Back to Journals » International Medical Case Reports Journal » Volume 18
From Eruptive Xanthoma to Acute Pancreatitis: Clinical Warning and Implications of Rapid Disease Progression
Authors Zhu Y ![]() , He X, Lan Y
, He X, Lan Y ![]() , Deng Y
, Deng Y
Received 28 March 2025
Accepted for publication 18 July 2025
Published 28 July 2025 Volume 2025:18 Pages 943—947
DOI https://doi.org/10.2147/IMCRJ.S531146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Yanling Zhu, Xin He, Ya Lan, Yongqiong Deng
Department of Dermatology, Chengdu Integrated TCM and Western Medicine Hospital, Chengdu, Sichuan Province, People’s Republic of China
Correspondence: Yongqiong Deng, Email [email protected]
Abstract: Xanthoma is a common cutaneous manifestation typically associated with abnormal lipid metabolism, particularly hyperlipidemia. Both hyperlipidemia and hyperglycemia are significant components of metabolic syndrome and can elevate the risk of pancreatitis. Acute pancreatitis is a serious inflammatory disease that can be life-threatening and may be triggered by various factors, including hyperlipidemia. In conclusion, there appears to be a potential link between xanthoma, hyperlipidemia, and acute pancreatitis, which seem to be distinct diseases. By analyzing the diagnostic and treatment processes for this patient, we found that early identification and intervention in xanthoma patients are crucial. This approach not only aids in controlling the progression of xanthoma but also helps prevent a range of serious complications associated with hyperlipidemia, such as acute pancreatitis. Ultimately, this reduces the impact of the disease on health and enhances the quality of life and survival rates for patients.
Keywords: xanthoma, pancreatitis, hyperlipidemia, hyperglycemia, case
Introduction
Xanthoma is a lesion characterized by the deposition of lipid components in the skin tissues. The skin lesions of xanthoma include papules, plaques, and nodules. Its occurrence is closely associated with hyperlipidemia,1 which has been found to be a risk factor for a variety of medical diseases such as acute pancreatitis and coronary heart disease. We present a case of a patient who visited a dermatology clinic with xanthomas as the initial manifestation. Blood test results revealed significantly elevated lipid levels. Despite aggressive treatment aimed at controlling these lipids, the patient unfortunately developed a potentially life-threatening case of acute pancreatitis.
Case Information
A 20-year-old female patient was admitted to the Department of Dermatology at our hospital due to yellowish-red papules on her trunk and limbs, accompanied by itching and pain for the past two weeks. The patient developed rashes on her trunk and limbs without any identifiable triggers, which she initially disregarded. Over the past two weeks, the rash progressively increased in size and number, accompanied by intermittent itching and pain. Physical examinations in the dermatology department revealed yellow or reddish semicircular papules that were either scattered or densely distributed on the skin of the trunk and limbs. These papules were firm to the touch and exhibited a smooth, non-scaly surface. Dermoscopy revealed orange-yellow structureless areas with dendritic capillary dilation, surrounded by vascular membranes (The lesions and dermoscopic findings are shown in Figure 1).
 |
Figure 1 The patient’s skin lesions and dermoscopic (65x) photos. |
The patient was obese with BMI >30. She was previously fit and denied any family history of diabetes mellitus or hyperlipidemia. Laboratory tests revealed the following results: triglycerides (TG) at 79.37 mmol/L, total cholesterol (CHOL) at 17.30 mmol/L, high-density lipoprotein (HDL-C) at 5.47 mmol/L, low-density lipoprotein (LDL-C) at 1.11 mmol/L, and fasting glucose (GLU) at 16.86 mmol/L. A skin biopsy indicated a significant infiltration of histiocytes in the superficial layer of the dermis and reticular layer, along with an increased number of foamy cells (Figure 2).
 |
Figure 2 Pathological picture of the patient’s skin biopsy. (A) shows 20x HE staining, (B) shows 40x HE staining. |
Dermatoscopy and pathology confirmed the diagnosis of eruptive xanthoma. According to the blood examination results of the patient, she can be diagnosed with mixed hyperlipidemia. The patient was subsequently transferred to the cardiology department for lipid-lowering therapy, which included an iloyumab injection. Five days later, the patient went to the surgery department with mid-upper abdominal pain. Blood tests revealed glucose levels of 27.8 mmol/L, cholesterol levels of 13.07 mmol/L, triglycerides at 68.29 mmol/L, HDL-C at 4.19 mmol/L, and LDL-C at 0.04 mmol/L (Table 1 illustrates the comparison of the results from the two blood tests). An abdominal CT scan indicated acute pancreatitis with scattered peripheral exudates. The diagnosis was hyperlipidemic pancreatitis (moderate to severe). The patient was discharged from the hospital with improvement following treatment of inhibition of pancreatic enzyme activity, lowering lipid levels, and adjusting blood glucose. After one week of follow-up blood examination, her total cholesterol decreased to 3.95 mmol/L, and triglycerides decreased to 2.66 mmol/L. The rash completely subsided, leaving significant hyperpigmentation.
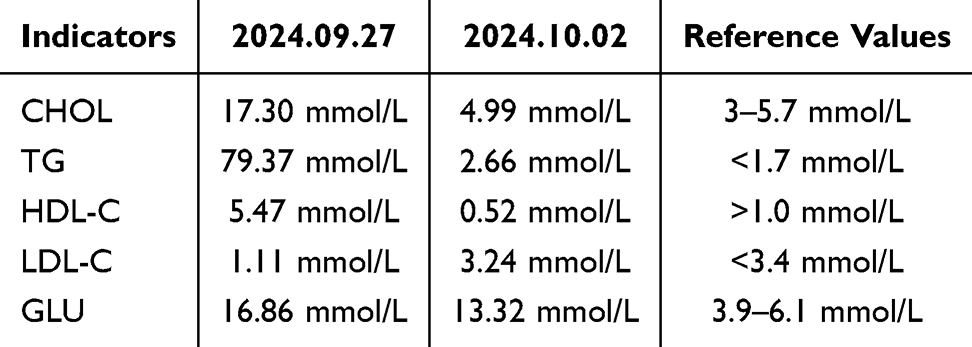 |
Table 1 Examination Results of Blood Lipid Related Indicators of This Patient |
Discussion
Xanthomas can be divided into primary and secondary. Familial xanthomas in primary xanthomas are often accompanied by abnormal lipid metabolism. Some xanthomas may also be related to some rare diseases.2 There is a potential pathophysiological link between eruptive xanthoma and hyperlipidemia and hyperglycemia.3 According to Frederickson hyperlipidemia classification, eruptive xanthoma associated hyperlipidemia can be seen in type 1 (increased chylomicrons), type 4 (increased very low density lipoprotein (VLDL)) and type 5 Hypertriglyceridemia.4 The abnormal metabolism of triglycerides leads to the increase of lipid composition in the circulation. Xanthomas may appear when the lipid composition deposited on the skin. Hypertriglyceridemic pancreatitis may be triggered by an increase in plasma triglyceride concentration, leading to local ischemia, inflammation, and the release of pancreatic enzymes. Similar cases have been reported in the literature, suggesting that eruptive xanthomas may serve as an early cutaneous marker of metabolic abnormalities.3
In this case, the patient presented to the dermatology department with cutaneous manifestations of xanthoma, which subsequently progressed to acute pancreatitis within a week, despite a rapid referral to an internal medicine specialist for aggressive treatment following the discovery of an extremely abnormal lipoglycemic state. This suggests that extreme hyperlipidemia (TG > 50 mmol/L) may exceed the conventional treatment threshold and necessitate more aggressive interventions. We also consider a correlation with the patient’s obesity, elevated BMI, and the lack of timely consultation regarding the presence of xanthomatous skin lesions. This underscores the importance of early recognition of the role of eruptive xanthomas as warning signs.5,6 Previous case reports have demonstrated that early presentation and intervention for patients with xanthomas in the dermatology department have been successful in preventing the progression to serious outcomes, such as pancreatitis.7 Therefore, dermatologists should pay closer attention to patients with eruptive xanthomas. They should conduct metabolic evaluations and interventions as early as possible, provide thorough patient education, and collaborate with specialists in cardiovascular medicine, endocrinology, and other internal medicine departments. This multidisciplinary approach aims to optimize disease management and enhance patient prognosis.
In addition, the literature indicates that other types of xanthomas or diseases with similar skin lesions with xanthomas may be associated with conditions such as multiple myeloma and histiocytosis.8,9 This suggests that the presence of xanthomas may have significant predictive value for various medical disorders, particularly metabolic disorders, and warrants further investigation and research.
Conclusion
The pathophysiological association between eruptive xanthomas and acute pancreatitis suggests a potential comorbid condition since both of them are closely related to hyperlipidemia. The high-fat state in the circulation not only leads to lipid deposits (xanthomas) on the skin, but also induces abnormal activation of pancreatic digestive enzymes and inflammatory responses. Eruptive xanthomas may serve as an early indicator of metabolic abnormalities and an increased risk of pancreatitis, particularly in individuals who are obese (BMI ≥ 30), present with sudden skin lesions that progress rapidly, and require immediate evaluation of their lipid profile. There is an urgent need to establish a comprehensive skin-metabolism pathway, which includes immediate lipid screening for patients with xanthomas, the development of an urgent intervention program for triglyceride levels exceeding 50 mmol/L, and patient education aimed at reducing metabolic risk in the obese population. This underscores the significance of this case report.
Data Sharing Statement
The data that support the findings of this study are available from the first author upon reasonable request (Yanling Zhu, [email protected]).
Consent Statement
The patient in this case signed an informed consent form and agreed to provide the case information and photographic images for the manuscript. The publication of case and image information does not require institutional approval.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has no fund.
Disclosure
All authors have no conflicts of interest in this work.
References
1. Zak A, Zeman M, Slaby A, et al. Xanthomas: clinical and pathophysiological relations. Biomed Papers Med Faculty Univ Palacky Olomouc Czechoslovakia. 2014;158(2):181–188. doi:10.5507/bp.2014.016
2. De Schaetzen V, Richert B, De La Brassinne M. [Xanthomas]. Revue Medicale de Liege. 2004;59(1):46–50.
3. Vu PQ, Thiriveedi M, Patel S, et al. Case report: acute pancreatitis in an uncontrolled diabetic patient presenting with a skin rash later found to be eruptive xanthoma, a dermatological manifestation and diagnostic clue to recognizing hypertriglyceridemia as the cause of disease. Cureus. 2024;16(7):e64563. doi:10.7759/cureus.64563
4. Pai VV, Shukla P, Bhobe M. Combined planar and eruptive xanthoma in a patient with type lla hyperlipoproteinemia. Indian J Dermatol Venereol Leprol. 2014;80(5):467–470. doi:10.4103/0378-6323.140323
5. Marogi EP, Ohiomoba RO, Stone NJ. Eruptive xanthomas: importance of recognition to reduce delay of effective triglyceride reduction. Am J Med. 2022;135(4):444–447. doi:10.1016/j.amjmed.2021.09.026
6. Stark M, Stuart J. Eruptive xanthoma in the setting of hypertriglyceridemia and pancreatitis. Am J Emerg Med. 2018;36(8):
7. Munoz NR, Agwuegbo CC, Gauhar F. Eruptive xanthomas precipitated by severe hypertriglyceridemia from diabetes and alcohol use. Cureus. 2023;15(8):e43288. doi:10.7759/cureus.43288
8. Marien KJ, Smeenk G. Plane xanthomata associated with multiple myeloma and hyperlipoproteinaemia. Br J Dermatol. 1975;93(4):407–415. doi:10.1111/j.1365-2133.1975.tb06514.x
9. Seward JL, Malone JC, Callen JP. Generalized eruptive histiocytosis. J Am Acad Dermatol. 2004;50(1):116–120. doi:10.1016/S0190-9622(03)02789-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.