplasm and mucinous change (H&E, 20x). (C) Tumor cells with pale eosinophilic cytoplasm and nuclear atypia forming irregular and fused glands, indicative of gastric differentiation (H&E, 20x). |
 |
Figure 4 Immunohistochemical staining: (A) ER(-), (B) PR(-), (C) PAX-8 (-), (D) P16 (+), (E) P53(+), (F) GATA-3(-), (G) TTF-1(-), (H) NapsinA(-), (I) Special stains: Mucicarmine (focal positive), AB-PAS (focal positive). |
Discussion
Clinical Features and Diagnostic Approaches
G-EAC, while exhibiting deceptively benign morphological features, demonstrates aggressive biological behavior characterized by occult progression and poor prognosis. Clinically, G-EAC presents with nonspecific and variable symptoms, most commonly manifesting as vaginal mucoid or watery discharge and pelvic/abdominal masses. Gynecologic examination typically reveals cervical hypertrophy with a smooth or eroded external os, often demonstrating a characteristic “barrel-shaped” configuration due to predominant mid-to-upper canal localization of these endophytic lesions, necessitating comprehensive diagnostic evaluation including HPV testing, imaging, cytology, and histologic assessment. G-EAC frequently demonstrates significant local invasion, with involvement of circumferential cervical infiltration, deep myometrial invasion, uterine corpus, parametrium, as well as lymphovascular space invasion (LVSI) and perineural invasion (PNI).4 Most G-EAC cases are diagnosed at advanced stages (FIGO II–IV), exhibiting aggressive metastatic behavior with frequent lymphatic spread, ovarian involvement, and peritoneal dissemination.3 Definitive histopathological examination is the basis for diagnosing G-EAC, where well-defined tumor cells with pale to clear eosinophilic cytoplasm and distinctly large cell size are found. Characteristic nuclear abnormalities are marked nuclear enlargement, severe hyperchromasia, and complete loss of polarity.5 The integrated use of immunohistochemistry (IHC) and mucin histochemistry constitutes a critical ancillary diagnostic approach for G-EAC. This tumor usually shows a distinctive immunophenotypic profile with absent or focal p16 expression, loss of estrogen (ER) and progesterone receptors (PR), and p53 mutation which helps distinguish it from HPV associated usual-type endocervical adenocarcinoma and benign counterparts.6 Notably, a diagnostic caveat exists wherein rare cases of both UEA and G-EAC may exhibit diffuse p16 positivity and wild-type p53 expression.5,7 The PAS stain demonstrates fuchsia-stained mucin in G-EAC, providing modest diagnostic utility in evaluation.7 G-EAC exhibits complex and heterogeneous features in both histopathological characteristics and immunophenotypic expression. Accurate distinction of G-EAC from other cervical lesions necessitates careful histopathologic and immunohistochemical evaluation integrated with clinical and imaging correlation. The patient in this study was incidentally found to have a cervical mass during CT evaluation for cholecystolithiasis and TCT demonstrated HSIL with negative HPV and Squamous Cell Carcinoma Antigen (SCC) results, indicative of HPV-independent carcinoma.
Cervical adenocarcinoma accounts for approximately 20–25% of all cervical carcinomas, with G-EAC being the second most common subtype following UEA.2,8,9 However, G-EAC has a significantly worse prognosis than UEA, with respective 5-year survival rates of 30% and 74%.2,10 G-EAC has significantly worse prognosis than UEA in the disease of early stage (Ia-Ib1), having the same outcome as in advanced stages (Ib2-II), demonstrating its distinct aggressive behavior during early progression, along with higher recurrence rates and higher incidence in advanced stages.11 The deep endocervical location of G-EAC lesions frequently complicates early diagnosis, necessitating histopathological confirmation with immunohistochemical analysis, while transvaginal ultrasound and pelvic MRI provide critical supplemental information for comprehensive diagnostic evaluation and surgical planning. This histological subtype typically presents as infiltrative endophytic lesions without exophytic components or distinct mass formation, often leading to radiological understaging.5 G-EAC lesions typically infiltrate the mid-to-upper endocervical stroma, appearing as barrel-shaped cervical enlargement with stromal thickening and cystic vascular spaces on ultrasound, while MRI more accurately delineates stromal invasion and metastatic spread through multiparametric imaging. Solid-predominant G-EAC is typically characterized as infiltrative masses with poorly defined margins, with T1 isointensity, T2 mild hyperintensity, restricted diffusion on DWI, and frequent cystic components. Cystic-predominant G-EAC is generally characterized by the presence of the “cosmos sign” - an inherently solid/cystic nidus in the middle with peripheral cysts, which is T1 hypointensity and high T2 hyperintensity.12 G-EAC frequently exhibits diffuse infiltration patterns that often extend beyond radiologically apparent tumor boundaries on MRI.13 Based on the patient’s auxiliary test results and gynecological examination findings, the case indicates at least FIGO 2018 stage IIA2 cervical carcinoma.
Treatment and Prognosis
G-EAC does not have uniform treatment protocols, where individualized therapy follows standard cervical cancer regimens. Surgical exploration revealed an atrophic uterus with 2.5 cm cervical canal expansion, normal bilateral adnexa, and no macroscopic abdominopelvic masses or lymphadenopathy. The patient subsequently underwent radical hysterectomy with lymphadenectomy, and definitive pathology demonstrated HPV-independent gastric-type adenocarcinoma (Silva C) with bilateral internal iliac nodal and ovarian metastases, consistent with its characteristic dissemination pattern. Adjuvant postoperative treatment is indicated in G-EAC patients who develop any high-risk pathological features including lymph node positivity, positive margins, or parametrial invasion. Given the confirmed parametrial invasion and nodal metastases, the patient completed adjuvant chemoradiation for this highly aggressive G-EAC variant known for its metastatic potential. G-EAC is predominantly diagnosed at advanced stages, with 59% of patients presenting with FIGO stage II–IV disease at initial diagnosis. G-EAC is typically diagnosed at advanced stages (59% FIGO II–IV), with 39% of cases showing metastases at primary surgery, which is linked with significantly reduced progression-free survival (PFS) and overall survival(OS).3 Current G-EAC management employs conventional cervical cancer protocols (surgery for early-stage disease, chemoradiation for advanced stages), yet these treatments have less than optimal efficacy against its distinct biology, evidenced by its significantly reduced radiosensitivity compared to HPV-associated carcinomas (50% versus 81.8% response rate) on retrospective analyses.11 Additionally, Kojima et al presented much lower response rates to neoadjuvant carboplatin-docetaxel chemotherapy in G-EAC groups.12 G-EAC’s poorer prognosis is attributed to diagnostic presentation delays in early-stage detection and inherent drug resistance to chemoradiotherapy. Postoperative histopathological examination predominantly confirms the diagnosis of G-EAC. For localized early-stage disease, comprehensive preoperative assessment guides surgical management involving radical hysterectomy with bilateral salpingo-oophorectomy, systematic pelvic lymphadenectomy, and selective para-aortic lymphadenectomy when indicated, preceded by meticulous intraoperative exploration. Chinese Expert consensus recommends prophylactic omentectomy/appendectomy with metastasectomy during primary cytoreduction for G-EAC, given the high peritoneal dissemination risk, with liberalized adjuvant chemoradiation indications. In advanced disease, the primary treatment is concurrent chemoradiation ± targeted therapy.14 Neoadjuvant chemotherapy (NACT) with TC significantly improves resectability in locally advanced cervical cancer, particularly for bulky tumors or surgically complex cases, as evidenced by clinical studies.15 Three cycles of neoadjuvant paclitaxel-carboplatin chemotherapy achieved significant tumor downstaging in this bulky cervical lesion, demonstrating marked volume reduction and enhanced lesion demarcation to optimize surgical resectability.
Conclusion
The asymptomatic patient presented with an incidental cervical mass. G-EAC’s diagnostic dilemma is a result of its rarity, the absence of specific symptoms, and typical deep endocervical lesions that frequently escape routine screening detection. Clinicians need to have a strong suspicion of G-EAC in HPV-negative women with radiologic cervical abnormality, as the aggressive invasive, chemoradioresistant, and highly recurrent high-grade malignancy necessitates early detection for ideal prognostic stratification. Clinicians should prioritize integrated assessment of serum tumor markers, advanced imaging, and cervical screening findings, with immunohistochemical-guided biopsies for suspicious lesions to optimize diagnostic accuracy. The pathogenesis of G-EAC remains poorly understood, necessitating novel therapeutic strategies that integrate mechanistic investigations of tumorigenesis, G-EAC specific clinical trials, and multimodal approaches combining surgery, chemoradiation, targeted therapy, and immunotherapy to address its poor therapeutic outcomes. The concurrent progress of prevention and screening techniques for non-HPV-associated cervical carcinomas is essential to improving survival outcomes and quality of life.
Statement of Ethics and Informed Consent
The case report was approved by the Research Ethics Committee of The First Affiliated Hospital of Guangzhou Medical University (ES-2025-K231-01). Written consent was obtained from the patient for the publication of this article and its contents, including the clinical details and images.
Acknowledgment
We express our sincere gratitude to the patient for providing informed consent for the publication of this case report. We also acknowledge the multidisciplinary team for their collaboration in the diagnosis and management of this case.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported in part by the National Science Foundation of China (81302249), the Natural Science Foundation of Guangdong Province (2021A1515010941), the Science and Technology Program of Guangdong (2014A020212609) and the Guangzhou Municipal Science and Technology Program Project Agreement (2024A03J1159).
Disclosure
The authors declare no competing interests.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–7. doi:10.3322/caac.21660
2. Stolnicu S, Barsan I, Hoang L, et al. International endocervical adenocarcinoma criteria and classification (IECC): a new pathogenetic classification for invasive adenocarcinomas of the endocervix. Am J Surg Pathol. 2018;42(2):214–226. doi:10.1097/PAS.0000000000000986
3. Karamurzin YS, Kiyokawa T, Parkash V, et al. Gastric-type endocervical adenocarcinoma: an aggressive tumor with unusual metastatic patterns and poor prognosis. Am J Surg Pathol. 2015;39(11):1449–1457. doi:10.1097/PAS.0000000000000532
4. Pirog EC, Park KJ, Kiyokawa T, et al. Gastric-type adenocarcinoma of the cervix: tumor with wide range of histologic appearances. Adv Anat Pathol. 2019;26(1):1–12. doi:10.1097/PAP.0000000000000216
5. Kerwin CM, Markese M, Moroney MR, Smith LP, Patel NU. Adenocarcinoma of the uterine cervix, gastric-type (GAS): a review of the literature focused on pathology and multimodality imaging. Abdom Radiol. 2023;48(2):713–723. doi:10.1007/s00261-022-03724-w
6. Garg S, Nagaria TS, Clarke B, et al. Molecular characterization of gastric-type endocervical adenocarcinoma using next-generation sequencing. Mod Pathol. 2019;32(12):1823–1833. doi:10.1038/s41379-019-0305-x
7. Stolnicu S, Park KJ, Kiyokawa T, Oliva E, McCluggage WG, Soslow RA. Tumor typing of endocervical adenocarcinoma: contemporary review and recommendations from the international society of gynecological pathologists. Int J Gynecol Pathol. 2021;40(Suppl 1):S75–S91. doi:10.1097/PGP.0000000000000751
8. Stolnicu S, Hoang L, Chiu D, et al. Clinical outcomes of HPV-associated and unassociated endocervical adenocarcinomas categorized by the international endocervical adenocarcinoma criteria and classification (IECC). Am J Surg Pathol. 2019;43(4):466–474. doi:10.1097/PAS.0000000000001224
9. Yang J, Peng Y, Ding Y, et al. The clinicopathological and molecular characteristics of endocervical gastric-type adenocarcinoma and the use of claudin18.2 as a potential therapeutic target. Mod Pathol. 2024;37(10):100569. doi:10.1016/j.modpat.2024.100569
10. Park E, Kim SW, Kim S, et al. Genetic characteristics of gastric-type mucinous carcinoma of the uterine cervix. Mod Pathol. 2021;34(3):637–646. doi:10.1038/s41379-020-0614-0
11. Nishio S, Mikami Y, Tokunaga H, et al. Analysis of gastric-type mucinous carcinoma of the uterine cervix - An aggressive tumor with a poor prognosis: a multi-institutional study. Gynecol Oncol. 2019;153(1):13–19. doi:10.1016/j.ygyno.2019.01.022
12. Sankai Gynecology Study Group, Kojima A, Shimada M, Mikami Y, et al. Chemoresistance of gastric-type mucinous carcinoma of the uterine cervix: a study of the sankai gynecology study group. Int J Gynecol Cancer. 2018;28(1):99–106. doi:10.1097/igc.0000000000001145
13. Saida T, Sakata A, Tanaka YO, et al. Clinical and MRI characteristics of uterine cervical adenocarcinoma: its variants and mimics. Korean J Radiol. 2019;20(3):364–377. doi:10.3348/kjr.2018.0458
14. Gong L, Zhang JW, Yin RT, et al. Safety and efficacy of neoadjuvant chemotherapy followed by radical surgery versus radical surgery alone in locally advanced cervical cancer patients. Int J Gynecol Cancer. 2016;26(4):722–728. doi:10.1097/IGC.0000000000000658
15. Yu XL, Wu MF, Ding L, Yang J, Bai SM. Enhanced efficacy of neoadjuvant chemotherapy with nab-paclitaxel and platinum for locally advanced cervical cancer. Cancer Manag Res. 2021;13:9297–9304. doi:10.2147/CMAR.S343602
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.