Back to Journals » Clinical Interventions in Aging » Volume 21
Four-Limb Coordinated Training and Neuroplasticity in Older Adults with Cognitive Frailty: Mechanisms and Clinical Evidence
Received 8 January 2026
Accepted for publication 27 April 2026
Published 18 May 2026 Volume 2026:21 594798
DOI https://doi.org/10.2147/CIA.S594798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Wenbiao Guan,1,* ChaoHui Li,2,* Tiansheng Bu3
1Department of Rehabilitation Medicine, The First People’s Hospital of Baiyin City, Baiyin, 730900, People’s Republic of China; 2Logistics Service Center Medical Office, University of South China, Hengyang, 421001, People’s Republic of China; 3Department of Traditional Chinese Medicine, The First People’s Hospital of Baiyin City, Baiyin, 730900, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tiansheng Bu, Department of Traditional Chinese Medicine, The First People’s Hospital of Baiyin City, Baiyin, 730900, People’s Republic of China, Email [email protected]
Abstract: Cognitive frailty (CF), the coexistence of physical frailty and cognitive impairment without dementia, is associated with disability, institutionalization, and mortality, yet exercise prescriptions for this syndrome remain insufficiently targeted. This review examined whether four-limb coordinated training, defined as exercise that combines integrated upper- and lower-limb movement with meaningful coordination or motor-cognitive demands, is associated with neuroplasticity-related and clinical benefits in older adults with CF. Following PRISMA 2020 guidance, we conducted a focused PubMed-based systematic search and included six controlled studies for qualitative synthesis. Because interventions, comparators, and outcomes were highly heterogeneous, results were synthesized narratively using a tiered framework covering direct neuroplasticity outcomes, mechanistic proxy biomarkers, and indirect clinical outcomes. Across Baduanjin, virtual reality motor-cognitive training, exergaming, and functional resistance exercise, the direction of effect was generally favorable for global cognition, executive-related outcomes, frailty status, and physical performance including gait, balance, and chair-rise function. Direct mechanistic evidence was limited but suggested possible improvements in cerebral hemodynamics and hippocampal subregion structure, while biomarker studies indicated reductions in oxidative stress and inflammatory burden. Taken together, current evidence suggests that four-limb coordinated training is a biologically plausible and clinically relevant intervention candidate for CF, but confidence remains limited by the single-database search, small samples, study heterogeneity, indirect mechanistic endpoints, and short follow-up. The distinctive contribution of this review is the integration of intervention classification with a cautious neuroplasticity framework that can guide future trials toward standardized definitions, better reporting of coordination complexity and dose, and multimodal mechanistic assessment.
Keywords: cognitive frailty, four-limb coordinated training, motor–cognitive training, neuroplasticity, cerebral hemodynamics, hippocampal subregions
Introduction
Global population aging is increasing the burden of late-life cognitive decline and physical vulnerability.1 Cognitive frailty, defined by the International Academy on Nutrition and Aging and International Association of Gerontology and Geriatrics consensus as the coexistence of physical frailty and cognitive impairment in the absence of dementia,2 identifies a subgroup at heightened risk of disability, hospitalization, dementia, and mortality.3 Existing estimates vary because definitions are inconsistent, but recent reviews indicate that the syndrome is common enough in community and clinical aging populations to justify targeted preventive intervention research.4
Exercise is one of the most promising intervention classes for cognitive frailty because it can act on both physical and cognitive vulnerability.5 However, exercise effects are unlikely to be modality-neutral. Emerging exercise neuroscience supports a type-specificity perspective in which aerobic, resistance, and coordination-rich motor-cognitive exercise may engage partly distinct neuroplastic pathways and functional outcomes.6 Recent systematic reviews of exercise in cognitive frailty or related populations have generally focused on multicomponent exercise effectiveness, rather than isolating coordination-based interventions or integrating mechanistic evidence.7 This leaves an important gap between efficacy-oriented summaries and mechanism-informed exercise prescription.
Four-limb coordinated training may be particularly relevant to CF because it combines whole-body movement with sequencing, rhythm, interlimb integration, attentional control, and error correction. These features differentiate it from conventional walking-based aerobic exercise or isolated strengthening paradigms and provide a rationale for potentially stronger engagement of sensorimotor integration and executive-control systems. Studies in older adults have shown that coordination training can produce cognitive and neural benefits that differ from those observed after cardiovascular training, supporting the argument that coordination complexity itself may matter.5
The present review therefore aimed to synthesize the available controlled evidence on four-limb coordinated training in older adults with CF while making three contributions relative to earlier reviews: first, offering an operational definition and classification of this intervention concept; second, integrating neuroplasticity-related findings with clinical outcomes through a tiered mechanistic framework; and third, interpreting the evidence cautiously in light of study quality, heterogeneity, and the limited depth of direct mechanistic assessment.
Methods
This review followed the PRISMA 2020 reporting framework and used a focused systematic search with narrative synthesis to summarize clinical and neuroplasticity-related evidence on four-limb coordinated interventions in older adults with cognitive frailty. Because the available studies were heterogeneous in intervention content and endpoint selection, we prespecified narrative rather than quantitative synthesis.
Information Source and Search Strategy (PubMed)
A focused search was conducted in PubMed from database inception to the final archived search run available from the author team. The review was intentionally framed as a PubMed-based evidence synthesis rather than a comprehensive multi-database review, and this restriction is acknowledged as a methodological limitation. The Boolean strategy combined three concept blocks: cognitive frailty; exercise or motor-cognitive coordinated movement modalities, including mind-body exercise, exergaming, resistance training, and virtual reality-based training; and cognition or neuroplasticity-related outcomes.
((“cognitive frailty”[Title/Abstract] OR “cognitive frailty”[MeSH Terms]) AND (exercise[Title/Abstract] OR training[Title/Abstract] OR “physical activity”[Title/Abstract] OR “multicomponent exercise”[Title/Abstract] OR “motor-cognitive”[Title/Abstract] OR “dual-task”[Title/Abstract] OR coordination[Title/Abstract] OR “coordinated movement”[Title/Abstract] OR baduanjin[Title/Abstract] OR “mind-body exercise”[Title/Abstract] OR exergam[Title/Abstract] OR “resistance training”[Title/Abstract]) AND (cognition[Title/Abstract] OR “cognitive function”[Title/Abstract] OR neuroplastic[Title/Abstract] OR “brain-derived neurotrophic factor”[Title/Abstract] OR BDNF[Title/Abstract] OR “cerebral blood flow”[Title/Abstract] OR hippocamp*[Title/Abstract] OR MRI[Title/Abstract]))**
The archived PubMed results page indicated 66 records for the executed strategy. Because the archived file did not retain a verifiable calendar date and no prospectively registered protocol was in place, we report these facts transparently rather than retrospectively reconstructing unverified search metadata. Both issues are incorporated into the limitations section and considered when interpreting the strength of the evidence.
Eligibility Criteria (PICOS)
The Population: Adults aged ≥60 years with cognitive frailty, defined as the co-occurrence of physical frailty and cognitive impairment in the absence of dementia, or operational definitions consistent with the international consensus concept.8
Intervention: Structured programs with explicit four-limb coordination or motor–cognitive integration, including coordinated mind–body exercise, interactive exergaming requiring whole-body coordination, resistance training with multi-limb functional execution, or virtual reality (VR) motor–cognitive training.
Comparator: Usual care, health education, no structured exercise, or low-intensity control interventions.
Outcomes: At least one cognitive outcome and/or neuroplasticity-related marker (cerebral hemodynamics, brain structural measures, oxidative/inflammatory biomarkers interpreted as mechanistic proxies).
Study design: Randomized controlled trials (RCTs) or controlled quasi-experimental studies.
Exclusion criteria included: dementia samples; non-interventional designs; animal studies; and studies without extractable outcomes relevant to cognition or neuroplasticity mechanisms.
Study Selection Process (PRISMA Flow: Text-Only)
Because only PubMed was searched, no duplicate records were removed before screening. Titles and abstracts were screened to identify potentially eligible studies. Records were excluded when they were clearly unrelated to cognitive frailty, did not evaluate explicit coordination-based or motor-cognitive integrated exercise, were non-interventional, or did not report cognition- or mechanism-relevant outcomes. Sixteen full-text articles were assessed against the prespecified PICOS criteria, and ten were excluded because the population did not meet the CF concept, the intervention lacked sufficient coordination content, the design was non-interventional, or extractable cognition or neuroplasticity-relevant outcomes were unavailable. Six studies were finally included in the qualitative synthesis. The process of study screening and final inclusion in accordance with PRISMA 2020 guidance is displayed in Figure 1.
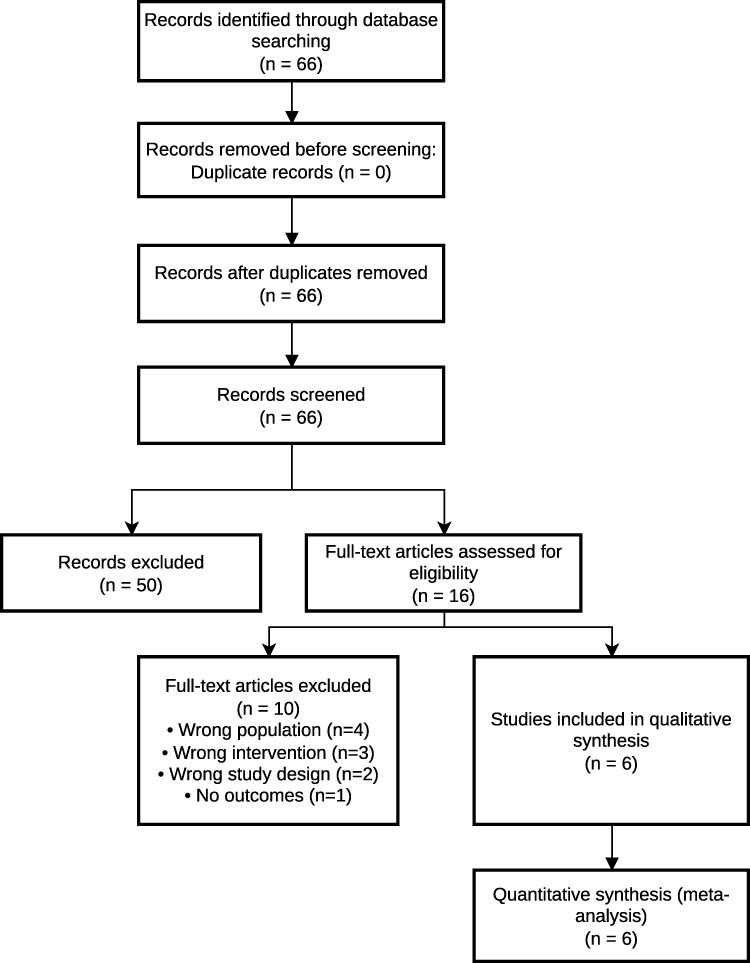 |
Figure 1 PRISMA 2020 flow diagram of the study selection process. |
Data Extraction
A standardized extraction form was used to collect: study design, setting, sample size, cognitive frailty operationalization, intervention dose and key coordination features, comparator, cognitive outcomes, physical/frailty outcomes, and neuroplasticity-related endpoints (direct measures or mechanistic proxies). Extracted outcomes were mapped to neuroplasticity domains (neurovascular/hemodynamic; structural MRI; immune–oxidative biomarkers; indirect cognitive outcomes). The core characteristics of the six included controlled studies are comprehensively presented in Table 1.
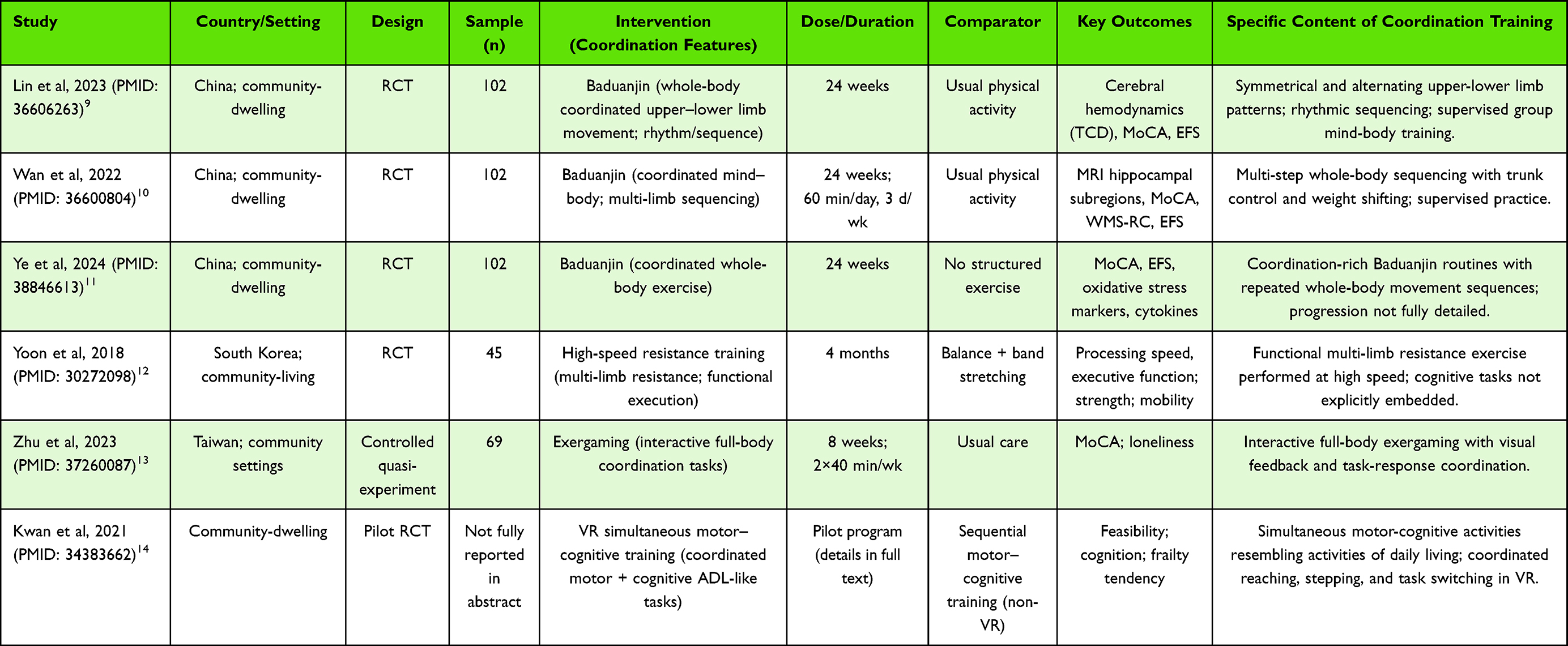 |
Table 1 Characteristics of Included Studies (PubMed-Indexed; n=6) |
Risk of Bias Assessment
RCTs were appraised using the Cochrane Risk of Bias 2 tool (RoB 2),15 while the controlled quasi-experimental study was assessed using ROBINS-I.16 Risk of bias was used to contextualize confidence in findings rather than as an exclusion criterion. Risk-of-bias judgments for included studies are presented in Table 2.
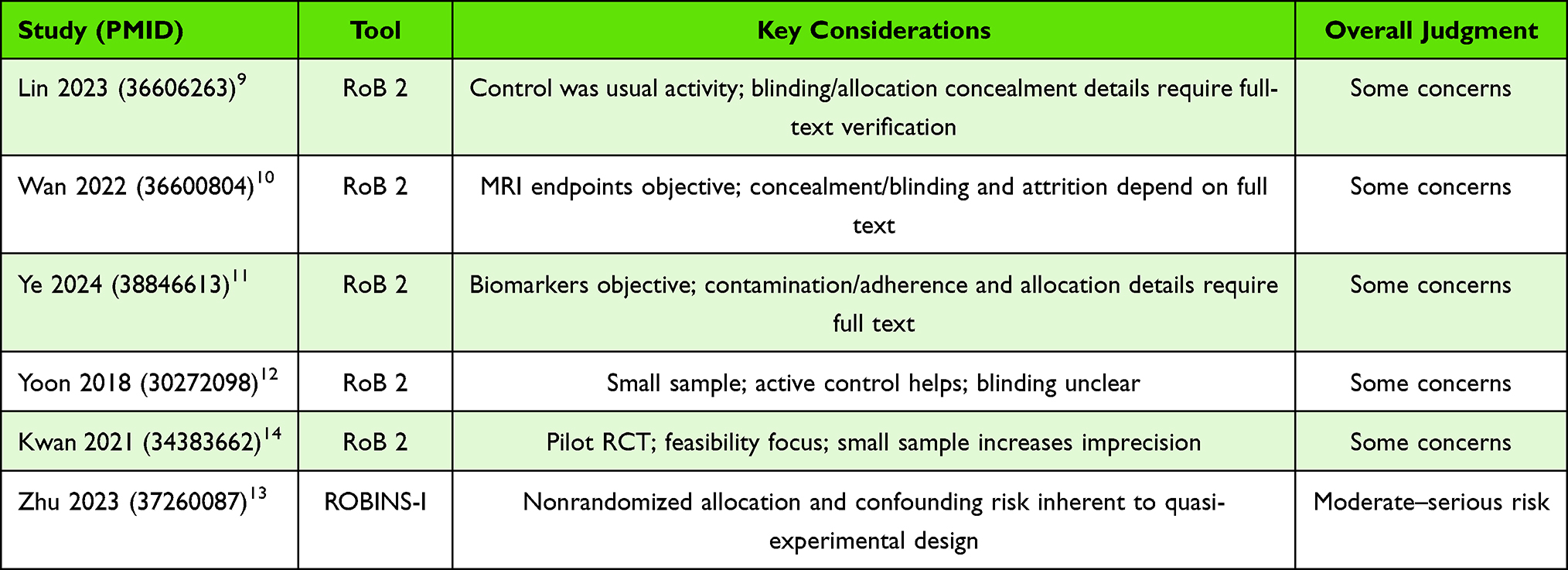 |
Table 2 Risk-of-Bias Appraisal of Included Studies |
Evidence Synthesis: Narrative Integration with Tiered Mechanistic Framework
Because intervention modalities, comparators, outcome definitions, and reporting formats were highly heterogeneous, a formal meta-analysis was not undertaken. In addition to narrative synthesis, we examined the direction of effect across studies as a descriptive consistency check. This approach showed that all six included studies reported at least one favorable intervention-related change in cognition, frailty status, physical performance, or mechanistic biomarkers; however, such directional assessment cannot quantify magnitude, account for small-study effects, or substitute for pooled estimates.
Tier 1 (Direct Neuroplasticity Outcomes)
Direct evidence linking four-limb coordinated training to neuroplasticity was available only in a subset of trials using cerebrovascular or neuroimaging outcomes.9,17 Coordinated mind-body exercise was associated with improvements in transcranial Doppler-derived measures of middle cerebral and basilar artery blood flow velocity, findings that are consistent with enhanced cerebral perfusion or neurovascular responsiveness but should not be interpreted as definitive proof of durable brain remodeling.18
Structural neuroplasticity was also explored in one randomized trial reporting modulation of hippocampal subregion volumes after prolonged coordinated exercise. Increases in memory-relevant subfields, including CA1, occurred alongside improvements in cognition and frailty scores.10 These observations are compatible with experience-dependent brain plasticity, although volumetric change alone cannot establish the specific cellular basis of adaptation.19
Tier 2 (Mechanistic Proxies)
Several randomized trials reported changes in biological markers closely linked to neuroplastic mechanisms. Coordinated exercise interventions were associated with increased antioxidant capacity (eg, elevated superoxide dismutase levels) and reduced oxidative stress markers (eg, malondialdehyde and 8-iso-prostaglandin F2α). In parallel, modulation of inflammatory cytokines, including interferon-γ and interleukins, was observed.
Several studies further reported that biomarker shifts statistically explained part of the cognitive improvement. Because these mediation analyses were conducted within small single-study datasets, they are better interpreted as hypothesis-supporting rather than as conclusive mechanistic proof.
Tier 3 (Indirect Clinical Outcomes)
Additional evidence was derived from trials reporting cognitive and functional improvements without direct neurobiological measurements. Motor–cognitive dual-task training, multicomponent resistance exercise, and interactive exergaming programs requiring coordinated limb movements were associated with improvements in global cognition, executive function, and processing speed in older adults with cognitive frailty.
Although these studies did not directly measure neuroplasticity, the pattern of benefit in executive-oriented cognitive outcomes and dual-domain function is broadly consistent with greater engagement of frontoparietal control and motor-cognitive integration processes. At the same time, the absence of direct head-to-head comparisons with aerobic exercise within CF populations means that any claim of superiority for coordinated training must remain provisional.
Conceptualization and Classification of Four-Limb Coordinated Training
Four-limb coordinated training is not a standardized term in geriatric rehabilitation. In this review, it is used as an operational category for interventions requiring integrated upper- and lower-limb movement under meaningful temporal, spatial, sequencing, or motor-cognitive constraints. We narrowed the concept to improve internal validity and to distinguish coordination-rich interventions from generic multicomponent exercise.
Conceptual Definition
In this review, four-limb coordinated training is defined as structured physical activity that engages both upper and lower extremities in coordinated movement patterns requiring motor planning, interlimb integration, and sustained attentional control. Core features include: concurrent involvement of at least three limbs, typically four; explicit coordination demands (eg, contralateral or alternating limb patterns, rhythmic sequencing, task switching); and engagement of higher-order motor–cognitive processes beyond repetitive single-joint movement.
This definition intentionally emphasizes movement complexity and coordination load, rather than metabolic intensity alone. Unlike traditional aerobic exercise (eg, walking) or isolated resistance training, four-limb coordinated training places sustained demands on sensorimotor integration, interhemispheric communication, and executive control, domains that are disproportionately vulnerable in cognitive frailty. From a systems perspective, such training simultaneously challenges musculoskeletal, cardiovascular, and central nervous system regulation, aligning closely with the multidimensional nature of cognitive frailty.
Distinction from Related Exercise Paradigms
Four-limb coordinated training overlaps with, but is not identical to, several better-known exercise paradigms. Multicomponent exercise may include balance, strength, and endurance components without sustained interlimb coordination. Dual-task training typically adds a separate cognitive task to movement, whereas four-limb coordinated training embeds coordination and attentional demands within the movement pattern itself. Mind-body exercise represents one subclass when synchronized upper-lower limb sequencing is central. Functional resistance exercise is included only when integrated multilimbed execution, rather than isolated strengthening alone, is clearly described.
This distinction is clinically relevant because neuroplastic adaptations appear to be more strongly associated with task complexity, novelty, and learning demands than with exercise intensity alone, particularly in older adults with compromised neural reserve.
Classification Framework
Based on intervention characteristics identified in the included studies and related literature, four-limb coordinated training can be classified into four non-mutually exclusive categories (Figure 2).
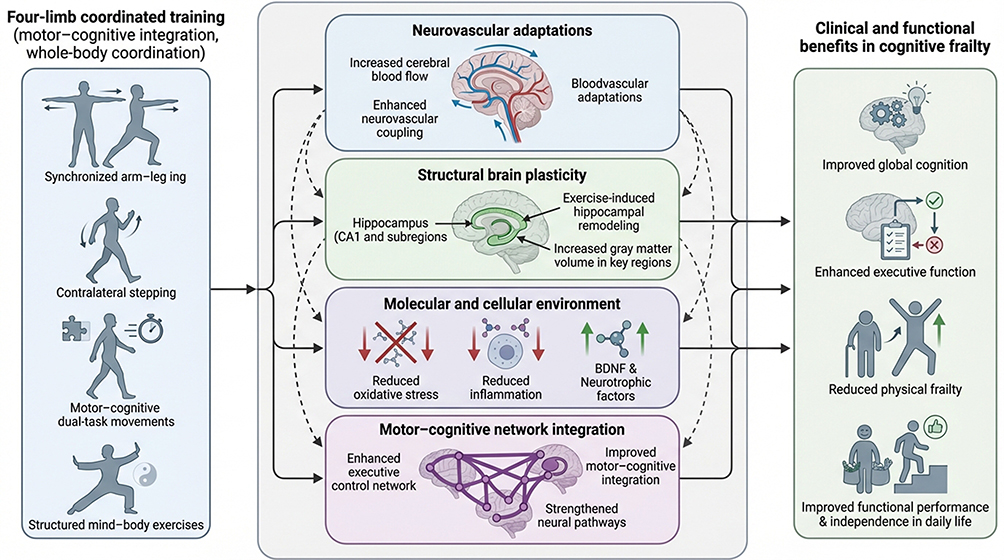 |
Figure 2 Proposed neuroplasticity mechanisms underlying the benefits of four-limb coordinated training in older adults with cognitive frailty. Green solid arrows indicate pathways supported by direct or convergent trial evidence; red dashed arrows indicate hypothesized or indirect pathways that require further confirmation. The framework illustrates how coordinated training may relate to neurovascular, structural, molecular, and network-level adaptations alongside cognitive, frailty, and physical-function outcomes. |
Type A: Coordinated Whole-Body Movement Training
This category includes exercises characterized by continuous, rhythmical coordination of upper and lower limbs, often performed in standing postures with weight shifting and trunk involvement. Baduanjin is a prototypical example, requiring contralateral limb movement, postural control, and sequential execution. Studies in cognitively frail older adults demonstrate that this modality is associated with improvements in cerebral hemodynamics and hippocampal subregion structure.9–11
Type B: Motor–Cognitive Coordinated Training
These interventions explicitly integrate cognitive operations (eg, attention switching, working memory, response inhibition) into coordinated limb movements. Examples include virtual reality–based motor–cognitive training and task-oriented coordination exercises in which movement patterns change in response to visual or auditory cues. Such approaches intensify executive control demands and may preferentially engage frontoparietal networks implicated in cognitive frailty.14
Type C: Functional Multilimbed Resistance Training
High-speed or functional resistance exercises involving simultaneous activation of upper and lower limbs fall into this category when coordination and timing are emphasized. Although resistance training is often classified separately from coordination training, evidence in cognitive frailty suggests that when resistance exercises require integrated, multi-limb execution, they may confer cognitive benefits beyond strength gains alone.12
Type D: Technology-Assisted Coordinated Training
Interactive exergaming platforms and sensor-based systems that require whole-body coordination represent an emerging category. These interventions combine real-time feedback, task variability, and coordinated movement, potentially enhancing motivation and adherence while imposing sustained motor–cognitive load. Preliminary evidence indicates improvements in global cognition in cognitively frail older adults.13
Key Training Parameters and Progression Principles
Across categories, several parameters appear central to the neuroplastic potential of four-limb coordinated training: coordination complexity, such as progression from symmetrical to asymmetrical or contralateral patterns; temporal demand, including rhythm, speed modulation, and task switching; cognitive engagement, such as sequence memory or rule updating; dose, with most included interventions lasting 8 to 24 weeks; and supervision, which appears important for safety, adherence, and progression. Importantly, progression is defined not only by load or intensity but also by increasing coordination and motor-cognitive challenge.
Importantly, progression in four-limb coordinated training is not solely defined by load or intensity, but by increasing coordination and cognitive challenge, a feature that distinguishes it from conventional exercise prescription models.
Relevance to Neuroplasticity in Cognitive Frailty
The conceptual and categorical framework outlined above provides a basis for understanding why four-limb coordinated training may be particularly well suited to cognitive frailty. By simultaneously engaging distributed neural systems responsible for movement execution, sensory integration, and executive control, such training may amplify activity-dependent neuroplasticity across vascular, structural, and molecular domains.20,21 This framework also enables systematic comparison across heterogeneous interventions and supports mechanistic synthesis in subsequent sections.22
Neuroplasticity Mechanisms Underlying Four-Limb Coordinated Training in Cognitive Frailty
Cognitive frailty is increasingly conceptualized as a clinical syndrome rooted in multisystem dysregulation, in which age-related declines in neural reserve interact with vascular, inflammatory, metabolic, and musculoskeletal impairments.23 Within this framework, exercise is best regarded as a biological stimulus that may promote adaptive change rather than as a uniform behavioral exposure.24 Four-limb coordinated training may exert particularly relevant effects because it simultaneously taxes movement execution, interlimb coordination, attention, and executive regulation.25
Neurovascular Adaptations and Cerebral Hemodynamics
Cerebrovascular dysfunction is a central pathophysiological feature of cognitive frailty, contributing to impaired cerebral perfusion, reduced neurovascular coupling, and vulnerability of cognitively relevant brain regions.26,27 Coordinated whole-body exercise has been shown to modulate cerebral blood flow dynamics more robustly than low-complexity or sedentary control conditions.28
Randomized evidence in older adults with CF suggests that sustained coordinated training, particularly Baduanjin, may improve transcranial Doppler indices of cerebral hemodynamics.9 These changes are compatible with better cerebrovascular responsiveness and perfusion of cognition-relevant regions, but the evidence remains limited to a small number of trials and short-term outcomes.29
Importantly, neurovascular benefits may be amplified by the rhythmic, whole-body nature of four-limb coordinated training, which combines moderate cardiovascular loading with postural control and attentional engagement.5 This combination may enhance endothelial function and cerebral autoregulation while avoiding excessive physiological stress, a balance particularly relevant for cognitively frail populations.30
Structural Neuroplasticity: Hippocampal and Network-Level Changes
In a randomized trial of community-dwelling older adults with CF, 24 weeks of Baduanjin was associated with larger volumes in several hippocampal subregions together with gains in global cognition and frailty status.31 These findings suggest that coordinated training may be linked to structural adaptation in vulnerable memory-related regions, although they do not establish neurogenesis or long-term disease modification.
In a randomized controlled trial involving community-dwelling older adults with cognitive frailty, 24 weeks of Baduanjin training was associated with increased volumes in multiple hippocampal subregions, including CA1 and related fields, compared with usual activity. These structural changes were accompanied by significant improvements in global cognition and frailty status, suggesting a meaningful link between exercise-induced brain remodeling and functional outcomes.32 While volumetric changes do not directly equate to neurogenesis, they are widely interpreted as markers of experience-dependent plasticity encompassing synaptic remodeling, dendritic complexity, and vascular support.33
The involvement of hippocampal subregions further supports the hypothesis that four-limb coordinated training engages learning-dependent mechanisms.34 Coordinated movement sequences require continuous updating of motor plans and sensorimotor predictions, potentially stimulating hippocampal–cortical interactions that extend beyond those elicited by repetitive, automated exercise.35
Molecular and Cellular Environment Favoring Neuroplasticity
Evidence from randomized trials indicates that coordinated whole-body exercise may improve the biological environment for neural adaptation in cognitively frail older adults.31 Reported changes include higher antioxidant enzyme activity, lower lipid peroxidation markers, and modulation of inflammatory cytokines. These findings strengthen biological plausibility, but most are proxy markers rather than direct indices of synaptic or network plasticity.
Evidence from randomized trials indicates that coordinated whole-body exercise can modulate this milieu in cognitively frail older adults.36 Specifically, four-limb coordinated training has been associated with increased antioxidant enzyme activity, such as superoxide dismutase, alongside reductions in lipid peroxidation markers, including malondialdehyde and 8-iso-prostaglandin F2α.11 Concurrent alterations in inflammatory cytokines, including interferon-γ and interleukins, have also been observed.
Notably, mediation analyses suggest that improvements in oxidative stress and inflammatory markers partially explain gains in cognitive performance following coordinated training. These findings support a mechanistic pathway in which four-limb coordinated exercise attenuates biological constraints on neural adaptability, thereby facilitating experience-dependent plasticity at the synaptic and network levels.37
Motor–Cognitive Integration and Network-Level Functional Adaptation
Four-limb coordinated training inherently challenges motor–cognitive integration, requiring the simultaneous engagement of motor execution, attentional control, and executive processing.35 This characteristic differentiates it from single-task aerobic or resistance exercise and may be particularly relevant for cognitive frailty, where executive dysfunction and reduced dual-task capacity are common.26,38
Indirect evidence from trials employing motor–cognitive training, high-speed functional resistance exercise, and technology-assisted coordinated movement suggests improvements in executive function, processing speed, and attentional control in cognitively frail older adults.39,40 Although these studies did not uniformly include direct neuroimaging or molecular markers, the cognitive domains most consistently improved align with frontoparietal control networks and basal ganglia–cortical circuits known to support coordinated action and cognitive flexibility.41,42
From a systems-neuroscience perspective, repeated engagement of these networks through complex whole-body coordination may strengthen functional efficiency. However, because direct connectivity measures are lacking in CF trials, this pathway should currently be treated as a mechanistic hypothesis supported indirectly by the pattern of cognitive benefit rather than as an established causal chain.43
Integration of Mechanistic Pathways
Taken together, the available evidence supports a multilevel but still incomplete neuroplasticity model for four-limb coordinated training in CF. Coordinated movement may act through converging neurovascular, structural, inflammatory, oxidative, and motor-cognitive pathways. These mechanisms are likely interdependent, yet the present evidence base is too limited to determine their relative contribution or temporal sequence with confidence.24
Crucially, these mechanisms are not independent. Improved neurovascular function may facilitate structural remodeling; reduced oxidative stress may permit more efficient synaptic modification; and repeated motor–cognitive engagement may translate these biological changes into durable functional gains.44,45 This convergence may explain why interventions emphasizing coordination and complexity show promise despite relatively modest metabolic intensity.5
However, the mechanistic evidence base remains incomplete. Standardized neuroplasticity markers are not consistently incorporated into trials, and long-term persistence of brain changes has rarely been assessed. Addressing these gaps will be essential for refining intervention design and for establishing causal pathways linking coordinated training to cognitive resilience in aging.46,47
Across the included studies, four-limb coordinated interventions were generally associated with improvements in global cognition, most often assessed with the Montreal Cognitive Assessment (MoCA). However, effect magnitudes varied, the number of trials was small, and the absence of pooled analysis limits precision. The overall pattern is therefore better described as consistently favorable than definitively established.
While neuroplasticity provides the biological foundation for exercise-induced cognitive improvement, its clinical relevance ultimately depends on whether such adaptations translate into meaningful gains in cognition, physical function, and frailty status.46 In cognitively frail older adults, these domains are tightly interrelated, and interventions capable of simultaneously improving cognitive and physical outcomes are of particular clinical value.8,26,48 Evidence from randomized and controlled studies indicates that four-limb coordinated training is associated with clinically relevant benefits across multiple functional domains.
Effects on Global Cognition and Domain-Specific Cognitive Function
Across included trials, four-limb coordinated interventions consistently demonstrated improvements in global cognitive performance, most commonly assessed using the Montreal Cognitive Assessment (MoCA).49 Coordinated mind–body exercise programs, such as Baduanjin, produced statistically and clinically meaningful increases in MoCA scores following 24 weeks of training compared with usual activity or no-exercise controls. The magnitude of improvement observed in these studies suggests potential relevance beyond short-term test–retest effects, particularly in populations characterized by elevated cognitive vulnerability.50
In addition to global cognition, domain-specific improvements were reported in executive function, processing speed, and attention, especially in studies incorporating explicit motor–cognitive integration or high-speed multilimbed resistance training.5,38 These domains are critically involved in daily decision-making, gait adaptability, and fall avoidance, and are often disproportionately impaired in cognitive frailty. The selective enhancement of executive-related domains aligns with the hypothesis that coordinated movement tasks preferentially engage frontoparietal control networks.41
Effects on Physical Frailty and Functional Performance
A defining feature of four-limb coordinated training is its potential to improve cognitive and physical outcomes concurrently.51 In the included studies, gains in global cognition often co-occurred with lower frailty scores or better physical performance.52 This convergence is clinically important, but it should not be interpreted as proof that a single shared mechanism was directly demonstrated.
High-speed functional resistance training involving coordinated upper and lower limb movements resulted in improvements in gait speed, chair-rise performance, and overall physical function in cognitively frail participants. Although changes in composite frailty scores were not always statistically significant in smaller samples, consistent gains in physical performance indicators suggest meaningful functional adaptation.48,53
Integrated Cognitive–Physical Benefits and Dual-Outcome Relevance
A defining feature of four-limb coordinated training is its capacity to produce concurrent cognitive and physical benefits, rather than improvements restricted to a single domain.5 This dual-outcome profile distinguishes coordinated interventions from more narrowly targeted exercise programs and aligns closely with the conceptual model of cognitive frailty as a combined cognitive–physical syndrome.8,26
Across trials, four-limb coordinated training was generally feasible and well tolerated in cognitively frail older adults, with few serious adverse events reported.54 Nevertheless, because balance and sequencing demands differ across interventions, safety likely depends on supervision, progression, and participant selection rather than on the intervention label alone.55
From a clinical perspective, interventions capable of improving both cognition and physical resilience are particularly attractive, as they may reduce care dependency and delay progression toward disability or dementia.47
Effects on Psychosocial and Quality-of-Life–Related Outcomes
Taken together, the clinical evidence suggests short- to medium-term benefits of four-limb coordinated training for cognition and functional status in older adults with CF.52 Confidence in this conclusion is moderated by the predominance of studies rated as having some concerns of bias and by one nonrandomized study at moderate-to-serious risk of bias.56 Accordingly, the evidence should be interpreted as promising but not yet definitive.
Mind–body coordinated exercises may offer additional psychosocial benefits through structured group participation and embodied attentional practices; however, current evidence remains insufficient to draw firm conclusions.57
Despite encouraging early results, several methodological limitations constrain inference.58 These include the single-database search strategy, inconsistent operationalization of CF, heterogeneous intervention reporting, limited direct neuroplasticity endpoints, short follow-up, and underpowered samples.59 These issues restrict both comparability across studies and confidence in causal interpretation.
Across trials, four-limb coordinated training was generally well tolerated and safe in cognitively frail older adults.60 Reported adverse events were minimal, and adherence rates were acceptable, particularly in supervised or group-based settings.61 Technology-assisted interventions, including virtual reality–based motor–cognitive training, demonstrated feasibility and acceptable adherence in pilot studies, suggesting potential for scalable and home-based applications.
A fundamental challenge is the lack of uniform diagnostic criteria for CF.62 Studies differ in frailty instruments, cognitive screening tools, and thresholds, which complicates cross-study comparison and may mask subtype-specific responses.63 Future trials should report diagnostic components explicitly and, where possible, distinguish vascular-dominant, neurodegenerative-dominant, or mixed vulnerability profiles.64
Clinical Interpretation of Evidence Strength
Another limitation concerns incomplete reporting of coordination-based interventions.65 Broad labels such as exercise, multicomponent training, or mind-body exercise are often used without enough detail on coordination pattern, sequencing demands, progression rules, supervision, or motor-cognitive load.66 Better reporting is essential if this intervention class is to become reproducible and clinically prescribable.67
However, limitations include relatively small sample sizes, variability in intervention protocols, and limited long-term follow-up. Despite these constraints, the convergence of cognitive and physical improvements, together with mechanistic support outlined in Section 4, suggests that four-limb coordinated training represents a clinically meaningful and biologically plausible intervention for cognitive frailty.
Methodological Challenges and Research Gaps
Despite accumulating evidence supporting the potential benefits of four-limb coordinated training in older adults with cognitive frailty, several methodological challenges and knowledge gaps limit the interpretability, comparability, and translational impact of existing studies. Addressing these issues is essential for advancing the field from promising pilot trials toward robust, evidence-based clinical recommendations.68
Most trials enrolled modest samples and lasted between 8 and 24 weeks.69 Such designs are suitable for feasibility or proof-of-concept work,70 but they are insufficient for determining durability of benefit, progression to dementia, or sustained modification of frailty trajectories.71
A fundamental challenge lies in the lack of uniform diagnostic criteria for cognitive frailty. Although the international consensus defines cognitive frailty as the coexistence of physical frailty and cognitive impairment in the absence of dementia, operational definitions vary substantially across studies.72 Differences include the choice of frailty instruments (eg, Fried phenotype versus multidimensional frailty scales), cognitive screening tools (eg, MoCA, MMSE), and threshold values used to define impairment.
This heterogeneity complicates cross-study comparisons and may contribute to variability in intervention effects.73 Importantly, cognitive frailty is increasingly recognized as a heterogeneous syndrome, encompassing subtypes driven predominantly by vascular, neurodegenerative, or physical vulnerability pathways. Current trials rarely stratify participants by such subtypes, limiting insights into differential responsiveness to coordinated training interventions.74
Inconsistent Conceptualization and Reporting of Four-Limb Coordinated Training
Finally, few studies explicitly tested whether mechanistic biomarkers statistically linked intervention exposure to cognitive or frailty outcomes.75 Without integrated mediation frameworks combining imaging, biological, and functional endpoints, neuroplasticity remains a plausible explanatory model rather than a confirmed causal pathway.76
This lack of granularity hampers replication and obscures dose–response relationships. Unlike conventional exercise prescription, where intensity can be quantified using heart rate or workload, four-limb coordinated training relies heavily on movement complexity and motor–cognitive load, which are rarely quantified or systematically progressed.52 The absence of standardized reporting frameworks for coordination complexity represents a significant barrier to evidence synthesis and clinical implementation.77
Discussion
This review synthesizes the available controlled evidence on four-limb coordinated training in older adults with CF and interprets it through a cautious neuroplasticity lens. The main message is not that coordinated training has been proven superior to other exercise modalities, but that it represents a conceptually coherent intervention class with encouraging early clinical signals and a plausible multilevel mechanistic rationale.
Moreover, there is no consensus on a core set of neuroplasticity outcomes appropriate for cognitive frailty research.78 Studies differ widely in the choice of biomarkers, imaging modalities, and analytic approaches, making it difficult to integrate findings across trials. Longitudinal assessment of neuroplastic changes and their persistence after intervention cessation is particularly scarce.
A central contribution of this review is the integration of direct neuroplasticity evidence, mechanistic proxy biomarkers, and functional outcomes within the same narrative framework. This approach helps distinguish what is directly shown, what is indirectly supported, and what remains hypothetical. Such differentiation is important because much of the current literature uses neuroplastic terminology broadly, even when evidence comes primarily from proxy measures or clinical outcomes.
Most trials investigating four-limb coordinated training in cognitive frailty are characterized by modest sample sizes and relatively short intervention periods, often ranging from 8 to 24 weeks.79 While such designs are appropriate for feasibility and proof-of-concept studies, they limit statistical power and the ability to detect clinically meaningful changes in cognition, frailty progression, or neuroplasticity trajectories.
Additionally, few studies include long-term follow-up, precluding conclusions about the durability of intervention effects or their potential to delay conversion to dementia or disability. Given the progressive nature of cognitive frailty, longer-term trials with repeated outcome assessments are necessary to establish sustained clinical relevance.
Compared with conventional aerobic or isolated resistance exercise, four-limb coordinated training appears theoretically well suited to CF because it couples physical loading with sequencing, timing, and executive demands.80 However, there are currently no adequately powered head-to-head CF trials demonstrating superiority over aerobic training,81 and this review therefore frames the advantage of coordinated training as a reasoned hypothesis grounded in exercise-type specificity rather than as a settled empirical fact.
The choice of control conditions represents another methodological challenge. Many trials compare coordinated training with usual activity or no-exercise controls, which may inflate observed effect sizes due to nonspecific factors such as social interaction, expectancy effects, or increased attention. Although some studies employ active control conditions (eg, stretching or balance exercises), these are not consistently matched for contact time or engagement level.79
The findings also have practical implications. Clinicians may consider coordination-rich whole-body exercise, motor-cognitive routines, functional multilimbed resistance tasks, or technology-assisted training for older adults with early CF when supervision and progression are available. In practice, task complexity, safety, and adherence may matter as much as metabolic intensity.
Limited Integration of Clinical and Mechanistic Endpoints
The current evidence base remains constrained by methodological limitations. Five of the six included studies were judged to have some concerns of bias, and the single quasi-experimental study carried moderate-to-serious risk of bias. The review itself is further limited by its PubMed-only search, absence of a prospectively registered protocol, and inability to verify an archived exact search date. These limitations should temper interpretation.
Discussion
Future work should prioritize multicenter randomized trials using standardized CF definitions, transparent reporting of coordination content and progression, active comparators, and multimodal mechanistic assessment. Emerging technologies such as virtual reality and sensor-based platforms may be especially useful because they can standardize task complexity while capturing detailed performance metrics.
Integration of Neuroplasticity Mechanisms and Clinical Outcomes
Cognitive frailty is a clinically important and potentially modifiable state at the interface of physical frailty and cognitive impairment.82 The currently available controlled studies suggest that four-limb coordinated training may improve global cognition, executive-related outcomes, frailty status, and selected physical-function measures in older adults with CF.52
Direct mechanistic evidence remains limited, but available trials are compatible with improvements in cerebral hemodynamics, hippocampal subregion structure, and inflammatory or oxidative profiles. The distinctive contribution of this review is to organize these signals within an intervention-classification and mechanistic framework rather than to claim definitive causal proof.
Compared with conventional exercise summaries, this review specifically focuses on coordination-rich training and distinguishes direct neuroplasticity evidence from mechanistic proxies and indirect clinical outcomes. That distinction may help future investigators design more rigorous trials and more reproducible coordination-based exercise prescriptions.
At the same time, the evidence base remains limited by heterogeneity in CF definitions, incomplete intervention reporting, small samples, short follow-up, and a focused PubMed-only search strategy. Four-limb coordinated training should therefore be viewed as a promising and biologically plausible intervention candidate, not yet as an established standard of care.
From a neurocognitive perspective, coordinated movement tasks likely engage distributed networks involving the prefrontal cortex, basal ganglia, cerebellum, and hippocampus.42 Repeated activation of these networks through complex, rhythmical, and attention-demanding movement may strengthen functional connectivity and improve network efficiency.83 Clinically, this is reflected in selective improvements in executive function and processing speed—domains closely linked to gait adaptability, fall risk, and daily functioning in older adults.84
Furthermore, many four-limb coordinated interventions (eg, mind–body exercise, exergaming) are inherently structured, progressive, and engaging, which may enhance adherence and sustainability. These features are particularly relevant for cognitively frail populations, where motivation and self-efficacy can be compromised.85
Clinical Implications and Practical Considerations
The findings of this review have several implications for clinical practice. First, four-limb coordinated training appears to be safe and feasible when appropriately supervised and progressed, with minimal adverse events reported across trials.84,86 Second, the dual benefits observed in cognition and physical function suggest that such interventions may serve as efficient, integrated strategies within geriatric rehabilitation and community-based aging programs.84
In practical terms, clinicians may consider incorporating coordinated whole-body exercises—such as structured mind–body routines, functional multilimbed resistance tasks, or motor–cognitive exergaming—into intervention plans for older adults with early cognitive frailty.87 Emphasis should be placed on progressive increases in coordination complexity and cognitive engagement, rather than solely on intensity or load.88 Individualization, clear safety protocols, and monitoring of adherence remain essential, particularly for individuals with balance impairments or comorbidities.89
Limitations of the Current Evidence Base
Despite promising findings, the evidence base remains constrained by methodological limitations. Sample sizes are generally modest, intervention protocols heterogeneous, and follow-up durations short.68 Neuroplasticity outcomes are inconsistently measured, and few studies integrate biological, neuroimaging, and functional endpoints within a single analytic framework. As a result, causal inferences regarding specific mechanisms remain tentative.90
Additionally, cognitive frailty itself is a heterogeneous condition, and current studies rarely stratify participants by frailty severity, cognitive profile, or vascular risk. Such heterogeneity may obscure subgroup-specific responses to coordinated training and contribute to variability in outcomes.
Future Directions
Future research should prioritize well-powered, multicenter randomized controlled trials with standardized definitions of cognitive frailty and clearly operationalized coordination-based interventions. Incorporating multimodal neuroplasticity markers—including neuroimaging, cerebrovascular measures, and molecular biomarkers—will be critical for validating mechanistic pathways. Longer-term follow-up is also needed to determine whether coordinated training can slow progression to dementia, reduce disability, or sustain functional independence.60
Emerging technologies, such as virtual reality and sensor-based systems, offer opportunities to deliver personalized, scalable four-limb coordinated training while capturing detailed performance metrics. Such approaches may facilitate precision interventions tailored to individual motor–cognitive profiles.
Conclusions
Cognitive frailty represents a critical and potentially reversible stage in the aging trajectory, characterized by the convergence of physical vulnerability and cognitive decline.68 The findings synthesized in this review indicate that four-limb coordinated training—encompassing coordinated whole-body movement, motor–cognitive integration, and functional multilimbed exercise—offers a promising, mechanism-informed intervention strategy for older adults with cognitive frailty.
Across available clinical trials, four-limb coordinated training was associated with consistent improvements in global cognition, executive function, and frailty-related outcomes.52 Importantly, emerging evidence demonstrates that these functional benefits are accompanied by neuroplasticity-related adaptations, including enhanced cerebral hemodynamics, structural modulation of hippocampal subregions, and favorable shifts in oxidative and inflammatory profiles. Together, these findings support a multilevel neuroplasticity model in which coordinated movement complexity and motor–cognitive engagement act as key drivers of adaptive brain change in cognitively frail older adults.52
Compared with conventional exercise paradigms, four-limb coordinated training appears uniquely suited to address the dual cognitive–physical nature of cognitive frailty.52 By simultaneously challenging motor coordination, attentional control, and executive processing, such interventions may strengthen distributed neural networks while also improving physical resilience. This integrated effect profile aligns closely with the clinical needs of cognitively frail populations and underscores the potential value of coordinated training within geriatric rehabilitation and community-based aging programs.91
Nevertheless, the current evidence base remains limited by heterogeneity in cognitive frailty definitions, variability in intervention protocols, and inconsistent measurement of neuroplasticity outcomes. While the available data are encouraging, definitive conclusions regarding long-term efficacy, optimal training parameters, and disease-modifying potential cannot yet be drawn. Future research should prioritize standardized diagnostic criteria, clearly operationalized coordination-based interventions, and the integration of multimodal neuroplasticity markers with clinically meaningful endpoints.
In conclusion, four-limb coordinated training represents a biologically plausible and clinically relevant approach to mitigating cognitive frailty in older adults. With further methodological refinement and high-quality longitudinal research, this intervention paradigm has the potential to contribute meaningfully to strategies aimed at preserving cognitive health, functional independence, and quality of life in aging populations.
Funding
This study was supported by the Baiyin Municipal Science and Technology Plan Project (Approval No. Shikefa [2024] 42; Project No. 2024-1-36S).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang XM, Wu XJ, Cao J, et al. Association between cognitive frailty and adverse outcomes among older adults: a meta-analysis. J Nutrition Health Aging. 2022;26(9):817–18. doi:10.1007/s12603-022-1833-5
2. Chen B, Wang M, He Q, et al. Impact of frailty, mild cognitive impairment and cognitive frailty on adverse health outcomes among community-dwelling older adults: a systematic review and meta-analysis. Front Med. 2022;9:1009794. doi:10.3389/fmed.2022.1009794
3. Bian J, Chen Z, Gao Y, et al. Prevalence of cognitive frailty, reversible and potentially reversible cognitive frailty among older adults without dementia: a systematic review and meta-analysis. J Gerontol Series B. 2026;81(1):Gbaf228.
4. Bregola AG, Ottaviani AC, Luchesi BM, et al. Accumulated cognitive impairment, frailty, burden, and perceived stress and the risk of hospitalization and mortality in older caregivers. Dementia Neuropsychol. 2022;16(1):33–44. doi:10.1590/1980-5764-DN-2020-0091
5. Voelcker-Rehage C, Godde B, Staudinger UM. Cardiovascular and coordination training differentially improve cognitive performance and neural processing in older adults. Front Human Neurosci. 2011;5:26. doi:10.3389/fnhum.2011.00026
6. Wang J, Kong D, Yu F, et al. Cognitive deficit, physical frailty, hospitalization and emergency department visits in later life. Aging Mental Health. 2021;25(3):521–527. doi:10.1080/13607863.2019.1699015
7. Dunsky A. The effect of balance and coordination exercises on quality of life in older adults: a mini-review. Front Aging Neurosci. 2019;11:318. doi:10.3389/fnagi.2019.00318
8. Kelaiditi E, Cesari M, Canevelli M, et al. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutrition Health Aging. 2013;17(9):726–734. doi:10.1007/s12603-013-0367-2
9. Lin H, Ye Y, Wan M, et al. Effect of Baduanjin exercise on cerebral blood flow and cognitive frailty in the community older adults with cognitive frailty: a randomized controlled trial. J Exercise Sci Fitness. 2023;21(1):131–137. doi:10.1016/j.jesf.2022.12.001
10. Wan M, Xia R, Lin H, et al. Baduanjin exercise modulates the hippocampal subregion structure in community-dwelling older adults with cognitive frailty. Front Aging Neurosci. 2022;14:956273. doi:10.3389/fnagi.2022.956273
11. Ye Y, Wan M, Lin H, et al. Effects of Baduanjin exercise on cognitive frailty, oxidative stress, and chronic inflammation in older adults with cognitive frailty: a randomized controlled trial. Front Public Health. 2024;12:1385542. doi:10.3389/fpubh.2024.1385542
12. Yoon DH, Lee JY, Song W. Effects of resistance exercise training on cognitive function and physical performance in cognitive frailty: a randomized controlled trial. J Nutrition Health Aging. 2018;22(8):944–951. doi:10.1007/s12603-018-1090-9
13. Zhu YZ, Lin CF, Yang HL, et al. Effects of exergaming on cognitive functions and loneliness of older adults with cognitive frailty. Int J Geriatric Psychiatr. 2023;38(6):e5944. doi:10.1002/gps.5944
14. Kwan RYC, Liu JYW, Fong KNK, et al. Feasibility and effects of virtual reality motor-cognitive training in community-dwelling older people with cognitive frailty: pilot randomized controlled trial. JMIR Serious Games. 2021;9(3):e28400. doi:10.2196/28400
15. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
16. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
17. Han YMY, Chan MMY, Choi CXT, et al. The neurobiological effects of mind-body exercise: a systematic review and meta-analysis of neuroimaging studies. Scientific Reports. 2023;13(1):10948. doi:10.1038/s41598-023-37309-4
18. Fico BG, Miller KB, Rivera-Rivera LA, et al. Cerebral hemodynamics comparison using transcranial Doppler ultrasound and 4D flow MRI. Front Physiol. 2023;14:1198615. doi:10.3389/fphys.2023.1198615
19. Asan L, Falfán-Melgoza C, Beretta CA, et al. Cellular correlates of gray matter volume changes in magnetic resonance morphometry identified by two-photon microscopy. Scientific Reports. 2021;11(1):4234. doi:10.1038/s41598-021-83491-8
20. Voelcker-Rehage C, Niemann C. Structural and functional brain changes related to different types of physical activity across the life span. Neurosci Biobehav Rev. 2013;37(9 Pt B):2268–2295. doi:10.1016/j.neubiorev.2013.01.028
21. Voss MW, Vivar C, Kramer AF, et al. Bridging animal and human models of exercise-induced brain plasticity. Trends Cognitive Sci. 2013;17(10):525–544. doi:10.1016/j.tics.2013.08.001
22. Kramer AF, Erickson KI. Capitalizing on cortical plasticity: influence of physical activity on cognition and brain function. Trends Cognitive Sci. 2007;11(8):342–348. doi:10.1016/j.tics.2007.06.009
23. Aguilar-Navarro SG, Mimenza-Alvarado AJ, Yeverino-Castro SG, et al. Cognitive frailty and aging: clinical characteristics, pathophysiological mechanisms, and potential prevention strategies. Archiv Med Res. 2025;56(1):103106. doi:10.1016/j.arcmed.2024.103106
24. He X, Jiao Y, Ma L, et al. The impact of exercise interventions on cognitive frailty: a scoping review of outcomes and biological mechanisms. Front Public Health. 2025;13:1738522. doi:10.3389/fpubh.2025.1738522
25. Lai X, Zhu H, Cai Y, et al. Effects of exercise-cognitive dual-task training on cognitive frailty in older adults: a randomized controlled trial. Front Aging Neurosci. 2025;17:1639245. doi:10.3389/fnagi.2025.1639245
26. Robertson DA, Savva GM, Kenny RA. Frailty and cognitive impairment--a review of the evidence and causal mechanisms. Ageing Res Rev. 2013;12(4):840–851. doi:10.1016/j.arr.2013.06.004
27. Iadecola C. The pathobiology of vascular dementia. Neuron. 2013;80(4):844–866. doi:10.1016/j.neuron.2013.10.008
28. Querido JS, Sheel AW. Regulation of cerebral blood flow during exercise. Sports Med. 2007;37(9):765–782. doi:10.2165/00007256-200737090-00002
29. Li W, Chen P, Li G, et al. Exercise and cognitive aging: a meta-analysis of macrovascular cerebral blood flow and cognitive function in older adults. J Gerontol Series A. 2025;80(8):glaf133.
30. Tao X, Chen Y, Zhen K, et al. Effect of continuous aerobic exercise on endothelial function: a systematic review and meta-analysis of randomized controlled trials. Front Physiol. 2023;14:1043108.
31. Gong XG, Wang LP, Yang LL, et al. Effects of Baduanjin exercise on cognitive impairment in older adults: a systematic review and meta-analysis. Front Public Health. 2025;13:1586011. doi:10.3389/fpubh.2025.1586011
32. Martín-Maestro P, Gargini R, García E, et al. Mitophagy failure in APP and Tau overexpression model of Alzheimer’s disease. J Alzheimer’s Dis. 2019;70(2):525–540. doi:10.3233/JAD-190086
33. Thomas AG, Dennis A, Bandettini PA, et al. The effects of aerobic activity on brain structure. Front Psychol. 2012;3:86. doi:10.3389/fpsyg.2012.00086
34. Eichenbaum H. The role of the hippocampus in navigation is memory. J Neurophysiol. 2017;117(4):1785–1796. doi:10.1152/jn.00005.2017
35. Herold F, Hamacher D, Schega L, et al. Thinking while moving or moving while thinking - concepts of motor-cognitive training for cognitive performance enhancement. Front Aging Neurosci. 2018;10:228. doi:10.3389/fnagi.2018.00228
36. Gleeson M, Bishop NC, Stensel DJ, et al. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev. 2011;11(9):607–615. doi:10.1038/nri3041
37. Cotman CW, Berchtold NC, Christie LA. Exercise builds brain health: key roles of growth factor cascades and inflammation. Trends Neurosci. 2007;30(9):464–472. doi:10.1016/j.tins.2007.06.011
38. Montero-Odasso M, Verghese J, Beauchet O, et al. Gait and cognition: a complementary approach to understanding brain function and the risk of falling. J Am Geriatrics Soc. 2012;60(11):2127–2136. doi:10.1111/j.1532-5415.2012.04209.x
39. Lauenroth A, Ioannidis AE, Teichmann B. Influence of combined physical and cognitive training on cognition: a systematic review. BMC Geriatrics. 2016;16:141. doi:10.1186/s12877-016-0315-1
40. Cadore EL, Rodríguez-Mañas L, Sinclair A, et al. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic review. Rejuvenation Res. 2013;16(2):105–114. doi:10.1089/rej.2012.1397
41. Niendam TA, Laird AR, Ray KL, et al. Meta-analytic evidence for a superordinate cognitive control network subserving diverse executive functions. Cognitive Affect Behav Neurosci. 2012;12(2):241–268. doi:10.3758/s13415-011-0083-5
42. Doyon J, Benali H. Reorganization and plasticity in the adult brain during learning of motor skills. Curr Opin Neurobiol. 2005;15(2):161–167. doi:10.1016/j.conb.2005.03.004
43. Li R, Zhu X, Yin S, et al. Multimodal intervention in older adults improves resting-state functional connectivity between the medial prefrontal cortex and medial temporal lobe. Front Aging Neurosci. 2014;6:39. doi:10.3389/fnagi.2014.00039
44. Iadecola C. The neurovascular unit coming of age: a journey through neurovascular coupling in health and disease. Neuron. 2017;96(1):17–42. doi:10.1016/j.neuron.2017.07.030
45. Citri A, Malenka RC. Synaptic plasticity: multiple forms, functions, and mechanisms. Neuropsychopharmacol. 2008;33(1):18–41. doi:10.1038/sj.npp.1301559
46. Stillman CM, Cohen J, Lehman ME, et al. Mediators of physical activity on neurocognitive function: a review at multiple levels of analysis. Front Human Neurosci. 2016;10:626. doi:10.3389/fnhum.2016.00626
47. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446. doi:10.1016/S0140-6736(20)30367-6
48. Cadore EL, Casas-Herrero A, Zambom-Ferraresi F, et al. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. Age. 2014;36(2):773–785. doi:10.1007/s11357-013-9586-z
49. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatrics Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
50. Ciesielska N, Sokołowski R, Mazur E, et al. Is the montreal cognitive assessment (MoCA) test better suited than the mini-mental state examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatria Polska. 2016;50(5):1039–1052. doi:10.12740/PP/45368
51. Rossi PG, Carnavale BF, Farche ACS, et al. Effects of physical exercise on the cognition of older adults with frailty syndrome: a systematic review and meta-analysis of randomized trials. Archiv Gerontol Geriatric. 2021;93:104322. doi:10.1016/j.archger.2020.104322
52. Luo H, Zheng Z, Yuan Z, et al. The effectiveness of multicomponent exercise in older adults with cognitive frailty: a systematic review and meta-analysis. Archiv Public Health. 2024;82(1):229. doi:10.1186/s13690-024-01441-y
53. Cadore EL, Sáez de Asteasu ML, Izquierdo M. Multicomponent exercise and the hallmarks of frailty: considerations on cognitive impairment and acute hospitalization. Experim Gerontol. 2019;122:10–14. doi:10.1016/j.exger.2019.04.007
54. Liu X, Chen L, Wei Z, et al. A retrospective controlled study on the effects of four-limb linkage training on clinical efficacy and antioxidative mechanisms in patients with chronic obstructive pulmonary disease. Int J Chronic Obstruct Pulmonary Dis. 2026;21:576646. doi:10.2147/COPD.S576646
55. Izquierdo M. Multicomponent exercise strategies for improving health outcomes. In: Uribarri J, Vassalotti JA, editors. Nutrition, Fitness, and Mindfulness: An Evidence-Based Guide for Clinicians. Cham: Springer Nature Switzerland; 2025:177–192.
56. Sirikul W, Buawangpong N, Pinyopornpanish K, et al. Impact of multicomponent exercise and nutritional supplement interventions for improving physical frailty in community-dwelling older adults: a systematic review and meta-analysis. BMC Geriatrics. 2024;24(1):958. doi:10.1186/s12877-024-05551-8
57. Gothe NP, Kramer AF, McAuley E. The effects of an 8-week Hatha yoga intervention on executive function in older adults. J Gerontol. 2014;69(9):1109–1116. doi:10.1093/gerona/glu095
58. Robinson TL, Gogniat MA, Miller LS. Frailty and cognitive function in older adults: a systematic review and meta-analysis of cross-sectional studies. Neuropsychol Rev. 2022;32(2):274–293. doi:10.1007/s11065-021-09497-1
59. De Las Heras B, Rodrigues L, Cristini J, et al. Measuring neuroplasticity in response to cardiovascular exercise in people with stroke: a critical perspective. Neurorehabil Neural Repair. 2024;38(4):303–321. doi:10.1177/15459683231223513
60. Kwan RYC, Liu J, Sin OSK, et al. Effects of virtual reality motor-cognitive training for older people with cognitive frailty: multicentered randomized controlled trial. J Med Internet Res. 2024;26:e57809. doi:10.2196/57809
61. Wei X, Huang C, Ding X, et al. Effect of virtual reality training on dual-task performance in older adults: a systematic review and meta-analysis. J Neuroengineer Rehabil. 2025;22(1):141. doi:10.1186/s12984-025-01675-z
62. Dobie K, Barr CJ, George S, et al. A systematic review of assessment tools for cognitive frailty: use, psychometric properties, and clinical utility. J Frailty Aging. 2025;14(2):100033. doi:10.1016/j.tjfa.2025.100033
63. Bu Z, Huang A, Xue M, et al. Cognitive frailty as a predictor of adverse outcomes among older adults: a systematic review and meta-analysis. Brain Behav. 2021;11(1):e01926. doi:10.1002/brb3.1926
64. Mantovani E, Zucchella C, Schena F, et al. Towards a redefinition of cognitive frailty. J Alzheimer’s Dis. 2020;76(3):831–843. doi:10.3233/JAD-200137
65. Hacke C, Schreiber J, Weisser B. Application of the templates TIDieR and CERT reveal incomplete reporting and poor replicability of exercise interventions for type 2 diabetes mellitus. Curr Diab Rev. 2022;18(4):e250821195838. doi:10.2174/1871525719666210825150957
66. Gallou-Guyot M, Perrochon A, Marie R, et al. Measured and perceived exercise intensity during the performance of single-task, cognitive-motor dual-task, and exergame training: transversal study. JMIR Serious Games. 2023;11:e36126. doi:10.2196/36126
67. Bünzen C, Knuth J, Bucher M, et al. CORE-CERT items as a minimal requirement for replicability of exercise interventions: results from application to exercise studies for breast cancer patients. J Strength Condition Res. 2023;37(5):e346–e360. doi:10.1519/JSC.0000000000004396
68. Li X, Zhang Y, Tian Y, et al. Exercise interventions for older people with cognitive frailty-a scoping review. BMC Geriatrics. 2022;22(1):721. doi:10.1186/s12877-022-03370-3
69. Blasco-Lafarga C, Cordellat A, Forte A, et al. Short and long-term trainability in older adults: training and detraining following two years of multicomponent cognitive-physical exercise training. Int J Environm Res Public Health. 2020;17(16):5984.
70. Schweda S, Munz B, Burgstahler C, et al. Proof of concept of a 6-month person-oriented exercise intervention ‘MultiPill-Exercise’ among patients at risk of or with multiple chronic diseases: results of a one-group pilot trial. Int J Environ Res Public Health. 2022;19(15). doi:10.3390/ijerph19159469
71. Ward DD, Flint JP, Littlejohns TJ, et al. Frailty trajectories preceding dementia in the US and UK. JAMA Neurol. 2025;82(1):61–71. doi:10.1001/jamaneurol.2024.3774
72. Nader MM, Cosarderelioglu C, Miao E, et al. Navigating and diagnosing cognitive frailty in research and clinical domains. Nat Aging. 2023;3(11):1325–1333. doi:10.1038/s43587-023-00504-z
73. Sugimoto T, Arai H, Sakurai T. An update on cognitive frailty: its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatric Gerontol Int. 2022;22(2):99–109. doi:10.1111/ggi.14322
74. Timmons S, Faherty M, Curtin C, et al. Cognitive frailty: a useful concept or a source of confusion? Insights from a survey of European geriatricians. BMC Geriatrics. 2025;25(1):280. doi:10.1186/s12877-025-05930-9
75. Yu T, Ding Q, Wang N, et al. Cranial repair-promoting effect of oxidised sodium alginate/amino gelatine injectable hydrogel loaded with deer antler blood peptides. Int J Biol Macromol. 2025;305(Pt 1):141116. doi:10.1016/j.ijbiomac.2025.141116
76. Eren TK, Aktaş E, Kaptan AY, et al. Recurrent anterior shoulder instability in patients 40-60 years old. Accompanying injuries and patient outcomes of arthroscopic repair. J Orthopaedic Sci. 2021;26(4):584–588. doi:10.1016/j.jos.2020.05.005
77. Zhang Z, Wang J, Qiao X, et al. Multicomponent exercise interventions for cognitive function in patients with mild cognitive impairment: a summary of best evidence. Front Rehabil Sci. 2025;6:1696284.
78. Ben Ezzdine L, Dhahbi W, Dergaa I, et al. Physical activity and neuroplasticity in neurodegenerative disorders: a comprehensive review of exercise interventions, cognitive training, and AI applications. Front Neurosci. 2025;19. doi:10.3389/fnins.2025.1502417
79. Reparaz-Escudero I, Izquierdo M, Bischoff-Ferrari HA, et al. Effect of long-term physical exercise and multidomain interventions on cognitive function and the risk of mild cognitive impairment and dementia in older adults: a systematic review with meta-analysis. Ageing Res Rev. 2024;100:102463. doi:10.1016/j.arr.2024.102463
80. Varela-Vásquez LA, Minobes-Molina E, Jerez-Roig J. Dual-task exercises in older adults: a structured review of current literature. J Frailty Sarcopenia Falls. 2020;5(2):31–37. doi:10.22540/JFSF-05-031
81. Torre MM, Langeard A, Hugues N, et al. Comparison of three physical-cognitive training programs in healthy older adults: a study protocol for a monocentric randomized trial. Brain Sci. 2021;11(1). doi:10.3390/brainsci11010066
82. Metsemakers WJ, Handojo K, Reynders P, et al. Individual risk factors for deep infection and compromised fracture healing after intramedullary nailing of tibial shaft fractures: a single centre experience of 480 patients. Injury. 2015;46(4):740–745. doi:10.1016/j.injury.2014.12.018
83. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psycholog Sci. 2003;14(2):125–130. doi:10.1111/1467-9280.t01-1-01430
84. Northey JM, Cherbuin N, Pumpa KL, et al. Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. British J Sports Med. 2018;52(3):154–160. doi:10.1136/bjsports-2016-096587
85. Ferrer-Ramos P, Garnacho-Castaño MV, Girabent-Farrés M, et al. Physical performance tests for preliminary cognitive screening in older adults: a systematic review of strength, walking, and balance assessments. Archiv Gerontol Geriatrics. 2025;130:105722. doi:10.1016/j.archger.2024.105722
86. Hernandez-Martinez J, Ramos-Espinoza F, Muñoz-Vásquez C, et al. Effects of active exergames on physical performance in older people: an overview of systematic reviews and meta-analysis. Front Public Health. 2024;12:1250299. doi:10.3389/fpubh.2024.1250299
87. Gavelin HM, Dong C, Minkov R, et al. Combined physical and cognitive training for older adults with and without cognitive impairment: a systematic review and network meta-analysis of randomized controlled trials. Ageing Res Rev. 2021;66:101232. doi:10.1016/j.arr.2020.101232
88. Martín-Rodríguez A, Dalamitros AA, Madrigal-Cerezo R, et al. Move to remember: the role of physical activity and exercise in preserving and enhancing cognitive function in aging-a narrative review. Geriatrics. 2025;10(6):143.
89. Esmaeilzadeh S, Kumpulainen S, Pesola AJ. Strength-cognitive training: a systemic review in adults and older adults, and guidelines to promote “strength exergaming” innovations. Front Psychol. 2022;13:855703. doi:10.3389/fpsyg.2022.855703
90. Sun G, Ding X, Zheng Z, et al. Effects of exercise interventions on cognitive function in patients with cognitive dysfunction: an umbrella review of meta-analyses. Front Aging Neurosci. 2025;17:1553868. doi:10.3389/fnagi.2025.1553868
91. Liu H, Sun Z, Zeng H, et al. Meta-analysis of the effects of multi-component exercise on cognitive function in older adults with cognitive impairment. Front Aging Neurosci. 2025;17:1551877.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.