Back to Journals » International Medical Case Reports Journal » Volume 19
Functional Hemispherectomy for Rasmussen Encephalitis in a Patient with Systemic Lupus Erythematosus and Type 1 Diabetes Mellitus: A Case Report
Authors Alshurem M ![]()
Received 23 December 2025
Accepted for publication 17 February 2026
Published 23 February 2026 Volume 2026:19 589469
DOI https://doi.org/10.2147/IMCRJ.S589469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Mohammed Alshurem1,2
1Neurology Department, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Neuroscience Research Department, Institute of Research and Medical Consultation, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Mohammed Alshurem, Neurology Department, College of Medicine, Imam Abdulrahman bin Faisal University, King Faisal Ibn Abd Al Aziz road, Dammam, 34212, Saudi Arabia, Tel +966555858533, Email [email protected]
Abstract: Rasmussen encephalitis (RE) is a rare disease caused by an autoimmune disorder. This study describes a rare case of co-occurrence of RE, systemic lupus erythematosus (SLE), and type 1 diabetes mellitus (DM), with emphasis on the autoimmune theory of RE in a patient with a strong family history of autoimmune disease and family consanguinity. A 32-year-old female diagnosed with type 1 DM at the age of 3, epilepsy at the age of 4, and SLE at the age of 13 years. This is the third case describing the co-occurrence of RE with SLE, and the first case describing RE with SLE and type 1 DM.
Keywords: Rasmussen encephalitis, systemic lupus erythematosus, epilepsy
Introduction
Rasmussen encephalitis (RE) was first described in 1958 by Rasmussen et al, who described three cases of focal seizures due to chronic localized encephalitis that did not respond to medical therapy, two of whom underwent hemispherectomy.1 RE is a rare progressive form of chronic encephalitis that typically affects one hemisphere of the brain and occurs primarily in pediatric patients.2 This is a sporadic disease, and its incidence in Germany has been reported to be 2.4 in 10 million people aged <18 years.3
Initially, viral infection was thought to be the cause; however, an autoimmune mechanism was later proposed. Viral infections that trigger an abnormal autoimmune response have also been proposed.4 Several case reports have described the co-occurrence of RE with other autoimmune diseases, including two patients with systemic lupus erythematosus (SLE), one with Hashimoto’s thyroiditis, one with ulcerative colitis, and one with Crohn’s disease, supporting the autoimmune theory (Table 1). Additionally, one case described limbic encephalitis in a patient with type 1 diabetes mellitus (DM) and anti-GAD65 antibodies.5–7
 |
Table 1 Summary of Previously Described RE with Autoimmune Disease |
We aimed to describe the association between RE and other autoimmune diseases, such as SLE and type 1 DM.
Case Presentation
A 32-year-old female presented to our hospital with recurrent seizures at the age of 25. Before her presentation in 2018, she was followed up at a secondary hospital. Her prenatal, natal, and postnatal histories were unremarkable, and she had normal development. She had been diagnosed with type 1 diabetes mellitus (DM) at the age of 3 years. Her sister and two of her brothers were diagnosed with type 1 diabetes, and three of her aunts were diagnosed with systemic lupus erythematosus (SLE). Her parents are third-degree cousins (her great-grandfather is her great-grandmother’s brother).
Her first seizure was nocturnal at the age of 4 years, which was initially thought to be due to hypoglycemia; however, the seizures recurred. She was administered 1500 mg of levetiracetam orally, and her semiology revealed generalized tonic-clonic (GTC) seizures.
Valproic acid (500 mg twice daily) and carbamazepine (400 mg twice daily) were added when the seizures were uncontrolled. Initial computed tomography (CT) of the head revealed a left occipital change possibly due to a remote insult. She had a focal tonic and clonic motor seizure over the right side of the face, arm, and legs, and a GTC seizure.
At the age of 13 years, she was diagnosed with SLE based on 1997 ACR criteria when she had malar rash, discoid rash, polyarthritis, anemia 9.9 (11.5–16.5 g/dl) and positive speckled ANA titer 1:160. She was treated with Imuran 100 mg daily, methotrexate 15 mg weekly, and hydroxychloroquine 200 mg daily.
At the age of 25 years, her rheumatologist discontinued hydroxychloroquine because the SLE was stable, and she developed a cluster of seizures, leading to an emergency room visit and admission. Her electroencephalogram showed continuous slowing 4–6 over the left hemisphere with multifocal epileptiform discharge (Figure 1), and magnetic resonance imaging without contrast showed unilateral left-sided diffuse cerebral atrophy with cortical thinning and abnormally high signal intensities with associated ex vacuo dilation of the left lateral ventricle and unremarkable right cerebral and bilateral cerebellar hemispheres (Figure 2), Lumbar puncture was not done, since the diagnosis of RE did not require CSF analysis. Her mother mentioned that she had progressive right arm weakness every year, and an examination revealed right arm and leg weakness 4/5 with spasticity. Laboratory results, including anti-nuclear antibody (ana) was 160 speckled (positive), rheumatoid factor was 14.4 IU/mL (borderline), ESR was 5 (0–20) mm/hr, CRP was 0.20 (0.05–0.3) anti-double-strand was 9.8 (negative), anti-cyclic citrullinated peptide was 4.6 (negative), HB A1c was 11.6, complete blood count and liver and renal function tests, were unremarkable.
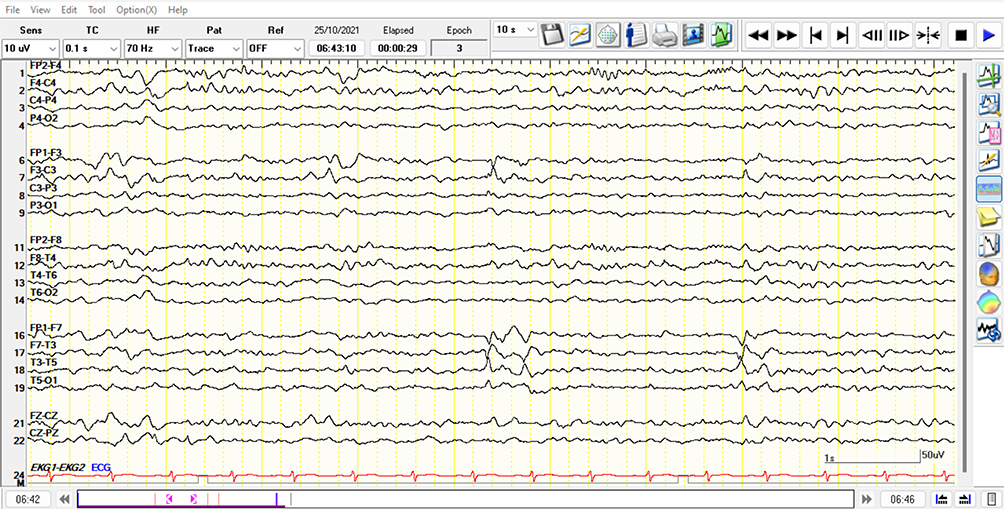 |
Figure 1 EEG epoch during sleep on bipolar montage showing sharp waves over the left frontotemporal region. Abbreviation: EEG, electroencephalogram. |
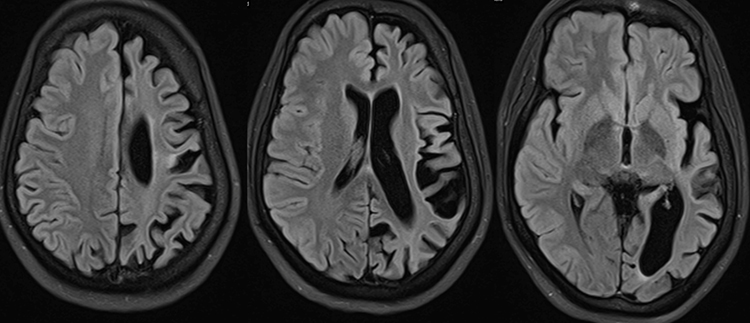 |
Figure 2 Selective FLAIR images demonstrating marked volume loss of the left cerebral hemisphere with widening of the cortical sulci, enlargement of the left lateral ventricle, and ex-vacuo dilatation of the adjacent cerebrospinal fluid space. A patchy and confluent FLAIR hyperintensity involving the left frontoparietal and temporal white matter is also seen, consistent with chronic gliotic changes. Abbreviation: FLAIR, fluid-attenuated inversion recovery. |
She was treated with pulse steroids, which improved her seizures, and hydroxychloroquine was resumed. She had GTC seizures, with injuries to her teeth ranging from one per week to one per month, leading to social isolation, and she avoided going out in public places.
Diagnostic and Therapeutic Intervention
After being diagnosed with RE, the patient agreed to undergo a left functional hemispherectomy in 2019 after an epilepsy monitoring unit evaluation, and five GTC seizures were captured.
Biopsy revealed focal, mild perivascular lymphocytic, and histiocytic infiltrates without significant parenchymal involvement or microglial nodules. Gliosis was noted.
Outcome
After surgery, she was seizure-free, and we tapered her medication after 2 years of seizure freedom. She is currently on two antiepileptics: lacosamide and levetiracetam.
Postoperatively, her right arm spasticity worsened, which was managed with botox administration and physiotherapy. Additionally, she developed a word-finding problem that improved over 2 years.
Discussion
This case report describes the co-occurrence of RE with SLE and type 1 DM, and the worsening of seizures after reducing immunotherapy. In this case, RE preceded SLE by nine years, whereas in the previously described case, RE preceded SLE by six years.6 In another case, RE preceded SLE by 19 years of age.5 All three patients showed improvement after hemispherectomy.
The diagnosis of Lupus encephalitis was considered in this case, but because the MRI was strictly unilateral and the lack of typical MRI findings in Lupus encephalitis, the diagnosis of RE was made. Despite the long duration between the onset of seizure and the diagnosis of RE, which was partially masked due to the immunotherapy of SLE, the patient responded well to functional hemispherectomy and the seizures were well-controlled, which is consistent with previous reports of 70–80% seizure control.8 Our patient underwent surgery in the dominant hemisphere 22 years after disease onset. Compared to the mean duration from diagnosis to surgery in other published cohorts (24 months in 35 patients), our patient had transient mild word-finding difficulties.9,10
Conclusion
This is the third reported case describing SLE occurring after RE and the first to describe the co-occurrence of RE, SLE, and type 1 DM, highlighting the role of autoimmune processes and the risk of consanguinity, which is still an issue in many countries in the Middle East. Also, the co-occurrence of epilepsy and other autoimmune diseases should alert the treating neurologist to the autoimmune possibility of encephalitis.
Data Sharing Statement
The data of the current study are available from the corresponding author on reasonable request, in a de-identified form to protect patient confidentiality.
Ethics Approval
Ethical approval for the study and publication of this case details was obtained from the Imam Abdulrahman Bin Faisal University Institutional Review Board Ethics Committee.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgment
We would like to thank Editage (www.editage.com) for English language editing.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author received no specific funding for this work.
Disclosure
The author declares that he has no competing interests in this work.
References
1. Rasmussen T, Olszewski J, Lloyd-smith D. Focal seizures due to chronic localized encephalitis. Neurology. 1958;8(6):435.
2. Leticia A, Caprara F, Rissardo JP, Nagele EP. Rasmussen encephalitis: clinical features, pathophysiology, and management strategies — a comprehensive literature review. Medicina. 2024;60(11):1858. doi:10.1111/jsr.14327
3. Bien CG, Tiemeier H, Sassen R, et al. Rasmussen encephalitis: incidence and course under randomized therapy with tacrolimus or intravenous immunoglobulins. Epilepsia. 2013;54(3):543–5. doi:10.1111/epi.12042
4. Granata T, Gobbi G, Spreafico R, et al. Rasmussen’s encephalitis: early characteristics allow diagnosis. Neurology. 2003;60(3):422–425. doi:10.1212/WNL.60.3.422
5. Amrom D, Kinay D, Hart Y. Rasmussen encephalitis and comorbid autoimmune diseases: a window into disease mechanism? Neurology. 2014;83(12):1049–1055. doi:10.1212/WNL.0000000000000791
6. Hospital G, Se L. Rasmussen’s encephalitis followed by lupus erythematosus Case report. Dev Med Child Neurol. 2002;44(8):572–574. doi:10.1111/j.1469-8749.2002.tb00331.x
7. Fishan N. Limbic encephalitis, type 1 diabetes mellitus and gad65 antibodies, have we connected the dots ? J Diabetes Metabol. 2024;15(3):1–2. doi:10.35248/2155-6156.10001099
8. Varadkar S, Bien CG, Kruse CA, et al. Rasmussen’s encephalitis: clinical features, pathobiology, and treatment advances. Lancet Neurol. 2014;13(2):195–205. doi:10.1016/S1474-4422(13)70260-6
9. Guan Y, Chen S, Liu C, et al. Timing and type of hemispherectomy for Rasmussen’s encephalitis: analysis of 45 patients. Epilepsy Res. 2017;132:109–115. doi:10.1016/j.eplepsyres.2017.03.003
10. Borne A, Perrone-bertolotti M, Jambaqu I. Cognitive outcome after left functional hemispherectomy on dominant hemisphere in patients with Rasmussen encephalitis: beyond the myth of aphasia. Patient Series. 2022;4(22):1–8. doi:10.3171/CASE22410
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.