Back to Journals » Clinical Ophthalmology » Volume 17
Fraud Claims Filed Involving Practicing Ophthalmologists from 1985 Through 2020
Authors Sharma M ![]() , Watane A, Cavuoto KM, Parikh R, Sridhar J
, Watane A, Cavuoto KM, Parikh R, Sridhar J
Received 10 November 2022
Accepted for publication 19 December 2022
Published 24 January 2023 Volume 2023:17 Pages 341—350
DOI https://doi.org/10.2147/OPTH.S397014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Meghan Sharma,1 Arjun Watane,2 Kara M Cavuoto,1 Ravi Parikh,3,4 Jayanth Sridhar1
1Department of Ophthalmology, Bascom Palmer Eye Institute, Miami, FL, USA; 2Department of Ophthalmology, Yale Eye Center, New Haven, CT, USA; 3Department of Ophthalmology, Manhattan Retina and Eye Consultants, New York, NY, USA; 4Department of Ophthalmology, New York University Grossman School of Medicine, New York, NY, USA
Correspondence: Jayanth Sridhar, Department of Ophthalmology, Bascom Palmer Eye Institute, 900 NW 17th Street, Room 271, Miami, FL, 33136, USA, Tel +1 305-326-6124, Fax +1 305-326-6417, Email [email protected]
Introduction: Like all United States physicians, ophthalmologists may be implicated in lawsuits claiming fraudulent medical practice. In order to educate, raise awareness, and mitigate fraudulent practice, we reviewed a legal database and analyzed fraud claims in ophthalmology lawsuits.
Methods: A retrospective legal literature review was performed on jury verdicts and settlements from the online legal database LexisNexis Academic from 1985 through 2020 that were filed by or against an ophthalmologist, involved a fraud claim, and included a final decision or settlement. Cases were evaluated for factors including demographics of plaintiffs and defendants, type of fraud claim, ophthalmologist party status (plaintiff or defendant), decision outcome, and amount awarded (when applicable).
Results: Of the 27 cases analyzed, all ophthalmologist defendants involved were male and the most common sub-specialty for an ophthalmologist defendant was refractive surgery. The most common fraud type was a fraud claim involving a malpractice lawsuit (12 of 27), followed by contract fraud and billing fraud. While the ophthalmologists in malpractice-related fraud cases experienced more rulings in favor of the defendant on the fraud claims (8 of 12), ophthalmologists in billing fraud cases experienced fewer rulings in their favor (0 of 5).
Discussion: Ophthalmology lawsuits involving fraud claims occurred in various settings, including malpractice lawsuits, contract cases, and Medicare and Medicaid billing. Defendants were all male and most commonly refractive surgeons.
Keywords: ophthalmology fraud, legal ophthalmology, fraud, medical fraud, medicolegal issues, legal medicine
Introduction
Like all United States physicians, ophthalmologists may be implicated in lawsuits claiming fraudulent medical practice. Fraud, the practice of making a false or misrepresented claim, is an issue contributing to inefficiencies, high healthcare costs, and waste in the practice of medicine.1,2 Fraudulent activity contributes to 3–10% of total health spending and more than $100 billion annually.2 The fight against fraud is costly as well — from 2011 to 2020, the federal government allotted $350 million to fighting Medicare fraud.3 While physicians may not intentionally commit fraud, studies show nearly all physicians will contribute to improper payments at some point in their careers.4 Thus, it is important to increase physician education and awareness on how to avoid fraudulent activity, such as improper billing, in order to reduce an individual physician’s risk of being implicated in a fraud lawsuit and to decrease systemic cost burden.
Chen et al previously examined the characteristics of physicians from all specialties who were excluded from US Medicare and state public programs for fraud, health crimes, or unlawful prescribing of controlled substances.5 Excluded physicians tended to be older, male, and/or osteopathic physicians. The most common specialties were family medicine, psychiatry, internal medicine, anesthesiology, surgery, and obstetrics/gynecology. However, little information regarding ophthalmology has been reported. Further analysis of fraud litigation in ophthalmology can allow for education, awareness, and mitigation of fraudulent practice.
Methods
The research adhered to the tenets of the Declaration of Helsinki, and the University of Miami Institutional Review Board approval was waived, as all data was publicly available. The LexisNexis Academic legal database was accessed using an institutional subscription to review state and federal case records from across the US. This database only contains cases filed at the state and federal level. Cases that were handled by a third-party arbitration or appealed at the district level were not included.6 On August 26, 2021 the database for US cases that were filed from January 1, 1985 to December 31, 2020 at the federal and state levels was queried using the following Boolean search term logic: (ophthalm* AND (fraud* OR extortion OR deceit)). The results were further filtered to only include those cases which had jury verdicts or settlements. Cases that were filed by or against an ophthalmologist, involved a claim involving fraud, and included a final decision or settlement were included in the analysis.
The included cases were evaluated for plaintiff gender, defendant gender, subspecialty of the ophthalmologist, age of the ophthalmologist at time of case (calculated using current age and year of the case), whether the ophthalmologist was the plaintiff or the defendant, US state involved in the claim, decision outcome, the amount won (if applicable), and the type of fraud. If demographic information could not be obtained on LexisNexis, a Google search was performed to attempt to find missing data. Type of fraud was categorized as follows: a fraud claim included in an ophthalmology malpractice case (“malpractice fraud”), a fraud claim regarding a contract with a company (“contract fraud”), a Medicare or Medicaid fraud claim (“billing fraud”), a fraud claim included in an employment harassment or wrongful termination case (“employment harassment and fraud”), a fraud claim among members of the same business or practice (“business fraud”), deception and fraud that occurred during an ophthalmology-related trial (“fraud during trial”), and fraud that occurred as a result of a company performing bribery (“kickback scheme fraud”).
Descriptive analyses were performed in order to evaluate factors including demographics of plaintiffs and defendants, type of fraud claim, ophthalmologist party status (plaintiff or defendant), decision outcome, and amount awarded (when applicable).
Results
A total of 100 cases were returned by the initial search query. Of these 100 cases, 49 were excluded because neither party was an ophthalmologist, 13 were repeated cases, 6 involved no fraud claim, and 5 did not provide enough information. As such, a total of 27 cases were included in the analysis (Table 1). Thirteen of the cases were ruled in favor of the plaintiff, five cases reached a settlement, and nine of the cases were ruled in favor of the defendant.
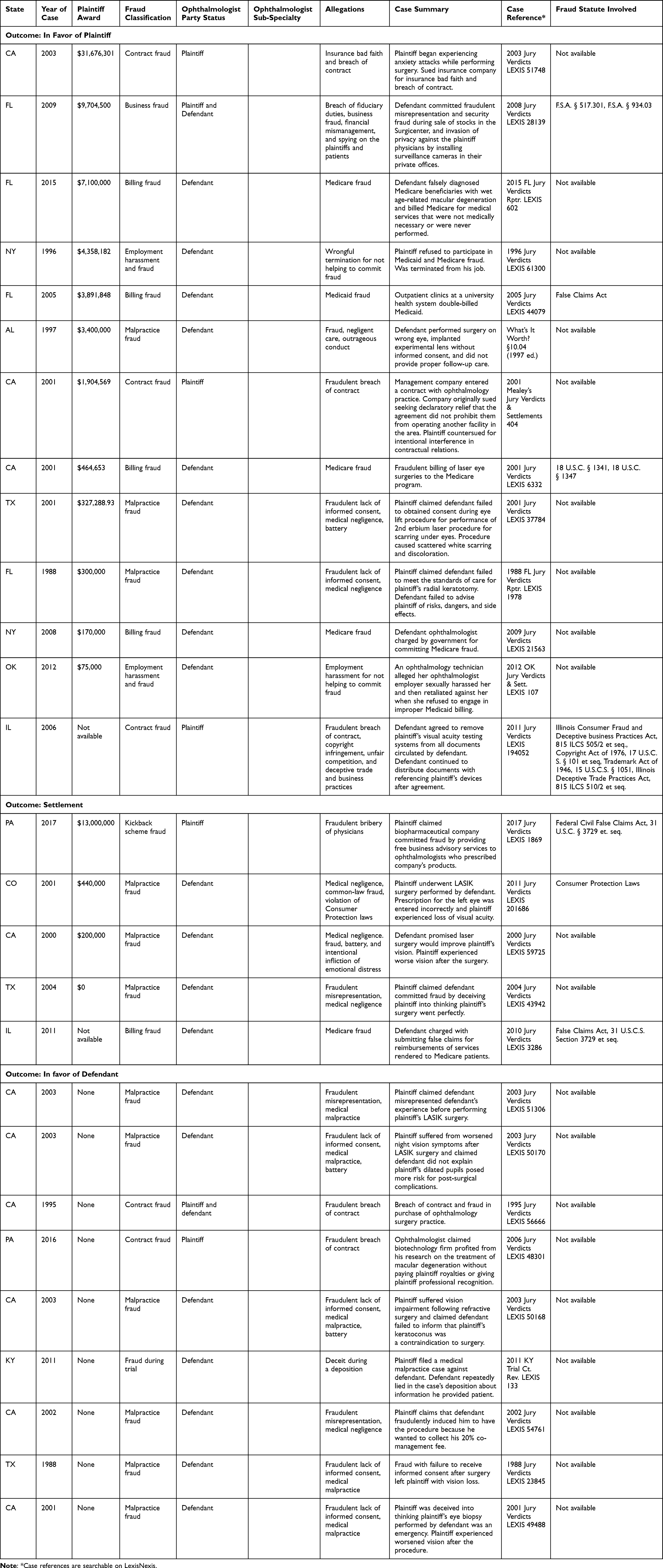 |
Table 1 Case Descriptions of Fraud in Ophthalmology Legal Cases 1985 through 2020 |
Case demographics are shown in Table 2. Among all 27 cases, there were 31 ophthalmologists involved. Ten ophthalmologists were plaintiffs with a median age of 48.5 years (IQR 42.5–56.5) during time of the case and 2 ages unknown. Twenty-one ophthalmologists were defendants with a median age of 53 years (IQR 44–58) and 8 unknown ages. All ophthalmologist defendants were male, and the most common specialty for an ophthalmologist defendant was refractive surgery.
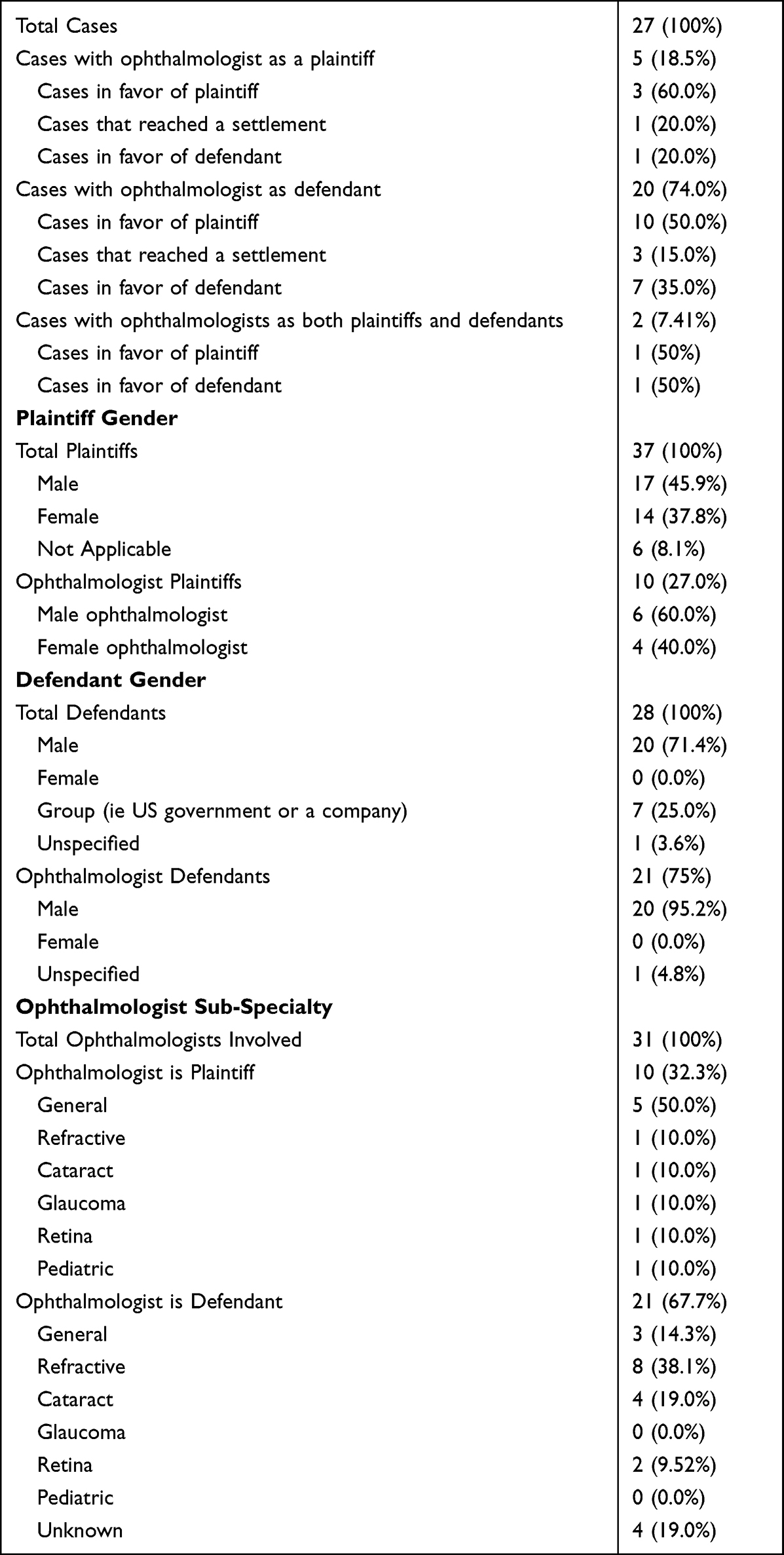 |
Table 2 Characteristics of Cases |
Litigation outcomes were collected (Table 3). The median payout for cases that were ruled in favor of the plaintiff was $2,652,285 (IQR $313,644-$5,729,091). Three of these cases noted prison sentences of 21 months, 60 months, and 10 years. The median settlement payout was $320,000 (IQR $100,000-$6,720,000) with no prison sentences.
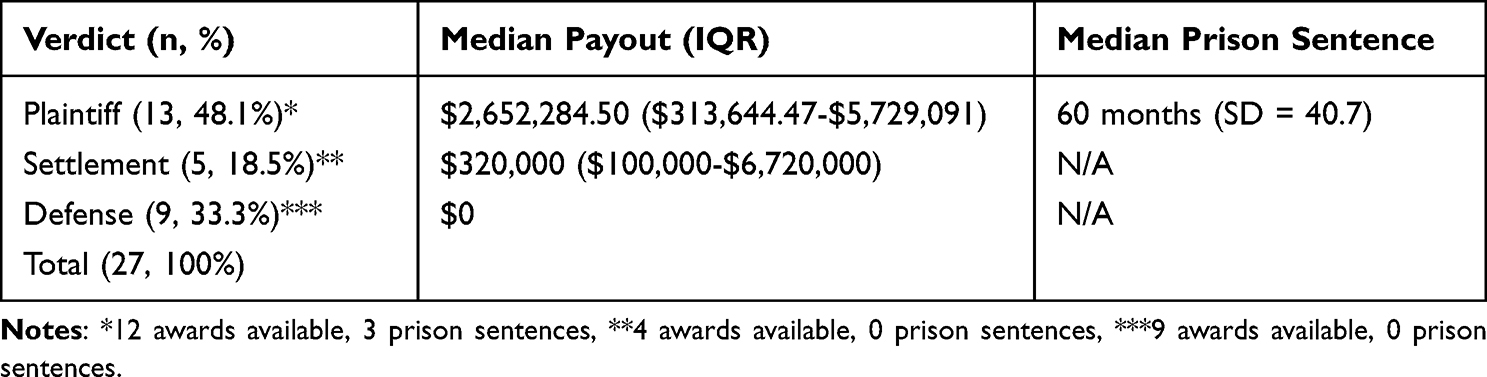 |
Table 3 Litigation Outcomes |
Of the 13 cases ruled in favor of the plaintiff, 3 were malpractice fraud, 3 were contract fraud, 4 were billing fraud, 2 were employment harassment and fraud, and 1 was business fraud (Table 4). Of the 5 cases that reached a settlement, 3 were malpractice fraud, 1 was billing fraud, and 1 was kickback scheme fraud. Of the 9 cases ruled in favor of the defendant, 6 were malpractice fraud, 2 were contract fraud, and 1 was fraud during a trial.
 |
Table 4 Fraud Classification |
Discussion
There is a literature gap regarding fraud in ophthalmology. While there is no standard on how to classify fraud, a 2015 study on fraud in medicine identified 18 fraud types, including providing unnecessary care and phantom billing (a process in which a physician bills for services not performed)1,7 The examples of fraud seen in this study show the broad scope of medical fraud claims that can be made and how ophthalmologists may experience a fraud claim in a variety of settings.
Of the cases analyzed, the most common type of fraud was malpractice fraud. Nevertheless, most of these malpractice fraud claims were not ruled in favor of the plaintiff, with 6 of 12 ruling in favor of the defendant entirely and another 2 cases ruling in favor of the defendant on the fraud claim but not the malpractice claim. Literature shows that most malpractice lawsuits are unsuccessful, correlating with the finding that most malpractice-related fraud claims were unsuccessful in this study.8 A possible explanation for this finding may be that the fraud claims in these cases were secondary to malpractice claims, thus warranting less attention. Many of the malpractice-related fraud cases in the current study also did not mention a clear violation of fraud legislation.
Generally, medical fraud cases claim that there is a violation of 1 of 3 statutes: the False Claims Act of 1863, the Anti-Kickback Statute of 1982, or the Stark Law of 1989. The False Claims Act imposes civil liability on any person who submits a false or fraudulent claim to the federal government for payment or approval.1 The act also allows whistleblowers to act on behalf of the government’s behalf to identify fraud and collect compensation.9 Of all the cases in the current study that mentioned fraud legislation, the False Claims Act was the most cited statute. The Anti-Kickback Statute prohibits anyone from receiving payment for making a referral to a federally reimbursed healthcare program. Kickbacks schemes were not commonly seen in this study, as only one case involved a biopharmaceutical company providing free business advisory services to ophthalmologists who prescribed the company’s products. The final law of the three is the Physician Self-Referral (Stark) Law, which prohibits physicians from making referrals to certain designated health services paid for by Medicare of Medicaid if the physician, or an immediate family member, has a financial relationship with the entity.1 None of the malpractice-related fraud lawsuits that were ruled in favor of the ophthalmologist cited a clear violation of a fraud statute; however, it is important to note that this study did not find clear citations of fraud claims in most of the malpractice-related fraud lawsuits included in the study, regardless of final outcome.
While defending ophthalmologists in this study were more likely to succeed on malpractice-related fraud claims, they experienced less success as defendants on billing claims fraud. Some of these billing fraud lawsuits cited the False Claims Act or other related legislation. One case that cited a violation of the False Claims Act involved double-billing of services to Medicaid. Another case cited a violation of the False Claims Act because the defending ophthalmologist made false claims for reimbursements of services rendered to Medicare patients. Both cases were ruled against the defendant ophthalmologist. A possible explanation for why these billing fraud cases were often ruled against the defendant may be the specificity of the False Claims Act against fraudulent actions including double billing or falsified claims. The plaintiff in these cases is also typically the United States government, which may make it harder for the defendant to obtain success with his or her case. Moreover, criminal charges may be included in these cases, as at least 3 of the 5 billing fraud cases included prison sentences.
Although few of the billing fraud cases resulted in prison sentences, the majority of the cases won by plaintiffs included a significant financial award. The case with the largest financial award ($31,676,301) was a contract fraud case in which the plaintiff sued an insurance company for insurance breach of contract after claiming he was experiencing anxiety attacks from performing surgeries, but the insurance company claimed he was not disabled from performing the surgeries. Other cases with the largest settlements included a kickback scheme, a business fraud case, a billing fraud, and an employment harassment and fraud case, indicating no notable association between fraud type and award amount. Of note, the decision to pursue the case in court or reach a settlement can also impact the amount of the financial award. The median payout for court cases won by the plaintiff was over 8 times greater than the median payout for cases that reached a settlement. Both jail sentences and financial losses can have a significant financial and emotional impact on the parties involved and highlight the importance of physician education on avoiding fraud lawsuits.8
While the malpractice-related fraud cases typically included the ophthalmologists as the defendants, ophthalmologists were also seen as plaintiffs in other types of fraud lawsuits, particularly contract fraud cases. These were cases in which the physician posited that there was a breach of contract with a company or other colleagues. Males were more likely to be sued than females, with all defendants being male. This finding coincides with the findings of the 2018 study by Chen et al, which found that physicians who were excluded from Medicare and state public programs due to fraud were commonly male physicians.5 Moreover, a retrospective, cohort study of 2251 malpractice claims reported to the Ophthalmic Mutual Insurance Company from 1990 to 2008 found that men were sued 54% more often than females over the period studied, indicating a prevalence of claims against men in not only medical fraud, as observed in this study, but also medical malpractice.10
A future study could investigate whether lawsuits in ophthalmology under the False Claims Act are associated with future reductions in fraudulent activity, such as providing unnecessary procedures or overbilling. A 2020 study by Howard and Desai performed a similar analysis in cardiology by examining cases in which hospitals were investigated under the False Claims Act for billing Medicare for unnecessary percutaneous coronary interventions (PCI) in order to assess the association between these investigations and PCI volumes. The study found that procedure volume declined at the hospitals under investigated by the False Claims Act upon initiation of the investigations, but it also stated that other factors may have been at play in this decline in procedure volume.11 In order to analyze the association between cases under the False Claims Act and reduction in fraudulent activity in ophthalmology, a more extensive review of cases involving the False Claims Act should be performed, perhaps by using multiple legal databases.
There were several limitations in this study. The number of cases was limited, as many cases queried in the search did not pertain to fraud litigation involving an ophthalmologist. The search strategy was also limited since only one database was used.12 Further, the database used typically provided summaries of the cases instead of the full text of the case, potentially limiting the amount of information obtained on each case. Since many of the cases were not provided in full text, it was difficult to confirm that the fraud claim did not include a statute or jail sentence, for instance. Additionally, not all plaintiff awards were provided, limiting the analysis of median payouts. Finally, details regarding the ages and specialties of the involved ophthalmologists were commonly found via Internet searches, which may limit their reliability.
In conclusion, fraud lawsuits can be seen in all fields of medicine, including ophthalmology, and can have a significant financial and emotional burden on a physician. Even if unintentional, almost all physicians will contribute to improper billing at some point in their careers.4 This emphasizes the importance of physician education on best practices for submitting appropriate claims, properly documenting information in medical records, and creating and executing contracts.
Funding
Supported by NIH Center Core Grant P30EY014801, Research to Prevent Blindness Unrestricted Grant.
Disclosure
Dr Parikh is advisory board for Apellis and reports consulting for Anthem Blue Cross Blue Shield, outside the submitted work. Dr. Sridhar is a consultant for Alcon, Allergan, Apellis, Dorc, Genentech, and Regeneron. The authors report no other conflicts of interest in this work.
References
1. Chen ZX, Hohmann L, Banjara B, et al. Recommendations to protect patients and health care practices from medicare and medicaid fraud. J Am Pharm Assoc. 2020;60(6):e60–e65. doi:10.1016/j.japh.2020.05.011
2. Drabiak K, Wolfson J. What should health care organizations do to reduce billing fraud and abuse? AMA J Ethics. 2020;22(3):E221–E231.
3. McGee J, Sandridge L, Treadway C, et al. Strategies for fighting medicare fraud. Health Care Manag. 2018;37(2):147–154. doi:10.1097/HCM.0000000000000204
4. Agrawal S, Tarzy B, Hunt L, et al. Expanding physician education in health care fraud and program integrity. Acad Med. 2013;88(8):1081–1087. doi:10.1097/ACM.0b013e318299f5cf
5. Chen A, Blumenthal DM, Jena AB. Characteristics of physicians excluded from us medicare and state public insurance programs for fraud, health crimes, or unlawful prescribing of controlled substances. JAMA Netw Open. 2018;1(8):e185805. doi:10.1001/jamanetworkopen.2018.5805
6. LexisNexis. LexisNexis Academic User Guide. LexisNexis: LexisNexis; 2020.
7. Dallas thornton MB, Amrit C, Aly R. Categorizing and describing the types of fraud in healthcare. Procedia Comput Sci. 2015;64:713.
8. Reddy AK, Engelhard SB, Shah CT, et al. Medical malpractice in uveitis: a review of clinical entities and outcomes. Ocul Immunol Inflamm. 2018;26(2):242–248. doi:10.1080/09273948.2016.1202289
9. Vogel RL. The false claims act and its impact on medical practices. J Med Pract Manage. 2010;26(1):21–24.
10. Fountain TR. Ophthalmic malpractice and physician gender: a claims data analysis (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2014;112:38–49.
11. Howard DH, Desai NR. US false claims act investigations of unnecessary percutaneous coronary interventions. JAMA Intern Med. 2020;180(11):1534–1536. doi:10.1001/jamainternmed.2020.2812
12. Hill C, Hunter A, Johnson L, et al. Medicare fraud in the United States: can it ever be stopped? Health Care Manag. 2014;33(3):254–260. doi:10.1097/HCM.0000000000000019
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.