Back to Journals » Research and Reports in Urology » Volume 13
Fused Supernumerary Kidney with Single Pelvis and Ureter; Presenting with Stones: A Case Report and Literature Review
Authors Berhe T, Hassen SM, Gebrehiwot FG ![]() , Mummed FO
, Mummed FO ![]() , Issack FH
, Issack FH ![]() , Dino MS, Akkasa SS
, Dino MS, Akkasa SS ![]() , Zerihun GA, Gebreselassie KH
, Zerihun GA, Gebreselassie KH ![]()
Received 11 November 2021
Accepted for publication 15 December 2021
Published 23 December 2021 Volume 2021:13 Pages 853—857
DOI https://doi.org/10.2147/RRU.S347328
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Guglielmo Mantica
Tekleberhan Berhe, Seid Mohammed Hassen, Fitsum Gebreegziabher Gebrehiwot, Ferid Ousman Mummed, Feysel Hassen Issack, Masresha Solomon Dino, Sena Sefera Akkasa, Getachew Adamu Zerihun, Kaleab Habtemichael Gebreselassie
Urology Unit, Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Ferid Ousman Mummed
Urology Unit, Department of Surgery, St. Paul’s Hospital Millennium Medical College, Swaziland St., Addis Ababa, Ethiopia
Tel +251904650705
Email [email protected]
Introduction: A supernumerary kidney is an extremely rare congenital anomaly, defined as the presence of one or more extra kidneys. Thus far, there have been less than 100 cases reported in the medical literature. It has its capsule, vascular supply, and collecting system. It frequently causes diagnostic challenges in clinical practice. The supernumerary kidney can be symptomatic due to the presence of stone.
Case Presentation: We present a case of a 19-year-old male patient who came to our clinic with the complaint of abdominal pain. On computed tomography urography (CTU), he was found to have a caudally located left fused supernumerary kidney with a separate vascular supply. Both left kidneys had a separately draining calyceal systems uniting at the left renal pelvis and drained by a single ureter. Multiple left renal stones (largest measures 4cm x 2.2cm) in both kidneys were also seen. The stones were removed surgically by doing pyelolithotomy and radial nephrolithotomy. The patient was doing well during follow-up visits with the improvement of abdominal pain.
Conclusion: Supernumerary kidney is a very rare congenital renal anomaly. This case is even unique, because of the fused supernumerary kidney and the presence of a single left renal pelvis and ureter. Imaging is very essential for planning surgical intervention. Stones in such kidneys can be managed with nephrolithotomy and/or pyelolithotomy.
Keywords: accessory kidney, congenital anomalies, fused kidney, renal calculi, nephrolithotomy, pyelolithotomy
Introduction
A supernumerary kidney is an extremely rare congenital renal anomaly, defined by the presence of one or more extra kidneys. Less than 100 cases have been reported in the medical literature. True incidence cannot be estimated because of its infrequent occurrence, and fused supernumerary kidney is even rarer. It is an accessory organ with a distinct well-encapsulated capsule, vascular supply, and collecting system.1,2
It can be either attached to the ipsilateral native kidney or a completely separated kidney. It may have single or double ureters. They are usually asymptomatic, but may rarely become symptomatic. A supernumerary kidney can be symptomatic due to the presence of stone.3 Although urinary stasis and recurrent UTI are the main risk factors, metabolic abnormalities have been suggested to contribute to stone formation. Stones in such kidneys with anomalous anatomy pose a particular challenge for the urologist.4
Radiological imaging such as computed tomography (CT) or magnetic resonance imaging (MRI) is used to confirm the diagnosis as well as to identify the anatomic variation and abnormal vasculature.3 Here, we report a case of renal stones in the left fused supernumerary kidney with a single renal pelvis and ureter.
Case Presentation
A 19-year-old male patient presented to our clinic with the complaint of intermittent left lower abdominal pain of one-year duration and increasing in severity for the last two months. He does not have any comorbidities. There was no family history of kidney disease. His physical examination was unremarkable. Routine laboratory investigations including CBC (complete blood count), serum electrolytes, serum creatinine, BUN (blood urea nitrogen), and urinalysis were normal.
Abdominal ultrasound showed a hydronephrotic left kidney with multiple stones. He further underwent computed tomography urography (CTU), which showed two fused left kidneys and a single right kidney (Figure 1A–D). The right kidney measures 11cm x 4.8cm and had normal anatomical findings. The cranially located kidney on the left side measures 11.5 cm x 5.1cm and the caudal accessory kidney measures 9cm x 4.3cm. The PCS (pelvicalyceal system) of the upper kidney was located anteromedially (Figure 1A) and that of the lower kidney was malrotated, facing anterolaterally (Figure 1B). There are two separate renal arteries (both arise from the aorta) and renal veins (Figure 2A and B). Multiple calyceal stones of varying sizes were seen in both left kidneys and one big obstructing stone (4cm x 2.2cm) in the common renal pelvis (Figure 2C). The left fused kidneys had a separately draining calyceal system with a common extrarenal left pelvis and a single ureter (Figure 2D).
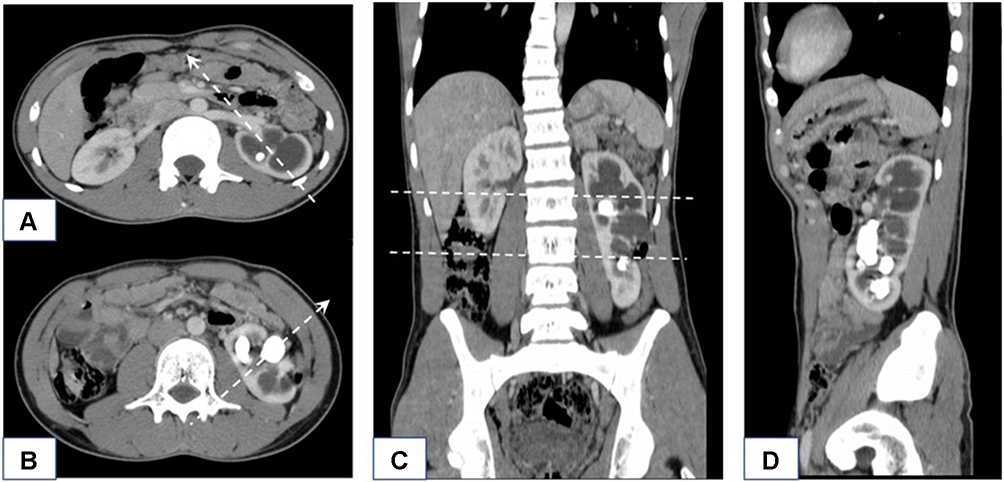 |
Figure 1 CT with Axial (A and B), Coronal (C), and Sagittal (D) views show two left fused kidneys with dilated PCS and multiple renal stones. The native kidney is located cranially and facing anteromedially (A). The caudally placed supernumerary kidney is malrotated, facing anterolaterally (B) as shown by arrows. Abbreviation: PCS, pelvicalyceal system. |
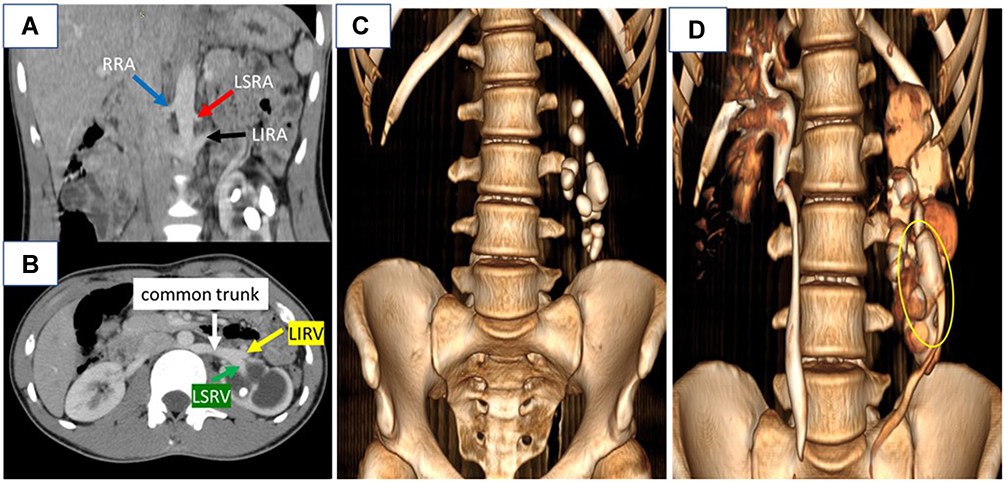 |
Figure 2 CT shows two left renal arteries (superior- red arrow, inferior- black arrow) and single right renal artery arising from the aorta (A), and two left renal veins (superior- green arrow, inferior- yellow arrow) forming a common trunk before joining IVC (B). A 3D reconstruction shows left multiple renal stones (C), and separately draining calyceal systems with a common renal pelvis and single ureter on excretory phase as shown by the yellow circle (D). Abbreviations: RRA, right renal artery; LSRA, left superior renal artery; LIRA, left inferior renal artery; LIRV, left inferior renal vein; LSRV, left superior renal vein. |
After informed consent, the patient was operated on. The intraoperative finding was two fused left kidneys in an “S-shaped” manner. The caudally placed supernumerary kidney was smaller in size and had a rotational anomaly, facing anterolaterally. Both kidneys had a common renal pelvis and ureter which are located along their anterolateral aspect. There was a dilated renal pelvis with a palpable big stone inside (Figure 3A). Left pyelotomy was done, and there was communication between the two fused kidneys. So, we were able to access both kidneys through the common renal pelvis, and most of the stones were extracted (Figure 3B). Radial nephrotomy was also done to remove the remaining stones in the native kidney. A total of 13 stones were removed (Figure 3C), and a Double-J stent was placed. The patient was doing well, with an improvement of abdominal pain, during the subsequent follow-up visits. Postoperative control X-ray showed 1.5cm x 1cm residual stone (Figure 4). We decided on extracorporeal shock wave lithotripsy (ESWL) for the treatment of residual stone. Since ESWL is not available in our hospital, the patient was referred to another hospital where the service was available.
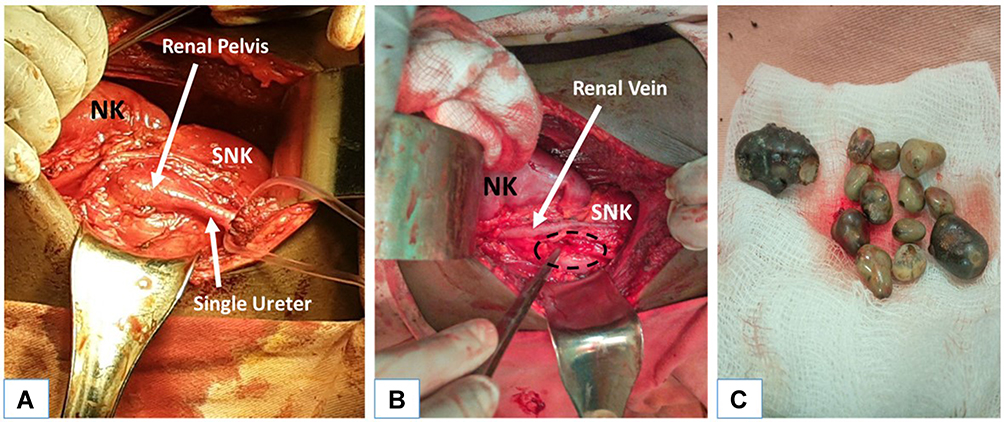 |
Figure 3 Intra-operative pictures (A–C). Fused left kidneys (relatively small caudally located SNK and normally placed NK) with single renal pelvis and ureter (A). Left pyelotomy site with access to both kidneys (dashed circle) (B). Multiple extracted renal stones (C). Abbreviation: NK, native kidney; SNK, supernumerary kidney. |
 |
Figure 4 Postoperative X-ray shows a 1.5 x 1cm radio-opaque structure at the level of L4 and Double-J stent on the left side. |
Discussion
A supernumerary kidney is a very rare congenital renal anomaly. It is an accessory organ that has a similar structure and function to the native kidney. Its embryological development has not been fully understood. However, the reason can be an abnormally divided nephrogenic cord into two metanephric blastemas. As a result, two kidneys are formed on the same side with completely or partially duplicated ureteral bud.1–3,5
A supernumerary kidney is more common on the left side. It is distinguished from the ipsilateral native kidney by its smaller size and abnormal position (usually caudal to the native kidney). When located caudally, they are commonly associated with a bifid ureter.3,5 But in the index case, the accessory kidney is located caudal to the native kidney with a common renal pelvis and ureter.
A supernumerary kidney is an accessory organ with a well-defined capsule, and a separate blood supply as well as collecting system. It may be attached to the ipsilateral native kidney by fibrous or parenchymal tissue. A duplex kidney is a common differential diagnosis, which may not have a separate blood supply and capsule.1,5,6 In the index case, the accessory kidney was partially fused with the native left kidney with a distinct collecting system uniting at the common renal pelvis and a separate blood supply.
A supernumerary kidney usually remains asymptomatic. However, several associated conditions such as hydronephrosis, renal stones, infection, and renal neoplasms may cause symptoms such as abdominal pain, hematuria, fever, and abdominal mass.3 Our patient had vague abdominal pain due to hydronephrosis and multiple renal stones.
The most common associated congenital anomalies are horseshoe kidney, ectopic ureter, ureteral or vaginal atresia, imperforate anus, coarctation of the aorta, ventricular septal defects, and meningomyelocele.1,3 Our patient had no such associated congenital anomalies.
Imaging such as ultrasound (US), CT scan, and MRI are essential to confirm the diagnosis. However, if surgical intervention is planned, CT angiography or MR angiography is recommended to demonstrate the blood supply and the anatomical environment.1,3 To date, no simple US parameters for detecting renal abnormalities, especially small kidneys, have been reported. The small kidney may be screened by two-dimensional measurements on US examination using the cutoff value of the ratio of the estimated area of 74.26% or maximum renal length of 4.97 cm.7
The management depends on the presence of associated symptoms or pathologies of the supernumerary kidney. No treatment is required unless the patient is symptomatic. Surgical intervention is challenging because of its peculiar vascular anatomy, and thus the correct diagnosis is of utmost importance for the individual patients.1,5 Stones and their treatment in the supernumerary kidney have not been reported vastly in the literature.
Although urinary stasis and recurrent UTI are the main risk factors, metabolic abnormalities have been suggested to contribute to stone formation.4,7,8 Stones in such kidneys with anomalous anatomy pose a particular challenge for the urologist. The management should be individualized, considering the function, location, and anatomy of the kidney, as well as the size and site of the stone. The possible surgical procedures include open surgery, ESWL, percutaneous nephrolithotomy (PCNL), ureterorenoscopy (URS), or laparoscopic surgery.3,4,9
URS is a minimally invasive technique with good stone clearance and fewer complications. Flexible URS is not widely available and it needs expertise as well as the need for a repeat procedure. PCNL in such kidneys is challenging, due to the varied anatomy of the PCS and vasculature. The chances of developing complications would be high and the surgeon’s unfamiliarity in accessing such kidney is also another problem. Laparoscopic surgery can be done for large and complex stones with better visualization and stone clearance, and pyeloplasty can be performed simultaneously. But it’s not widely available and needs expertise.3,9,10
ESWL remains one of the effective and less invasive options for stones <2 cm in anomalous kidneys. Due to anatomic abnormalities, this technique is usually associated with a low clearance rate and the need for auxiliary treatments.8–10
Our patient had multiple and large stones in his left fused kidneys with moderate hydronephrosis and rotational abnormality. Despite the abovementioned types of stone management, the only available treatment option we had was open surgical removal via pyelolithotomy with radial nephrolithotomy. So, the limitations related to our case are the unavailability of CT/MR angiography and other options of stone treatment in our setup.
Conclusion
A supernumerary kidney is an extremely rare congenital anomaly. The index case is even more unique in many aspects. First, the accessory kidney is fused to the native kidney. Second, the fused kidneys have a common renal pelvis and single ureter. CT/MR angiography is essential for the evaluation of its vascular anatomy and planning surgical intervention. Stones management in such kidneys should be tried with a less invasive procedure.
Abbreviations
BUN, blood urea nitrogen; CBC, Complete blood count; CT, Computed tomography; CTU, Computed tomography urography; ESWL, Extracorporeal shock wave lithotripsy; MRI, Magnetic resonance imaging; NK, Native Kidney; PCNL, Percutaneous nephrolithotomy; PCS, Pelvicalyceal system; SNK, Supernumerary Kidney; URS, Ureterorenoscopy; US, Ultrasound.
Data Sharing Statement
All the generated data are included in this article.
Ethics Approval and Consent to Participate
No institutional review board approval was required.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Funding
The authors received no funding for this work.
Disclosure
Ferid Ousman Mummed is the guarantor for this study. The authors have no competing interests in this work.
References
1. Manandhar S, Khanal A. Fused right supernumerary kidney: a case report. JNMA J Nepal Med Assoc. 2019;57(219):376–378.
2. Sen V, Bozkurt IH, Yonguc T, Aydogdu O, Basmaci I. A rare case of supernumerary fused and malrotated kidney. Int Braz J Urol. 2017;43(3):561–562. doi:10.1590/s1677-5538.ibju.2015.0420
3. Parmar K, Manoharan V, Kumar S, Khanna A, Thakur A. Supernumerary kidney with stone: successfully managed with semirigid ureteroscopy and laser lithotripsy. J Endourol Case Rep. 2019;5(3):92–95. doi:10.1089/cren.2019.0006
4. Gross AJ, Fisher M. Management of stones in patients with anomalously sited kidneys. Curr Opin Urol. 2006;16(2):100–105. doi:10.1097/01.mou.0000193380.16480.e1
5. Suresh J, Gnanasekaran N, Dev B. Fused supernumerary kidney. Radiol Case Rep. 2015;6(4):552. doi:10.2484/rcr.v6i4.552
6. da Silva RM, Chaib Neto J, de Morais Júnior MF. Supernumerary kidney with pelvic communication and a single ureter. Radiol Bras. 2018;51(1):66–67. doi:10.1590/0100-3984.2016.0094
7. Kon M, Nakamura M, Moriya K, et al. What are the optimal renal ultrasound parameters for detecting small kidney in young children? Res Rep Urol. 2021;13:767–772. doi:10.2147/RRU.S318793
8. Küpeli B, Isen K, Biri H, et al. Extracorporeal shockwave lithotripsy in anomalous kidneys. J Endourol. 1999;13:349–352. doi:10.1089/end.1999.13.349
9. El-Nahas AR, Shokeir AA. Minimally invasive treatment of calculi in renal anomalies. In: Urolithiasis. Talati J, Tiselius HG, Albala D, Ye Z, editors. London: Springer; 2012. doi:10.1007/978-1-4471-4387-1_73
10. Gupta M, Lee MW. Treatment of stones associated with complex or anomalous renal anatomy. Urol Clin North Am. 2007;34(3):431–441. doi:10.1016/j.ucl.2007.04.004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.