Back to Journals » Journal of Healthcare Leadership » Volume 18
From Women’s Rights Denial to Increased Integration: The Evolution of Women in Medicine in Lebanon
Authors Al Rachid M ![]() , El Hadi C, Kazan D, Chakhtoura G
, El Hadi C, Kazan D, Chakhtoura G
Received 11 September 2025
Accepted for publication 19 January 2026
Published 17 February 2026 Volume 2026:18 566847
DOI https://doi.org/10.2147/JHL.S566847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Maria Al Rachid,1 Christopher El Hadi,2 Daniel Kazan,1 Ghassan Chakhtoura1
1Digestive and Endocrine Surgery Department, Saint Joseph University, Faculty of Medicine, Beirut, Lebanon; 2Internal Medicine Department, Lebanese American University, Beirut, Lebanon
Correspondence: Maria Al Rachid, Email [email protected]
Background: Over the past decades, women have entered the medical profession in Lebanon in increasing numbers. However, their advancement into leadership roles and high-impact specialties remains limited.
Objective: This study explores the historical evolution, current status, and systemic challenges faced by women in medicine in Lebanon.
Methods: A descriptive, narrative-based analysis was conducted using data from institutional reports, professional associations, and existing literature. Trends in enrollment and registration were examined, and findings were contextualized through comparison with selected European experiences reported in the literature.
Results: Women now represent nearly half of medical students and registered physicians in Lebanon; however, they remain underrepresented in surgical specialties and decision-making roles. Key challenges identified include limited institutional policies, persistent gender bias, and insufficient structures supporting work–life integration.
Conclusion: While numerical gains are encouraging, structural inequities persist across career pathways. Contextual insights from European countries highlight potential strategies for institutional reform, including mentorship programs, flexible training pathways, and national gender equity policies.
Keywords: inclusivity, gender inequity, challenges, leadership in healthcare, medical workforce, health profession education
Introduction
Throughout history, women have faced significant challenges in pursuing their medical education and realizing their aspirations. From trailblazers like Saniya Habboub, the first woman to practice medicine in Lebanon, and Elizabeth Blackwell, the first woman enrolled in a medical school in the United States, to present-day female leaders in the health professions, the battle against sexism and misogyny has been long and ongoing.1,2 As we navigate the landscape of 2025, where women now make up nearly half of the health workforce, the barriers have shifted from outright denial of access to medical education to combating stereotypes and navigating micro-aggressions.3
In the Middle East, these challenges are particularly pronounced due to entrenched religious and patriarchal norms that limit women’s representation in leadership roles, often relegating them to traditional family roles.4 Despite these obstacles, there has been a noticeable trend towards feminization of the workforce in the Arab World, albeit within stringent societal constraints.5 Similar patterns have been documented in other Middle Eastern countries, where women increasingly constitute the majority of medical students, yet remain underrepresented in senior positions, underscoring a regional disconnection between numerical growth and structural equity.5
In Lebanon, a country ranked 132 out of 146 in the 2023 Gender Gap Index report, with a concerning score of 90 in educational attainment, a significant gender disparity persists, particularly evident in surgical specialties. Despite this, there is a notable lack of studies documenting the progression of women in the field of medicine within the Lebanese context. While international evidence suggests that workforce feminization does not automatically translate into gender equity in leadership or specialty distribution, country-specific analysis remains essential to understanding how local sociopolitical contexts shape these disparities. This gap in research highlights the need for a comprehensive examination of the challenges and advancements experienced by women pursuing careers in medicine in Lebanon, shedding light on the evolving landscape of gender equality within the medical profession.6
This study aims to provide a descriptive overview of the evolution of women’s participation in medicine in Lebanon across different time periods. It explores the historical entry points of women into the profession, tracks their growing presence in various medical specialties and leadership positions, and highlights the persistent challenges they face today. By combining available national data, institutional records, and qualitative insights, this article seeks to offer a nuanced picture of gender dynamics in Lebanese medicine and to inform future strategies for achieving greater equity.
Methods
Study Design and Data Collection
This study is a retrospective time-series analysis of physician registration data in Lebanon. Data were retrieved in December 2023 from the publicly available registry of the Lebanese Order of Physicians (LOP). The dataset included aggregated counts of male and female physicians registered with the LOP across successive time periods.
The authors extracted and compiled sex-disaggregated registration data and calculated the number and proportion of female and male physicians registered over time. Registration with the LOP is mandatory for medical practice in Lebanon; therefore, the registry serves as a comprehensive national source for assessing physician workforce trends.
All data used in this study were publicly accessible, eliminating the requirement for ethical approval. No individual-level or identifiable information was collected. Physicians’ names and identification numbers were not accessed, and all analysis were conducted on anonymized, aggregated data only.
Statistical Analysis
Statistical analysis were conducted using R version 4.3.1 (Vienna, Austria). A Chi-squared test for trend was utilized to evaluate the annual change in the proportion of female physicians enrolled by the Ministry. To determine if the pattern of female physician enrollments in the early 1990s followed a Poisson distribution,a marker of rarity,a goodness-of-fit test was applied. If a trend was identified, a fixed simple linear regression was used to illustrate the annual increase in the proportion of female physicians enrolled.
Results
From 1946 to 2022, there was a significant positive trend in the proportion of women enrolled by the Lebanese Order of Physicians (P < 0.001). An increase of percentage can be clearly seen in Table 1.
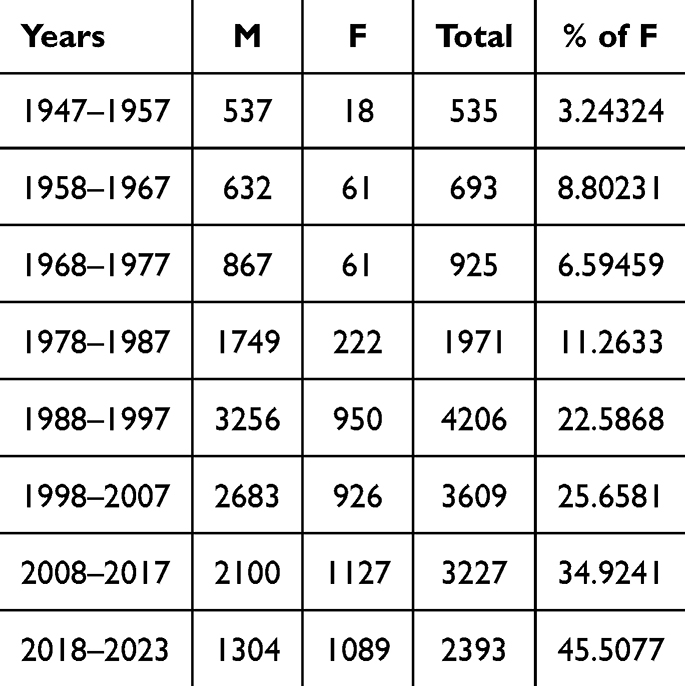 |
Table 1 Gender Distribution of Physicians Registered with the Lebanese Order of Physicians by Decade (1947–2023) |
Each year saw an increase of 0.5375% in the proportion of female enrolled (95% CI: 0.4874–0.5877, P < 0.001), with an intercept of −1049 (95% CI: −1149 to −950, P < 0.001). The probability of a woman being enrolled was considered a significantly rare event until 1974 (P = 0.07 until 1974, P = 0.046 until 1975), as it can be seen in Figure 1.
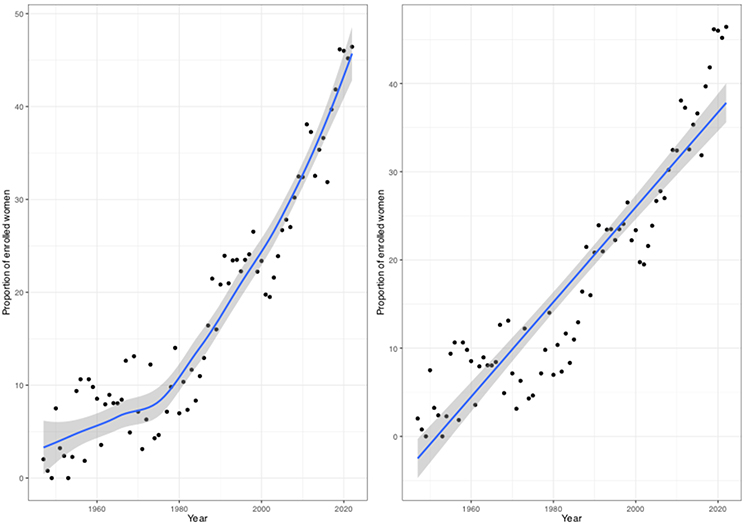 |
Figure 1 Trend/Regression of enrolled women proportion as a function of time: (left) polynomial regression and (right) linear regression. |
Discussion
As expected, the number of females enrolled in the order of physician increased however the cinetics of this increase witnessed several stepping stones, from denying them the right of medical education to being an integral part of the workforce. The statistical results can help us confirm the presence of a historical overview that can be divided into three eras. The division into three historical eras—Early Pioneers (pre-1975), Institutional Growth and Resistance (1975–2000), and Contemporary Presence and Persistent Gaps (2000–present) is based on the statistical trends observed in our dataset, while commentary on mentorship, leadership, and policy reforms draws from existing literature and comparative frameworks rather than study-derived evidence.
Early Pioneers (Pre-1975)
The entry of women into the medical profession in Lebanon began slowly during the early 20th century. Medicine, traditionally seen as a male-dominated field, posed significant cultural and institutional barriers to women. However, despite these constraints, a handful of pioneering women enrolled in medical schools in Beirut and abroad, often coming from urban, educated families that supported female higher education.7,8
These early female physicians were typically limited to what was considered “acceptable” specialties such as pediatrics, obstetrics and gynecology, or general practice, where their caregiving roles aligned with societal gender norms. Their visibility was low, and they rarely occupied academic or leadership positions. However, they laid the foundation for future generations and began challenging the notion that medicine was an exclusively male domain.1
Institutional Growth and Resistance (1975–2000)
The period of the Lebanese Civil War (1975–1990) created disruption in all sectors, including medical education and healthcare. Nonetheless, this era witnessed a gradual increase in female enrollment in medical schools, partly due to the broader rise in women’s access to higher education in Lebanon.9
By the 1990s, women represented a growing minority in medical training programs. Yet structural resistance remained palpable. Career progression was still skewed in favor of men, particularly in surgical specialties, hospital administration, and academic medicine.10 Female physicians often faced implicit bias, lack of mentorship, and challenges in balancing career demands with family responsibilities.
Despite these challenges, the post-war reconstruction period also gave rise to early examples of women entering subspecialties and hospital leadership roles, although in limited numbers. Professional networks for women in healthcare remained largely informal or nonexistent during this time.11
Contemporary Presence and Persistent Gaps (2000–Present)
The early 2000s marked a turning point in the visibility of women in medicine in Lebanon. Several medical schools began reporting gender parity,or even female majority,among incoming medical students, a reflection of global trends and improved access to education for women in Lebanon.9
Today, women are present across most medical specialties, including fields traditionally dominated by men such as surgery, emergency medicine, and interventional radiology. Female physicians have taken on leadership roles as deans, department heads, and members of national medical societies.11 However, despite these advances, gender disparities persist, particularly in:
- Representation in academic promotions and professorships
- Access to competitive fellowships and international exposure
- Leadership in hospital governance and health policy decision-making12
Surveys and anecdotal accounts suggest that work-life balance expectations, gendered mentorship gaps, and invisible barriers still affect women’s full participation and advancement.10 Institutional efforts to promote gender equity are emerging but remain fragmented and often underfunded.
Despite the persistence of microaggressions and lingering sexism in the workplace, the rise of women empowerment movements and genuine mentorship opportunities have significantly transformed the professional landscape. These initiatives have emboldened women to assert themselves with greater confidence, breaking through barriers and securing leadership positions that were once out of reach. As a result, women are increasingly taking on higher roles, reshaping the health workforce and challenging the status quo.
Lessons from Europe
While Lebanon has made considerable strides in increasing the number of women entering the medical profession,particularly over the past two decades,comparative insights from European countries reveal both parallels and persistent structural gaps. In many Western European nations, gender parity in medical school admissions was achieved in the 1990s, with some countries like Sweden and France reporting a consistent female majority among medical students for over two decades.13 Lebanon has only recently approached similar enrollment figures,9 signaling important progress, yet occurring within a context of limited institutional gender equity frameworks.
What distinguishes the European experience is not only the presence of women in medicine, but the policy infrastructure that supports their advancement. Across much of Europe, national-level interventions such as gender wage gap, mentorship programs, protected parental leave, tenure-clock extensions, and flexible residency training pathways have been implemented to mitigate gender-based career interruptions.14–16 These policies have played a significant role in improving female representation in surgical subspecialties, academic medicine, and hospital leadership—areas where Lebanese women remain underrepresented despite rising numbers in general practice and non-surgical fields.17 (Table 2)
 |
Table 2 Comparison of Gender Equity in Medicine: Lebanon vs Selected European Countries |
In Lebanon, most progress remains driven by individual effort rather than systemic reform. Professional networks such as Women in Surgery Lebanon (WiSL) have begun filling this gap, but broader national strategies are lacking. Compared to European systems, Lebanese women physicians face greater challenges related to work-life balance, mentorship access, and promotion pathways, which collectively contribute to a slower pace of change at senior levels.
This contrast underscores the importance of moving beyond gender parity in education to the more complex goal of equity in career development, leadership, and policy inclusion. Lessons from European models may offer valuable frameworks for designing context-specific solutions in Lebanon.
Recommendations
Addressing gender disparities in medicine in Lebanon requires coordinated efforts across institutions and policymaking bodies. Based on national gaps and international models, the following actions are recommended:
Medical schools and hospitals should implement clear, transparent policies on recruitment, promotion, and leadership pathways, supported by gender equity offices.12
Standardized parental leave and adaptable residency structures must be integrated to reduce the motherhood penalty and support work-life integration.14
Structured mentorship programs,particularly in underrepresented specialties,can promote retention and leadership among female physicians.13
Robust data collection on workforce trends, specialty distribution, and academic advancement is essential to monitor equity progress.9
Bias Awareness and Inclusion Training
Curricular reforms should include gender sensitivity and leadership development to foster inclusive institutional cultures from medical school onward.15
Limitations and Further recommendations
The study is limited to the data shared by the Lebanese Order of Physicians, many more people could have earned the degree without enrolling or practicing. A further study of the factors influencing this major transformation is needed.
Conclusion
In conclusion, the journey of women in medicine, particularly in Lebanon, reflects a remarkable evolution from exclusion to increased participation. Starting with pioneers like Saniya Habboub, who defied societal norms to pursue a career in medicine, to the present day where women are increasingly represented in the medical field, the trajectory has been shaped by perseverance, resilience, and a growing support system. The increasing presence of women in medicine not only enriches the profession but also contributes to a more diverse and inclusive healthcare system.
Yet, this increase in numbers has not been matched by structural equity in specialty choice, leadership, or career progression. Persistent cultural norms, policy gaps, and institutional inertia continue to limit women’s full participation and advancement in the field. While the present study focuses on physician registration trends rather than workforce participation or leadership outcomes, the data and analysis can help initiate work toward the development and implementation of evidence-informed policy documents.
By learning from successful European models and committing to national reforms,ranging from mentorship initiatives to maternity leave policies,Lebanon can take meaningful steps toward gender equity in medicine. The future of the profession depends not only on who enters it, but also on who is supported to lead, teach, and thrive within it.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Haffar D. Woman Pioneer: alumna Saniya Habboub. LAU archives. 2023.
2. Reed V, Buddeberg-Fischer B. Career obstacles for women in medicine: an overview.
3. Parmer LL. The road to gender equality: persisting obstacles for American women in the workforce. Psychol Manag J. 2021;24(2):85–7. doi:10.1037/mgr0000115
4. Salem R, Haibe Y, Dagher C, et al. Female oncologists in the Middle East and North Africa: progress towards gender equality. ESMO Open. 2019;4(3):e000487. doi:10.1136/esmoopen-2019-000487
5. Mohamed NA, Abdulhadi NN, Al-Maniri AA, Al-Lawati NR, Al-Qasmi AM. The trend of feminization of doctors’ workforce in Oman: is it a phenomenon that could rouse the health system? Hum Resour Health. 2018;16(1). doi:10.1186/s12960-018-0283-y
6. El Hage S, Wakim E, Sayde G, Akiki D, Salameh P. Assessment of gender gap in surgical specialties among Lebanese medical personnel: the need for involvement of women in surgery. East Mediterr Health J. 2022;28(10):743–750. doi:10.26719/emhj.22.077
7. Zuhur S. Women and empowerment in the Arab World [Internet]. Vol. 25. Arab Studies Quarterly. 2003. Available from: https://www.jstor.org/stable/41858460.
8. Joseph S. Patriarchy and development in the Arab world. Gend Dev. 1996;4(2):14–19. doi:10.1080/741922010
9. UNESCO. Women in science: fact sheet. 2022.
10. AlQirem L, Al-Huneidy L, Hammouri M, et al. Perceived barriers towards the importance and application of medical research: a source of gender disparity among medical undergraduates. BMC Med Educ. 2022;22(1):767.
11. Alansari AN, Alhussaini NW, Elshaikh U, Al-Zoubi RM. The journey of female surgeons in the Arab region: a scoping review. Surgeon. 2024;22:307–318. doi:10.1016/j.surge.2024.07.009
12. Miller VM, Rice M, Schiebinger L, et al. Embedding concepts of sex and gender health differences into medical curricula. J Women’s Health. 2013;22(3):194–202. doi:10.1089/jwh.2012.4193
13. OECD. Gender equality in the workplace. OECD Publishing. 2023.
14. Boniol M, Mcisaac M, Xu L, Wuliji T, Diallo K, Campbell J. Gender Equity in the Health Workforce: Analysis of 104 Countries. World Health Organization; 2019.
15. Riska E. Gender and medical careers. Maturitas. 2011;68(3):264–267. doi:10.1016/j.maturitas.2010.09.010
16. Shannon G, Jansen M, Williams K, et al. Gender equality in science, medicine, and global health: where are we at and why does it matter? Lancet. 2019;393(10171):560–569. doi:10.1016/S0140-6736(18)33135-0
17. Al Sabah S, AlHamdan F, Qadhi I, Shuaibi S, Younes S, Al Haddad E. Female physicians leading health care in the Arab World. Med Princ Pract. 2019;28(4):315–323. doi:10.1159/000499592
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.