Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
From Tradition to Future: Pathophysiological Mechanisms and Clinical Research Progress in the Treatment of Hypothyroidism with Traditional Chinese Medicine——A Narrative Review
Authors Piao L, Ma J, Zhao N, Liu C, Hou Y ![]() , Wang T
, Wang T
Received 12 November 2025
Accepted for publication 9 March 2026
Published 21 March 2026 Volume 2026:22 581042
DOI https://doi.org/10.2147/TCRM.S581042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Lei Piao,1 Jian Ma,2 Na Zhao,2 Chunyan Liu,2 Yongqing Hou,1 Tehasi Wang1
1Department of Graduate School, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China; 2Department of Endocrinology, First Affiliated Hospital, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China
Correspondence: Jian Ma, Department of Endocrinology, First Affiliated Hospital, Heilongjiang University of Chinese Medicine, 26 Heping Road, Harbin, Heilongjiang, 150040, People’s Republic of China, Email [email protected]
Abstract: Hypothyroidism, a prevalent endocrine disorder primarily resulting from inadequate thyroid hormone secretion, is commonly attributed to etiologies, such as Hashimoto’s thyroiditis and iodine deficiency. Currently, levothyroxine (LT4) replacement therapy is the standard treatment in Western medicine. However, suboptimal therapeutic responses in certain patients have motivated the investigation of alternative interventions. In recent years, TCM, particularly the integrative approach of combining acupuncture with herbal medicine, has demonstrated promising potential in the management of hypothyroidism. Through a systematic review of 12 randomized controlled trials (RCTs) onTCM for hypothyroidism conducted in the past decade, this article found that TCM exerts therapeutic effects by regulating immune function, improving thyroid antibody levels, and modulating metabolic status. Commonly used herbs include Astragalus membranaceus (Huangqi), Codonopsis pilosula (Dangshen), and Rehmannia glutinosa (Shudihuang), whose mechanisms of action involve key signaling pathways such as MAPK and PI3K-AKT.Acupuncture and moxibustion therapies target specific acupoints (e.g. Guanyuan and Zusanli) to improve thyroid function by regulating apoptosis and the associated signaling cascades. Multiple randomized controlled trials have demonstrated that the combination of acupuncture and herbal medicine not only significantly ameliorates clinical symptoms, but also modulates serum concentrations of TSH, T3, and T4, thereby enhancing treatment efficacy. Nonetheless, current research is limited by factors such as small sample sizes, insufficient long-term follow-up, and a lack of comprehensive mechanistic studies. Future investigations employing large-scale, multi-center, high-quality clinical trials are warranted to further substantiate the efficacy and safety of these integrative therapeutic modalities.
Keywords: hypothyroidism, TSH, TCM, acupuncture and moxibustion
Introduction
Hypothyroidism is an endocrine disorder caused by insufficient synthesis or secretion of thyroid hormones to meet the physiological demands of peripheral tissues.1 Thyroid hormones are critical for the normal development of various human tissues, and play a pivotal role in regulating the metabolism of nearly all cells and organs throughout their lifespan. Primary hypothyroidism is defined as thyroid gland failure attributable to intrinsic thyroid pathology, accounting for over 99% of hypothyroid cases.1 The diagnosis of overt primary hypothyroidism is established by an elevated serum thyroid-stimulating hormone (TSH) level concurrent with a serum thyroxine (T4) level below the population reference range. TSH, secreted by the adenohypophysis, is regulated by thyrotropin-releasing hormone (TRH) from the hypothalamus, and is subject to negative feedback inhibition by circulating thyroid hormones, constituting the hypothalamic-pituitary-thyroid axis.
Primary hypothyroidism arises from pathological alterations within the thyroid gland with no associated hypothalamic or pituitary abnormalities. The predominant etiologies include chronic lymphocytic thyroiditis (Hashimoto thyroiditis), radiation-induced thyroiditis, chronic thyroiditis, thyroidectomy, and high-dose radiation therapy in the head and neck region. Notably, severe endemic iodine deficiency remains the leading cause of hypothyroidism globally.1 Less common causes include non-autoimmune infiltrative disorders such as amyloidosis. Additionally, various pharmacological agents can impair thyroid function and precipitate primary hypothyroidism.1 In contrast, central hypothyroidism results from hypothalamic or pituitary dysfunction, which impairs TSH secretion.2 Common etiologies include neoplasms, surgical interventions, radiation exposure, hemorrhage, infections, infiltrative diseases, traumatic brain injury, and certain medications.3 Subclinical hypothyroidism is characterized by the absence of overt clinical symptoms, normal circulating thyroid hormone levels, and elevated TSH levels detected via laboratory assays, often resulting from diverse thyroid impairments.4
L-thyroxine (LT4), a synthetic analog of T4, is the primary therapeutic agent for hypothyroidism and ranks as the third most prescribed medication in the United States, with over 100 million prescriptions annually.5 Data indicate that approximately 30% of patients exhibit normal thyroid function parameters at the initiation of treatment.6 Despite the normalization of TSH and free T4 (FT4) levels, up to 15% of patients receiving LT4 therapy continue to experience persistent symptoms. As a synthetic replacement preparation of thyroxine T4, LT4 merely serves to supplement the insufficient secretion of thyroid hormones in the body and cannot address the multiple pathological links of hypothyroidism. In clinical practice, some patients fail to achieve target hormone levels even with a standardized dose of LT4, primarily due to individual heterogeneity in absorption and metabolism. This indicates that the single hormone replacement therapy with LT4 cannot fully cover the pathophysiological landscape of hypothyroidism, and it is imperative to explore more comprehensive new treatment models.
TCM has a long history in the treatment of hypothyroidism and has accumulated rich experience in syndrome differentiation and treatment through long-term clinical practice. Among them, the acupuncture combined with Chinese materia medica therapy, relying on its dual effects of meridian regulation and medication intervention, is regarded as a potential ideal strategy to break through the current therapeutic bottleneck.At present, there still exist critical knowledge gaps in TCM research on hypothyroidism treatment: the synergistic mechanism of acupuncture combined with Chinese materia medica remains unclear, and research on multi-target regulation is insufficient; clinical protocols lack unified standards with high heterogeneity; differentiated protocols for different types of hypothyroidism and special populations have not been established; and the dose adjustment, curative effect and safety of its combination with LT4 lack systematic summary. Adopting the method of narrative review, this study comprehensively collates relevant literature published in the past decade, integrates basic experimental and clinical evidence, systematically evaluates the application status and synergistic mechanism of acupuncture combined with Chinese materia medica in the treatment of hypothyroidism, analyzes the research defects and sources of heterogeneity, and proposes the standardization path of clinical protocols and future research directions. It is expected to provide theoretical support for the standardized clinical application of acupuncture combined with Chinese materia medica and promote the improvement of the integrated traditional Chinese and Western medicine treatment system.
Literature Search Strategy and Methods
Search Strategy
A systematic search was conducted in the China National Knowledge Infrastructure (CNKI), Wanfang Database, VIP Database, PubMed, Cochrane Library, and Web of Science for randomized controlled trials (RCTs) on Traditional Chinese Medicine for hypothyroidism. The search timeframe covered Chinese and English literature published in the past decade, from 2014 to 2024. Search terms included “hypothyroidism,” “traditional Chinese medicine,” “decoction,” “acupuncture,” “moxibustion,” “electroacupuncture,” “clinical study,” “clinical observation,” and “randomized,” using a combination of MeSH terms and free-text words. Relevant meta-analyses and review articles were also traced to supplement the literature.
Inclusion Criteria
① Study types: randomized controlled trials (RCTs), case-control studies, basic experimental studies, and relevant network pharmacology analyses. ② Study subjects: patients with a confirmed diagnosis of primary hypothyroidism, subclinical hypothyroidism, or Hashimoto’s thyroiditis with hypothyroidism. ③ Interventions: The control group could receive no treatment (blank control), traditional Chinese medicine, acupuncture, Western medicine, placebo, or another effective treatment. The treatment group must receive comprehensive TCM interventions, including any combination of two or more of the following: decoctions, acupuncture, moxibustion, Chinese patent medicines, pills, or Western medicine. No restrictions were placed on treatment duration. ④ Primary outcome measures: thyroid function (TSH, FT4, FT3, T3, T4), thyroid autoantibodies (TPOAb, TGAb), TCM syndrome scores, and overall clinical response rate.
Exclusion Criteria
① Studies with confounded interventions where effects could not be isolated. ② Empirical summaries and purely theoretical discussions (lacking experimental data support). ③ Studies with incomplete data. ④ Duplicate publications; conference papers or subsequently published versions were excluded.
Literature Screening and Data Extraction
Two researchers independently conducted the literature search, screening, and data extraction. In case of disagreement, a third researcher was consulted for consensus. Data extraction included title, authors, publication year, number of trial arms, actual number of enrolled cases, interventions, outcome measures, and treatment duration.
Quality Assessment
The Cochrane Risk of Bias Tool was used to assess the risk of bias in the included studies. The assessment covered seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other sources of bias. Each domain was judged as “low risk,” “high risk,” or “unclear.” However, as this article is a literature review, it is difficult to fully adhere to the quality assessment standards of a systematic review.
Epidemiology
Data from the National Health and Nutrition Examination Survey in the United States indicate a prevalence of hypothyroidism, encompassing both primary and subclinical forms, of approximately 4.6%.7 A separate screening study conducted in the U.S. reported prevalence rates of 0.4% for primary hypothyroidism and 9% for subclinical hypothyroidism.8 A meta-analysis of European populations revealed prevalence estimates of 0.37% for primary hypothyroidism and 3.8% for subclinical hypothyroidism, incorporating both diagnosed and undiagnosed cases, with an estimated annual incidence rate of 226 cases per 100,000 individuals.9 Domestic epidemiological data show that the incidence rate of overt hypothyroidism in China is approximately 2.9 per 1,000 individuals. The overall incidence increases with age, and the prevalence is significantly higher in females than in males. Among patients with autoimmune thyroiditis, 2% to 4% progress to hypothyroidism annually.10 Hypothyroidism is influenced by a combination of genetic, intrinsic, and environmental factors. A genome-wide association study (GWAS) meta-analysis, which included over 70,000 participants from 22 cohorts, identified 42 genetic loci associated with circulating TSH levels within the normal reference range.11 Among these loci, seven are specifically linked to hypothyroidism, including the thyroid peroxidase (TPO) gene, which encodes a key enzyme involved in thyroid hormone biosynthesis.11 Individuals possessing a TSH-based genetic risk score in the highest quartile exhibited a 2.5-fold increased risk of developing hypothyroidism compared with those in the lowest quartile.11
Regarding environmental influences, TPO antibody concentrations were found to be lower in smokers than in non-smokers.12 Furthermore, current smokers demonstrated lower TSH levels than former smokers, who in turn had lower TSH levels than those who had never smoked.13 Obesity has been associated with elevated serum TSH concentrations in both pediatric and adult populations, with evidence suggesting a potentially bidirectional relationship.14 Additionally, children born small for gestational age present with higher serum TSH levels than those born appropriate for gestational age, resulting in a higher frequency of subclinical hypothyroidism diagnoses in this group.15 The prevalence of primary hypothyroidism is notably higher among individuals with either excessive iodine intake or severe iodine deficiency than among those with adequate iodine consumption.16 Prevalence rates decline as the severity of iodine deficiency decreases, but increase when iodine intake transitions from mild deficiency to optimal or excessive levels. Moreover, improvements in iodine status have been associated with increased positivity for thyroid antibodies,17 which may consequently reduce the risk of Hashimoto’s thyroiditis.A summary of the epidemiological factors contributing to hypothyroidism is presented in Figure 1.
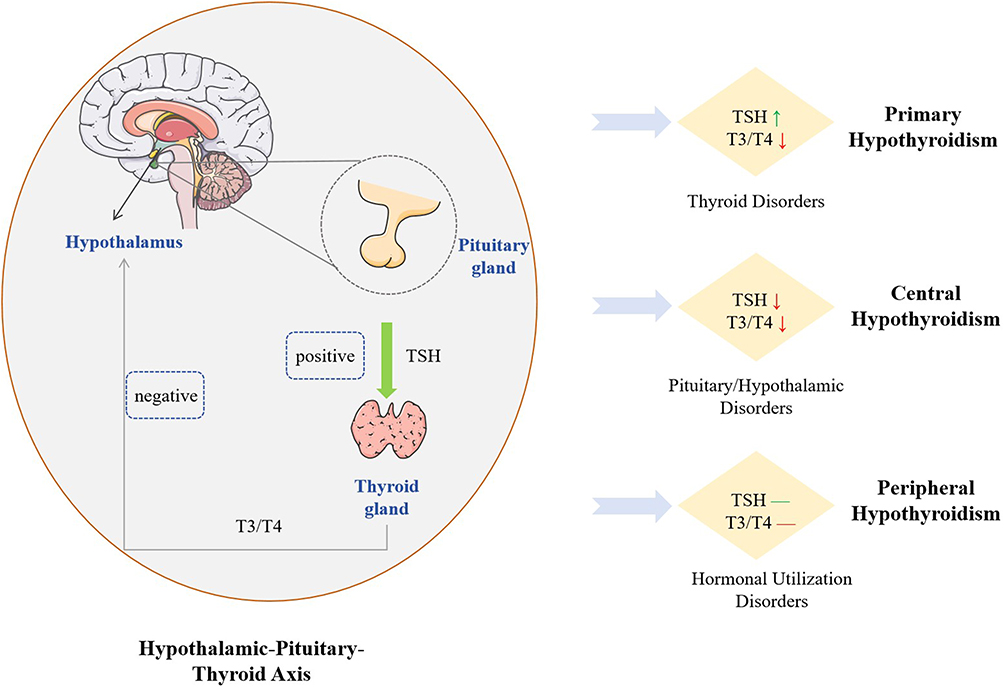 |
Figure 1 Epidemiological characteristics of hypothyroidism. The green-colored upward arrows represent an increase, while the red-colored downward arrows represent a decrease. The red and green lines represent hormonal utilization disorders. |
Signs and Symptoms of Hypothyroidism
Hypothyroidism exerts clinical effects on nearly all organ systems, resulting in varying degrees of thyroid hormone deficiency, irrespective of the etiology.18 The majority of hypothyroid manifestations stem from a generalized reduction in metabolic activity, manifesting as symptoms such as fatigue, cold intolerance, bradycardia, and weight gain, or from the accumulation of matrix glycosaminoglycans within interstitial tissues, which contribute to features such as coarse hair and hoarseness. The clinical presentations of hypothyroidism range from mild or asymptomatic cases to severe forms, including life-threatening myxedema coma. Typically, the progression of hypothyroidism is insidious, with nonspecific and widespread signs and symptoms that often emerge late, complicating its differential diagnosis from other conditions. Fatigue and exhaustion are among the most prevalent symptoms along with dry skin, weight gain, and constipation. Impaired gastrointestinal and gallbladder motility19 have been identified as key mechanisms underlying constipation, gallbladder hypofunction, and biliary stone formation in patients with hypothyroidism. Additionally, mild hepatocellular dysfunction may occur, and hypothyroidism is recognized as a risk factor for non-alcoholic fatty liver disease and sporadic steatohepatitis.20
In adults, hypothyroidism may precipitate intercalated neuropathy and metabolic polyneuropathy, cognitive deficits including memory impairment and poor concentration, musculoskeletal complaints, sleep apnea, depression, and other psychiatric disorders.21 Severe and persistent hypothyroidism is associated with increased vascular resistance, reduced cardiac output, and diminished left ventricular function.22 Cardiovascular complications also include myocardial injury, pericardial effusion, and features of metabolic syndromes, such as hypertension, central obesity, and dyslipidemia.23
However, most signs and symptoms linked to hypothyroidism are nonspecific and insufficient for diagnosis based solely on the clinical presentation. Moreover, several symptoms commonly attributed to hypothyroidism have a high prevalence in the general adult population.24 For instance, a study conducted at a health fair reported that 12% of individuals with overt hypothyroidism, 7.4% with mild hypothyroidism, and 7.7% with hyperthyroidism exhibited symptoms typically associated with hypothyroidism.8 Furthermore, the extent to which these symptoms are attributable to aging remains unclear, especially given that serum TSH levels tend to increase with age.25 Notably, an escalation in symptom severity may predict hypothyroidism. One study reported a likelihood ratio of 8 for hypothyroidism when patients experienced seven or more symptom changes within a year.26 Nonetheless, reliance on symptoms alone for diagnosis leads to an unacceptably high rate of false-positive diagnoses among healthy individuals.27 A summary of the clinical signs and symptoms associated with hypothyroidism is shown in Figure 2.
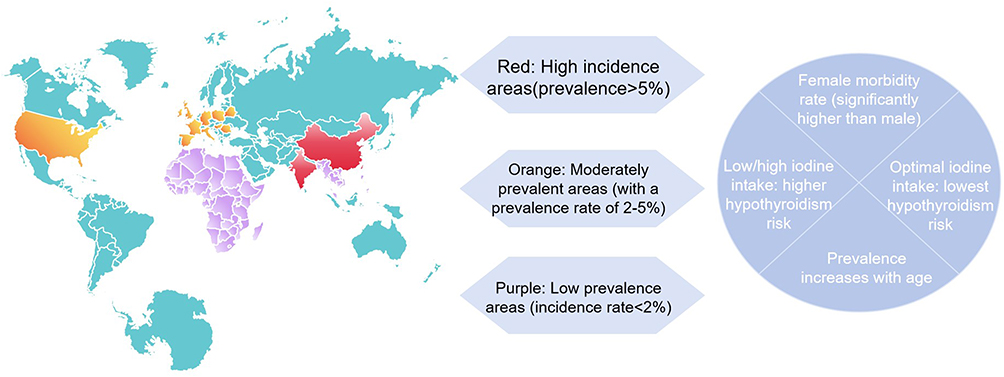 |
Figure 2 Symptoms and effects of hypothyroidism. |
Diagnosis of Hypothyroidism
The clinical manifestations of hypothyroidism are predominantly non-specific and may overlap with the symptoms observed in various non-thyroidal conditions. According to empirical evidence, the most frequently reported symptoms of overt hypothyroidism include xerosis, cold intolerance, coarse skin texture, periorbital edema, diminished sweating, weight gain, paresthesia, cold skin, and constipation.28 A study conducted in 2014 identified fatigue, dry skin, dyspnea, emotional lability, and constipation as the predominant clinical features.24 Notably, the severity of thyroid hormone deficiency does not consistently correlate with symptomatology: some patients with biochemically significant hypothyroidism may exhibit minimal or no symptoms, whereas others with mild biochemical abnormalities may present with numerous symptoms. Furthermore, individuals with hypothyroidism have a higher prevalence of psychiatric diagnoses and are more frequently prescribed psychotropic medications including antidepressants, anxiolytics, and antipsychotics.21
The SerumTSH level remains the most reliable diagnostic tool for primary hypothyroidism. A log-linear inverse relationship exists between serum TSH and FT4 concentrations, whereby minor reductions in free T4 elicit substantial elevation in TSH levels. Elevated TSH levels are highly indicative of primary hypothyroidism, whereas normal TSH values generally suggest euthyroid status. It is important to recognize that serum TSH exhibits diurnal variation, peaking in the late afternoon.1 Additionally, advancing age is associated with a physiological increase in serum TSH levels among individuals who are otherwise euthyroid.20
Diagnosing central hypothyroidism is more complex. In symptomatic individuals, low free T4 levels accompanied by low or inappropriately normal TSH concentrations suggest central TSH deficiency.2 Differentiating between central hypothyroidism and non-thyroidal illness syndromes can be particularly challenging. In such scenarios, the measurement of total serum T3 and reverse T3 (rT3) may aid in diagnosis. Both conditions typically exhibit low or low-normal TSH levels; however, central hypothyroidism is characterized by disproportionately reduced T4 levels relative to T3 levels and low rT3 concentrations. Conversely, non-thyroidal illness syndrome demonstrates a relatively lower T3 level compared to T4 and elevated rT3 levels. Upon diagnosis of central hypothyroidism in the absence of a known hypothalamic-pituitary pathology, comprehensive hypothalamic-pituitary imaging and evaluation of other pituitary hormones are warranted.29 Flowchart for the Diagnostic Approach to Hypothyroidism (Figure 3).
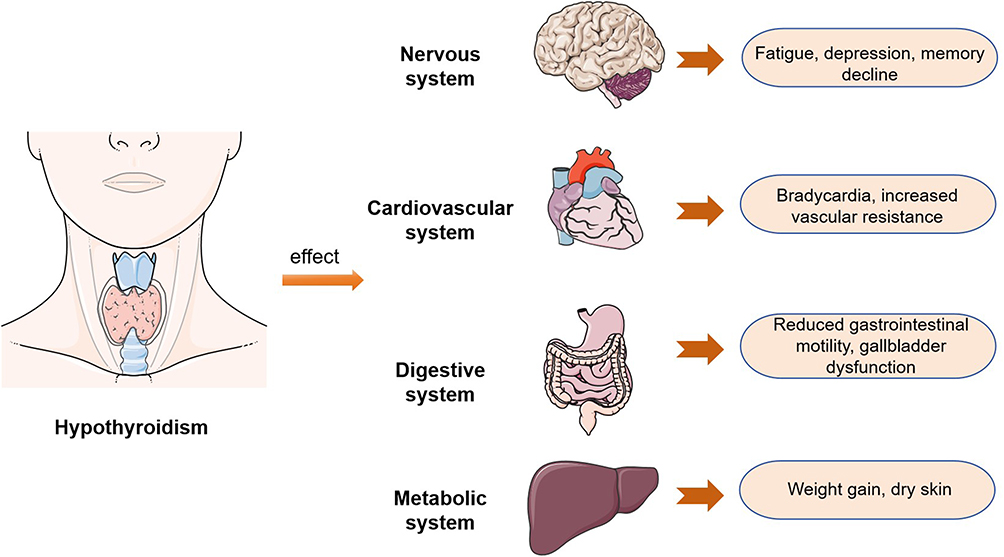 |
Figure 3 Flowchart for the Diagnostic Approach to Hypothyroidism. |
Pathophysiological Mechanisms
The pathophysiological mechanisms of primary hypothyroidism are complex, involving multiple aspects including autoimmunity, nutritional imbalance, iatrogenic injury, and abnormal central regulation.30 Among these, chronic autoimmune thyroiditis (Hashimoto’s thyroiditis) is the most common etiology. It is driven by a combination of genetic, environmental, and immune disorders, characterized by T cell-mediated destruction of thyroid follicles, and is often accompanied by positive anti-thyroid antibodies.31,32 Positive TPOAb during pregnancy not only impairs the compensatory function of the thyroid gland but is also associated with adverse pregnancy outcomes and neurodevelopmental disorders in offspring.33 Iodine metabolic disturbance can also lead to hypothyroidism: severe iodine deficiency directly impairs hormone synthesis, whereas excessive iodine inhibits the release and synthesis of thyroid hormones via the Wolff-Chaikoff effect, triggering hypothyroidism in high-risk populations.34,35 In addition, iatrogenic factors such as radioactive iodine therapy, thyroidectomy, and external irradiation to the head and neck are common causes of permanent hypothyroidism.36–38 Central hypothyroidism results from insufficient TSH secretion due to pituitary or hypothalamic lesions, presenting as decreased fT4 with normal or low TSH;39 peripheral hypothyroidism is rare and mostly caused by impaired hormone transport or metabolism.40 The diversity of the above mechanisms determines the complexity of the clinical classification of hypothyroidism and provides a theoretical basis for the formulation of individualized therapeutic strategies. A comprehensive overview of the classification and pathophysiological mechanisms underlying hypothyroidism is shown in Figure 4.
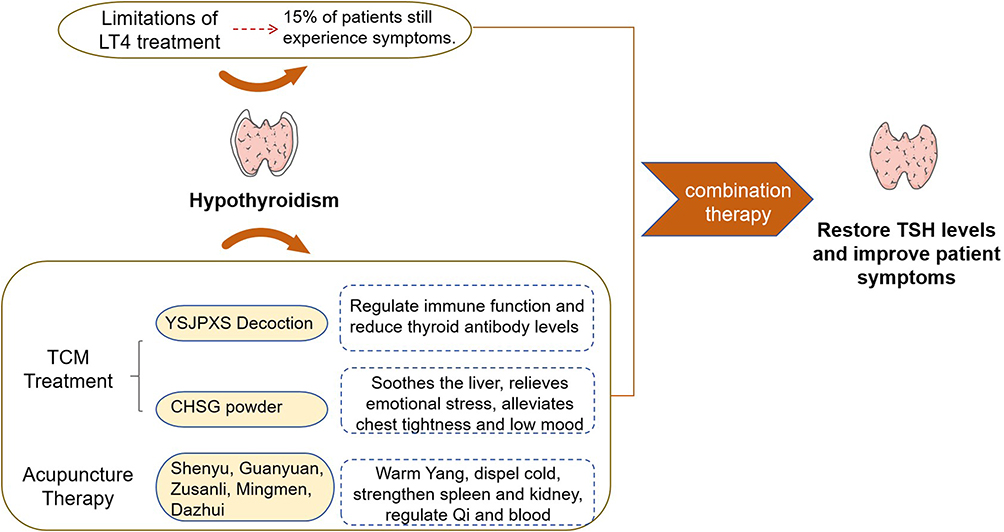 |
Figure 4 Classification and pathological mechanism of hypothyroidism. |
Cognition of Hypothyroidism in TCM
As early as the Warring States Period of China, the condition of ying (goiter) was recorded in Zhuangzi·Dechongfu,41 which explicitly described symptoms of cervical swelling and laid a foundation for the understanding of thyroid-related diseases in later generations. In the Tang Dynasty, Essential Prescriptions for Emergency Use categorized this condition as laoying (consumptive goiter),42 and for the first time associated “fatigue and emotional states” with cervical swelling—an association highly consistent with the clinical characteristics of persistent fatigue and emotional disorders in patients with hypothyroidism.Subsequent physicians gradually enriched the understanding of this disease through clinical practice: General Treatise on the Etiology and Symptoms of Diseases clearly stated that
One should not dwell for long in places with black soil and mountain springs flowing through; constant consumption of local food causes ying disease, and emotional agitation exacerbates the condition.43
It elaborated on the impacts of water and soil environment (external causes) and emotional fluctuations (internal causes) on the onset of ying disease, a perception largely consistent with the modern medical view that hypothyroidism is influenced by environmental, genetic and emotional factors, reflecting the profound understanding of thyroid diseases by ancient Chinese physicians. Ancient medical texts including Golden Mirror of Medicine, General Collection of Holy Relief and Orthodox Manual of External Medicine further refined the classification, etiology and pathogenesis of ying disease, and identified “qi stagnation, phlegm congelation and blood stasis” as the core pathological factors, providing a theoretical origin for modern TCM treatment of hypothyroidism.Building on ancient medical works and combining the modern clinical characteristics of hypothyroidism, contemporary TCM physicians have further refined the TCM understanding of the disease. They have clarified that “spleen-kidney yang deficiency, liver qi stagnation, qi and blood insufficiency, and intermingled phlegm and stasis” are the core pathogenesis of hypothyroidism, and developed a treatment approach centered on syndrome differentiation and treatment—one that is highly consistent with the TCM herbal and acupuncture treatment regimens focused on in this paper.
TCM’s Etiology and Pathogenesis of Hypothyroidism
Within the TCM domain, multiple perspectives exist regarding the etiology and pathogenesis of hypothyroidism. According to Yi Zong Jin Jian, gallbladder disorders can be categorized into internal and external causes. External causes are attributed to the invasion of the Rong and Wei Qi by six pathogenic factors, leading to qi stagnation and blood stasis. Internal causes predominantly involve seven emotions, particularly anxiety and anger.44 In TCM theory, the “seven emotions” (joy, anger, worry, pensiveness, grief, fear and shock) are normal emotional responses of the human body. However, prolonged emotional dysregulation (eg., chronic anxiety, anger and melancholy) can lead to dysfunction of the liver in governing free flow of qi. The core function of the liver in governing free flow of qi, as defined in TCM, is to regulate emotions, promote the circulation of qi and blood, and mediate body fluid metabolism. Chronic anxiety can induce “liver qi stagnation”, which impedes the circulation of qi and blood and gives rise to internal production of phlegm-dampness. This constitutes the core theoretical basis for the consensus among contemporary TCM physicians that “liver failure in governing free flow of qi is one of the essential pathogenesis of hypothyroidism”. Sheng Ji Zong Lu classified gallbladder diseases into stone galls resulting from acclimatization, fatigue galls, and qi galls caused by internal emotional injury.45 The Treatise Surgical Orthodoxy posits that gallbladder disease arises from qi, phlegm, and blood stasis within the five Zang organs, with a particular emphasis on blood stasis, phlegm coagulation, and qi stagnation localized in the anterior neck region.46 Contemporary scholars offer further insights: Wang Xingkuan identified the liver as the primary locus of the disease, closely interconnected with the spleen, kidney, and heart, with liver depression and qi stagnation, visceral dysfunction, and phlegm-dampness combined with blood stasis constituting the central pathogenesis.47 Guo Junjie considered congenital deficiency as a predisposing factor, liver dysfunction in dispersal as the core pathological mechanism, involvement of the spleen and kidney in chronic pathological alterations, and phlegm coagulation alongside blood stasis as the resultant pathological products.48 Chen Ruquan emphasizes Yang deficiency of the spleen and kidney as pivotal to disease onset, with Qi and blood deficiency driving disease progression and blood stasis representing the principal concurrent syndrome.49
Treatment of Hypothyroidism with TCM
Yingjie et al investigated the clinical efficacy of the Yishen Jianpi Xiaoying Decoction, comprising Radix Astragali, Rhizoma Curculiginis, Radix Rehmanniae Preparata, Herba Cistanches, Bulbus Fritillariae Thunbergii, Flos Lonicerae, Spica Prunellae, Rhizoma Atractylodis Macrocephalae, Fructus Forsythiae, Radix Angelicae Sinensis, Rhizoma Chuanxiong, Herba Scutellariae Barbatae, Carapax Trionycis, Radix Ophiopogonis, and Radix Glycyrrhizae Preparata.50 In their study, 84 patients diagnosed with Hashimoto’s thyroiditis complicated by hypothyroidism were randomly assigned to either a control or observation group, each consisting of 42 participants. The control group received levothyroxine sodium tablets, whereas the observation group was administered Yishen Jianpi Xiaoying Decoction in addition to levothyroxine treatment. After 12 weeks of treatment, the total effective rate was 95.24% in the observation group and 78.57% in the control group. Compared with baseline, the observation group showed a significant reduction in TSH (P<0.05) and significant elevations in FT3 and FT4 (P<0.05), with greater improvements than the control group. Meanwhile, the observation group exhibited significantly lower levels of anti-thyroid peroxidase antibody (TPOAb) and anti-thyroglobulin antibody (TGAb) compared with the control group (P<0.05), as well as obviously reduced thyroid volume and isthmus thickness (P<0.05). These results indicate triple improvements in thyroid function, autoimmune status, and thyroid morphology.
Yingna et al examined the clinical efficacy of Chaihu Shugan Powder, which includes Radix Paeoniae Alba, Concha Ostreae, Rhizoma Atractylodis Macrocephalae, Radix Bupleuri, Poria, Pericarpium Citri Reticulatae, Spica Prunellae, Rhizoma Cyperi, Rhizoma Chuanxiong, Rhizoma Pinelliae Preparata, Radix Angelicae Sinensis, and Radix Glycyrrhizae Preparata, in treating Hashimoto’s thyroiditis (HT) complicated by hypothyroidism, characterized by liver depression and spleen deficiency syndrome.51 A total of 84 patients with Hashimoto’s thyroiditis complicated with hypothyroidism and liver-stagnation and spleen-deficiency syndrome were randomly divided into a control group (42 cases, treated with conventional Western medicine) and an observation group (42 cases, treated with conventional therapy plus modified Chaihu Shugan San). After 12 weeks of treatment, the total clinical effective rate was 90.48% in the observation group and 71.43% in the control group.TCM syndrome scores in the observation group decreased by 72.5% compared with baseline (41.2% in the control group, P<0.05), with substantial relief of symptoms including depression, chest tightness and abdominal distension.Regarding thyroid function, the observation group showed a significant reduction in TSH (P<0.05) and significant elevations in FT3 and FT4 (P<0.05), with greater improvements than the control group.For autoimmune antibodies and inflammatory factors, the observation group exhibited reductions of 40.1% and 36.8% in TPOAb and TGAb levels, respectively, compared with the control group (P<0.05). Levels of interleukin-6 (IL-6), interleukin-23 (IL-23) and interferon-γ (IFN-γ) were also significantly lower in the observation group (P<0.05), indicating dual regulation of immune disturbance and inflammatory response.In addition, thyroid volume and isthmus thickness were significantly reduced in the observation group compared with the control group (P<0.05).
Chen et al explored the therapeutic effects of a modified Shengjiang Decoction combined with Banxia Houpu Decoction, containing Radix Codonopsis, Radix Astragali, Rhizoma Atractylodis Macrocephalae, Pericarpium Citri Reticulatae, Cortex Magnoliae Officinalis, Endothelium Corneum Gigeriae Galli, Rhizoma Anemarrhenae, Radix Paeoniae Alba, Ramulus Cinnamomi, Rhizoma Chuanxiong, Rhizoma Pinelliae, Poria, and Folium Perillae, in patients with subclinical hypothyroidism secondary to Hashimoto’s thyroiditis exhibiting liver depression and spleen deficiency.52 Sixty-four patients were randomly allocated to treatment and control groups (n = 32 each). The control group received levothyroxine sodium tablets, whereas the treatment group received combined decoctions for four weeks. Comparative analyses of clinical efficacy, symptom scores, and TSH, TGAb, and TPOAb levels were conducted before and after treatment. The study concluded that the combination of Shengjiang and Banxia Houpu Decoctions effectively ameliorated clinical symptoms and reduced TSH, TPOAb, and TGAb levels, thereby improving thyroid function in this patient population.
Zhou et al assessed the impact of a modified Yougui Pill decoction composed of Radix Rehmanniae Preparata, Radix Codonopsis, Radix Astragali, Fructus Corni, Radix Glycyrrhizae Preparata, Rhizoma Cimicifugae, Semen Cuscutae, Fructus Lycii, Radix Bupleuri, Fructus Jujubae, Rhizoma Atractylodis Macrocephalae, Radix Angelicae Sinensis, Pericarpium Citri Reticulatae, Rhizoma Dioscoreae, Cortex Eucommiae, Rhizoma Zingiberis Recens, and Cortex Cinnamomi, in conjunction with Euthyrox, for the treatment of hypothyroidism.53 A total of 85 patients with hypothyroidism were randomly divided into a control group (42 cases, treated with LT4 alone) and an observation group (43 cases, treated with LT4 combined with modified Yougui Wan). After 12 weeks of treatment, the total clinical effective rate was 93.02% in the observation group and 76.19% in the control group.In the observation group, TSH level was reduced by 62.3% compared with baseline, while FT3 and FT4 levels were increased by 41.5% and 38.7%, respectively, all of which were significantly superior to those in the control group (P<0.05). Meanwhile, the observation group showed significant reductions in TGAb and TPOAb levels by 35.2% and 38.9% (P<0.05) compared with the control group.Total cholesterol (TC), triglyceride (TG), and low-density lipoprotein cholesterol (LDL-C) were decreased by 21.4%, 25.6%, and 23.8% (P<0.05), respectively, and high-density lipoprotein cholesterol (HDL-C) was increased by 18.3% (P<0.05) in the observation group.In addition to improving thyroid function and regulating autoimmunity, the combined treatment effectively corrected lipid metabolism disorders in patients with hypothyroidism.A summary of the mechanisms underlying the therapeutic effects of TCM on hypothyroidism is provided in Table 1.
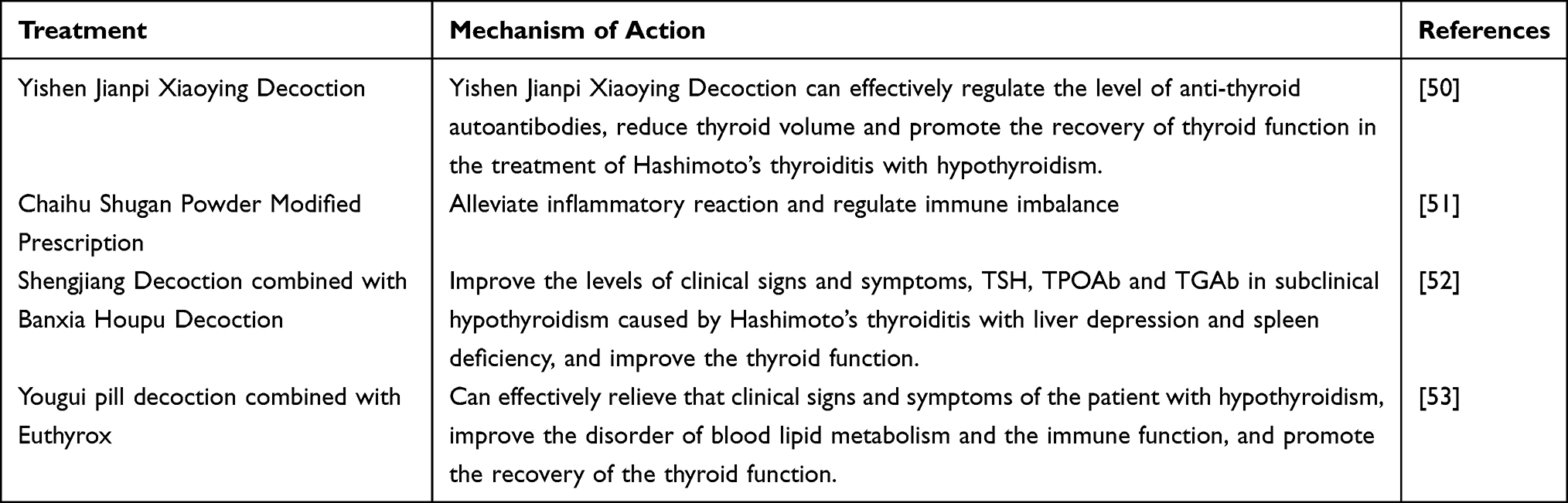 |
Table 1 Mechanism of Traditional Chinese Medicine in the Treatment of Hypothyroidism |
Acupuncture Treatment of Hypothyroidism
Acupuncture treatment for hypothyroidism primarily functions through the modulation of the hypothalamic-pituitary-thyroid (HPT) axis. This regulatory effect of acupuncture and moxibustion on the HPT axis is potentially mediated by the neuroendocrine-immune system. Specifically, acupuncture stimulates designated acupoints on the body surface, eliciting somatosensory inputs that are then transduced into bioelectrical signals. These electrical stimuli activate the brainstem reticular formation and subsequently influence the hypothalamus. Additionally, acupuncture affects the immune system by promoting the release of neurotransmitters, neuropeptides, and hormones from the central nervous system, which, in turn, affects immune organs and functions. The neuroendocrine and immune systems are intricately interconnected and mutually regulatory, with the nervous system playing a predominant role, while the endocrine and immune systems exert modulatory influences.54
Zhang et al investigated the clinical efficacy of warming needle moxibustion targeting the Shenshu, Mingmen, and Pishu acupoints in patients diagnosed with subclinical hypothyroidism characterized by spleen-kidney Yang deficiency.55 In this protocol, after needle insertion at the specified points, a 2 cm segment of moxa stick was affixed to the needle handle at Shenshu and Pishu and ignited following the arrival of qi; the needles were retained for 20 min until the moxa burned out. Fifty-six patients were randomized into a treatment group (n=30) that received warm acupuncture and a control group (n=26) that received lifestyle guidance without pharmacological or acupuncture intervention. Both the groups underwent an 8-week treatment period. Pre- and post-treatment assessments included serum FT3, FT4, TSH, and TPOAb levels as well as TCM symptom scores and clinical signs. The results indicated that warm needling and moxibustion significantly reduced TSH and TPOAb levels and improved clinical symptoms and quality of life in patients with subclinical hypothyroidism of the spleen-kidney yang deficiency type.
Wang et al evaluated the effects of fire acupuncture on lipid profiles in a rat model of hypothyroidism.56 Forty healthy six-week-old Wistar rats were allocated into a blank control group (n=10) and a hypothyroidism model group (n=30). The latter group was established via total thyroidectomy followed by subcutaneous L-thyroxine administration. The model group was further subdivided into untreated, Western medicine (Euthyrox), and fire needle treatment groups (n=10 each). The treatments were administered for 30 consecutive days. Subsequent serum analyses measured the TG, TC, HDL-C, and LDL-C levels. These findings demonstrated that fire needle therapy exerted a significant regulatory effect on blood lipid levels in hypothyroid rats, surpassing the efficacy observed in the Western medicine group.
Min et al examined the therapeutic effects of the “Fifty Ying” acupuncture technique combined with nuclear cheese injection acupoint therapy in patients with hypothyroidism.47 The acupuncture protocol involved needling multiple acupoints along the Ren, Lung, Large Intestine, Stomach, Spleen, Heart, Pericardium, Kidney, and Liver meridians by employing reinforcing and reducing techniques aligned with the meridian qi circulation sequence. Needle retention lasted 30 min, corresponding to 50 cycles of meridian qi circulation over 24 h (each cycle was approximately 28.48 minutes). Thirty-seven patients with hypothyroidism, classified into spleen-kidney yang deficiency (n=22) and yin-yang deficiency (n=15) subtypes per TCM, received this combined treatment. Serum FT3, FT4, and sensitive TSH (sTSH) levels were measured pre- and post-intervention, and treatment efficacy was compared between subtypes. Color Doppler flow imaging (CDFI) was used to assess the superior thyroid artery blood flow distribution and velocity changes. The combined therapy significantly improved thyroid function, potentially by restoring the systemic balance between deficiency and excess, and harmonizing yin and yang.
Zhou et al conducted a clinical study on warming acupuncture targeting the Zhongwan, Xiawan, Qihai, Guanyuan, and bilateral Zusanli acupoints.57 Patients were prepared by voiding urine and positioned supine; the skin at acupoints was disinfected, and disposable stainless steel filiform needles (0.258 mm × 40 mm) were inserted to depths of 15–20 mm using reinforcing and reducing techniques. Preprepared moxa sticks were affixed to needle handles and ignited to provide localized warmth. The needles were removed after moxa combustion and cooling. Subjects were randomized into warm acupuncture and western medicine groups. Serum levels of T3, T4, FT3, FT4, and TSH were measured before and after treatment, and therapeutic outcomes were evaluated according to the established criteria. The results indicated that warming needle moxibustion demonstrated superior clinical efficacy compared to Western medicine in adult hypothyroidism, with advantages including convenience, time efficiency, mild stimulation, and cost-effectiveness.
Wang et al designed a randomized controlled trial to assess the clinical efficacy of the “Yiqi Zhouliu” acupuncture method in treating hypothyroidism secondary to Hashimoto’s thyroiditis with liver-qi stagnation.58 Sixty patients were randomized into an acupuncture plus medication group and a medication only group (n=30 each). Both groups received levothyroxine sodium daily for eight weeks. The acupuncture medication group additionally underwent acupuncture at Baihui, Neiguan, Hegu, Taichong, Zusanli, Yinlingquan, Taixi, and the locally selected acupoints Tiantu, Futu, and Renying, with acupoint selection tailored to symptomatology. The sessions lasted 20 minutes, twice weekly, over two four-week courses. The primary outcomes included symptom scores and serum TSH, TPOAb, and TgAb levels. The combined treatment yielded superior therapeutic effects, notably in alleviating emotional distress and chest discomfort and reducing TSH and TgAb levels, compared to levothyroxine alone.In summary, the mechanisms underlying the therapeutic effects of acupuncture in hypothyroidism involve modulation of the neuroendocrine-immune network, with clinical studies demonstrating improvements in thyroid function, symptomatology, and associated biochemical markers. A detailed overview of these mechanisms is presented in Table 2.
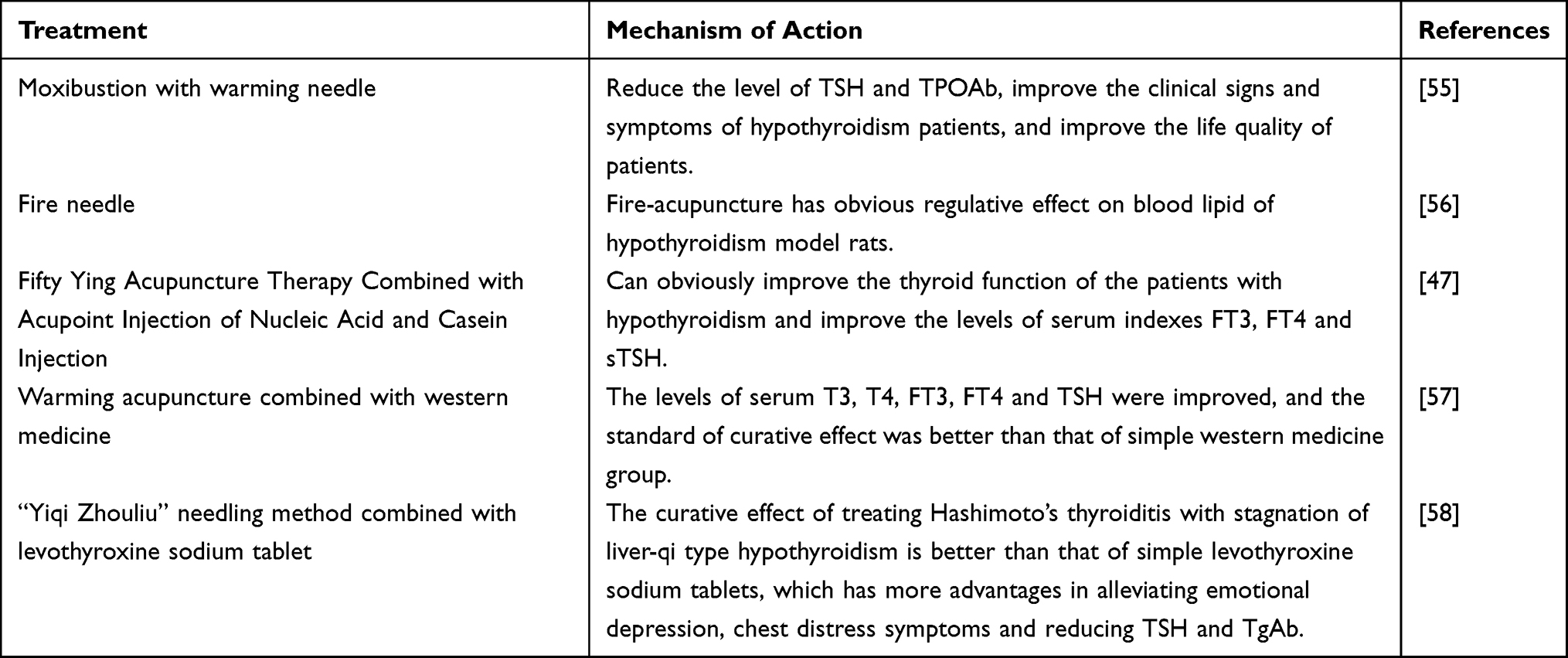 |
Table 2 Mechanism of Action of Acupuncture and Moxibustion on Hypothyroidism |
Comprehensive Treatment of Hypothyroidism with TCM
Gao et al investigated the therapeutic effects of TCM comprising Astragalus membranaceus, Cuscuta chinensis, Atractylodes macrocephala, Loranthus mulberry mistletoe, Eucommia ulmoides, Codonopsis pilosula, Dioscorea opposita, and Glycyrrhiza uralensis, in combination with acupuncture and moxibustion targeting acupoints Tiantu, Guanyuan, Zusanli, and Sanyinjiao, on hypothyroidism.59 The patients were positioned supine, and the skin and needles at the specified acupoints were routinely disinfected. Disposable Huaying brand filiform needles were inserted sequentially using a perpendicular needling technique, followed by flat reinforcing and reducing manipulation. After the arrival of qi, needles were retained for 20 min, and treatment was administered once daily. Concurrently, moxibustion was applied by holding a lit moxa stick 2 to 3 cm above the acupoint, moving it slowly to evenly warm the skin until slight erythema and sustained warmth were perceived; each session lasted 20 min and was conducted every two days. Eighty-six pregnant women diagnosed with hypothyroidism were randomly assigned to either the study or control group, each comprising 43 participants. Both groups received conventional treatment. The control group additionally underwent acupuncture and moxibustion, whereas the study group received TCM alongside these interventions. Clinical efficacy and adverse pregnancy outcomes were evaluated, and thyroid function parameters, including TSH, FT4, TPOAb positivity rate, and pregnancy-related hormones, such as progesterone (P) and estradiol (E2), were measured pre- and post-treatment. The findings indicated that the combination of TCM with acupuncture and moxibustion effectively ameliorated hypothyroidism during pregnancy by modulating thyroid hormone secretion and enhancing progesterone levels.
Chunping et al60 examined the efficacy and safety of Shugan Sanjie Xiaoying Decoction, composed of Radix Bupleuri, Rhizoma Cyperi, Radix Curcumae, Bulbus Fritillariae Thunbergii, Rhizoma Curcumae, Ramulus Euonymi, Radix Paeoniae Alba, Poria, Rhizoma Atractylodis Macrocephalae, Spica Prunellae, Herba Centellae, Concha Ostreae, and Rhizoma Dioscoreae Nipponicae, in conjunction with acupoint catgut embedding at Xinshu and Ganshu acupoints for the treatment of hypothyroidism accompanied by goiter in patients with HT characterized by liver depression and spleen deficiency. The procedure involved routine disinfection and insertion of 1 cm of No.1 catgut into a medical catgut embedding needle, which was then inserted at a 45° angle until the patient experienced soreness, swelling, or numbness, and was subsequently embedded fully into the acupoint before needle withdrawal, followed by application of a postoperative patch. A total of 140 patients with HT-related hypothyroidism were randomly allocated into four groups of 35 patients each. All groups received levothyroxine sodium; the treatment group additionally received Shugan Sanjie Xiaoying Decoction combined with acupoint catgut embedding; control group 1 received only the decoction; control group 2 received only acupoint catgut embedding; and control group 3 was treated with Xiweier. After 12 weeks, comprehensive therapeutic outcomes were assessed, including thyroid hormone levels, antibody titers, T-lymphocyte subset profiles, thyroid volume, and levothyroxine dosage. The results demonstrated that the combined therapy of Shugan Sanjie Xiaoying Decoction and acupoint catgut embedding was superior to either TCM alone, Western medicine alone, or acupoint catgut embedding alone in improving thyroid function, reducing antibody titers, modulating immune function, and decreasing goiter size in patients with liver depression and spleen deficiency-type hypothyroidism.
Liu et al61 evaluated the effects of acupuncture targeting auricular triple energizer, spleen, kidney, governor vessel, Dazhui, Zhiyang, and Mingmen acupoints, combined with Bupi Wenshen Paste, which contains Radix Codonopsis, Rhizoma Atractylodis Macrocephalae, Poria, Rhizoma Dioscoreae, Radix Rehmanniae, Radix Aconiti Lateralis Preparata, Ramulus Cinnamomi, Rhizoma Zingiberis, Radix Astragali Preparata, Radix Aucklandiae, Fructus Amomi, Semen Coicis, Radix Angelicae Sinensis, Pericarpium Citri Reticulatae, Radix Glycyrrhizae Preparata, Radix Puerariae, and Radix Salviae Miltiorrhizae, in patients with subclinical hypothyroidism. Acupuncture involves precise localization and disinfection of acupoints, gentle needle insertion using forceps, fixation with small square adhesive tape, and intermittent pressing for 1–2 minutes every 4 hours. Auricular acupoints were treated unilaterally, alternating sides, with sessions conducted once every 7 days. Sixty patients exhibiting serum TSH levels between 4.5 and 10.0 mU/L were randomly divided into two groups: the control group (n=30) received Bupi Wenshen Paste alone, while the treatment group (n=30) received acupuncture in addition to the paste. The treatment courses lasted 7 days, with 2-day intervals between courses, totaling five courses. Post-treatment assessments included clinical efficacy, thyroid function parameters (TSH, FT3, FT4), and blood lipid profiles (TG, TC, HDL-C, LDL-C). The study concluded that acupuncture combined with Bupi Wenshen Paste significantly enhances thyroid function and regulates lipid metabolism in patients with subclinical hypothyroidism, demonstrating clear clinical benefits. The mechanisms underlying the therapeutic effects of TCM in hypothyroidism are summarized in Table 3 and illustrated in Figure 5.
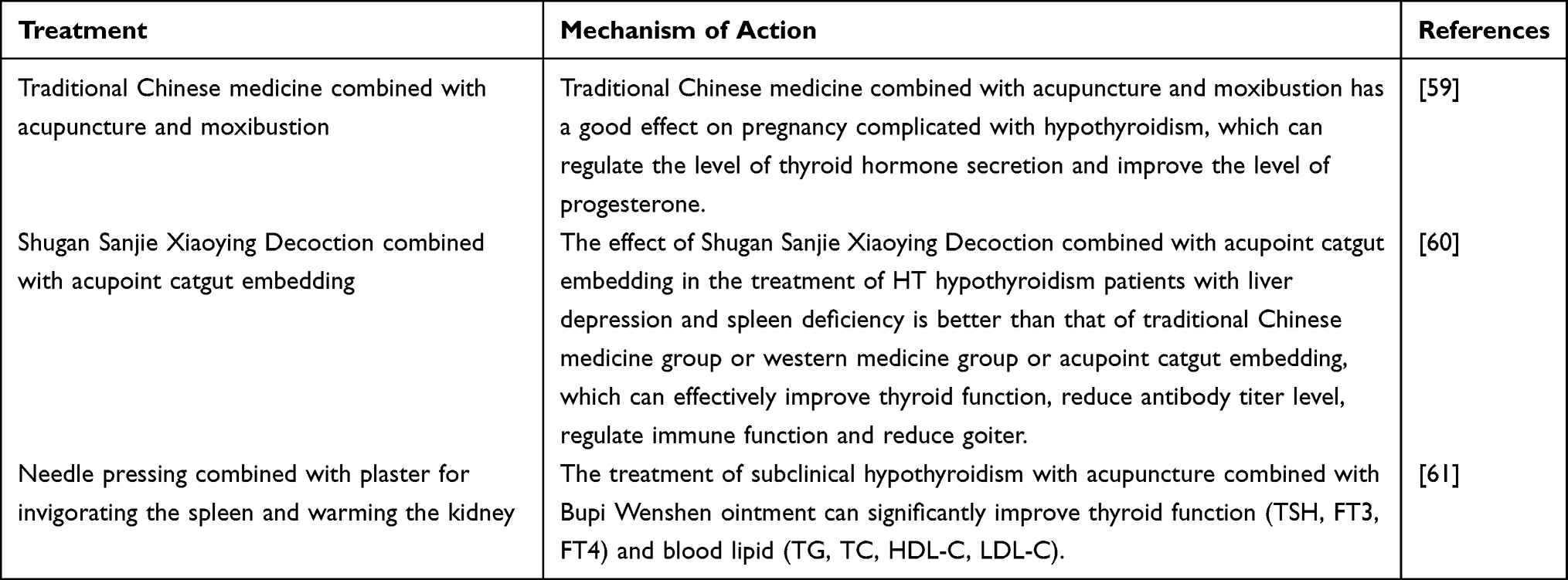 |
Table 3 Mechanism of Action of TCM in the Treatment of Hypothyroidism |
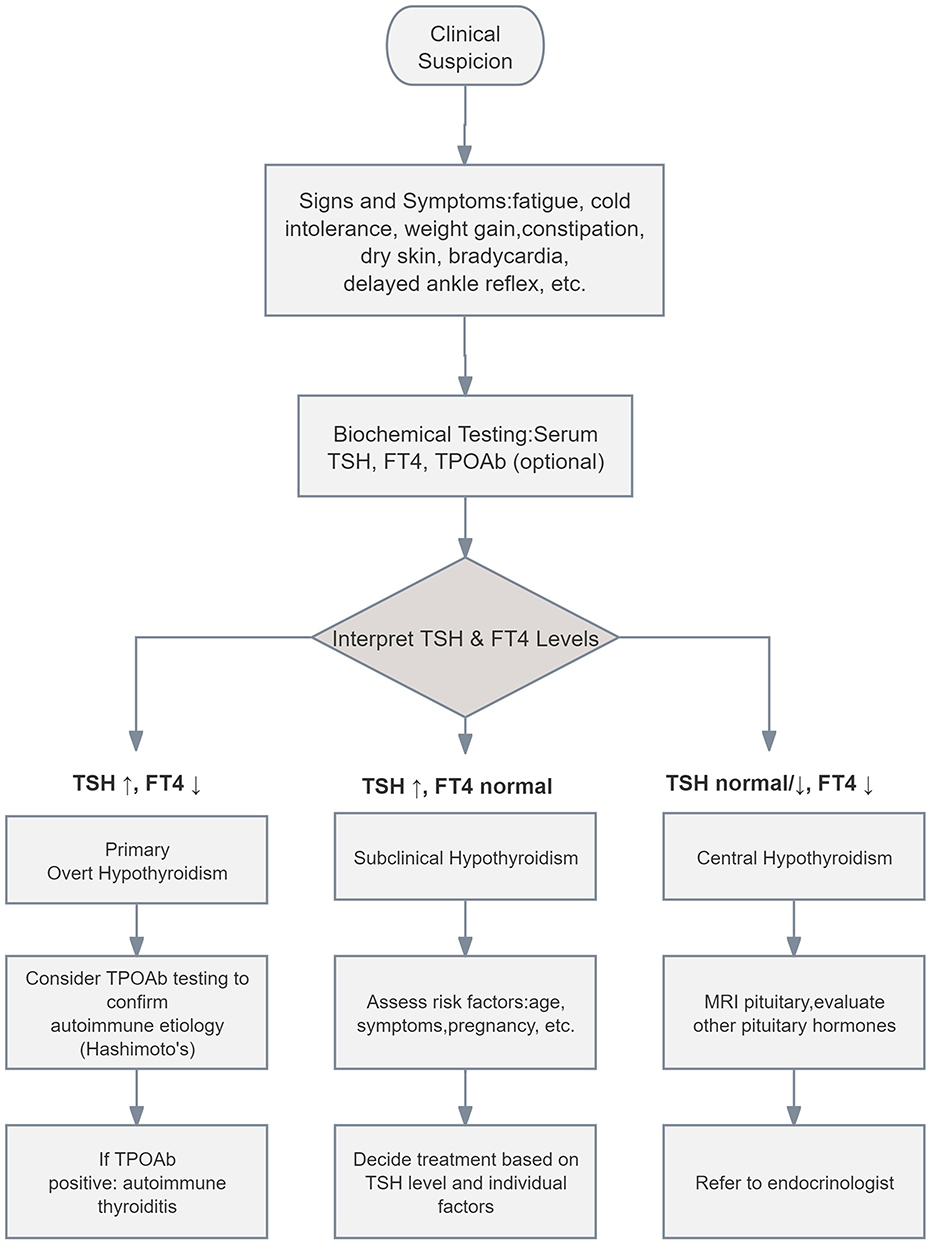 |
Figure 5 Diagnostic pathway for hypothyroidism. ↑:This arrow indicates an increase in the indicator value. ↓: This arrow indicates a decrease in the indicator value. |
Discussion
The reviewed studies predominantly employed TCM decoctions as treatment modalities, incorporating herbs such as Astragalus membranaceus, Codonopsis pilosula, Atractylodes macrocephala, Rehmannia glutinosa, Dioscorea opposita, Prunella vulgaris, Bupleurum chinense, and Epimedium brevicornum, among others. Network pharmacology analyses have demonstrated that the combination of Radix Rehmanniae Preparata and Rhizoma Dioscoreae exerts therapeutic effects on hypothyroidism by modulating processes, including apoptosis, inflammatory response regulation, and cell proliferation. These effects are mediated through MAPK and PI3K-AKT signaling cascades.62 Xu et al63 identified key bioactive compounds in Astragalus membranaceus and Epimedium brevicornum, namely quercetin, kaempferol, and luteolin, targeting molecules such as interleukin-1β, tumor necrosis factor, and the tumor suppressor protein p53. These findings underscore the multicomponent and multitarget characteristics inherent in TCM interventions for hypothyroidism.The primary acupoints utilized in the included studies were Zusanli, Guanyuan, and Mingmen. Animal model investigations have revealed that moxibustion applied at the Guanyuan point significantly reduces apoptosis in thyroid follicular epithelial cells, promotes cellular proliferation, and ameliorates local pathological alterations in hypothyroid rats, thereby enhancing thyroid function.64 Further research indicates that the therapeutic effects of moxibustion at Guanyuan are associated with the regulation of the apoptotic proteins Bcl-2 and Bax, as well as modulation of the PI3K-AKT signaling pathway.65
TCM and acupuncture-medicine combined therapy have shown unique advantages in alleviating clinical symptoms, regulating immune disorders, and improving quality of life in patients with hypothyroidism, our systematic review of the available literature reveals several limitations in current research.The most critical challenge is the high heterogeneity of TCM herbal interventions. For example, even under the same therapeutic principle, the composition of herbal compounds and the compatibility of jun-chen-zuo-shi (principal, assistant, adjuvant, and messenger herbs) vary considerably. In terms of dosage forms and treatment duration, studies have used decoctions, granules, and pastes, with treatment courses ranging from 4 to 12 weeks—variations that directly affect drug absorption and cumulative efficacy. Regarding combination regimens, some studies used TCM alone, some combined TCM with levothyroxine (LT4), and others used acupuncture plus medicine; such overlapping interventions further reduce comparability across studies.This high heterogeneity has introduced substantial inconsistency and uncertainty into the research and clinical translation of TCM for hypothyroidism. It is difficult to identify core effective herbs, optimal formulations, and standardized treatment protocols for different TCM syndromes of hypothyroidism from existing data. As a result, current studies cannot produce reproducible, generalizable conclusions or provide consistent prescribing guidance for clinicians.In addition, the methodological quality of clinical studies is generally low. First, high-quality, large-sample, multi-center RCTs are scarce. Second, condition-specific treatment strategies are lacking: most studies do not distinguish between primary, central, or subclinical hypothyroidism, nor do they design differentiated protocols for special populations such as pregnant women and the elderly, limiting the generalizability of findings. Third, the outcome evaluation system is incomplete: most studies focus only on short-term improvements in laboratory markers, lacking systematic assessment of quality of life, long-term prognosis, and adverse reactions.
To address these limitations, future research should focus on standardization, mechanistic clarification, and formalization to promote clinical translation and academic progress of acupuncture-medicine combined therapy for hypothyroidism.First, unified standards must be established to resolve heterogeneity. For instance, a unified TCM Syndrome Differentiation Standard for Hypothyroidism should be developed. Meanwhile, acupuncture-medicine combined protocols should be standardized, including acupoint combinations, stimulation parameters, treatment duration, and timing of combination with LT4, to lay a foundation for subsequent high-quality research.Second, mechanistic studies should be deepened to explain synergistic effects. Using single-cell sequencing, animal models, and other approaches, the synergistic networks of acupuncture and herbal medicine can be systematically dissected at the organismal, organ, cellular, and molecular levels—especially in regulating immune balance, repairing thyroid follicular cells, and improving energy metabolism—to provide a solid theoretical basis for clinical application.Third, clinical design should be optimized to improve the level of evidence. Multi-center, large-sample, long-term follow-up RCTs are encouraged, with study design strictly compliant with the CONSORT statement. A comprehensive outcome evaluation system should be established that includes laboratory markers, TCM symptom scores, and quality-of-life scales to fully evaluate the clinical value and safety of acupuncture-medicine combined therapy. Ultimately, evidence-based clinical guidelines can be developed to advance the integrated traditional Chinese and Western medicine system for hypothyroidism.
Conclusion
This review confirms that acupuncture-herb combination therapy holds clinical potential as a complementary treatment strategy for hypothyroidism. Current evidence indicates that Traditional Chinese Medicine exerts synergistic effects in improving thyroid hormone levels (TSH, FT3, FT4), reducing autoantibody titers, and alleviating clinical symptoms through the regulation of signaling pathways such as MAPK and PI3K-AKT.However, two core limitations exist in current research: First, interventions are highly heterogeneous, with a lack of standardized syndrome differentiation and treatment protocols; second, the level of evidence is insufficient, as most studies have small sample sizes and lack long-term follow-up, limiting clinical translation.Future research should focus on: 1) Standardization—developing evidence-based consensus on acupuncture-herb combination diagnosis and treatment; 2) Mechanistic exploration utilizing omics technologies to elucidate the multi-target regulatory mechanisms within the neuro-endocrine-immune network; and 3) Evidence enhancement conducting multicenter, large-sample randomized controlled trials to provide high-quality evidence for integrative medicine in the treatment of hypothyroidism.
Disclosure
The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
References
1. Mcdermott M. Hypothyroidism. Ann Internal Med. 2020;173(1):ITC1–17.
2. Grunenwald S, Caron P. Central hypothyroidism in adults: better understanding for better care. Pituitary. 2015;18(1):169–175. doi:10.1007/s11102-014-0559-8
3. Winther K, Rayman M, Bonnema S, et al. Selenium in thyroid disorders - essential knowledge for clinicians. Nat Rev Endocrinol. 2020;16(3):165–176. doi:10.1038/s41574-019-0311-6
4. Chaker L, Razvi S, Bensenor I, et al. Hypothyroidism. Nat Rev Dis Primer. 2022;8(1):30. doi:10.1038/s41572-022-00357-7
5. Kantor ED, Rehm CD, Haas JS, Chan AT, Giovannucci EL. Trends in prescription drug use among adults in the United States from 1999-2012. JAMA. 2015;314(17):1818–1830. doi:10.1001/jama.2015.13766
6. Brito JP, Ross JS, El Kawkgi OM. Levothyroxine use in the United States, 2008-2018. JAMA Intern Med. 2021;181(10):1402–1405. doi:10.1001/jamainternmed.2021.2686
7. Hollowell JG, Staehling NW, Flanders WD. Serum TSH, T 4, and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002;87(2):489–499. doi:10.1210/jcem.87.2.8182
8. Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The Colorado thyroid disease prevalence study. Archiv Inter Med. 2000;160(4):526–534. doi:10.1001/archinte.160.4.526
9. Garmendia Madariaga A, Santos Palacios S, Guillén-Grima F, et al. The incidence and prevalence of thyroid dysfunction in Europe: a meta-analysis. J Clin Endocrinol Metab. 2014;99(3):923–931. doi:10.1210/jc.2013-2409
10. Endocrinology Branch of the Chinese Medical Association. Guideline for diagnosis and management of hypothyroidism in adults. Chin J Endocrinol Metab. 2017;33(2):167–180.
11. Teumer A, Chaker L, Groeneweg S, et al. Genome-wide analyses identify a role for SLC17A4 and AADAT in thyroid hormone regulation. Nat Commun. 2018;9(1):4455. doi:10.1038/s41467-018-06356-1
12. Belin R M, Astor B C, Powe N R, et al. Smoke exposure is associated with a lower prevalence of serum thyroid autoantibodies and thyrotropin concentration elevation and a higher prevalence of mild thyrotropin concentration suppression in the third National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2004;89(12):6077–6086.
13. Chaker L, Korevaar TIM, Medici M. Thyroid function characteristics and determinants: the Rotterdam study. Thyroid. 2016;26(9):1195–1204. doi:10.1089/thy.2016.0133
14. Kuś A, Marouli E, Del Greco MF, et al. Variation in normal range thyroid function affects serum cholesterol levels, blood pressure, and type 2 diabetes risk: a mendelian randomization study. Thyroid. 2021;31(5):721–731. doi:10.1089/thy.2020.0393
15. Liu C, Wang K, Guo J, et al. Small for gestational age is a risk factor for thyroid dysfunction in preterm newborns. BMC Pediatric. 2020;20:1–7. doi:10.1186/s12887-020-02089-7
16. Zimmermann MB, Boelaert K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015;3(4):286–295. doi:10.1016/S2213-8587(14)70225-6
17. Pedersen IB, Knudsen N, Carlé A, et al. A cautious iodization programme bringing iodine intake to a low recommended level is associated with an increase in the prevalence of thyroid autoantibodies in the population. Clin Endocrinol. 2011;75(1):120–126. doi:10.1111/j.1365-2265.2011.04008.x
18. Chaker L, Bianco A, Jonklaas J, et al. Hypothyroidism. Lancet. 2017;390(10101):1550–1562. doi:10.1016/S0140-6736(17)30703-1
19. De Rezende LP, Fortunato Silva J, Da Costa VAA, et al. Effects of maternal hypothyroidism in the gastrointestinal system of male young offspring from Wistar rats. J Dev Orig Health Dis. 2021;12(2):286–292. doi:10.1017/S204017442000029X
20. Rahadini A, Rahadina A. Association between hypothyroidism and liver fibrosis risk: a systematic review and meta-analysis. Clin Experi Hepatol. 2022;8(3):188–194. doi:10.5114/ceh.2022.118594
21. Thvilum M, Brandt F, Almind D, et al. Increased psychiatric morbidity before and after the diagnosis of hypothyroidism: a nationwide register study. Thyroid. 2014;24(5):802–808. doi:10.1089/thy.2013.0555
22. Razvi S, Jabbar A, Pingitore A, et al. Thyroid hormones and cardiovascular function and diseases. J Am College Cardiol. 2018;71(16):1781–1796. doi:10.1016/j.jacc.2018.02.045
23. Tiller D, Ittermann T, Greiser K, et al. Association of serum thyrotropin with anthropometric markers of obesity in the general population. Thyroid. 2016;26(9):1205–1214. doi:10.1089/thy.2015.0410
24. Carlé A, Pedersen I, Knudsen N, et al. Hypothyroid symptoms and the likelihood of overt thyroid failure: a population-based case-control study. Eur J Endocrinol. 2014;171(5):593–602. doi:10.1530/EJE-14-0481
25. Waring A, Arnold A, Newman A, et al. Longitudinal changes in thyroid function in the oldest old and survival: the cardiovascular health study all-stars study. J Clin Endocrinol Metab. 2012;97(11):3944–3950. doi:10.1210/jc.2012-2481
26. Khan L. Thyroid disease in children and adolescents. Pediatr Ann. 2021;50(4):e143–e7. doi:10.3928/19382359-20210322-01
27. Seshadri M, Samuel B, Kanagasabapathy A, et al. Clinical scoring system for hypothyroidism: is it useful? J Gen Intern Med. 1989;4(6):490–492. doi:10.1007/BF02599546
28. Zulewski H, Müller B, Exer P, et al. Estimation of tissue hypothyroidism by a new clinical score: evaluation of patients with various grades of hypothyroidism and controls. J Clin Endocrinol Metab. 1997;82(3):771–776. doi:10.1210/jcem.82.3.3810
29. Beck-Peccoz P, Rodari G, Giavoli C, et al. Central hypothyroidism - a neglected thyroid disorder. Nat Rev Endocrinol. 2017;13(10):588–598. doi:10.1038/nrendo.2017.47
30. Merrill S, Minucci S. Thyroid autoimmunity: an interplay of factors. Vitamin Hormon. 2018;106:129–145.
31. Theofilopoulos A, Kono D, Baccala R. The multiple pathways to autoimmunity. Nat Immunol. 2017;18(7):716–724. doi:10.1038/ni.3731
32. Rapoport B, Mclachlan S. Reflections on thyroid autoimmunity: a personal overview from the past into the future. Hormone Metab Res. 2018;50(12):840–852. doi:10.1055/a-0725-9297
33. Derakhshan A, Korevaar TIM, Taylor PN. The association of maternal thyroid autoimmunity during pregnancy with child IQ. J Clin Endocrinol Metab. 2018;103(10):3729–3736. doi:10.1210/jc.2018-00743
34. Braverman KD, Pearce EN. Iodine and hyperthyroidism: a double-edged sword. Endocr Pract. 2025;31(3):390–395. doi:10.1016/j.eprac.2024.10.014
35. Liontiris MI, Mazokopakis EE. A concise review of hashimoto thyroiditis (HT) and the importance of iodine, selenium, vitamin D and gluten on the autoimmunity and dietary management of HT patients. Points that need more investigation. Hell J Nucl Med. 2017;20(1):51–56. doi:10.1967/s002449910507
36. Aung E, Zammitt N, Dover A, et al. Predicting outcomes and complications following radioiodine therapy in Graves’ thyrotoxicosis. Clin Endocrinol. 2019;90(1):192–199. doi:10.1111/cen.13873
37. Kahraman D, Keller C, Schneider C, et al. Development of hypothyroidism during long-term follow-up of patients with toxic nodular goitre after radioiodine therapy. Clin Endocrinol. 2012;76(2):297–303. doi:10.1111/j.1365-2265.2011.04204.x
38. Bonnema S, Bertelsen H, Mortensen J, et al. The feasibility of high dose iodine 131 treatment as an alternative to surgery in patients with a very large goiter: effect on thyroid function and size and pulmonary function. J Clin Endocrinol Metab. 1999;84(10):3636–3641. doi:10.1210/jcem.84.10.6052
39. Persani L, Ferretti E, Borgato S, et al. Circulating thyrotropin bioactivity in sporadic central hypothyroidism. J Clin Endocrinol Metab. 2000;85(10):3631–3635. doi:10.1210/jcem.85.10.6895
40. Maynard MA, Marino-Enriquez A, Fletcher JA. Thyroid hormone inactivation in gastrointestinal stromal tumors. N Engl J Med. 2014;370(14):1327–1334. doi:10.1056/NEJMoa1308893
41. Chen W. Internal Medicine. Beijing: People’s Medical Publishing House; 2005.
42. Jingrong L. Prescriptions for Emergency. Beijing: People’s Medical Publishing House; 2014.
43. Jiannan Y, Quanlin Z. Discussion on gall disease in treatise on the causes and symptoms of diseases. Modern Chin Med. 2015;35(01):41–42.
44. Hui LIU, Cansheng LU, Haiyan LIU, et al. Based on data mining to analyze the medication rules of Yi Zong Jin Jian · indications of ulcer. Med Theor Pract. 2023;36(01):6–9.
45. ZHAO J. Sheng Ji Zong Lu. Beijing: People’s Medical Publishing House; 1982.
46. Xinhe Z, Yong Z, Xun P, et al. Contribution of surgical orthodoxy to gall disease. Sichuan J Tradit Chin Med. 2016;34(11):13–15.
47. Min YU, Ying JI, Liang GU. Observation on the therapeutic effect of 50 Ying acupuncture combined with acupoint injection on hypothyroidism. J Shanghai Jiaotong Univer. 2010;30(09):1156–1159.
48. Pengyun Z, Junjie G. Guo Junjie’s experience in treating Hashimoto’s thyroiditis with hypothyroidism. Hunan J Tradit Chin Med. 2018;34(11):25–26.
49. Wei F, Ruquan C. Professor Chen Ruquan’s experience in treating hypothyroidism with anemia. World J Traditional Chin Med. 2017;12(04):853–856.
50. Yingjie Z, Songchang X. Clinical study on treatment of Hashimoto’s thyroiditis with hypothyroidism by Yishen Jianpi Xiaoying decoction. Henan Tradit Chin Med. 2023;43(07):1067–1071.
51. Yingna W, Tianshu G, Pin L, et al. Clinical observation of Chaihu Shugan Powder in treating Hashimoto’s thyroiditis with hypothyroidism of liver depression and spleen deficiency. J Zhejiang Univer Tradit Chin Med. 2023;47(03):291–5+311.
52. Chen Z, Jing L, Juju S. Clinical effect of modified Shengjiang Decoction and Banxia Houpu Decoction on subclinical hypothyroidism of Hashimoto’s thyroiditis with liver depression and spleen deficiency. China Med J. 2022;19(33):71–74.
53. Aiping Z, Xiaofan Y, Yuehong T, et al. Effect of modified Yougui pill decoction combined with Euthyrox on symptoms and thyroid function in patients with hypothyroidism. J Pract Int Med Tradit Chin Med. 2022;36(02):74–76.
54. Chen Y, Su T. Research progress of acupuncture and moxibustion treatment of hypothyroidism. J Traditional Chin Med. 2020;48(04):63–67.
55. Zhang JY, Zou P, Fang QX. Clinical observation of warming needle moxibustion on subclinical hypothyroidism of spleen-kidney Yang deficiency type. J Guangzhou Univer Tradit Chin Med. 2021;38(02):294–300.
56. Caixia W, Chongyao H, Tiansheng Z, et al. Effect of fire acupuncture on blood lipid in hypothyroidism model rats. J Shanxi Univer Tradit Chin Med. 2019;20(06):410–412.
57. Julun Z. Analysis of clinical efficacy of warming needle moxibustion on adult hypothyroidism. Chin Contemp Med. 2013;20(16):139–40+42.
58. Clinical study on, Wang WL, Gu JH, Wang J, et al. And Qi circulation “acupuncture therapy for hypothyroidism of Hashimoto’s thyroiditis of stagnation of liver-qi type. J Traditional Chin Med. 2023;29(12):57–61.
59. Gao D, Jiang SL, Ding JP. Clinical study on treatment of pregnancy complicated with hypothyroidism by traditional Chinese medicine combined with acupuncture and moxibustion. New J Tradit Chin Med. 2021;53(18):76–79.
60. Chunping H, Jianfang C, Manman L, et al. Curative effect observation of Shugan Sanjie Xiaoying decoction combined with acupoint catgut embedding on Hashimoto’s thyroiditis with hypothyroidism and goiter of liver depression and spleen deficiency type. J Modern Integrat Tradit Chin West Med. 2020;29(27):2997–3002.
61. Zhulin LIU, Shuyan LI. Curative effect observation of acupuncture combined with Bupi Wenshen ointment on subclinical hypothyroidism and its influence on thyroid function and blood lipid. Hebei Tradit Chin Med. 2017;39(09):1373–1377.
62. Yan L, Yanqi C, yuan F. Exploring the medication rule and mechanism of traditional Chinese medicine in the treatment of hypothyroidism based on data mining and network pharmacology. J Yunnan College Tradit Chin Med. 2022;45(05):79–87.
63. Haixu XU, Changhui LI. Exploring the mechanism of astragalus-epimedium in the treatment of hypothyroidism based on network pharmacology and molecular docking technology. J Chronic Dis Integrat Tradit Chin West Med. 2024;1(01):39–47.
64. Kang CM, Liu D, Yifan H. Effect of moxibustion at Guanyuan on hypothyroidism in rats. J Traditional Chin Med. 2022;37(09):1921–1927.
65. Chunmei K, Shan L, Zhiling G. Study on the mechanism of moxibustion at Guanyuan point for hypothyroidism based on the regulation of PI3K-AKT pathway. World J Integrat Tradit Chin West Med. 2021;16(10):1831–1835.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.