Back to Journals » Journal of Asthma and Allergy » Volume 19
Formaldehyde Allergy Presenting with Anaphylaxis Due to Prolonged Immediate-Type Reaction
Authors Masumitsu H, Oshikata C, Takaoka S, Nakashima T, Matsunaga K, Kodama Y, Terada K, Yamashita Y, Miyasaka A, Muraoka T, Masumoto N, Kaneko T, Tsurikisawa N ![]()
Received 11 March 2026
Accepted for publication 2 June 2026
Published 8 June 2026 Volume 2026:19 608431
DOI https://doi.org/10.2147/JAA.S608431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Hinako Masumitsu,1 Chiyako Oshikata,1 Sachiko Takaoka,1 Takuya Nakashima,1 Kaho Matsunaga,1 Yuka Kodama,1 Kosuke Terada,1 Yuga Yamashita,1,2 Atsushi Miyasaka,1 Tatsuya Muraoka,1 Nami Masumoto,1 Takeshi Kaneko,2 Naomi Tsurikisawa1,2
1Department of Respirology, National Hospital Organization Yokohama Medical Center, Yokohama, Japan; 2Department of Pulmonology, Yokohama City University Graduate School of Medicine, Yokohama, Kanagawa, Japan
Correspondence: Naomi Tsurikisawa, Department of Respirology, National Hospital Organization Yokohama Medical Center, 3-60-2 Harajuku, Totsuka-ku, Yokohama, 245-8575, Japan, Tel +81-45-851-2621, Fax +81-45-851-3902, Email [email protected]
Abstract: Formaldehyde is a low-molecular-weight chemical used as a disinfectant and in some dental materials. Although formaldehyde is a well-known cause of allergic contact dermatitis, systemic allergic reactions related to dental treatment are rare and may be overlooked, particularly when symptoms are delayed or overlap with pre-existing allergic diseases. Here we present the case of a 36-year-old woman with a history of allergic rhinoconjunctivitis, atopic bronchial asthma, and eosinophilic gastroenteritis who presented with recurrent systemic allergic symptoms after root canal treatment. Eight years earlier, she had experienced nausea and diarrhea during endodontic therapy, which were attributed to eosinophilic gastroenteritis. During subsequent dental procedures, she developed delayed-onset abdominal pain, watery diarrhea, facial edema, generalized urticaria, dyspnea, and impaired consciousness. She was diagnosed with anaphylaxis and successfully treated with epinephrine. Extensive allergological evaluations, including oral drug challenge tests and skin prick and intracutaneous tests for aspirin, antibiotics, local anesthetics, and multiple dental materials, were negative. In contrast, skin prick testing with formaldehyde-containing dental agents was positive, and serum formaldehyde-specific IgE antibodies were detected, leading to the diagnosis of formaldehyde-induced anaphylaxis. This case highlights formaldehyde-containing dental materials as an under-recognized cause of anaphylaxis. Delayed symptom onset and overlapping manifestations with underlying allergic diseases may contribute to diagnostic delay. Awareness of formaldehyde allergy is essential in patients with unexplained or recurrent allergic reactions after dental treatment.
Keywords: anaphylactic reaction, dental treatment, formaldehyde, root canal
Introduction
The most common allergic reactions in dental staff are allergies to latex, acrylates, and formaldehyde.1 Anaphylaxis associated with dental treatment is rare but potentially life-threatening. Although local anesthetics are most commonly suspected,2 dental materials themselves may be unrecognized allergens. Formaldehyde, a volatile low-molecular-weight chemical widely used in industry and medicine, remains a component of certain endodontic materials.3,4 Formaldehyde is a well-known cause of allergic contact dermatitis,5 particularly in women presenting with eczema of the hands or face.6,7 At high concentrations, it has direct toxic effects; however, as a reactive hapten, formaldehyde can induce allergic sensitization, leading predominantly to IgE-mediated reactions or contact dermatitis. IgE-mediated formaldehyde allergy has been most frequently reported in hemodialysis patients, resulting from repeated exposure to formaldehyde-sterilized medical devices.3,4
Immediate allergic reactions to formaldehyde- or paraformaldehyde-containing root canal compounds have been reported in the dental literature,8 typically manifesting as anaphylaxis,9,10 shock,11,12 or generalized urticaria.8,13 During endodontic procedures, these agents are applied within the root canal; experimental studies have demonstrated that they are not completely confined to the canal space but can diffuse through dentinal tubules and the apical foramen, eventually entering the systemic circulation.14
Notably, formaldehyde-induced type I allergic reactions following dental treatment can occur not only within 1 h but also several hours after exposure, representing a delayed onset compared with typical immediate hypersensitivity reactions.9,13 Furthermore, previous reports have shown a marked discrepancy between serological and skin test results, with formaldehyde-specific IgE antibodies frequently detected despite negative skin prick tests.13,15
We have performed challenge tests using local anesthetics, antibiotics, dental fillings, and other drugs known to be common causes of anaphylaxis during dental treatment, and have experienced cases in which the diagnosis was ultimately formaldehyde-induced anaphylaxis. Here, we report a case of formaldehyde-induced anaphylaxis in which sensitization developed over an extended period of 8 years, and severe systemic reactions occurred after two root canal treatment sessions performed 50 h apart. The precisely documented temporal course highlights the risk of diagnostic delay and repeated exposure, underscoring the need for heightened clinical awareness of dental materials as potential causes of anaphylaxis.
The Ethics Committee of National Hospital Organization Yokohama Medical Center approved the allergen identification studies (skin prick tests and oral/subcutaneous provocation tests) reported herein, and written informed consent was obtained from the patient prior to allergen challenges. Human Subject Protection Committee approvals were obtained at the National Hospital Organization Yokohama Medical Center (2022–03) for the retrospective review of existing medical records. The study was performed in accordance with the tenets of the Declaration of Helsinki.
Case Presentation
The 36-year-old woman whose case is presented here was diagnosed with allergic rhinoconjunctivitis when she was 2 years of age. At 35 years of age, she developed atopic bronchial asthma and eosinophilic gastroenteritis and was treated with 800 µg inhaled fluticasone propionate and 10 mg montelukast. Although her asthma was well controlled with inhaled corticosteroids, she occasionally developed abdominal pain and diarrhea related to eosinophilic gastroenteritis. Eight years earlier, at 28 years of age, she had developed nausea and frequent episodes of diarrhea during a 4-month course of root canal treatment. At the age of 36 years, she had undergone weekly root canal treatment for 3 months starting in May of that year. Two months later, in October, she underwent root canal treatment again, developing abdominal pain immediately after the procedure. One hour later, she experienced watery diarrhea, with facial edema appearing 18 h later. The abdominal pain persisted for more than 30 h. Fifty hours after her last root canal treatment, she underwent a second root canal procedure. Thirty minutes later, her abdominal pain was further exacerbated, with generalized urticaria developing after 3 h, followed by dyspnea and impaired consciousness 5 h after the procedure (Figure 1). She presented to the emergency department, where she was diagnosed with anaphylaxis and treated with subcutaneous epinephrine, resulting in clinical improvement.
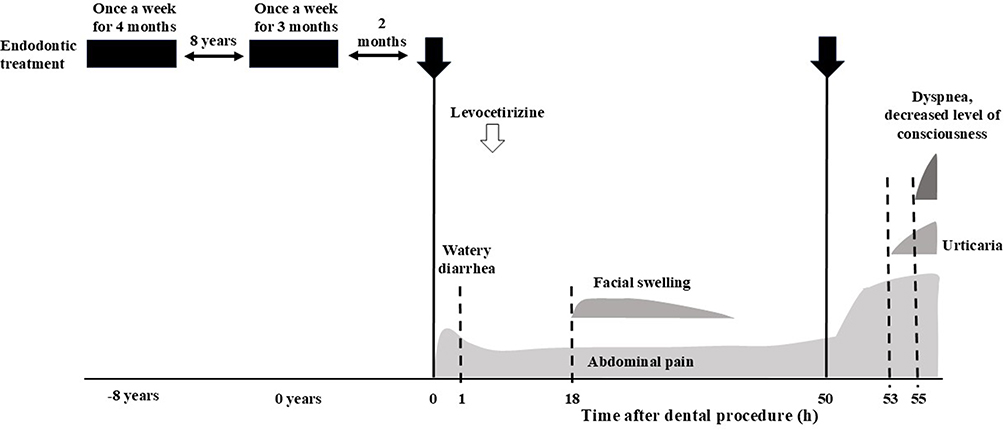 |
Figure 1 The patient’s clinical course from a 4-month course of endodontic treatment at 28 years of age to the onset, 8 years later, of the current anaphylactic symptoms. Black downward-facing arrows and bars indicate endodontic treatment. Shaded areas represent the occurrence of each of the patient’s symptoms. The white arrow indicates the administration of antihistamines. |
To confirm the cause of anaphylaxis, drug challenge tests were performed for medications administered during or after the patient’s dental treatment.
Aspirin was administered orally in escalating doses of 30, 60, 120, 240, and 480 mg at 3-h intervals, and clinical responses were assessed.16 For antibiotics, including cefaclor, amoxicillin, clarithromycin, and levofloxacin, half the standard single dose was administered initially, followed by a full single dose 3 h later, with careful monitoring for allergic reactions (Table 1). For local anesthetics, including lidocaine (with epinephrine and without additive tested separately), procaine, and mepivacaine, skin prick tests were first performed (Table 2), followed by intracutaneous injection tests (Table 3). Skin prick tests were also performed for dental materials, namely hinokitiol, hydrocortisone acetate, rosin, ester gum, eugenol, hydrogen peroxide, ethanol, chloroform, and calcium hydroxide. In skin prick testing, histamine and normal saline were used as the positive and negative control, respectively. In the prick-to-prick tests for hinokitiol, rosin, ester gum, eugenol, ethanol, chloroform, and calcium hydroxide, the highest concentrations (undiluted stock solutions) were those actually used in dental treatments. Test solutions were subsequently prepared by serial 10-fold dilutions (1/10 and 1/100) of the undiluted stock solutions with normal saline. All prick-to-prick tests were conducted using these standardized dilutions. All challenge tests and skin prick tests for these medications and dental materials yielded negative results (Table 2).
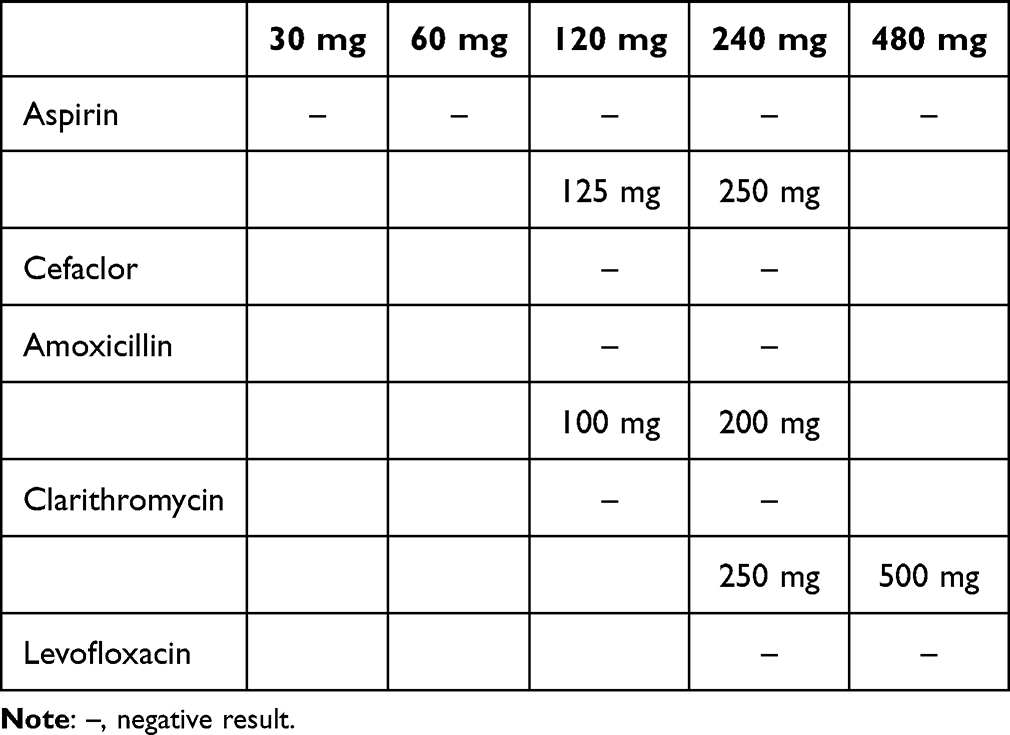 |
Table 1 Results of Oral Challenge Tests for Antibiotics |
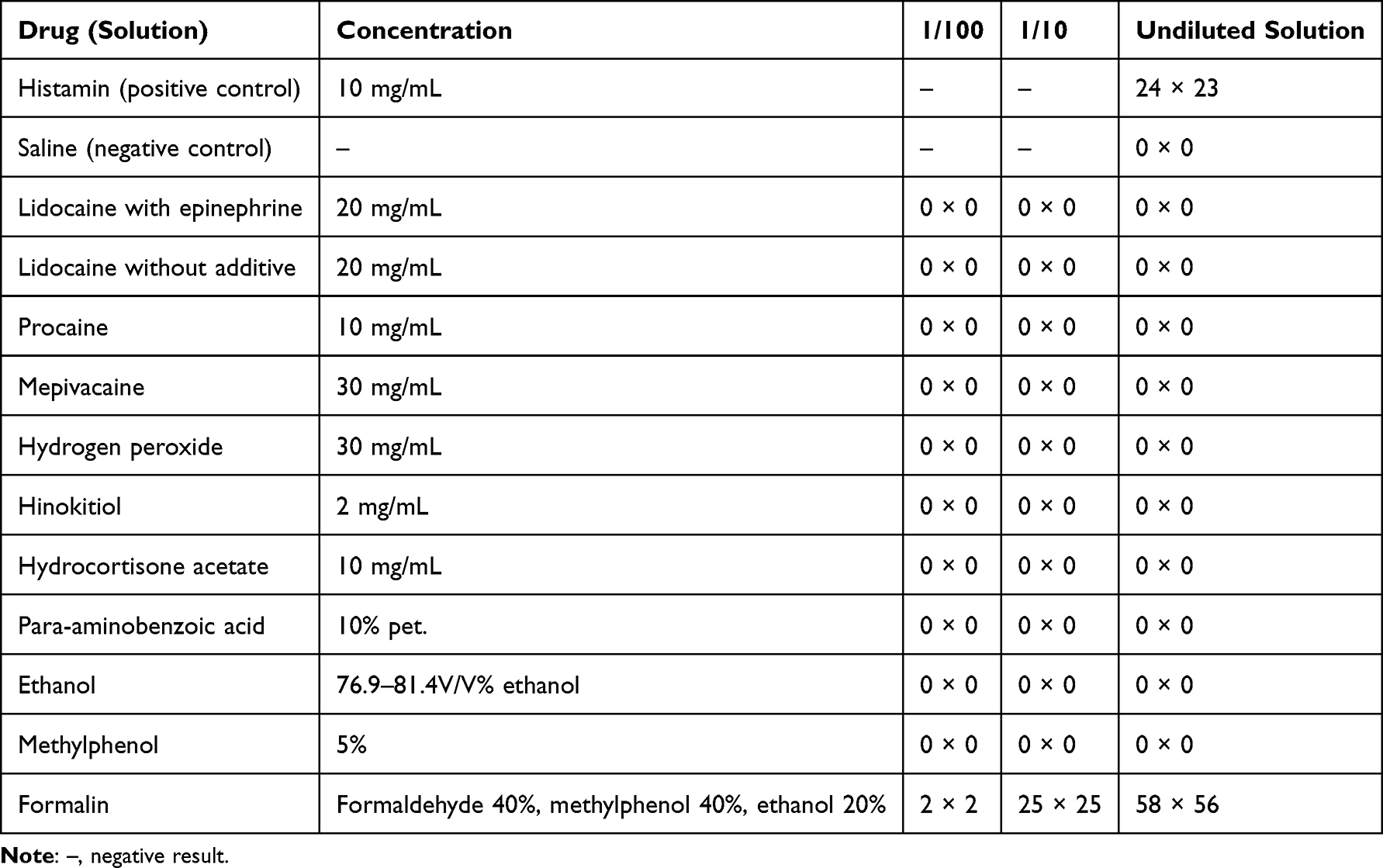 |
Table 2 Results of Skin Prick Tests for Drugs Used During Dental Treatment in This Patient |
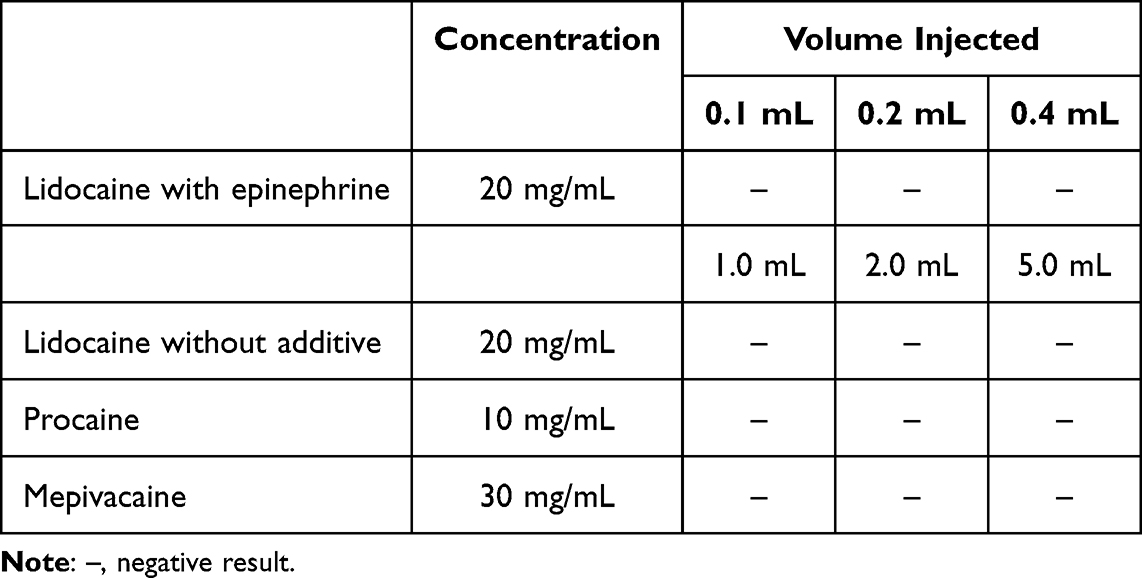 |
Table 3 Results of Intracutaneous Challenge Tests for Local Anesthetics |
To evaluate responses to agents used in dental treatment, skin prick tests were performed using a formalin solution containing formaldehyde, cresol (methylphenol), and ethanol, with histamine and normal saline used as the positive and negative control, respectively. Testing was conducted with an undiluted solution, defined as above, as well as with solutions diluted 1:10 and 1:100 in normal saline. The skin prick tests showed positive reactions to the 1:10 dilution of the formalin solution containing formaldehyde, methylphenol, and ethanol, and strongly positive reactions to the undiluted solution (Table 2 and Figure 2). Because the skin prick tests for ethanol and methylphenol alone were both negative (Table 2), the positive reaction to the formalin solution was considered to be attributable to formaldehyde (Figure 2).
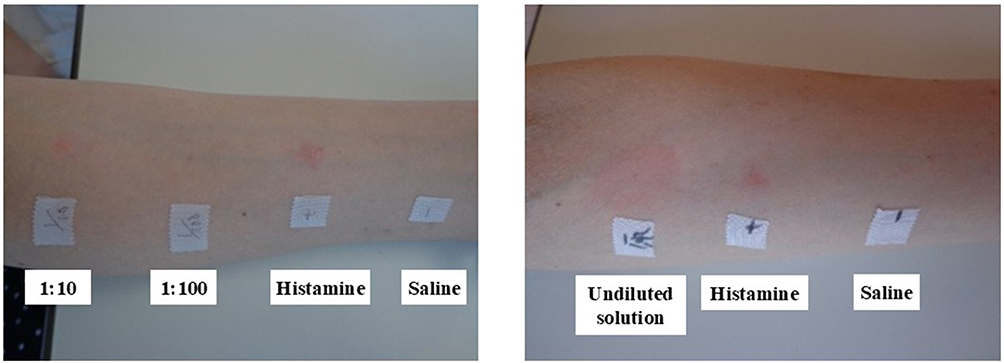 |
Figure 2 Skin prick tests for formalin solution containing formaldehyde (40%), methylphenol (40%), and ethanol (20%): Left, 1:10 and 1:100 dilutions; Right, undiluted solution. Histamine and normal saline were used as the positive and negative control, respectively. In skin prick tests, redness that was more widespread than that for the positive control (histamine) was judged to be a positive result. |
The patient’s total serum IgE level before the skin prick test was 88.0 IU/mL (normal range <232 IU/mL), as determined by ELISA and the nephelometry method using an Elecsys IgE II immunoassay (Cobas-e411; Roche Diagnostics, Tokyo, Japan).17 In addition, an ImmunoCAP fluorescence enzyme immunoassay (Thermo Fisher Scientific, Uppsala, Sweden)18 revealed that the patient had antigen-specific IgE antibodies against house dust mites (0.98 IU/mL) and formaldehyde (4.05 IU/mL; normal range <0.35 IU/mL). Based on these findings, she was diagnosed with formaldehyde-induced anaphylaxis.
After the diagnosis of formaldehyde-induced anaphylaxis, formaldehyde-containing dental materials were avoided during subsequent dental treatments. As a result, the frequency of abdominal pain and diarrhea decreased markedly, leading to an improvement in the patient’s quality of life.
Discussion
This case highlights a rare but clinically important cause of anaphylaxis associated with dental treatment: formaldehyde-containing endodontic materials.2 Although formaldehyde allergy has been reported previously,10,12,13 the present case is distinctive in that sensitization developed over an extended period of 8 years, and anaphylaxis occurred after repeated dental exposure within a short period of time. The precisely documented temporal course provides valuable insights into the clinical presentation and diagnostic challenges of formaldehyde-induced anaphylaxis. Formaldehyde-induced immediate hypersensitivity reactions related to dental procedures have been reported only sporadically.10,12,13 After injection of a high-concentration formalin solution into the root canal, it may leak continuously into the circulation over an extended period of time, potentially leading to delayed-onset immediate hypersensitivity reactions. In previous case reports of formaldehyde-induced allergic reactions associated with dental treatment, symptom onset occurred as late as 12 h after exposure.8,19 In the present case, the reactions that occurred 5–18 h after treatment were also delayed-onset immediate hypersensitivity reactions, supporting our proposed mechanism.
Consistent with previous reports, systemic manifestations such as gastrointestinal symptoms and urticaria were prominent in our patient, whereas respiratory compromise was not initially evident. These atypical presentations may contribute to the under-recognition of anaphylaxis, particularly when symptoms do not occur immediately after dental treatment. In the present case, abdominal pain and diarrhea developed or worsened 1 h after each of the two root canal treatments and persisted thereafter, followed by facial edema 18 h after the first procedure and impaired consciousness 5 h after the second procedure. Notably, the patient had been free from gastrointestinal symptoms for more than 2 months before the root canal treatment. Although the recurrence of gastrointestinal symptoms after both exposures to formaldehyde does not completely exclude the possibility of eosinophilic gastroenteritis, we considered these episodes to be more likely attributable to a formaldehyde-induced reaction.
Several factors contributed to the diagnostic delay in the present case. First, eosinophilic gastroenteritis has been observed in patients with atopic conditions, including those with bronchial asthma and food allergies, suggesting an atopy-linked eosinophilic phenotype across organ systems.20 Our patient had pre-existing allergic diseases, including bronchial asthma and eosinophilic gastrointestinal disorder, leading clinicians to attribute her recurrent symptoms to underlying comorbidities rather than exposure to a new allergen. Second, formaldehyde is often overlooked as a causative agent in dental-related allergic reactions, with local anesthetics and antibiotics more commonly suspected.2 Third, the delayed onset of symptoms in our patient, occurring several hours after exposure, further obscured the causal relationship with dental treatment. This case illustrates how repeated low-level exposure to formaldehyde may result in progressive sensitization and eventually provoke severe systemic reactions.
Our patient underwent a second root canal treatment 50 h after the first root canal treatment; however, neither the attending dentist nor the patient had recognized that the first root canal treatment had triggered an allergic reaction. The diagnosis was only established retrospectively, based on the clinical course.
The formalin solution containing formaldehyde, methylphenol, and ethanol that yielded a positive skin prick test result was the actual agent used during the patient’s dental treatment. The skin prick test was performed at the patient’s request to identify the causative antigen. According to the package insert, the agent is intended “for dental use only;” thus, skin testing in healthy persons represented off-label use of the compound. Therefore, skin testing in healthy controls could not be performed.
However, our patient had negative results to all other agents evaluated in the skin prick tests, with the positive control (histamine) eliciting an appropriate response. In addition, our patient was positive for formaldehyde-specific IgE antibodies. Taking all this into consideration, we consider the positive skin prick test result is unlikely to represent a nonspecific irritant reaction.
Previous studies have demonstrated that formaldehyde can diffuse beyond the root canal space and enter the systemic circulation, providing a plausible mechanism for systemic allergic reactions.14 Notably, the discrepancy between positive formaldehyde-specific IgE antibodies and negative skin prick test results, as reported in the literature,12 suggests that reliance on skin prick testing alone may lead to false-negative results. Thus, serological testing for formaldehyde-specific IgE may be particularly useful when formaldehyde allergy is suspected. As a low-molecular-weight substance, formaldehyde is believed to acquire antigenicity by binding to carrier proteins such as albumin. Its ability to bind to various proteins may result in heterogeneous antigen complexes, potentially explaining the variability observed in skin test reactivity and the complexity of both immediate- and delayed-type allergic reactions.15
From a clinical perspective, this case underscores the importance of considering dental materials as potential triggers of anaphylaxis in patients with unexplained allergic reactions. A detailed history of recent and past dental procedures, including the specific materials used during endodontic treatment, is essential. Increased awareness of formaldehyde-induced anaphylaxis may facilitate earlier diagnosis, prevent repeated exposure, and reduce the risk of life-threatening reactions.
Conclusion
Formaldehyde-containing dental materials can cause IgE-mediated anaphylaxis, even after prolonged sensitization and with delayed symptom onset. Pre-existing allergic diseases may obscure the causal relationship and contribute to diagnostic delay. Awareness of dental materials as potential allergens is essential to prevent repeated exposure and life-threatening reactions.
Consent for Publication
Written informed consent was obtained from this patient.
Author Contributions
Hinako Masumitsu: patient examination, construction of the figures and tables, and writing of the main document. Chiyako Oshikata, Sachiko Takaoka, Takuya Nakashima, Kaho Matsunaga, Kosuke Terada, Yuka Kodama, Yuga Yamashita, Atsushi Miyasaka, and Tatsuya Muraoka: patient examination and contributions to the discussion. Takeshi Kaneko: contributions to the discussion. Naomi Tsurikisawa: patient examination, construction of the figures and tables, discussion and revising the paper. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific funding.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Syed M, Chopra R, Sachdev V. Allergic reactions to dental materials- a systematic review. J Clin Diagn Res. 2015;9:ZE4–7.
2. Hascoët E, Mahé J, Meillard H, Théophile H, Cloitre A, Lesclous P. Anaphylactic reactions to local anesthetics in dental practice: a nationwide French retrospective study. Clin Oral Investig. 2022;26(2):1667–1676. doi:10.1007/s00784-021-04139-5
3. Maurice F, Rivory J-P, Larsson PH, et al. Anaphylactic shock caused by formaldehyde in a patient undergoing long-term hemodialysis. J Allergy Clin Immunol. 1986;77(4):594–597. doi:10.1016/0091-6749(86)90351-9
4. Bousquet J, Michal F-B. Allergy to formaldehyde and ethylene-oxide. Clin Rev Allergy. 1991;9(3–4):357–370. doi:10.1007/BF02802313
5. Latorre N, Silvestre JF, Monteagudo AF. Allergic contact dermatitis caused by formaldehyde and formaldehyde releasers. Actas Dermosifiliogr. 2011;102(2):86–97. doi:10.1016/j.ad.2010.09.004
6. Cronin E. Formaldehyde is a significant allergen in women with hand eczema. Contact Dermatitis. 1991;25(5):276–282. doi:10.1111/j.1600-0536.1991.tb01874.x
7. Agner T, Flyvholm MA, Menné T. Formaldehyde allergy: a follow-up study. Am J Contact Dermat. 1999;10(1):12–17. doi:10.1016/S1046-199X(99)90088-X
8. Tas E, Pletscher M, Bircher AJ. IgE mediated urticaria from formaldehyde in a dental root canal compound. J Investig Allergol Clin Immunol. 2002;12(2):130–133.
9. Kunisada M, Adachi A, Asano H, Horikawa T. Anaphylaxis due to formaldehyde released from root-canal disinfectant. Contact Dermatitis. 2002;47(4):215–218. doi:10.1034/j.1600-0536.2002.470405.x
10. Haïkel Y, Braun JJ, Zana H, Boukari A, de Blay F, Pauli G. Anaphylactic shock during endodontic treatment due to allergy to formaldehyde in a root canal sealant. J Endod. 2000;26(9):529–531. doi:10.1097/00004770-200009000-00011
11. Wantke F, Hemmer W, Haglmiiller T, Gotz M, Jarisch R. Anaphylaxis after dental treatment with a formaldehyde-containing tooth-filling material. Allergy. 1995;50(3):274–276. doi:10.1111/j.1398-9995.1995.tb01146.x
12. Braun JJ, Zana H, Purohit A, et al. Anaphylactic reactions to formaldehyde in root canal sealant after endodontic treatment: four cases of anaphylactic shock and three of generalized urticaria. Allergy. 2003;58(11):1210–1215. doi:10.1034/j.1398-9995.2003.00295.x
13. Kijima A, Nishino H, Umeda J, Kataoka Y. Type 1 allergy to formaldehyde in root canal sealant after dental treatment: two case reports and review of the literature. Arerugi. 2007;56(11):1397–1402.
14. Wemes JC, Purdell-Lewis D, Jongebloed W, et al. Diffusion of carbon-14-labeled formocresol and glutaraldehyde in tooth structures. Oral Surg Oral Med Oral Pathol. 1982;54(3):341–346. doi:10.1016/0030-4220(82)90107-4
15. Modre B, Ènke BK. Anaphylactic reaction to formaldehyde. Allergy. 2001;56(3):263–264. doi:10.1034/j.1398-9995.2001.056003263.x
16. Stevenson DD, Simon RA, Mathison DA. Aspirin‐sensitive asthma: tolerance to aspirin after positive oral aspirin challenges. J Allergy Clin Immunol. 1980;66(1):
17. Scalabrin DMF, Bavbek S, Perzanowski MS, et al. Use of specific IgE in assessing the relevance of fungal and dust mite allergens to atopic dermatitis: a comparison with asthmatic and nonasthmatic control subjects. J Allergy Clin Immunol. 1999;104(6):1273–1279. doi:10.1016/S0091-6749(99)70024-2
18. Kontis KJ, Valcour A, Patel A, et al. Correlation of the turbo-MP RIA with ImmunoCAP FEIA for determination of food allergen-specific immunoglobulin E. Ann Clin Lab Sci. 2006;36(1):79–87.
19. Ebner H, Kraft D. Formaldehyde-induced anaphylaxis after dental treatment? Contact Dermatitis. 1991;24(4):307–309. doi:10.1111/j.1600-0536.1991.tb01733.x
20. Park HS, Kim HS, Jang HJ. Eosinophilic gastroenteritis associated with food allergy and bronchial asthma. J Korean Med Sci. 1995;10(3):216–219. doi:10.3346/jkms.1995.10.3.216
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.