Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
From Anatomical Modifications to Skin Quality: Case Series of Botulinum Toxin and Facial Fillers for Facial Feminization in Transgender Women
Authors Viscomi B
Received 2 April 2022
Accepted for publication 2 June 2022
Published 14 July 2022 Volume 2022:15 Pages 1333—1345
DOI https://doi.org/10.2147/CCID.S363882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Video abstract presented by Bianca Viscomi.
Views: 273
Bianca Viscomi
Dermatology, Private Practice, São Paulo, São Paulo, Brazil
Correspondence: Bianca Viscomi, Dermatology, Private Practice, R Correia Dias, 530 suite 131, São Paulo, São Paulo, ZIP 04104-001, Brazil, Tel +55 11 97222-0525 ; +55 113051-2304, Email [email protected]
Abstract: A transgender individual is someone who does not identify with his or her biological sex1. During the transgender transition process, minimally invasive procedures (MIP) provide a versatile tool in the clinician’s therapeutic armamentarium, since the changes can be impactful for the patient, yet reversible, especially for the patient who is unsure about proceeding with a definite surgery. We report 5 cases of facial feminization of transgender women, illustrating the use of minimally invasive facial remodeling procedures for male-to-female transitioning patients.
Keywords: transgender, feminization, botulinum toxin, hyaluronic acid fillers, calcium hydroxyapatite, skin quality
Introduction
A transgender individual is someone who does not identify with his or her biological sex.1 Trans beauty imposes a unique aesthetic task, since transgender women may seek feminization, but the aesthetic goal may not be achievement of femininity or masculinity itself, but rather acquiring feminine or masculine attributes that best align with the patient’s self-affirmation.2 In order to recognize themselves as women, transgender women go through a transition process, which includes hormonal therapy, psychological support, and physical alterations that can be accomplished by surgery or minimally invasive procedures. According to literature data, transgender women often prefer to modify their faces, prior to body alterations3.
Minimally invasive procedures (MIP) play an important role in the transition process for many reasons: MIP provide fast, reversible, and impactful results, with lower risks and downtime, whilst results with hormonal therapy, for example, may take 2 years to fully develop. There is minimal need for psychological assessment, pre-medication, or other delays that would routinely be needed before surgery.4 Especially for patients who are unsure about proceeding with definitive surgery, injectables can serve as a reversible surrogate for what patients can potentially expect from a definite facial surgery.5 Moreover, for those patients who are not suitable for surgery, MIP may remain the only option.5 Health care providers should be familiar with the needs of the transgender patient population.3 Nevertheless, applicable literature in the field is still lacking. Thus, herein we present 5 cases of facial feminization in transgender women, illustrating the use of minimally invasive facial remodeling procedures for male-to-female transitioning patients.
Materials and Methods
All procedures performed in this report involving human patients were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Ethics Approval
The study was approved by a centralized institutional review board (Faculdade Santa Marcelina 53,265,821.9.0000.8125/5.218.58). No institutional approval was required to publish case details. Written informed consent has been provided by all the patients to have the case details and any accompanying images published.
We report 5 cases of facial feminization of transgender women with minimally invasive procedures (ie, hyaluronic acid fillers (HA; Belotero®; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany), botulinum toxin type A (BonTA; Incobotulinum toxin; Xeomin®, Merz Pharmaceuticals GmbH, Frankfurt, Germany) and calcium hydroxyapatite (CaHA; Radiesse®; Merz Pharmaceuticals GmbH, Frankfurt, Germany)). Eligible patients were transgender women, older than 18 years, who sought facial feminization through MIP. Photographs were taken at baseline, immediately after injection and after a follow-up interval of 60 days after the procedure, with the longest follow-up being 140 days. Two-dimensional (2D) photographs were taken, using a stereovision digital camera (LifeVizTM; Quantificare S.A., Sophia Antipolis, France). Standardized indirect light, aperture, speed and distance of the camera were controlled. Digital photographs were reconstructed in three dimensions (3D) with LifeVizTM App software (Quantificare S.A., Sophia Antipolis, France). Two-dimensional (2D) photographs were taken, using a digital camera (Vectra Software, Canfield, New Jersey, United States). Standardized indirect light, aperture, speed and distance of the camera were controlled. Digital photographs were reconstructed in three dimensions (3D) with Vectra Software (Canfield, New Jersey, United States). At the last meeting for evaluation, patients were asked to rate the overall improvement after the treatment using a 4-point scale (1 = Excellent (90–100% improvement); 2 = Good (50–89% improvement); 3 = Fair (less than 50% improvement); 4 = No change (no improvement)).
Case Series Presentation
Demography
Patients enrolled were between 28 and 38 years of age (median age 31 years) and no relevant medical history (eg, diabetes, previous facial surgery, myasthenia gravis, Eaton-Lambert syndrome, multiple sclerosis, history of upper eyelid ptosis or Bell’s palsy); urticaria, angioedema and allergies, conditions that cause Koebner response, hypertrophic scars or keloids; connective tissue diseases; recent history of upper respiratory tract infections or acute respiratory infections; presence of active infections, dental treatment, and other inflammatory processes in the area to be treated, use of medications that cause bleeding. Only one patient did not report use of hormonal therapy (Case#2). Two patients were in use of oral cyproterone acetate 25 mg only (Case# 1 and case #3); 2 years and 4 years, respectively. One patient (Case #4) was in use of oral cyproterone acetate 50 mg and oral estrogen 3 mg for 1 month and one patient was in use of topical estrogen (Case#5). No patient had performed any injectable procedure within the last 12 months, had any surgery or used permanent fillers.
Treatment Plan
Patients were treated first with botulinum toxin type A, followed by calcium hydroxyapatite injection 15 days thereafter. Hyaluronic acid (HA) injection was performed 30 days after the first CaHA injection session. Nevertheless, if more than one CaHA session was needed and different anatomical areas were approached, CaHA and HA injections could be performed in the same treatment session. A summary of all treatment options for facial feminization and rationale for each type of injectable used in this study is provided in Figures 1–3. Dosage or volume per area and product injected into each patient are displayed in Tables 1 and 2.
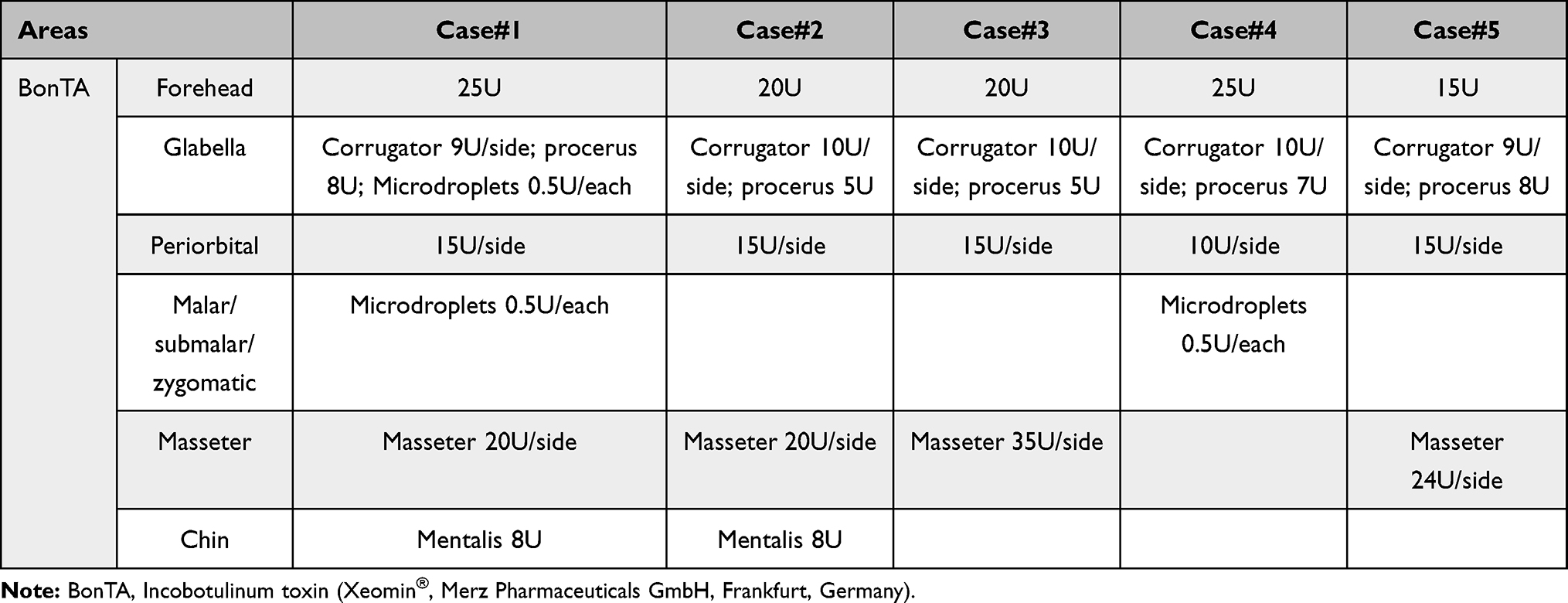 |
Table 1 BonTA Treatment Details per Patient |
 |
Table 2 HA and CaHA Treatment Details per Patient |
 |
Figure 1 Treatment options for transgender facial feminization with BonTA. |
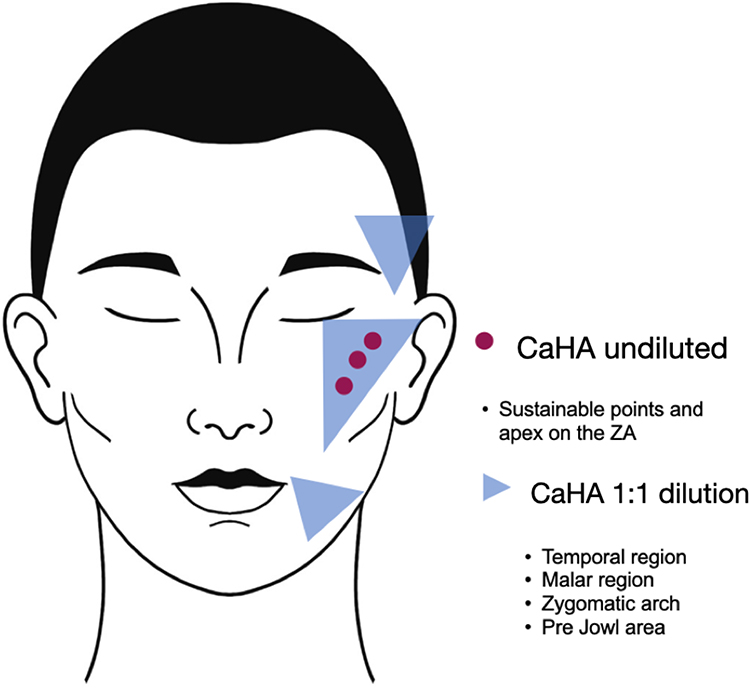 |
Figure 2 Treatment options for transgender facial feminization with CaHA. |
 |
Figure 3 Treatment options for transgender facial feminization with hyaluronic Acid. |
Upper Face
BonTA was injected into the forehead following the “One21” technique6 to minimize dynamic wrinkles, and create a flatter and softer forehead, whereas frontalis muscle activity above the lateral one-third of the brow was retained to lift the eyebrow, giving the eyebrow a more angled shape.5 Treatment of the glabella with high doses of BonTA aimed at glabellar complex weakening and eyebrow arching (Figures 1 and 4–8).
 |
Figure 4 Case #1: Images taken with Vectra Software at baseline (A, C, E, G and I) and after 60 days of the first treatment session with Vectra Software (B, D, F, H and J). |
 |
Figure 5 Case #2: Images taken with Vectra Software at baseline (A, C, E, G and I) and after 60 days of the first treatment session with Vectra Software (B, D, F, H and J). |
 |
Figure 6 Case#3: Images taken with Vectra Software at baseline (A, C, E, G and I) and after 60 days of the first treatment session with Vectra Software (B, D, F, H and J). |
 |
Figure 7 Case #4: Images taken with Vectra Software at baseline (A, C, E, G and I) and after 60 days of the first treatment session with Vectra Software (B, D, F, H and J). |
 |
Figure 8 Case #5: Images taken with Vectra Software at baseline (A, C, E, G and I) and after 140 days of the first treatment session (B, D, F, H and J). |
CaHA diluted 1:1 was injected with a 22G cannula in the anterior temporal and forehead areas to improve neocollagenesis, whereas a viscous, yet malleable and easy to shape HA7 (HA-V; Belotero Volume®; Cohesive polydensified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany) was injected with a 22G cannula in the subcutaneous plane and with needle in the supraperiosteal plane in order to achieve a more convex forehead, improve the temporal fossae (Figures 2 and 4), soften the brow ridge and raise the lateral brow. A massage to accommodate the product was performed immediately after the injection.
Middle Face
Small boluses of subcutaneous CaHA (0.05mL/point; dilution 1:1) were injected into the malar and sub-malar areas, along with ascending vectors to improve skin quality and acne scars with minimal volume gain (Figures 2 and 4–8).8 For a more curvilinear cheekbone and to relocate the apex lateral and superiorly, HA-V was injected with a 22G cannula in the subcutaneous plane, in the malar and zygomatic areas (Figure 3–7), due to its capability of projection while retaining moldability, allowing a subtle transition between the treated and untreated areas.7
In the pyriform fossa and nasolabial folds, the product of choice was a high projection capacity HA, which does not deform easily (HA-I; Belotero Intense®; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany),7 allowing correction to be achieved with a smaller amount of product (Figures 3–5, 7 and 8).
In the tear though, since the skin is thinner, a low elasticity and viscosity and high cohesivity HA (HA-B; Belotero Balance®; Cohesive polydensified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany) was injected to provide seamless and natural tissue integration properties (Figures 3–7).7 Micro-droplets of BonTA were injected into the malar area to reduce pore size and sebaceous activity (Figures 1, 4 and 7).
Lower Face
BonTA was injected into the masseter (Figures 1, 4–6 and 8) and mentalis (Figures 1, 4 and 5) to promote a more feminine heart-shaped lower contour,5 while undiluted CaHA was injected along the jawline to improve mandible contour, without volumization (Figures 3 and 7).
Injections of HA-B into the superficial dermis were used to improve lip contour, while HA-V was chosen to improve lip volume, maintaining the upper lip/lower lip proportion to ensure a natural aesthetic outcome (Figures 3–8).
All patients rated the overall improvement after the treatment as good (1/5) or excellent (4/5) at the final evaluation.
Discussion
Although the estimated number of transgender individuals in the US is increasing, this community still struggles to get adequate health care access.4,9,10 Transgender patients face several health care barriers, among which are social stigmatization or discrimination,11 economic marginalization and lack of specialized healthcare providers.1 Due to hurdles to receive adequate medical care or aesthetic procedures, transitioning patients may submit themselves to serious risks during the gender transition process, such as injection of liquid silicone or other illegal products directly into tissues, often performed in unsanitary conditions by untrained, unqualified providers.1,12 Moreover, transgender beauty differs from regular cis-women aesthetic approach, since it involves not only rejuvenation and/or beautification but rather acquiring feminine or masculine attributes that best align with the patient’s self-affirmation.2 In Brazil, where the life expectancy of a transgender individual is 35 years of age, half of the age of the general population, mainly due to violence and suicide,13 medical transitioning assistance has an even more profound impact since it may improve patient’s acceptance in the society and result in protection from violence and increase in life expectancy. Thus, it is paramount that health care providers are well trained in caring for that part of the population. While the literature upon facial remodeling of cis-women with MIP is abundant, the use of MIP for facial remodeling in the scope of the transitioning process of transgender women is still scarce.
Generally accepted characteristics of a female face include smooth forehead with some convexity, small narrow nose, arched eyebrows, wider eyes, prominent and full cheekbones, heart-shaped lower face, and full vermilion lips.5 Figures 1–3 aim to provide a simple and schematic overview of the different treatment possibilities when using MIP for facial feminization. Nevertheless, clinicians should be aware that there are different steps to be taken in the transition process, and that the needs and expectations may vary at each stage. For instance, changes in facial structure, soft tissue distribution and skin quality vary if a patient has not yet started hormone therapy compared to the patient who has been on hormone therapy for many years.2 Thus, the treatment plan should be tailored for each patient’s needs and transitioning phase. Comparing male and female skulls, a prominent supraorbital region is characteristic of men, whereas among females the forehead is straighter, the glabella is more curved, less pronounced and the supraorbital rim is less noticeable than males.14 BonTA injection may be used to feminize the forehead, eyebrows, or periorbital skin by eliminating rhytids and widening of the eyes, whereas HA improves the forehead convexity and smoothens the supraorbital-forehead transition. Transgender women may require higher doses of neurotoxin in all treatment areas because individuals assigned male at birth tend to have greater muscle mass compared to individuals assigned female.5 Female skulls also present a more curvilinear and prominent cheekbone, with more subtle angles, and the injection of HA lateral on the zygomatic arch and inferolateral to the lateral canthus, can approximate the female apex and minimize the angles.14 Usually, the volume of AH required to achieve the desirable results is greater than compared to the amount needed for a cis female of the same age. CaHA used undiluted or slightly diluted provides immediate correction that is gradually followed by new tissue formation through neocollagenesis, leading to long-term deposition of new collagen.15 As a result, the use of CaHA in the malar area increases support in the mid-third, reducing the overall HA volume needed.
In Western cultures, the ideal width of the female chin is approximately the same width as the intercanthal distance and special care must be taken not to masculinize a female face by making the chin too wide.7 Therefore, a single supraperiosteal injection was performed with HA-I to project the chin (Figures 3–5 and 7). Moreover, since in males the mandible is larger than in females,14 BonTA was injected in the masseter to induce gradual atrophy and give a more heart-shaped contour to the face. For an optimal lip contour,16 comprising a well-defined upper and lower vermilion border, cupids bow, and a J-shaped curve, a low elasticity and low viscosity HA was used, whilst lip volume was accomplished with injections of a moldable HA.
The process of feminization must include not only anatomical modifications but also skin quality assessment, since skin features are also important for gender perception. Skin quality significantly influences perception of age, attractiveness, health and youth17. Good skin quality is defined as healthy, undamaged, youthful in appearance, and it can be described across all ethnicities by four emergent perceptual categories (EPCs): skin tone evenness, skin surface evenness, skin firmness, and skin glow.17 Baseline hormonal variation also exerts a great influence on the skin. Although testosterone may yield a denser collagen network, the skin becomes thicker with more visible pores and higher secretion of sebum and sweat.1 MIP are versatile tools since they can also be used to improve skin quality. Injections of intradermal micro-droplets of BonTA in the malar area and forehead lead to pore size and sebaceous activity minimization.18 Besides, when used in hyper-diluted form (ie, 1.5 mL of product plus ≥1.5 mL of diluent), CaHA has a minimal or absent immediate volumizing effect, generating only long-term tissue remodeling by the CaHA microspheres, allowing its injection more superficially for dermal rejuvenation, improving skin appearance and reducing pores and scars.8
Conclusion
MIP allow facial remodeling of transgender women, tailoring of the cosmetic treatment plan, yielding fast and reversible results, and should be considered important and versatile tools in the clinician’s therapeutic assortment during the transition process of transgender women.
Funding
This publication was funded by Merz Pharmaceuticals. All injectable products were provided by Merz Pharmaceuticals. The sponsor had no role in the design and conduct of the study, collection, analysis and interpretation of data.
Disclosure
Dr Viscomi is a speaker for Merz Pharmaceuticals. The author reports no other potential conflicts of interest in relation to this work.
References
1. Dhingra N, Bonati LM, Wang EB, Chou M, Jagdeo J. Medical and aesthetic procedural dermatology recommendations for transgender patients undergoing transition. J Am Acad Dermatol. 2019;80(6):1712–1721. doi:10.1016/j.jaad.2018.05.1259
2. de Boulle K, Furuyama N, Heydenrych I, et al. Considerations for the use of minimally invasive aesthetic procedures for facial remodeling in transgender individuals. Clin Cosmet Investig Dermatol. 2021;14:513–525. doi:10.2147/CCID.S304032
3. Ginsberg BA, Calderon M, Seminara NM, Day D. A potential role for the dermatologist in the physical transformation of transgender people: a survey of attitudes and practices within the transgender community. J Am Acad Dermatol. 2016;74(2):303–308. doi:10.1016/j.jaad.2015.10.013
4. MacGregor JL, Chang YC. Minimally invasive procedures for gender affirmation. Dermatol Clin. 2020;38(2):249–260. doi:10.1016/j.det.2019.10.014
5. Ascha M, Swanson MA, Massie JP, et al. Nonsurgical management of facial masculinization and feminization. Aesthet Surg J. 2019;39(5):NP123–NP137. doi:10.1093/asj/sjy253
6. de Sanctis Pecora C. One21: a novel, customizable injection protocol for treatment of the forehead with IncobotulinumtoxinA. Clin Cosmet Investig Dermatol. 2020;13:127–136. doi:10.2147/CCID.S237519
7. van Loghem J, Sattler S, Casabona G, et al. Consensus on the use of hyaluronic acid fillers from the cohesive polydensified matrix range: best practice in specific facial indications. Clin Cosmet Investig Dermatol. 2021;14:1175–1199. doi:10.2147/CCID.S311017
8. de Almeida AT, Figueredo V, da Cunha ALG, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7(3):e2160. doi:10.1097/GOX.0000000000002160
9. Clark K, Fletcher JB, Holloway IW, Reback CJ. Structural inequities and social networks impact hormone use and misuse among transgender women in los angeles county. Arch Sex Behav. 2018;47(4):953–962. doi:10.1007/s10508-017-1143-x
10. Scheim AI, Coleman T, Lachowsky N, Bauer GR. Health care access among transgender and nonbinary people in Canada, 2019: a cross-sectional survey. CMAJ Open. 2021;9(4):E1213–E1222. doi:10.9778/cmajo.20210061
11. Jia JL, Polin DJ, Sarin KY. Ways to improve care for LGBT patients in dermatology clinics. Dermatol Clin. 2020;38(2):269–276. doi:10.1016/j.det.2019.10.012
12. Murariu D, Holland MC, Gampper TJ, Campbell CA. Illegal silicone injections create unique reconstructive challenges in transgender patients. Plast Reconstr Surg. 2015;135(5):932e–933e. doi:10.1097/PRS.0000000000001192
13. Goodman M, Adams N, Corneil T, Kreukels B, Motmans J, Coleman E. Size and distribution of transgender and gender nonconforming populations. Endocrinol Metab Clin North Am. 2019;48(2):303–321. doi:10.1016/j.ecl.2019.01.001
14. Toledo Avelar LE, Cardoso MA, Santos Bordoni L, de Miranda Avelar L, de Miranda Avelar JV, de Miranda Avelar JV. Aging and sexual differences of the human skull. Plast Reconstr Surg Glob Open. 2017;5(4):e1297. doi:10.1097/GOX.0000000000001297
15. Loghem J, Van, Yutskovskaya YA, Werschler WP. Calcium hydroxylapatite: over a decade of clinical experience. J Clin Aesthet Dermatol. 2015;8(1):38–49.
16. Ghannam S, Sattler S, Frank K, et al. Treating the lips and its anatomical correlate in respect to vascular compromise. Facial Plast Surg. 2019;35(2):193–203. doi:10.1055/s-0039-1683856
17. Goldie K, Kerscher M, Fabi SG, et al. Skin quality – a holistic 360° view: consensus results. Clin Cosmet Investig Dermatol. 2021;14:643–654. doi:10.2147/CCID.S309374
18. Park JY, Cho S, Hur K, Lee D. Intradermal Microdroplet Injection of Diluted Incobotulinumtoxin-A for Sebum Control, Face Lifting, and Pore Size Improvement. J Drugs Dermatol. 2021;20(1):49–54. doi:10.36849/JDD.5616
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.