Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Free Skin Anterolateral Thigh Flap and Vacuum-Assisted Closure Therapy for Reconstruction of Snakebite-Induced Complex Hand Defects
Authors Nghĩa PT ![]() , Sơn TT, Thúy TTH, Trọng NH, Nam ĐP
, Sơn TT, Thúy TTH, Trọng NH, Nam ĐP ![]()
Received 6 September 2025
Accepted for publication 15 December 2025
Published 26 December 2025 Volume 2025:21 Pages 1847—1853
DOI https://doi.org/10.2147/TCRM.S560853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Phan Tuấn Nghĩa,1– 3 Trần Thiết Sơn,1– 3 Tạ Thị Hồng Thúy,1,2 Nguyễn Hữu Trọng,2 Đặng Phương Nam1,3
1Department of Plastic and Reconstructive Surgery, Hanoi Medical University, Hanoi, Vietnam; 2Department of Plastic Reconstructive and Aesthetic Surgery, Bach Mai Hospital, Hanoi, Vietnam; 3Department of Plastic Reconstructive and Aesthetic Surgery, Vinmec International Hospital, VinUniversity, Hanoi, Vietnam
Correspondence: Phan Tuấn Nghĩa, Department of Plastic and Reconstructive Surgery, Hanoi Medical University, No. 1 Ton That Tung Street, Dong Da District, Hanoi, Vietnam, Tel +84 353057322, Email [email protected]
Introduction: Cobra (Naja species) envenomation in tropical regions like Vietnam frequently leads to severe hand tissue necrosis, creating complex defects that challenge conventional reconstruction. This study evaluates a staged approach combining vacuum-assisted closure (VAC) therapy with free anterolateral thigh (ALT) flap for these challenging injuries.
Methods: Eleven patients with extensive hand defects involving skin and/or tendon due to cobra envenomation were included. Following surgical debridement, VAC therapy was applied to prepare the wound bed. Subsequently, definitive reconstruction was performed using tailored ALT flaps, which included fasciocutaneous or thinned configurations depending on defect complexity. Postoperative evaluation included flap viability, range of motion (ROM), and complication assessment.
Results: The mean duration of VAC therapy was 11.5 ± 4.2 days. Eleven ALT flaps with an average dimension of 14.5× 7.0 cm were harvested. Flap thinning was performed in eight cases (72.7%), achieving a mean final thickness of 4.6 ± 1.3 mm. Eight flaps (72.7%) were used to cover defects spanning both digital and dorsal or palmar subunits. Over a mean follow-up of 15.3 months, patients with digital reconstruction achieved a functional ROM at the metacarpophalangeal joint, with 0° of extension and up to 60° of flexion. The main issue was flap bulkiness; no donor-site morbidity was observed.
Conclusion: A staged approach combining VAC therapy for wound bed preparation and subsequent reconstruction with a free ALT flap is a safe and effective strategy for managing complex hand defects resulting from cobra bites. This method facilitates optimal wound conditions and provides versatile, well-vascularized tissue coverage, thereby promoting functional hand recovery.
Keywords: snakebite, skin necrosis, VAC therapy, ALT flap, hand reconstruction
Introduction
Snakebite envenomation constitutes a significant public health burden in tropical nations, particularly in Vietnam, where bites from cobra (Naja species) are prevalent.1,2 While systemic toxicity from cobra bites may be mild, the resultant local tissue damage is often severe, leading to extensive necrosis and complex sequelae. Soft-tissue necrosis following cobra envenomation is primarily caused by the effects of venom toxins, especially cytotoxins. In addition, secondary infection at the bite site further aggravates the wound.3–5 The hand is one of the most frequently affected anatomical sites. This can result in a spectrum of soft tissue destruction, from superficial necrosis to full-thickness loss involving tendons, bones, and neurovascular structures. Consequently, aggressive surgical debridement is often necessary, creating significant, composite defects that expose vital structures and present formidable challenges for functional and aesthetic reconstruction. Conventional reconstructive options, such as skin grafting or local pedicled flaps, are frequently inadequate for these extensive defects, which are often compromised by poor vascularity at the wound periphery. As a bridge to definitive reconstruction, vacuum-assisted closure (VAC) therapy has emerged as an effective adjunct for wound bed preparation, as it reduces edema and bacterial load while promoting the formation of healthy granulation tissue.6,7 However, durable coverage for large, multi-component hand defects necessitates a reconstructive solution that provides a substantial volume of well-vascularized tissue. The free anterolateral thigh (ALT) flap is an excellent option that fulfills these criteria, offering a large, versatile tissue paddle with a long and reliable vascular pedicle, making it highly suitable for restoring hand form and function.8,9 Therefore, this study aims to present our clinical outcomes using a staged approach that combines VAC therapy for wound bed optimization with subsequent free ALT flap transfer for the reconstruction of complex hand defects secondary to cobra envenomation.
Patient and Method
From January 2020 to April 2025, a total of 214 patients were admitted to our department with cobra envenomation to the hand. The cobra species was identified by snake identification experts or toxicologists based on the snake specimen brought in by the patient or on photographic evidence. Of these, eleven consecutive patients who presented with extensive soft-tissue defects of the hand secondary to cobra envenomation and were subsequently managed with a staged protocol of VAC therapy and free ALT flap reconstruction. The mean patient age was 39.5 ± 15.6 years (range, 21–67), with a male-to-female ratio of 10:1. The mean body mass index (BMI) was 22.8 ± 1.8 kg/m2 (range, 19.8–25.1). Comorbidities like diabetes or hypertension were present in 27.3%. All eleven patients received antivenom serum upon ICU admission. Surgical debridement followed by full antivenom dose, with wound cultures and broad-spectrum IV antibiotics. Post-debridement, patients underwent VAC therapy for 1–2 weeks to control infection, reduce edema, and promote granulation for wound closure.
Surgical Technique
All patients initially underwent aggressive surgical debridement of all necrotic tissue. Following debridement, the VAC system (KCI, an Acelity company, USA) was applied to the wound bed using a polyurethane foam dressing under a continuous negative pressure of 125 mmHg. Dressings were changed every three to four days. VAC therapy was continued until the wound bed was deemed suitable for definitive coverage, characterized by the absence of infection and the presence of healthy granulation tissue. Definitive reconstruction was performed using a free ALT flap harvested from the contralateral thigh. Perforator vessels were identified preoperatively with a handheld Doppler probe. The flap was designed to match the dimensions and contour of the defect. The incision was made from the medial edge of the skin flap down to the subfascial plane. Dissection was then carried out within the subfascial plane until the descending branch or oblique branch of the lateral circumflex femoral artery (LCFA) and its perforators were identified. The flap was configured as either a standard fasciocutaneous flap or was thinned intraoperatively. The recipient vessels, most often the radial artery with its venae comitantes or superficial veins, were chosen. The skin paddles were carefully positioned to match the defect layout. The reconstructed hand was immobilized in a plaster cast in a functional position to prevent tension on the vascular anastomosis or tendon repair sites. Passive range of motion (ROM) exercises were initiated after one week, followed by gradual introduction of active movements starting from the third postoperative week. Patients were followed postoperatively for 6 months to 2 years. Functional outcomes were assessed using range of wrist joint motion (ROM) for dorsal or palmar injuries, and range of metacarpophalangeal joint motion were evaluated for digital reconstructions, beginning at 3 months after surgery.
Results
The average time from snakebite to hospital admission and administration of antivenom serum was 11.8 ± 7.7 hours (range: 2–30 hours). The bite locations varied: five patients were bitten on the fingers, three on the dorsum of the hand, and three on both the dorsum and fingers. Cutaneous necrosis was observed in all patients within the first 48 hours. All patients underwent surgical debridement shortly after completing antivenom therapy, followed by VAC therapy for a mean of 11.5 ± 4.2 days (range: 6–16 days). Wound cultures were positive in nine of 11 patients, with Enterococcus faecalis being the most common isolate (five cases). All patients had significant defects, with eight patients (72.7%) having combined digital and dorsal or palmar defects. One case involved defects of the dorsum and palm; Two patients had an isolated dorsal defect. Regarding defect depth, five cases (45.5%) involved exposed tendons, five hands (45.5%) had a combined loss of skin and tendons, and one case (9.1%) presented with bone exposure.
Following successful wound bed preparation, a total of 11 free ALT flaps were transferred. The mean flap dimension was 14.5 ± 3.0 cm in length (11–22 cm) and 7.0 ± 1.6 cm in width (5–11 cm). The mean number of perforators was 1.4 (range: 1–3), with an average pedicle length of 12.7 ± 2.4 cm (10–17 cm). Flap thinning was selectively performed: four flaps (36.4%) underwent microdissection thinning, four flaps (36.4%) underwent primary thinning, and three flaps (27.3%) were harvested as a fasciocutaneous flap. Pre-thinned flap thickness was 15.4 ± 3.6 mm (10–18 mm), reduced to 4.6 ± 1.3 mm (3–7 mm) after thinning. All flaps were anastomosed to the radial artery. All cases used the radial vein as the recipient vein. Donor sites were closed primarily in 10 cases (90.9%), and one case required a split-thickness skin graft. Detailed patient characteristics and results are summarized in Table 1. All flaps survived completely, and no donor-site complications occurred. The average hospital stay was 35.1 ± 6.3 days (23–43 days), and the mean follow-up was 15.3 ± 6.0 months (3–20 months). Five patients experienced bulkiness of the flap. Among nine patients with digital injuries, the range of motion at the metacarpophalangeal (MP) joint reached 0° extension and at least 60° flexion. The remaining two patients, who had dorsal hand defects without digital involvement, achieved at least wrist range of motion of 40° in extension and 50° in flexion. Patient results are shown in Figures 1 and 2.
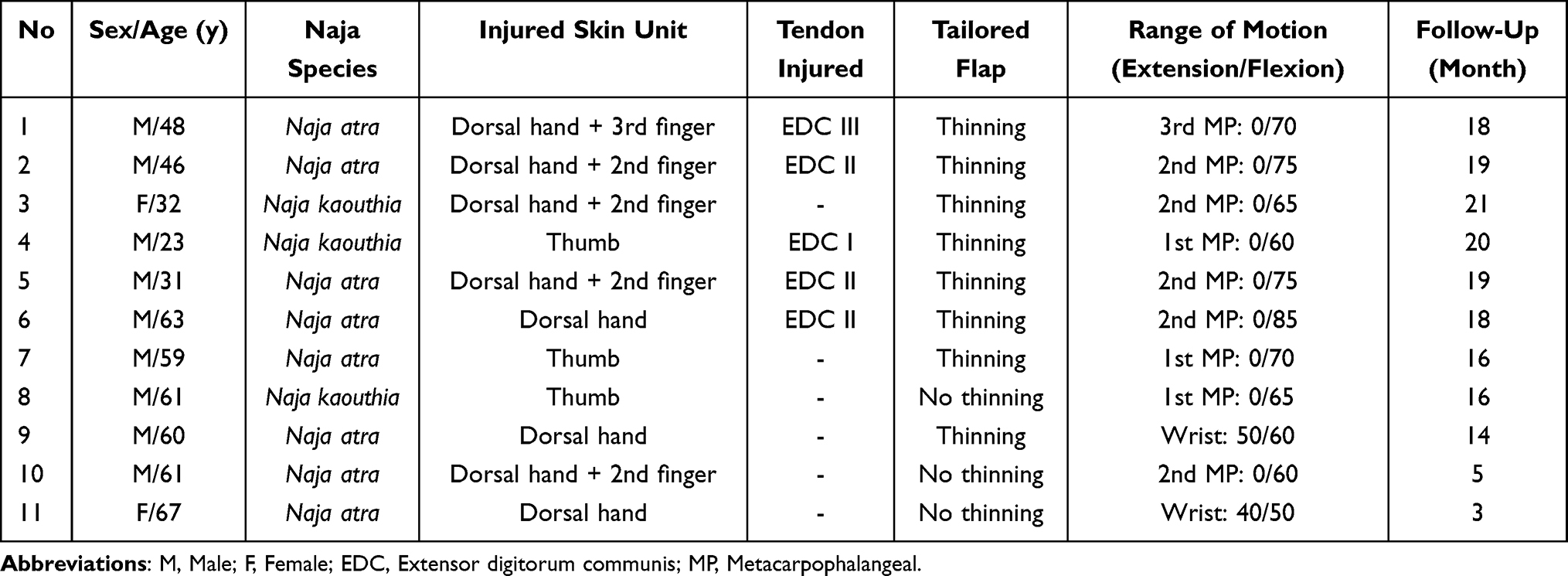 |
Table 1 Patient Data |
 |
Figure 1 Reconstructive sequence for a 61-year-old male following envenomation by Naja atra. (A) Initial clinical presentation demonstrating extensive cutaneous necrosis on the dorsum of the hand. (B) The resultant soft-tissue defect after surgical debridement. (C) A harvested ALT fasciocutaneous flap before transfer. (D) Immediate postoperative appearance of the reconstructed hand. (E and F) Anterior and oblique views at 2 months postoperatively, showing stable coverage and satisfactory contour. |
 |
Figure 2 Staged reconstruction in a 63-year-old male with a dorsal hand injury from a Naja atra bite. (A) Exposed necrotic fascia and subcutaneous tissue following initial injury. (B) Appearance of a healthy granulation bed after a 7-day course of negative pressure wound therapy (NPWT). (C) The ALT flap is undergoing primary thinning intraoperatively to match the defect’s requirements. (D) Immediate postoperative result after flap inset and microvascular anastomosis. (E and F) Final clinical outcome at the 4-month follow-up, demonstrating excellent aesthetic integration and preserved hand architecture. |
Discussion
Snakebite envenomation presents a uniquely challenging clinical scenario, particularly in tropical nations like Vietnam, where cobra (Naja species) bites are prevalent. Injuries to the upper limb, with the hand being the most commonly affected site, constitute a significant proportion of these cases.10–12 Extensive local tissue destruction can evolve over several days, frequently necessitating aggressive surgical debridement.4,13 This multi-layered tissue damage is a primary contributor to the complexity of reconstruction and underscores why long-term functional recovery is often more challenging compared to that of other etiologies. As supported by literature, wide excision and thorough debridement can substantially reduce the toxin load, limit the extent of necrosis, and promote a healthier wound healing environment.14 The extensive removal of necrotic skin and fascia, however, often results in the exposure of critical underlying structures such as tendons, joints, or bone. In our series, the majority of patients underwent their initial debridement 5–7 days post-envenomation. Secondary infection was a common clinical finding and played a significant role in wound progression and further tissue destruction, occurring in the majority of our patients (81.8%). A key pathological feature of cobra envenomation is central fascial and adipose tissue necrosis, particularly in bites to the dorsum of the hand—a phenomenon we have previously reported.15 Tissue necrosis created reconstructive challenges, as the hand’s function and aesthetics depend on preserving tendon gliding, joint movement, and finger shape.
VAC therapy constituted a pivotal component of the reconstructive strategy for these complex hand injuries.16,17 This modality has demonstrated significant efficacy in the management of venomous snakebite injuries. Beyond its established benefits in hand reconstruction—namely, the reduction of microbial load, promotion of granulation tissue, and demarcation of viable tissue planes—VAC therapy has been reported to specifically mitigate edema, accelerate wound healing, and limit the propagation of tissue necrosis in envenomated patients. Furthermore, its application has been correlated with reduced hospital stays, thereby facilitating subsequent definitive procedures such as free flap transfer.6,7 Following this evidence, all defects in our patient were managed with VAC therapy following initial debridement and before definitive reconstruction. This standardized approach yielded favorable results, with no instances of postoperative flap infection or wound dehiscence observed.
The free anterolateral thigh (ALT) flap demonstrated exceptional utility in these reconstructions, attributable to its inherent versatility, consistent vascular anatomy, and the generous dimensions of the available skin paddle.18 The favorable tissue characteristics and surgical adaptability of the ALT flap render it particularly advantageous for the complex demands of hand reconstruction.19–21 In our series, the flap was employed in several configurations: standard fasciocutaneous flaps were utilized for defects requiring robust coverage, whereas selectively thinned flaps were preferred for resurfacing the hand dorsum and digits to optimize contour and function. However, the thinning procedure necessitates meticulous technique, as excessive dissection around the perforator vessels can compromise flap perfusion and elevate the risk of partial necrosis.22–24 Conversely, for pressure-bearing zones such as the palmar surface and thenar eminence, a full-thickness fasciocutaneous configuration was intentionally preserved to ensure adequate durability. While not traditionally considered the primary choice for hand dorsum coverage due to its potential bulk, the ALT flap distinguishes itself as a superior option for extensive, multi-component defects precisely because this thickness can be addressed. The ability to perform primary thinning allows a large, well-vascularized flap to be tailored for areas requiring a thin, pliable tissue interface. Furthermore, the long vascular pedicle of the ALT flap is a critical advantage in the post-envenomation setting, where the local vasculature is often compromised by venom-induced thrombosis, rendering it unsuitable for anastomosis. This permitted the selection of reliable recipient vessels outside the zone of injury, such as the radial artery at the wrist. Therefore, this requires a material with a sufficiently long and reliable vascular pedicle, which is also an advantage over other microsurgical flaps. Beyond the immediate challenge of soft-tissue reconstruction, the formidable musculoskeletal sequelae of envenomation—including joint stiffness, tendon adhesions, and bone pathology—posed significant obstacles to restoring a full range of motion and functional capacity.25 In select cases, a decision was made to preserve functionally compromised, yet anatomically intact, hand units rather than proceed with amputation. This approach, which prioritizes aesthetic integrity and psychological well-being at the expense of optimal function, illustrates a fundamental principle in reconstructive surgery: the careful balancing of functional goals with aesthetic outcomes, particularly in the context of snakebite injuries where the true extent of tissue damage is often initially underestimated.
This study is subject to several limitations. First, the absence of a control group—such as a cohort with traumatic or thermal burn-related hand defects—precludes a direct comparative analysis of outcomes across different etiologies. Second, the modest number of patients who met the criteria for ALT flap reconstruction may limit the generalizability of our findings to a broader population. Finally, the comprehensive assessment of long-term functional outcomes within this patient population remains a significant challenge. Although the follow-up period extended to 12 months for most patients, a more prolonged observational period may be necessary to fully capture the recovery of fine dexterity and complete reintegration into activities of daily living. The progressive nature of post-envenomation sequelae, particularly tendon adhesions and joint stiffness, warrants further investigation with long-term follow-up to delineate the complete functional recovery trajectory.
Conclusion
For complex hand defects caused by snakebite, combining VAC therapy as a preparatory step with ALT flap reconstruction offers a reliable and effective approach. VAC therapy improves the wound environment by managing infection and defining the extent of damage, while the ALT flap provides versatile coverage adapted to multi-component tissue loss.
This study establishes that a staged protocol, integrating VAC. therapy for wound bed optimization with subsequent free ALT flap transfer, constitutes a superior and highly reliable strategy for reconstructing complex hand defects from snakebite envenomation.
Declaration of Patient Consent
All participants provided written informed consent before enrolment in the study. The privacy and confidentiality of patient records were adhered to in managing the clinical information in conducting this research.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. This study was approved by our institution’s Research Ethics Committee (Bach Mai Hospital, Ref: 61/BM-HĐĐĐ).
Consent to Publish
The authors affirm that human research participants provided informed consent to publish the images in the Figures.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Blessmann J, Nguyen TPN, Bui TPA, Krumkamp R, Vo VT, Nguyen HL. Incidence of snakebites in 3 different geographic regions in Thua Thien Hue province, central Vietnam: green pit vipers and cobras cause the majority of bites. Toxicon. 2018;156:61–65. doi:10.1016/j.toxicon.2018.11.009
2. Ngo ND, Le QX, Pham AQ, et al. Clinical features, bacteriology, and antibiotic treatment among patients with presumed Naja Bites in Vietnam. Wilderness Environ Med. 2020;31(2):151–156. doi:10.1016/j.wem.2020.01.002
3. Ho C-H, Chiang L-C, Mao Y-C, et al. Analysis of the necrosis-inducing components of the venom of Naja atra and assessment of the neutralization ability of freeze-dried antivenom. Toxins. 2021;13(9):619. doi:10.3390/toxins13090619
4. Lai C-S, Liu P-Y, Lee C-H, et al. The development of a surgical risk score and evaluation of necrotizing soft tissue infection in 161 Naja atra envenomed patients. PLoS Negl Trop Dis. 2022;16(2):e0010066. doi:10.1371/journal.pntd.0010066
5. Mao Y-C, Liu P-Y, Chiang L-C, et al. Naja atra snakebite in Taiwan. Clin Toxicol. 2018;56(4):273–280. doi:10.1080/15563650.2017.1366502
6. Kim KJ, Min JH, Yoo I, et al. Negative pressure wound therapy for skin necrosis prevention after snakebite in the emergency department: a retrospective cohort study. Medicine. 2021;100(3):e24290. doi:10.1097/MD.0000000000024290
7. Lu H-Y, Mao Y-C, Liu P-Y, et al. Clinical predictors of early surgical intervention in patients with venomous snakebites. Eur J Med Res. 2023;28(1):131. doi:10.1186/s40001-023-01101-x
8. Lee YJ, Kim J, Lee CR, et al. Anterolateral thigh chimeric flap: an alternative reconstructive option to free flaps for large soft tissue defects. J Clin Med. 2023;12(21):6723. doi:10.3390/jcm12216723
9. Coquillard CL, Bai J, Ko JH. Thin and thinned anterolateral thigh flaps for upper extremity reconstruction. Hand Clinics. 2024;40(2):199–208. doi:10.1016/j.hcl.2023.12.001
10. Patikorn C, Blessmann J, Nwe MT, et al. Estimating economic and disease burden of snakebite in ASEAN countries using a decision analytic model. PLoS Negl Trop Dis. 2022;16(9):e0010775. doi:10.1371/journal.pntd.0010775
11. Patra A, Mukherjee AK. Assessment of snakebite burdens, clinical features of envenomation, and strategies to improve snakebite management in Vietnam. Acta Trop. 2021;216:105833. doi:10.1016/j.actatropica.2021.105833
12. Herzel BJ, Samuel SP, Bulfone TC, Raj CS, Lewin M, Kahn JG. Snakebite: an exploratory cost-effectiveness analysis of adjunct treatment strategies. Am J Trop Med Hyg. 2018;99(2):404–412. doi:10.4269/ajtmh.17-0922
13. Liu -C-C, Chou Y-S, Chen C-Y, et al. Pathogenesis of local necrosis induced by Naja atra venom: assessment of the neutralization ability of Taiwanese freeze-dried neurotoxic antivenom in animal models. PLoS Negl Trop Dis. 2020;14(2):e0008054. doi:10.1371/journal.pntd.0008054
14. Lin J-H, Sung W-C, Mu H-W, Hung D-Z. Local cytotoxic effects in cobra envenoming: a pilot study. Toxins. 2022;14(2):122. doi:10.3390/toxins14020122
15. Nam ĐP, Thuận LQ, Quang TD, Nghĩa PT, Sơn TT. The clinical significance and management of finger necrosis due to cobra bite in Vietnam. JPRAS Open. 2025;45:159–169. doi:10.1016/j.jpra.2025.05.011
16. Shim HS, Choi JS, Kim SW. A role for postoperative negative pressure wound therapy in multitissue hand injuries. BioMed Res Int. 2018;2018:1–7. doi:10.1155/2018/3629643
17. Wang L, Liu H, Ma T, Wu X, Zhang L. Reconstruction of soft tissue defects in the hand with a free anterolateral thigh deep fascia flap. Orthop Surg. 2021;13(3):758–767. doi:10.1111/os.12948
18. Agostini T, Russo GL, Zhang YX, Spinelli G, Lazzeri D. Adipofascial anterolateral thigh flap safety: applications and complications. Arch Plast Surg. 2013;40(02):91–96. doi:10.5999/aps.2013.40.2.91
19. Mekky M. Versatility of anterolateral thigh flap in dorsal hand reconstruction. Egypt J Plast Reconstr Surg. 2018;42:311–315. doi:10.21608/ejprs.2018.79717
20. Suondoh MS, Sulaiman WAW, Ismail WFW, Saad AZM. One stage microsurgical reconstruction with chimeric flap for salvaging a complex hand injuries. Arch Hand Microsurg. 2020;25(2):156–160. doi:10.12790/ahm.20.0007
21. Meky M, Safoury Y. Composite anterolateral thigh perforator flaps in the management of complex hand injuries. J Hand Surg Eur Vol. 2013;38(4):366–370. doi:10.1177/1753193411427648
22. Agostini T, Lazzeri D, Spinelli G. Anterolateral thigh flap thinning: techniques and complications. Ann Plast Surg. 2014;72(2):246–252. doi:10.1097/SAP.0b013e31825b3d3a
23. Alkureishi LWT, Shaw-Dunn J, Ross GL. Effects of thinning the anterolateral thigh flap on the blood supply to the skin. Br J Plast Surg. 2003;56(4):401–408. doi:10.1016/S0007-1226(03)00125-5
24. Torres-Ortíz Zermeño CA, López Mendoza J. Aesthetic and functional outcomes of the innervated and thinned anterolateral thigh flap in reconstruction of upper limb defects. Plast Surg Int. 2014;2014:1–7. doi:10.1155/2014/489012
25. Jayawardana S, Gnanathasan A, Arambepola C, Chang T. Chronic musculoskeletal disabilities following snake envenoming in Sri Lanka: a population-based study. PLoS Negl Trop Dis. 2016;10(11):e0005103. doi:10.1371/journal.pntd.0005103
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.