Back to Journals » Clinical Ophthalmology » Volume 20
Functional Intermediate Vision and Pupil-Dependent Optical Behavior After Implantation of a Segmented Refractive Multifocal Intraocular Lens
Received 12 February 2026
Accepted for publication 6 May 2026
Published 20 May 2026 Volume 2026:20 598921
DOI https://doi.org/10.2147/OPTH.S598921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Wei Cui,1– 4 Songlin Yang1
1Department of Ophthalmology, Peking University First Hospital, Beijing, People’s Republic of China; 2Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, Qingdao, Shandong, People’s Republic of China; 3State Key Laboratory Cultivation Base, Shandong Provincial Key Laboratory of Ophthalmology, Qingdao, Shandong, People’s Republic of China; 4School of Ophthalmology, Shandong First Medical University, Qingdao, Shandong, People’s Republic of China
Correspondence: Songlin Yang, Email [email protected]
Purpose: To evaluate functional visual outcomes, defocus characteristics, pupil-dependent intraocular higher-order aberrations (HOAs), and their interrelationships in eyes implanted with a segmented refractive multifocal intraocular lens (MIOL), a design intended to provide both near and intermediate visual function.
Methods: This retrospective observational study included 88 eyes (64 patients) implanted with a segmented refractive MIOL (SBL-3) and a monofocal IOL (Akreos Adapt AO) as a reference. Postoperative functional visual acuity at distance, intermediate, and near was assessed. Distance-corrected defocus curves were obtained. Intraocular wavefront aberrations were measured under bright and dim lighting conditions, and pupil diameter was recorded. Correlation analyses were performed to explore the relationships between pupil diameter, intraocular HOAs, and intermediate visual acuity in the SBL-3 group.
Results: Distance visual acuity did not differ significantly between groups. The SBL-3 group demonstrated significantly better uncorrected and distance-corrected intermediate and near visual acuity compared with the monofocal reference group. The defocus curve of the SBL-3 IOL showed a relatively smooth functional visual profile across intermediate defocus levels. Intraocular HOAs, particularly coma and trefoil, were significantly higher in the SBL-3 group and exhibited strong pupil-dependent behavior under both bright and dim conditions. However, no significant linear correlations were observed between intraocular HOAs and intermediate visual acuity.
Conclusion: The segmented refractive multifocal IOL provided improved functional intermediate vision while exhibiting pupil-dependent increases in intraocular HOAs. These findings provide clinically relevant insights into the pupil-dependent optical behavior of segmented refractive MIOLs and suggest that increased HOAs may not necessarily compromise functional intermediate visual acuity.
Keywords: segmented refractive multifocal intraocular lens, intermediate visual acuity, higher-order aberrations, pupil-dependent optical behavior
Introduction
Cataract surgery has evolved from merely aiming at vision restoration to a surgical procedure dedicated to optimizing functional vision at all distances.1 In modern daily activities, intermediate-distance vision plays a crucial role in tasks such as operating computers, checking instrument panels, and indoor activities.2 Therefore, the design of intraocular lenses (IOLs) that can provide good intermediate-distance visual performance while taking into account distance vision has attracted increasing attention.3
Multifocal intraocular lenses (MIOLs), including diffractive and refractive designs, have been developed to address spectacle dependence.4 However, traditional multifocal IOLs are often associated with increased higher-order aberrations (HOAs), photic phenomena, and reduced contrast sensitivity, which may compromise optical quality.5 Segmented refractive multifocal IOLs represent a distinct design concept, characterized by an asymmetric near segment that redistributes light energy to extend functional vision rather than creating discrete focal points.6
Owing to their asymmetric optical design, segmented refractive multifocal IOLs exhibit pupil-dependent optical behavior.7 Previous optical bench and clinical studies have demonstrated that pupil size may influence the magnitude and profile of induced HOAs, particularly coma and trefoil.8 In addition, several studies have reported that the relationship between HOAs and functional visual performance is complex and not strictly linear, with certain aberration profiles potentially contributing to an extended depth of focus rather than deteriorating visual quality.9–11
Despite increasing clinical use of segmented refractive multifocal IOLs, the relationship between pupil diameter, intraocular HOAs, and functional intermediate vision remains incompletely understood. In particular, it is unclear whether pupil-dependent increases in HOAs directly compromise intermediate visual acuity or contribute to an extension of depth of focus through non-linear optical mechanisms.
From a clinical perspective, understanding pupil-dependent optical behavior is important for optimizing patient selection and preoperative counseling when considering implantation of multifocal IOLs.
Therefore, the purpose of this study was to evaluate postoperative functional visual acuity, defocus characteristics, and pupil-dependent intraocular HOAs in eyes implanted with a segmented refractive MIOL, using a monofocal IOL as a reference. We specifically hypothesized that pupil-dependent increases in intraocular HOAs would not necessarily compromise functional intermediate visual acuity, suggesting a non-linear relationship between optical aberrations and visual performance.
Materials and Methods
Study Design and Participants
This retrospective observational study analyzed anonymized clinical data from consecutive patients who underwent uncomplicated cataract surgery with implantation of either a segmented refractive MIOL (SBL-3; Lenstec Inc., St. Petersburg, FL, USA) or a monofocal IOL (Akreos Adapt AO; Bausch & Lomb, Rochester, NY, USA) at Peking University First Hospital between November 2017 and January 2019. A total of 88 eyes from 64 patients were included in the study. The monofocal IOL group was included as a reference control to provide a baseline comparison of visual and optical outcomes.
Inclusion criteria were age-related cataract, absence of ocular comorbidities affecting visual function, and availability of complete postoperative visual acuity and wavefront aberration data. Exclusion criteria included previous ocular surgery, corneal pathology, retinal disease, glaucoma, pupillary abnormalities, neuro-ophthalmological problems, intraoperative complications, or postoperative complications that could influence visual outcomes.
Surgical Procedure
All surgeries were performed by one experienced surgeon using a standard phacoemulsification technique through a clear corneal incision. In the SBL-3 group, a SBL-3 MIOL was implanted in the capsular bag. In the reference group, an Akreos Adapt AO IOL was implanted.
Target postoperative refraction was emmetropia in all eyes. No intraoperative or postoperative complications were observed.
Postoperative Examinations
Postoperative examinations were performed at 1 month after surgery. Uncorrected and corrected distance visual acuity (UDVA and CDVA) were measured at 4 m using standardized logMAR charts. Intermediate visual acuity was assessed at 80 cm, which represents a standard intermediate viewing distance in daily activities, and near visual acuity was measured at 40 cm. Both uncorrected and distance-corrected intermediate and near visual acuities (UIVA, DCIVA, UNVA, and DCNVA) were recorded.
Defocus Curve Assessment
Distance-corrected defocus curves were obtained by adding spherical lenses in 0.50 diopter (D) steps from +0.50 D to −3.00 D while maintaining best distance correction. Visual acuity at each defocus level was recorded in logMAR units.
Wavefront Aberration Analysis
Intraocular wavefront aberrations were measured using a Hartmann–Shack aberrometer OPD-Scan III (Nidek Co., Ltd., Gamagori, Aichi, Japan). Measurements were obtained under bright and dim conditions. Pupil diameter was recorded simultaneously.
Total HOAs (root mean square, RMS), coma, trefoil, and spherical aberration were analyzed. Only intraocular aberrations were included in the analysis.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation. Normality of data distribution was assessed using the Shapiro–Wilk test. Comparisons between groups were performed using independent-samples t tests or nonparametric tests as appropriate. Categorical variables were compared using the chi-square test.
Spearman correlation analyses were performed to evaluate the relationships between pupil diameter, intraocular HOAs, and functional intermediate visual acuity in the SBL-3 group. Correlation coefficients and corresponding P values were calculated. A P value of <0.05 was considered statistically significant.
Because some patients contributed both eyes to the analysis, inter-eye correlation may exist. In this study, both eyes were included in the statistical analysis, and no specific statistical adjustment for clustered data (such as generalized estimating equations or mixed-effects models) was applied. Given the exploratory nature of this study and the relatively limited sample size, inclusion of both eyes was intended to maximize statistical power. This limitation has been acknowledged and discussed in the Discussion section.
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. According to the institutional regulations of Peking University First Hospital, retrospective observational studies using fully anonymized clinical data are exempt from formal ethical approval. The Ethics Committee of Peking University First Hospital confirmed that formal approval was not required. Patient data were anonymized prior to analysis, and the requirement for informed consent was waived due to the retrospective design.
Results
Baseline Characteristics
A total of 88 eyes from 64 patients were included in the analysis, including 46 eyes implanted with the SBL-3 and 42 eyes implanted with the Akreos Adapt AO. Baseline demographic and ocular characteristics are summarized in Table 1. No significant differences were observed between groups in terms of age, sex distribution, keratometric values, or preoperative pupil diameter. Axial length was slightly longer in the Akreos Adapt AO group compared with the SBL-3 group (P = 0.048).
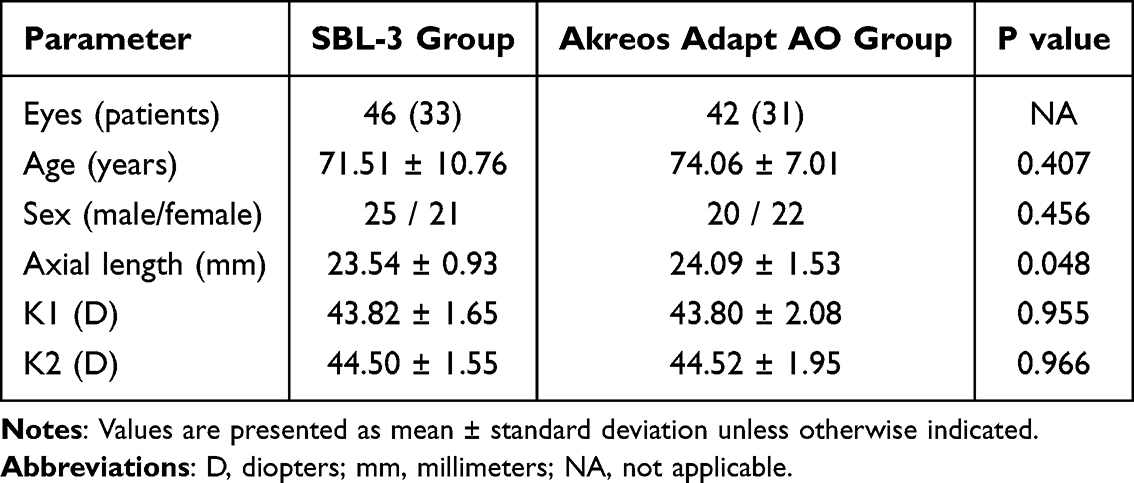 |
Table 1 Baseline Demographic and Ocular Characteristics of the Study Population |
Postoperative Functional Visual Acuity
Postoperative functional visual acuity outcomes are shown in Table 2. There were no significant differences between groups in UDVA and CDVA. In contrast, the SBL-3 group demonstrated significantly better UIVA and DCIVA compared with the Akreos Adapt AO group (both P ≤ 0.001). Similarly, UNVA and DCNVA were significantly better in the SBL-3 group (P < 0.01).
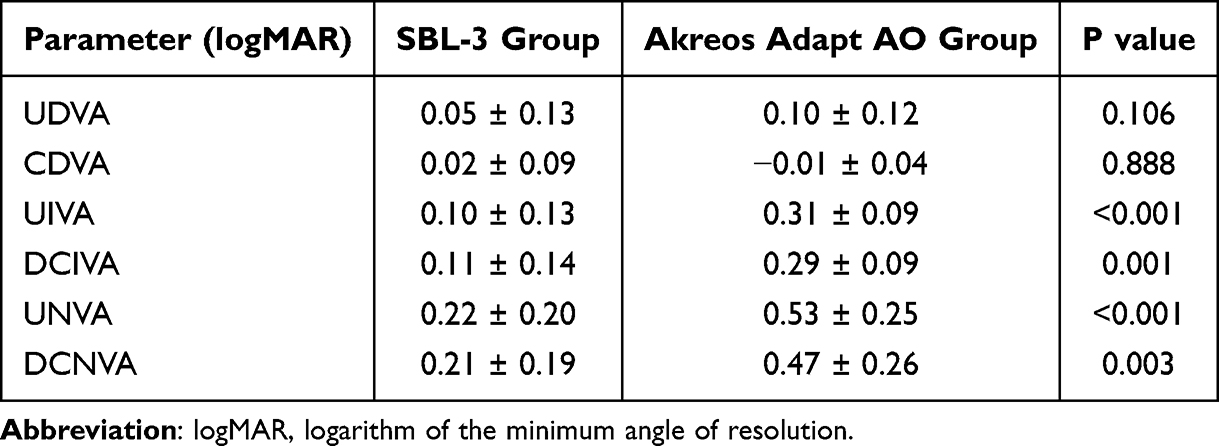 |
Table 2 Postoperative Functional Visual Acuity Outcomes at Different Viewing Distances |
Defocus Curve
The distance-corrected defocus curve of the SBL-3 is shown in Figure 1. The SBL-3 lens demonstrated a relatively smooth functional visual acuity profile across intermediate defocus levels, with gradual decline toward higher negative defocus.
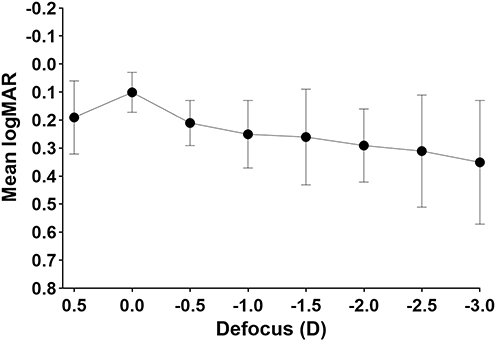 |
Figure 1 Distance-corrected defocus curve of the segmented refractive MIOL. Distance-corrected visual acuity (logMAR) across different defocus levels from +0.50 D to −3.00 D in eyes implanted with the SBL-3. Data are presented as mean ± standard deviation. |
Pupil Diameter and Intraocular HOAs
Intraocular HOAs measured under bright and dim conditions are summarized in Table 3. Pupil diameter did not differ significantly between groups under either lighting condition. However, total HOAs, coma, and trefoil were significantly higher in the SBL-3 group compared with the Akreos Adapt AO group under both bright and dim conditions (all P < 0.001). Spherical aberration did not differ significantly between groups.
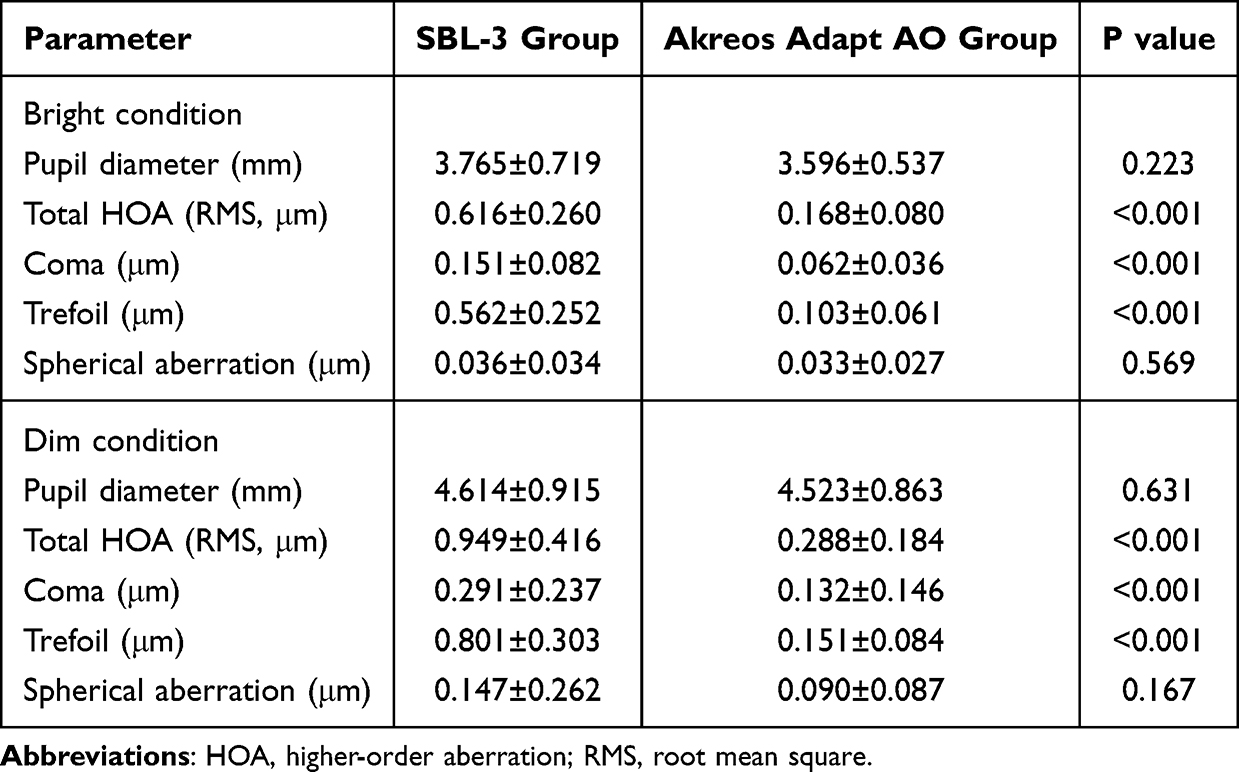 |
Table 3 Pupil Diameter and Intraocular HOAs Under Different Lighting Conditions |
Correlation Analysis
Correlation analysis in the SBL-3 group revealed strong positive correlations between pupil diameter and total HOAs, coma, and trefoil under both bright and dim conditions (all P < 0.001; Table 4). However, no significant correlations were observed between total HOAs and intermediate visual acuity (UIVA or DCIVA).
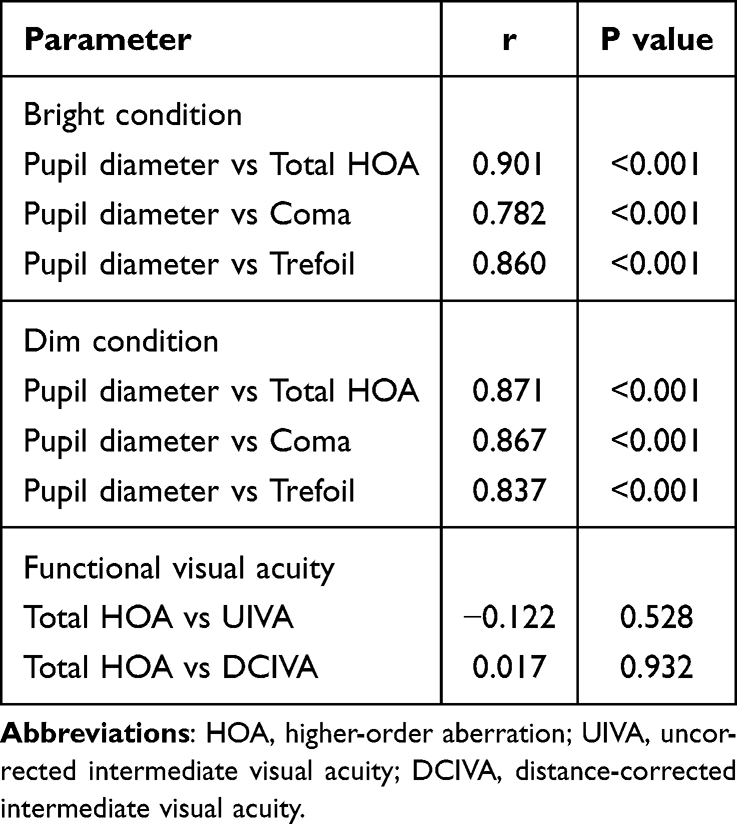 |
Table 4 Correlations Between Pupil Diameter, Intraocular HOAs, and Functional Visual Acuity in the SBL-3 Group |
Relationship Between Pupil Diameter and HOAs
Scatter plots illustrating the relationship between pupil diameter and intraocular HOAs under dim conditions are shown in Figure 2. A strong positive correlation was observed between pupil diameter and both total HOAs and coma.
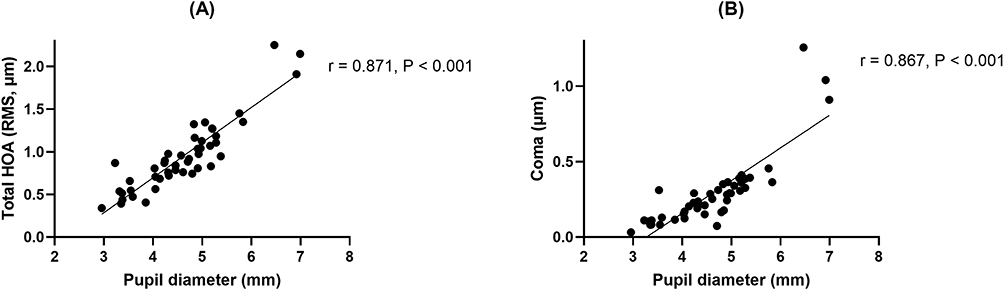 |
Figure 2 Relationship between pupil diameter and intraocular HOAs under dim conditions in the SBL-3 group. (A) Pupil diameter vs total HOA (dim condition): Scatter plot showing the relationship between pupil diameter and total intraocular HOAs (root mean square). (B) Pupil diameter vs coma (dim condition): Scatter plot showing the relationship between pupil diameter and coma aberration. Each dot represents one eye. Solid lines indicate linear regression fits. |
Discussion
The present study evaluated functional visual outcomes, defocus characteristics, pupil-dependent intraocular HOAs, and their interrelationships in eyes implanted with a segmented refractive MIOL. The inclusion of a monofocal IOL group allows comparison with a conventional optical design and helps contextualize the optical behavior of the segmented refractive MIOL. The principal findings can be summarized as follows: first, the segmented refractive IOL provided satisfactory distance vision and significantly improved intermediate and near visual acuity compared with a monofocal reference lens; second, intraocular HOAs, particularly coma and trefoil, were significantly increased and strongly correlated with pupil diameter under different lighting conditions; third, despite the pupil-dependent increase in HOAs, no linear correlation was observed between HOAs and intermediate visual acuity.
The increase in HOAs observed in the segmented refractive IOL group is consistent with the asymmetric optical design of this lens type. Unlike rotationally symmetric diffractive designs, segmented refractive IOLs intentionally redistribute light energy through an asymmetric near segment, which inherently induces certain HOAs, particularly coma and trefoil.12,13 Optical bench and clinical wavefront studies have previously demonstrated that such aberration profiles are characteristic of segmented refractive multifocal designs rather than indicative of suboptimal lens performance.14,15
A notable finding of this study is the strong pupil-dependent behavior of intraocular HOAs in eyes implanted with the segmented refractive IOL. Pupil diameter showed a robust positive correlation with total HOAs, coma, and trefoil under both bright and dim conditions, whereas pupil size itself did not differ between IOL groups. These findings indicate that the observed optical changes are primarily lens-related and become more pronounced with physiological pupil dilation rather than being attributable to interindividual differences in pupil size.16,17
Despite the significant and pupil-dependent increase in HOAs, no linear correlation was identified between total HOAs and intermediate visual acuity. This finding suggests that the relationship between optical aberrations and functional vision in segmented refractive multifocal IOLs is not purely linear.18 Certain aberration profiles may contribute to an extension of depth of focus without directly compromising functional intermediate vision, potentially through non-linear optical effects or neural adaptation mechanisms.10,11
Although the magnitude of HOAs observed in the segmented refractive MIOL group may appear relatively high compared with monofocal IOLs, such aberration profiles are an inherent consequence of the asymmetric optical design.19 These induced aberrations, particularly coma and trefoil, may contribute to an extension of depth of focus rather than a deterioration of functional vision. This phenomenon has been described in previous studies,20 suggesting that certain aberration patterns may enhance intermediate visual performance through non-linear optical mechanisms and neural adaptation.
Several recent studies have explored the relationship between higher-order aberrations (HOAs) and functional vision in multifocal intraocular lenses (IOLs). For example, a study by Rua Amaro21 found that increased HOAs are common in segmented refractive IOLs and may contribute to the extension of depth of focus, similar to our findings. Additionally, Diao22 reported that pupil diameter has a significant role in modulating these optical errors, which aligns with our results showing pupil-dependent HOA changes. However, other recent studies such as Parimi23 observed less impact of HOAs on functional vision, suggesting that clinical outcomes may depend not only on optical aberrations but also on neural adaptation and patient-specific factors. Our findings add to this body of literature by providing clinical data from a real-world postoperative population and emphasize the importance of considering pupil-dependent aberrations when selecting IOLs for cataract patients.
Compared with previous studies, the present study provides a comprehensive clinical evaluation integrating functional visual acuity, defocus characteristics, and pupil-dependent intraocular HOAs within the same cohort. In particular, this study uniquely focuses on the relationship between pupil diameter, intraocular aberrations, and intermediate visual acuity, which has not been fully explored in prior clinical investigations of segmented refractive MIOLs.
Furthermore, the inclusion of a monofocal IOL as a reference group allows better contextualization of the optical and functional outcomes, enhancing the clinical interpretability of the findings. These aspects distinguish the present study from previous reports and highlight its contribution to understanding the pupil-dependent optical behavior of segmented refractive MIOLs in real-world clinical settings.
From a clinical standpoint, these findings provide clinically relevant insights into the optical behavior of segmented refractive MIOLs and may assist surgeons in optimizing patient selection and preoperative counseling. While pupil dilation accentuates HOAs, this does not necessarily translate into inferior intermediate visual function. Preoperative assessment of pupil behavior may therefore help identify suitable candidates and optimize patient counseling.24
This study has several limitations. Its retrospective design and relatively short follow-up period (1 month) may limit the generalizability of the findings and may not fully capture long-term visual adaptation after MIOL implantation. In addition, both eyes from some patients were included in the analysis, which may introduce inter-eye correlation and affect statistical independence. Subjective patient-reported outcomes, such as spectacle independence, dysphotopsia, and contrast sensitivity, were not evaluated, which may limit the comprehensive assessment of visual quality and patient satisfaction associated with this IOL design. In addition, although correlations were analyzed, causal relationships between optical aberrations and visual performance cannot be inferred. Future prospective studies incorporating patient-reported outcomes and longer follow-up are warranted to further elucidate the complex relationship between pupil-dependent optical behavior and functional vision.
In addition, no formal sample size calculation or statistical power analysis was performed due to the retrospective design of the study, which may limit the statistical robustness of the findings.
Conclusion
In conclusion, the segmented refractive MIOL provided satisfactory distance vision and improved intermediate visual performance. Although intraocular HOAs increased in a pupil-dependent manner, these changes did not show a linear association with intermediate visual acuity, suggesting a non-linear optical mechanism contributing to extended depth of focus. These findings highlight the pupil-dependent optical behavior of segmented refractive MIOLs and may assist in optimizing patient selection and preoperative counseling. However, the observed associations should be interpreted with caution, as no causal relationships can be inferred from this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ribeiro F, Cochener B, Kohnen T, et al. Definition and clinical relevance of the concept of functional vision in cataract surgery ESCRS position statement on intermediate vision: ESCRS functional vision working group. J Cataract Refract Surg. 2020;46(Suppl 1):S1–8.
2. Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses in 2020. Ophthalmology. 2021;128(11):e164–e85. doi:10.1016/j.ophtha.2020.09.026
3. Tavassoli S, Ziaei H, Yadegarfar ME, et al. Trifocal versus extended depth of focus (EDOF) intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2024;7(7):Cd014891. doi:10.1002/14651858.CD014891.pub2
4. Cho J-Y, Won YK, Park J, et al. Visual outcomes and optical quality of accommodative, multifocal, extended depth-of-focus, and monofocal intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and bayesian network meta-analysis. JAMA Ophthalmol. 2022;140(11):1045–1053. doi:10.1001/jamaophthalmol.2022.3667
5. Lee YW, Choi CY, Moon K, et al. Clinical outcomes of new multifocal intraocular lenses with hydroxyethyl methacrylate and comparative results of contrast sensitivity, objective scatter, and subjective photic phenomena. BMC Ophthalmol. 2022;22(1):379. doi:10.1186/s12886-022-02600-x
6. Xu Z, Li W, Wu L, Xue S, Chen X, Wu Q. Comparison of the clinical performance of refractive rotationally asymmetric multifocal IOLs with other types of IOLs: a meta-analysis. J Ophthalmol. 2018;2018:4728258. doi:10.1155/2018/4728258
7. Pazo EE, McNeely RN, Richoz O, Nesbit AM, Moore TCB, Moore JE. Pupil influence on the quality of vision in rotationally asymmetric multifocal IOLs with surface-embedded near segment. J Cataract Refract Surg. 2017;43(11):1420–1429. doi:10.1016/j.jcrs.2017.08.013
8. Liao X, Wang M-J, Tan -Q-Q, Lan C-J. Repeatability of i.Profiler for measuring wavefront aberrations in healthy eyes. Int Ophthalmol. 2022;42(8):2525–2531. doi:10.1007/s10792-022-02300-x
9. Hayashi K, Yoshida M, Hayashi H. Correlation of higher-order wavefront aberrations with visual function in pseudophakic eyes. Eye. 2008;22(12):1476–1482. doi:10.1038/sj.eye.6702921
10. Garzón N, Gómez-Pedrero JA, Albarrán-Diego C, Fernández-Núñez S, Villanueva gómez-chacón S, García-Montero M. Optical power profiles and aberrations of a non-diffractive wavefront-shaping extended depth of focus intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2024;262(9):2897–2906. doi:10.1007/s00417-024-06469-y
11. Bang SP, Sabesan R, Yoon G. Effects of neural adaptation to habitual spherical aberration on depth of focus. Res Sq. 2024. doi:10.21203/rs.3.rs-3917931/v1
12. Song IS, Yoon SY, Kim JY, Kim MJ, Tchah H. Influence of near-segment positioning in a rotationally asymmetric multifocal intraocular lens. J Refract Surg. 2016;32(4):238–243. doi:10.3928/1081597X-20160217-06
13. Li H, Liu D, Gao H, Sun J, Bai H, Wu X. Visual performance following bilateral implantation of refractive rotationally asymmetric bifocal intraocular lens (LS-313 MF30) or apodized diffractive bifocal intraocular lens (ReSTOR SN6AD1). Ther Clin Risk Manag. 2021;17:917–926. doi:10.2147/TCRM.S325287
14. Schmid R, Borkenstein AF. Analysis of higher order aberrations in recently developed wavefront-shaped IOLs. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):609–620. doi:10.1007/s00417-021-05362-2
15. Steinmüller LN, Greve D, Rua Amaro D, Bertelmann E, von Sonnleithner C. Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL. Eur J Ophthalmol. 2023;33(6):2096–2105. doi:10.1177/11206721221134171
16. Fernández J, Rodríguez-Vallejo M, Martínez J, Burguera N, Piñero DP. Pupil dependence assessment with multifocal intraocular lenses through visual acuity and contrast sensitivity defocus curves. Eur J Ophthalmol. 2021;31(6):2989–2996. doi:10.1177/1120672120940202
17. Vega F, Alba-Bueno F, Millán MS, Varón C, Gil MA, Buil JA. Halo and through-focus performance of four diffractive multifocal intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(6):3967–3975. doi:10.1167/iovs.15-16600
18. Bosc C, Le Maléfan E, Boury P, Bernier M, Barrucand A. Visual performance correlation with corneal aberrometric profile and pupil size after implantation of a trifocal hydrophobic IOL. Clin Ophthalmol. 2024;18:4053–4061. doi:10.2147/OPTH.S500386
19. Wakabayashi T, Anderson HE, Samuelson AG, et al. Outcomes of laser retinopexy for retinal tears in pseudophakic eyes with multifocal versus monofocal intraocular lenses: a matched cohort study. Curr Eye Res. 2023;48(7):669–673. doi:10.1080/02713683.2023.2197185
20. Son Y, Bang SP, Park CY. Basic optics underlying current intraocular lenses. J Clin Med. 2025;14(23):8608. doi:10.3390/jcm14238608
21. Rua Amaro D, Bertelmann E, von Sonnleithner C, von Sonnleithner C. Clinical outcomes and optical performance of a new segmental refractive extended depth-of-focus intraocular lens. BMC Ophthalmol. 2024;24(1):320. doi:10.1186/s12886-024-03586-4
22. Diao C, Lan Q, Liao J, et al. Influence of decentration of plate-haptic toric intraocular lens on postoperative visual quality. BMC Ophthalmol. 2023;23(1):332. doi:10.1186/s12886-023-03061-6
23. Parimi V, Elsner AE, Burns SA, Gast TJ. Potential vision tester using Maxwellian view, small pupil, and different levels of wavefront correction with adaptive optics. Biomed Opt Express. 2025;16(6):2528–2542. doi:10.1364/BOE.559475
24. Davidova P, Kaiser KP, Hemkeppler E, Böhm M, Kohnen T. Effects of pupil size on functional outcomes of a simultaneous vision intraocular lens. J Refract Surg. 2025;41(7):e645–e54. doi:10.3928/1081597X-20250515-02
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.