Back to Journals » Clinical Interventions in Aging » Volume 20
Frailty as a Predictor of Falls in Older Adults with Type 2 Diabetes: Evidence from Vietnam
Authors Dinh HT ![]() , Ha LVH
, Ha LVH ![]() , Luu NM, Do TTT, Nguyen TTH
, Luu NM, Do TTT, Nguyen TTH ![]() , Nguyen TX
, Nguyen TX ![]() , Nguyen AT
, Nguyen AT ![]() , Nguyen AL, Nguyen HTT
, Nguyen AL, Nguyen HTT ![]() , Phan HH, Nguyen TN, Vu HTT
, Phan HH, Nguyen TN, Vu HTT ![]()
Received 15 August 2025
Accepted for publication 11 December 2025
Published 23 December 2025 Volume 2025:20 Pages 2641—2650
DOI https://doi.org/10.2147/CIA.S560920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Hoa Trung Dinh,1,2 Linh vu Huyen Ha,1 Ngoc Minh Luu,3 Toan Thi Thanh Do,3 Thu Thi Hoai Nguyen,4,5 Thanh Xuan Nguyen,4,6 Anh Trung Nguyen,4,5 Anh Lan Nguyen,4,5 Huong Thi Thu Nguyen,4,6 Hiep Hoang Phan,2 Tam Ngoc Nguyen,4,7 Huyen Thi Thanh Vu4,7
1Department of Internal Medicine, Hanoi Medical University, Hanoi, Vietnam; 2Department of Requested Treatment, National Hospital of Endocrinology, Hanoi, Vietnam; 3School of Preventive medicine and Public Health, Hanoi Medical University, Hanoi, Vietnam; 4Department of Geriatrics, Hanoi Medical University, Hanoi, Vietnam; 5Scientific Research Department, National Geriatric Hospital, Hanoi, Vietnam; 6Oncology and Palliative Care department, National Geriatric Hospital, Hanoi, Vietnam; 7Endocrinology and Rheumatology department, National Geriatric Hospital, Hanoi, Vietnam
Correspondence: Huyen Thi Thanh Vu, Department of Geriatrics, Hanoi Medical University, No. 1 Ton That Tung, Hanoi, 100000, Vietnam, Tel +84-913-531-579, Email [email protected]
Background: Frailty and falls significantly impact the health and quality of life of older adults with type 2 diabetes (T2D), increasing morbidity and dependency. However, their association in Vietnamese populations remains understudied. This study aimed to examine the association between frailty and fall risk and identify additional fall-related factors among older Vietnamese outpatients with T2D.
Methods: A cross-sectional study was conducted among 740 outpatients with T2D aged ≥ 60 years at a geriatric hospital in Hanoi, Vietnam, from March 2024 to December 2024. Fall risk was assessed using the 21-item Fall Risk Index (21-FRI), and frailty was determined by the Clinical Frailty Scale (CFS). Four multivariable logistic regression models evaluated frailty’s association with falls, adjusting for demographics, diabetes-related factors, and geriatric syndromes.
Results: Among 740 older participants with T2D, 17.8% were frail, and 16.8% reported at least one fall in the past year. Frailty was strongly associated with a higher fall rate (p< 0.001). In the fully adjusted logistic regression model, frailty emerged as a powerful and independent predictor of falls, increasing the odds by over four-fold (AOR 4.47, 95% CI 2.00– 5.29). Other significant risk factors included advanced age, poor glycemic control, diabetic complications, and co-existing geriatric syndromes (depression, urinary incontinence, cognitive impairment, and sarcopenia).
Conclusion: Routine frailty screening should be integrated into T2D care to identify high-risk older adults and implement tailored fall prevention strategies.
Keywords: frailty, falls, fall risk, type 2 diabetes, older adults, Vietnam, geriatric syndromes
Introduction
Vietnam is experiencing one of the fastest rates of population aging globally, with individuals aged 60 and older comprising 11.9% of the population in 2023, projected to reach 17.9% by 2030.1 This demographic shift has amplified the burden of chronic diseases, particularly type 2 diabetes (T2D), which affects approximately 7.3% of Vietnamese adults, with higher prevalence among older individuals.2 The convergence of aging and T2D poses significant challenges to public health, increasing the risk of complications and reducing quality of life.
Falls are a leading cause of morbidity and mortality among older adults, with approximately 28% of individuals aged 65 and older experiencing at least one fall annually.3 Older adults with T2D face a 59% higher risk of falls compared to their non-diabetic peers, driven by complications such as peripheral neuropathy, diabetic retinopathy, and autonomic dysfunction.4 Peripheral neuropathy impairs sensory feedback and balance, while retinopathy diminishes visual acuity, increasing the likelihood of missteps.5 Additionally, cardiovascular autonomic neuropathy can cause orthostatic hypotension, leading to dizziness and falls.6 Furthermore, T2DM-associated cardiovascular pathologies can accelerate cognitive decline, which in turn impairs hazard perception and judgment, further increasing fall risk.7 These diabetes-related impairments, combined with age-related declines, create a complex interplay that heightens fall risk.
Frailty, characterized by reduced physiological reserve and multisystem deterioration, further exacerbates fall risk in older adults with T2D.8 Frailty compromises muscle strength, balance, and resilience, amplifying the impact of diabetic complications. Despite its significance, the relationship between frailty and falls in T2D patients remains understudied, particularly in low- and middle-income countries (LMIC) like Vietnam, where healthcare systems face unique challenges in managing aging populations.9 The challenges are compounded by constrained geriatric capacity, as Vietnam has a single national geriatric hospital and geriatric departments in 49 out of 62 provinces, totaling 106 departments nationwide.10 Furthermore, consistently elevated out-of-pocket health expenditures (approximately 41% of total health expenditure in 2016) may restrict access to multifactorial fall-prevention and rehabilitation services.11 Prior studies have primarily focused on Western populations, leaving a critical gap in understanding frailty and falls in Asian contexts with distinct genetic, lifestyle, and healthcare access factors.12
Despite growing evidence linking frailty and falls in older adults with T2D globally, data in the Vietnamese population remain scarce. Moreover, a recent study among older Vietnamese rural community-dwellers revealed insufficient knowledge and only moderate attitudes and actions regarding fall prevention among older adults, highlighting substantial gaps in fall prevention.13
This study aimed to examine the association between frailty and risk of falls and identify fall-related factors among older Vietnamese patients with T2D. These findings could guide the development of tailored fall prevention strategies in Vietnam’s rapidly aging population.
Methods
Study Design and Participants
This cross-sectional study was conducted among patients aged ≥60 with T2D, defined by American Diabetes Association (ADA) 2024, who visited the outpatient department at a Geriatric Hospital, Hanoi, Vietnam, from March 2024 to December 202414 Participants were excluded if they: (1) were unable to understand and/or answer the questions, (2) suffered from acute or severe illness, or (3) did not consent to participate in the study (Figure 1).
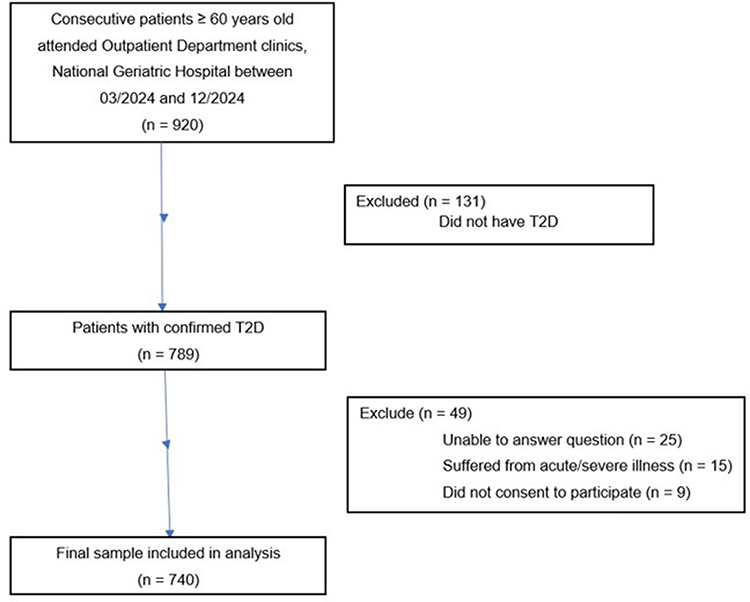 |
Figure 1 Flowchart of the participant recruitment process. |
Sample Size Calculation
The sample size was calculated using the single population proportion formula: n = Z21-a/2 * [p * (1-p)]/d2, where Z1-a/2 = 1.96 (95% confidence interval), p = 0.237 (fall prevalence from a 2021 study15), and d = 0.035 (precision). This yielded a minimum sample size of 631 participants to achieve 3.5% precision.
Data Collection
Geriatric specialists with clinical and research experience conducted standardized in-person interviews. Prior to data collection, they underwent training on the study protocol, objectives, eligibility criteria, and questionnaire administration.
Measurements
Falls
Participants reported falls in the previous 12 months (≥1 fall). For those with falls, additional details were collected on frequency, location (eg, bedroom, bathroom, stairs, hallway, outdoors, other), contributing factors (eg, postural dizziness, slippery surfaces, loss of balance, other), and fall-related consequences (eg, any injury, fracture, laceration/bruise, hospitalization).
The risk of falling was assessed using a 21-item fall risk index (FRI-21).16 FRI-21 is a self-report, yes/no questionnaire that screens community-dwelling older adults for multifactorial fall risk. It comprises 21 items spanning intrinsic factors (prior falls, reduced gait speed, balance problems, kyphosis, dizziness on standing, visual/hearing problems), treatment factors (polypharmacy, assistive device use), and environmental hazards (barriers, slippery/uneven surfaces, stairs/slopes). The total score of 21 items (0–21) was defined as higher risk of fall if having a score ≥9 points.17
Frailty Assessment
Frailty was assessed using the Clinical Frailty Scale (CFS).18,19 The score evaluates specific domains including comorbidity and loss of physical and cognitive function. The score ranges from very fit (CFS = 1) to very severely frail (CFS = 8) and terminally ill (CFS = 9). Frailty is defined as CFS ≥ 5.20
Independent Variables
Sociodemographic data included age (categorized as 60–69, 70–79, ≥80 years), gender (male/female), and living arrangement (with family/caregiver or alone). Diabetes-related variables, validated against medical records, included disease duration (<10 vs ≥10 years), HbA1c (<7.5% vs ≥7.5%), insulin use (yes/no), and chronic complications (yes/no, assessed via physical examination, including diabetic neuropathy, retinopathy, diabetic foot).
Geriatric Syndromes
Cognitive Function
Assessed using the Mini-cog test, including the three-word test and the clock test, with scores <3 indicating cognitive impairment.21
Comorbidities
Measured using the Charlson Comorbidity Index, with higher scores indicating greater morbidity.22
Depression
Evaluated with the 15-item Geriatric Depression Scale (GDS-15), with scores >5 indicating depression.23
Urinary incontinence
Assessed using the 3 Incontinence Questions (3IQ), with dichotomous responses (yes/no).24
Sarcopenia
Defined using the Asian Working Group for Sarcopenia (AWGS) criteria,25 including: (1) low muscle mass (appendicular skeletal muscle mass/height2 <7.0 kg/m2 for men, <5.7 kg/m2 for women, measured by bioelectrical impedance analysis [BIA 770, Korea]), (2) low muscle strength (handgrip strength <28 kg for men, <18 kg for women, measured by Jamar™ Hydraulic Hand Dynamometer), and/or (3) low gait speed (<0.8 m/s, assessed via a 4-meter walking test).
Statical Analysis
Data were analyzed using Stata version 18.0. Categorical variables were presented as frequencies and percentages, and continuous variables as medians with interquartile ranges (IQRs) due to non-normal distributions. All data collected for the variables used in this analysis were complete; therefore, no imputation or special handling for missing data was required. Differences between frail (CFS ≥ 5) and non-frail groups were assessed using Chi-squared or Fisher’s exact tests for categorical variables and Wilcoxon rank-sum tests for continuous variables. Four multivariable logistic regression models evaluated the association between frailty and falls: Model 1 (frailty only), Model 2 (adjusted for age, gender, living status), Model 3 (Model 2 plus diabetes duration, HbA1c, complications, insulin use), and Model 4 (Model 3 plus depression, urinary incontinence, cognitive impairment, sarcopenia, and Charlson Comorbidity Index). Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. All tests were two-tailed, with p < 0.05 considered statistically significant.
Results
Participant Characteristics
Among 740 older adults with type 2 diabetes (T2D) (mean age 74.6 ± 7.3 years, 63.9% female), 132 (17.8%) were frail. Frail participants were significantly older (47.0% aged ≥80 years vs 22.0% non-frail, p < 0.001) and had a higher prevalence of geriatric syndromes, including depression (42.4% vs 10.4%, p < 0.001), urinary incontinence (33.3% vs 14.1%, p < 0.001), cognitive impairment (68.9% vs 36.2%, p < 0.001), and sarcopenia (95% vs 75%, p < 0.001). They also had higher Charlson Comorbidity Index scores (median 6 [IQR 5–6] vs 4 [IQR 4–5], p < 0.001). No significant differences were observed in gender, living status, diabetes duration, or insulin use (Table 1).
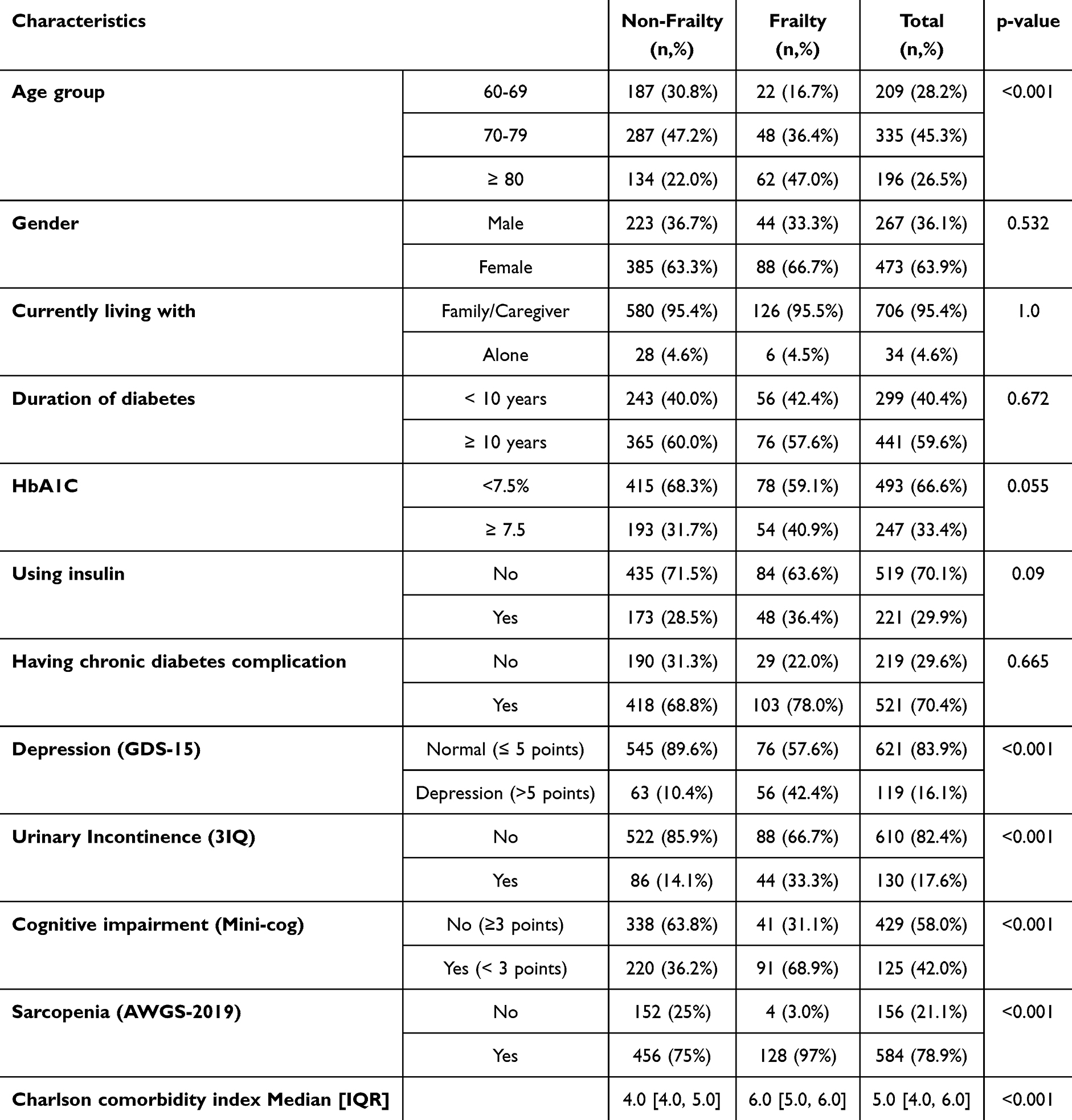 |
Table 1 Patients Socio-Demographic and Clinical Characteristics, Older Patients with Type 2 Diabetes (N = 740) |
Fall Prevalence and Characteristics
Overall, 124 participants (16.8%) reported at least one fall in the past year, and 44 (5.9%) experienced recurrent falls (≥2 falls). Frail participants had a significantly higher single fall rate (28.0% vs 14.3%, p < 0.001) but not recurrent falls (7.6% vs 5.6%, p = 0.503) compared to non-frail participants. Falls commonly occurred in bedrooms (6.8%) and bathrooms (2.6%), with frail participants reporting higher rates in these locations (p = 0.001 and p = 0.011, respectively). Slippery floors (49.6%) and loss of balance (24.8%) were the primary fall triggers, with no significant differences between groups. Injuries included bruises (36.9%) and fractures (9.0%), with hospitalizations reported in 2.5% of cases (Table 2).
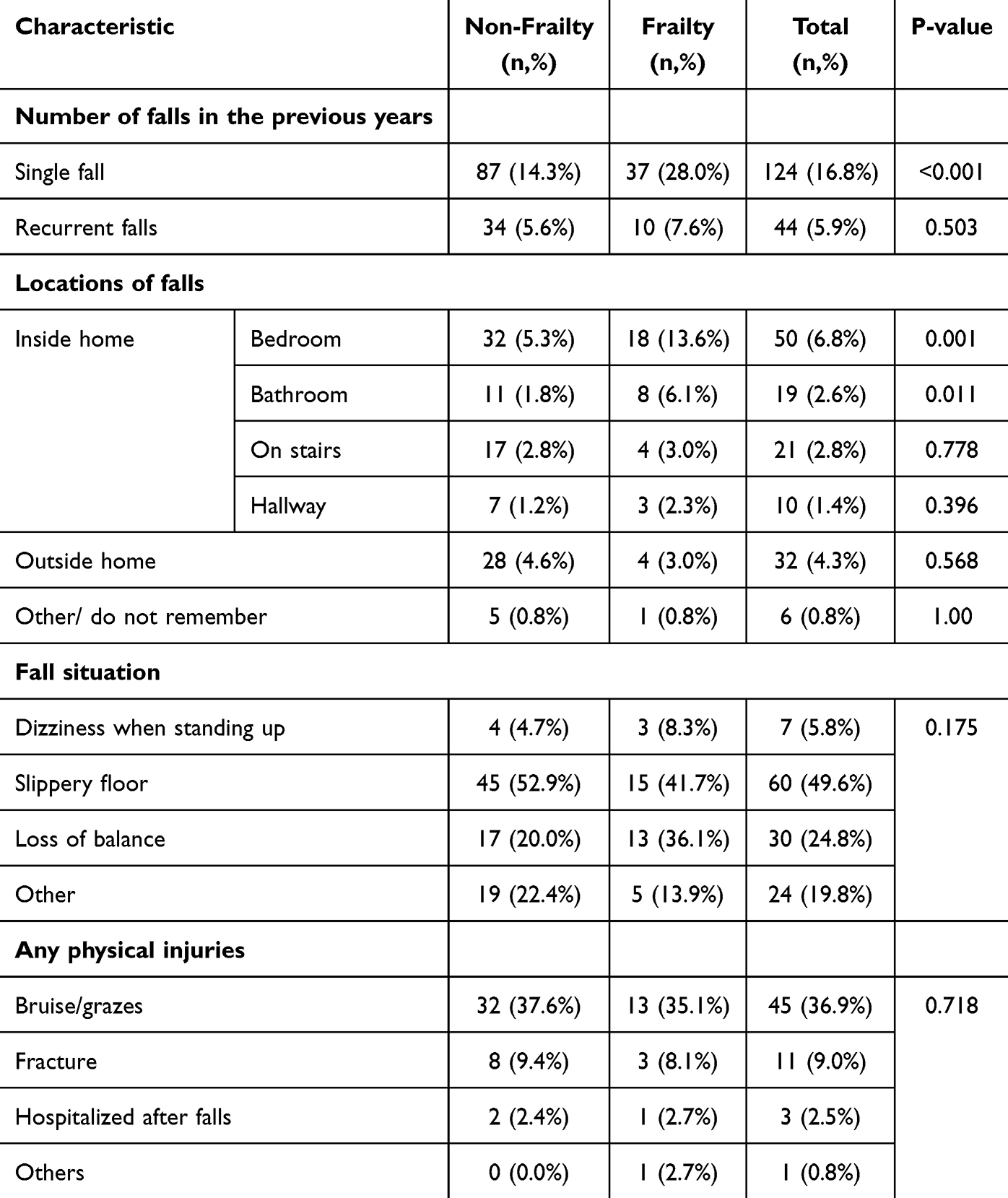 |
Table 2 Characteristics of Falls in Older Patients with/Without Frailty (N = 740) |
Factors Associated with Falls
Logistic regression analyses showed a strong association between frailty and risk of falls. In the unadjusted model (Model 1), frailty was associated with an odds ratio (OR) of 7.35 (95% CI 4.64–11.64). This association remained significant after adjustments: Model 2 (adjusted for demographics: AOR 6.82, 95% CI 4.25–10.94), Model 3 (Model 2 plus diabetes-related factors: AOR 6.66, 95% CI 4.12–10.77), and Model 4 (fully adjusted: AOR 4.47, 95% CI 2.00–5.29). In Model 4, other significant risk factors included age 70–79 years (AOR 2.64, 95% CI 1.17–2.95), HbA1c ≥7.5% (AOR 2.37, 95% CI 1.08–2.37), diabetic complications (AOR 2.81, 95% CI 1.20–2.85), depression (AOR 5.20, 95% CI 2.51–7.70), urinary incontinence (AOR 6.46, 95% CI 3.34–9.59), cognitive impairment (AOR 2.97, 95% CI 1.20–2.49), and sarcopenia (AOR 2.16, 95% CI 1.03–2.21) (Table 3).
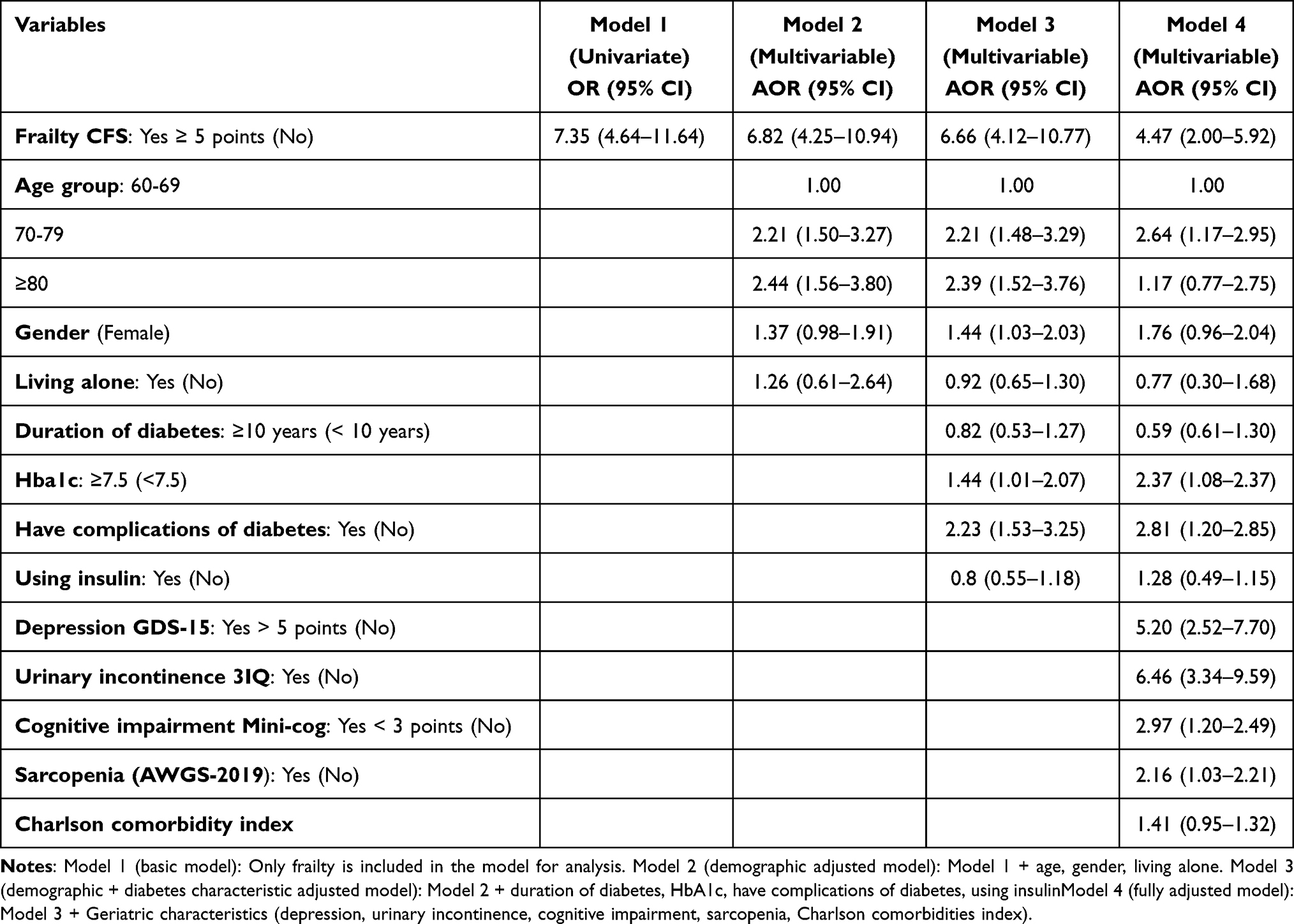 |
Table 3 Factors Associated with Increased Risk of Falls From the Univariate and Multivariable Models Regarding Relationship Between Frailty and Risk of Falls, Older Patients with T2D (N=740) |
Discussion
This study provides novel insights into the association between frailty and falls among older Vietnamese adults with type 2 diabetes (T2D), identifying frailty as a predominant risk factor. With 17.8% of participants classified as frail, our findings align with global estimates of frailty prevalence in T2D patients, which range from 15% to 30%.26 However, our frailty prevalence is lower than reported in Western cohorts (eg, 25% in the U.S27), possibly due to differences in lifestyle, diet, or healthcare access in Vietnam. Especially, Vietnamese multigenerational living arrangements may enhance nutritional status and social support for older adults, possibly mitigating frailty severity.28 Frail participants exhibited a significantly higher fall rate (28.0% vs 14.3% in non-frail, p < 0.001), particularly in domestic settings like bedrooms and bathrooms, underscoring the need for home-based fall prevention strategies.
Frailty’s robust association with falls persisted across all regression models, consistent with prior studies linking frailty to impaired neuromuscular function and balance.12 Frailty integrates multiple deficits, including sarcopenia, cognitive decline, and polypharmacy, which compromise postural stability and resilience, hence amplifying fall risk in T2D patients.8 For instance, sarcopenia reduces lower-limb strength, impairing gait stability, while cognitive impairment hinders hazard recognition, increasing trip likelihood. The study demonstrated that depression exacerbates risk via psychomotor retardation and gait instability, consistent with a longitudinal meta-analysis indicating that elevated depressive symptoms increased the odds of subsequent falls by 34%.29 Similarly, UI also increases falls risk plausibly due to the interaction of urgent voiding needs with impaired mobility and balance, particularly during rapid transitions.30,31 Reflecting this pathway, our cohort showed a significant increase in falls occurring in the bathroom, emphasizing the crucial role of systematic home-safety assessments. These geriatric syndromes, prevalent in our cohort, interact synergistically with T2D complications like peripheral neuropathy and retinopathy, which impair sensory feedback and visual acuity.5 This interaction creates a “vicious cycle” where, for example, frailty and cardiovascular disease, or diabetes and depression, mutually reinforce one another, further compounding a patient’s overall vulnerability and fall risk.32,33
Poor glycemic control (HbA1c ≥ 7.5%) and diabetic complications independently increased fall risk, aligning with studies showing that hyperglycemia induces microvascular damage and neuropathy, reducing proprioception and balance.6 Concordantly, a recent study among older T2D outpatients showed that longer diabetes duration (≥5 years) and diabetes complications were associated with poor glycaemic control, reinforcing cumulative neurovascular and visual pathways to falls.34 Unlike some studies reporting higher insulin-related fall risks,4 insulin use was not significant in our cohort, possibly due to lower insulin prevalence (29.9%) or better glycemic management.
This study’s strengths include its large sample size (n = 740), use of validated tools (eg, CFS, 21-FRI), and comprehensive multivariable modeling. As one of the first studies on frailty and falls in Vietnamese T2D patients, it addresses a critical gap in low- and middle-income countries, where aging and diabetes burdens are rising. However, limitations include the cross-sectional design, which precludes causality inference. Second, reliance on participant self-report for fall history over 12 months may introduce recall bias and underreport minor incidents. Integrating objective monitoring methods such as fall diaries with regular follow-up, and verification via medical records, can enhance data accuracy in future research. Third, we did not collect detailed data on polypharmacy or specific fall-risk-increasing drugs (eg, psychotropics, antihypertensives), apart from insulin. This is a known confounder, and future studies should include a comprehensive medication review. Lastly, the single-center urban setting may limit generalizability to rural populations with differing healthcare access.
Our findings advocate for routine frailty screening (eg, using CFS) and comprehensive geriatric assessments in T2D outpatient care to identify high-risk patients. Targeted interventions, such as strength training, home safety modifications, and cognitive therapy, could reduce falls.35–37 Future longitudinal studies with objective fall monitoring and multicenter designs are needed to confirm causality and explore rural–urban differences. In Vietnam’s rapidly aging population, these strategies are critical to reducing fall-related morbidity and enhancing quality of life. Furthermore, these results offer baseline, Vietnam-specific evidence that could benefit in the development of the first official Vietnamese national fall-prevention guidelines. Considering the similar constraints present in LMICs, a framework that includes CFS triage, and a cost-effective multifactorial bundle is readily transferable and could facilitate the advancement of guidelines in LMIC settings.
Conclusion
Considering the projected rise of the Vietnamese older population, mitigating falls in adults with T2D requires systemic intervention. Our findings indicate that frailty significantly stratifies fall risk independent of inadequate glycemic control, diabetes complications, and the existence of coexisting geriatric syndromes. These results support integrating frailty screening and comprehensive geriatric assessment into daily diabetes care to facilitate early detection of high-risk individuals and guide tailored fall prevention interventions.
Data Sharing Statement
The datasets of this study are available from the corresponding author on reasonable request.
Ethics Statement
The study was approved by Hanoi Medical University Ethics Committee in Vietnam (Ref: No 113526th December 2023), conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
All participants or their representatives/guardians were asked to give their written informed consent and they could withdraw anytime. Their information was kept confidential and used only for research purposes.
Acknowledgments
We would like to thank all patients participating in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Hoa Trung Dinh has been awarded a PhD scholarship funded by the Vingroup Innovation Foundation (VINIF), grant number VINIF.2024.TS.059.
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. General Statistics Office of Vietnam. Population and housing census. 2023.
2. Nguyen CT, Pham NM, Lee AH, Binns CW. Prevalence of and risk factors for type 2 diabetes mellitus in Vietnam: a systematic review. Asia Pac J Public Health. 2015;27(6):588–600. doi:10.1177/1010539515595860
3. World Health Organization. Falls: fact Sheet, 2021. 2021.
4. Yang Y, Hu X, Zhang Q, Zou R. Diabetes mellitus and risk of falls in older adults: a systematic review and meta-analysis. Age Ageing. 2016;45(6):761–767. doi:10.1093/ageing/afw140
5. Schwartz AV, Vittinghoff E, Sellmeyer DE, et al. Diabetes-related complications, glycemic control, and falls in older adults. Diabetes Care. 2008;31(3):391–396. doi:10.2337/dc07-1152
6. Vinik AI, Erbas T. Diabetic autonomic neuropathy. Handb Clin Neurol. 2013;117:279–294. doi:10.1016/B978-0-444-53491-0.00022-5
7. Militaru M, Lighezan DF, Tudoran C, Militaru AG. Connections between cognitive impairment and atrial fibrillation in patients with diabetes mellitus type 2. Biomedicines. 2024;12(3):672.
8. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet Lond Engl. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
9. HTT V, Nguyen TTH, Le TA, et al. Comprehensive geriatric assessment in older patients with diabetes mellitus in Hanoi, Vietnam. Gerontology. 2022;68(10):1132–1138. doi:10.1159/000521601
10. UNFPA Viet Nam. Market outlook for elderly care service in Viet Nam. Available from: https://vietnam.unfpa.org/sites/default/files/pub-pdf/en_-_vccihcm_report_-_market_mapping_on_elderly_care_service.pdf.
11. World Health Organization. Health financing in Viet Nam. 2025. Available from: https://www.who.int/vietnam/health-topics/health-financing.
12. Kojima G. Frailty as a predictor of future falls among community-dwelling older people: a systematic review and meta-analysis. J Am Med Dir Assoc. 2015;16(12):1027–1033. doi:10.1016/j.jamda.2015.06.018
13. Tang HT, Vu HM, Tang HT, et al. Knowledge, attitude and practice on fall risk factors and prevention among rural older community-dwellers in Vietnam. PLoS One. 2023;18(11):e0295119. doi:10.1371/journal.pone.0295119
14. ElSayed NA, McCoy RG, Aleppo G, American Diabetes Association Professional Practice Committee. 2 diagnosis and classification of diabetes: standards of care in diabetes—2025. Diabetes Care. 2024;48(Supplement_1):S27–S49. doi:10.2337/dc25-S002
15. VAT H, Nguyen TN, Nguyen TX, et al. Prevalence and factors associated with falls among older outpatients. Int J Environ Res Public Health. 2021;18(8):4041. doi:10.3390/ijerph18084041
16. Nguyen TN, Nguyen TN, Thillainadesan J, et al. Factors associated with frailty in geriatric patients with and without sarcopenia in Vietnam. Australas J Ageing. 2024;43(2):281–287. doi:10.1111/ajag.13253
17. Wada T, Ishimoto Y, Hirosaki M, et al. Twenty-one-item fall risk index predicts falls in elderly community-dwelling Japanese. J Am Geriatr Soc. 2009;57(12):2369–2371. doi:10.1111/j.1532-5415.2009.02591.x
18. HTT V, Nguyen TX, Nguyen TN, et al. Prevalence of frailty and its associated factors in older hospitalised patients in Vietnam. BMC Geriatr. 2017;17(1):216. doi:10.1186/s12877-017-0609-y
19. Nguyen TV, Ly TT, Nguyen TN. A pilot study of the clinical frailty scale to predict frailty transition and readmission in older patients in Vietnam. Int J Environ Res Public Health. 2020;17(5):1582. doi:10.3390/ijerph17051582
20. Church S, Rogers E, Rockwood K, Theou O. A scoping review of the clinical frailty scale. BMC Geriatr. 2020;20(1):393. doi:10.1186/s12877-020-01801-7
21. Tran LV, Nguyen TTH, Dinh HT, et al. TUG and six-minute walk test in vietnamese community-dwelling elderly. Lifestyle Med. 2025;6(6):e70031. doi:10.1002/lim2.70031
22. Charlson ME, Carrozzino D, Guidi J, Patierno C. Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91(1):8–35. doi:10.1159/000521288
23. Parsons M, Qiu L, Levis B, et al. Depression prevalence of the geriatric depression scale-15 was compared to structured clinical interview for DSM using individual participant data meta-analysis. Sci Rep. 2024;14(1):17430. doi:10.1038/s41598-024-68496-3
24. Brown JS, Bradley CS, Subak LL, et al. The sensitivity and specificity of a simple test to distinguish between urge and stress urinary incontinence. Ann Intern Med. 2006;144(10):715–723. doi:10.7326/0003-4819-144-10-200605160-00005
25. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e2. doi:10.1016/j.jamda.2019.12.012
26. Hanlon P, Fauré I, Corcoran N, et al. Frailty measurement, prevalence, incidence, and clinical implications in people with diabetes: a systematic review and study-level meta-analysis. Lancet Healthy Longev. 2020;1(3):e106–e116. doi:10.1016/S2666-7568(20)30014-3
27. Boccardi V, Bahat G, Balci C, et al. Challenges, current innovations, and opportunities for managing type 2 diabetes in frail older adults: a position paper of the European geriatric medicine society (EuGMS)-special interest group in diabetes. Eur Geriatr Med. 2025;16(4):1231–1247. doi:10.1007/s41999-025-01168-1
28. Xi JY, Zhong SR, Zhou YX, Lin X, Hao YT. Effects of family multi-generational relationship on multimorbidity and healthy life expectancy for second generations: insight from the China health and retirement longitudinal study. BMC Geriatr. 2023;23(1):100. doi:10.1186/s12877-022-03714-z
29. Bu H, Lu S, Wang L, et al. Depressive symptoms increase the risk of falls and injurious falls in Chinese adults aged ≥ 45 years: a 3-year cohort study. Front Public Health. 2022:10. doi:10.3389/fpubh.2022.964408
30. Paquin MH, Duclos C, Lapierre N, et al. The effects of a strong desire to void on gait for incontinent and continent older community-dwelling women at risk of falls. Neurourol Urodyn. 2020;39(2):642–649. doi:10.1002/nau.24234
31. Fritel X, Lachal L, Cassou B, Fauconnier A, Dargent-Molina P. Mobility impairment is associated with urge but not stress urinary incontinence in community-dwelling older women: results from the Ossébo study. BJOG Int J Obstet Gynaecol. 2013;120(12):1566–1572. doi:10.1111/1471-0528.12316
32. Shin JH, Kang GA, Kim SY, Won WC, Yoon JY. Bidirectional relationship between depression and frailty in older adults aged 70-84 years using random intercepts cross-lagged panel analysis. Res Community Public Health Nurs. 2024;35(1):1–9. doi:10.12799/rcphn.2023.00381
33. Sharma K, Dhungana G, Adhikari S, Bista Pandey A, Sharma M. Depression and anxiety among patients with type ii diabetes mellitus in Chitwan medical college teaching hospital, nepal. Nurs Res Pract. 2021;2021:1–8. doi:10.1155/2021/8846915
34. Nguyen TTH, Do HT, Dinh HT, et al. Medication adherence and its associated factors on glycemic control in older outpatients with type 2 diabetes in Vietnam. Clin Diabetol. 2025. doi:10.5603/cd.105762
35. Yang Y, Wang K, Liu H, et al. The impact of Otago exercise programme on the prevention of falls in older adult: a systematic review. Front Public Health. 2022;10:953593. doi:10.3389/fpubh.2022.953593
36. Campani D, Caristia S, Amariglio A, et al. IPEST working group. Home and environmental hazards modification for fall prevention among the elderly. Public Health Nurs. 2021;38(3):493–501. doi:10.1111/phn.12852
37. Lipardo DS, Tsang WWN. Falls prevention through physical and cognitive training (falls PACT) in older adults with mild cognitive impairment: a randomized controlled trial protocol. BMC Geriatr. 2018;18(1):193. doi:10.1186/s12877-018-0868-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.