Back to Journals » International Medical Case Reports Journal » Volume 19
Foreign Body-Associated Eikenella corrodens Aspiration Pneumonia in an Elderly Immunocompetent Adult: A Case Report
Received 22 December 2025
Accepted for publication 5 March 2026
Published 17 March 2026 Volume 2026:19 591026
DOI https://doi.org/10.2147/IMCRJ.S591026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Thomas E Hutson
Anika Trudić,1,2,* Vladimir Stojšić3,4,*
1Department of Microbiology with Parasitology and Immunology, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia; 2Department for Microbiology, Institute for Pulmonary Diseases of Vojvodina, Sremska Kamenica, Serbia; 3Department of Internal Medicine, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia; 4Department for Thoracic Oncology, Institute for Pulmonary Diseases of Vojvodina, Sremska Kamenica, Serbia
*These authors contributed equally to this work
Correspondence: Anika Trudić, Department for Microbiology, Institute for Pulmonary Diseases of Vojvodina, Put doktora Goldmana 4, Sremska Kamenica, 21204, Serbia, Tel +381/21-480-5348, Email [email protected]
Background: Eikenella corrodens, a member of the HACEK group, is a fastidious Gram-negative bacillus that is part of the normal oropharyngeal microbiota and rarely causes lower respiratory tract infections. Pulmonary infections caused by E. corrodens are typically associated with predisposing factors such as aspiration, mucosal injury, or airway obstruction.
Case Presentation: We report the case of a 79-year-old woman without known immunosuppressive conditions who presented with a several-week history of productive cough and progressive respiratory symptoms. The initial clinical evaluation and chest radiography findings were nonspecific. Subsequent chest computed tomography (CT) revealed left lower lobe consolidation and bilateral apical bronchiolitis. Flexible bronchoscopy revealed a whitish-yellow, plant-derived endobronchial foreign body causing near-complete obstruction of the basal segmental bronchus with purulent secretions distally. Following bronchoscopic removal, a bronchial aspirate collected immediately after extraction yielded E. corrodens in pure culture (> 105 CFU/mL), supporting true lower respiratory infection rather than contamination. Histopathological examination confirmed the presence of organic foreign material. The isolate was susceptible to all tested beta-lactams, fluoroquinolones, tetracycline, and co-trimoxazole, and resistant to azithromycin. Susceptibility-guided therapy based on susceptibility testing resulted in clinical and radiological improvement.
Conclusion: This case highlights the diagnostic value of bronchoscopy in persistent focal pneumonia and underscores that isolation of E. corrodens in pure culture from appropriately collected lower respiratory specimens should prompt careful evaluation for aspiration or airway obstruction.
Keywords: Eikenella corrodens, HACEK group, foreign body aspiration, aspiration pneumonia
Introduction
Eikenella corrodens (E. corrodens) is a facultative anaerobic, non-motile, Gram-negative, non-spore-forming rod that belongs to the family Neisseriaceae. It exhibits a slow growth rate, which is mainly attributed to its high nutritional requirement. In the clinical microbiology context, E. corrodens is recognized as a member of the HACEK group, together with Haemophilus spp., Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, and Kingella kingae, which are organisms most commonly associated with infective endocarditis but also cause a wide range of infections.1,2
This fastidious Gram-negative bacterium is commonly found in the human oral and upper respiratory tract microbiota. Therefore, the isolation of E. corrodens from lower respiratory tract specimens must be interpreted with caution because contamination from oropharyngeal flora is possible, particularly when mixed cultures are recovered. Pulmonary infections due to E. corrodens are uncommon, with only sporadic case reports and small case series described in the literature, and no large epidemiological studies defining their incidence. Predisposing factors include immunosuppression, mucosal disruption, dental diseases or procedures, and substance abuse.1,3
Although the virulence mechanisms of E. corrodens have not been fully characterized, biofilm formation and persistence in anaerobic environments may contribute to infection in settings of mucosal disruption or foreign-body retention.4 Despite these properties, E. corrodens is generally regarded as an organism of low virulence. Clinically relevant lower respiratory tract infections typically occur in the presence of local predisposing conditions such as aspiration, mucosal injury, or airway obstruction. These characteristics may help explain its involvement in foreign-body–associated pulmonary infections, in which adherent biofilm-forming bacteria may evade host immune clearance and establish a localized nidus of infection.
Tracheobronchial foreign-body aspiration is a potentially life-threatening event most frequently encountered in children and older adults. Although bronchoscopic removal generally prevents permanent airway damage, diagnosis may be delayed when the clinical symptoms are subtle, nonspecific, or atypical. In adults, this condition represents a small but clinically important proportion of airway emergencies, particularly among older patients, in whom diagnosis is frequently delayed.5 Foreign-body aspiration in adults is often underrecognized, as the initial aspiration event may be unwitnessed and symptoms can be mild or nonspecific. Organic material may remain impacted for weeks, leading to delayed complications such as obstructive pneumonitis, recurrent bronchitis, or nonresolving pneumonia. Therefore, persistent focal pulmonary findings should prompt evaluation for an occult endobronchial foreign-body.
Here, we describe a case of aspiration pneumonia caused by E. corrodens in an elderly adult, confirmed by isolation in pure culture from a bronchial aspirate obtained immediately after foreign-body extraction. Adult foreign-body aspiration with microbiologically confirmed E. corrodens infection is rarely reported, and this case highlights the importance of distinguishing true lower respiratory infection from oropharyngeal contamination.
Case Report
A 79-year-old woman presented with a several-week history of cough and production of thick clear sputum accompanied by profuse watery nasal discharge. Her medical history included stable angina pectoris, arterial hypertension, endoscopic colorectal polyp removal, and deep vein thrombosis of the right lower extremity. She had been treated for pneumonia on multiple occasions, most recently affecting the left lung, six months prior to the current illness.
On physical examination, the patient was alert, oriented, afebrile, normocardic, and mildly dyspneic. Arterial blood gas analysis revealed hypoxemic respiratory failure (Type I), which did not require supplemental oxygen therapy. Routine laboratory testing did not reveal a clear systemic inflammatory response at the initial presentation, and no systemic signs of infection were present. Pulmonary auscultation was unremarkable. Spirometry revealed a mild obstructive ventilatory defect. A chest radiograph showed obliteration of the left costophrenic angle and poor delineation of the left hemidiaphragm, without clear parenchymal consolidation (Figure 1). The patient was treated with bronchodilator inhalation therapy and intranasal corticosteroids.
 |
Figure 1 Initial chest radiograph of the patient. Frontal chest radiograph demonstrating blunting of the left costophrenic angle and subtle obscuration of the left hemidiaphragm, findings suggestive of an early left lower lobe infiltrate with a small associated pleural effusion. |
Six weeks later, the patient returned with clinical deterioration, reporting worsening cough and increased sputum production. Chest computed tomography (CT) demonstrated bilateral apical bronchiolitis, which was more pronounced on the right side, and an area of consolidation and/or atelectasis in the left lower lobe (Figure 2). These findings were consistent with subtle abnormalities observed on the initial chest radiograph, including poor delineation of the left hemidiaphragm and blunting of the costophrenic angle, suggestive of an early left lower lobe infiltrate. A small left-sided pleural effusion and borderline mediastinal lymphadenopathy were also noted. Although CT did not demonstrate a definite endobronchial lesion, the persistence of focal left lower lobe consolidation despite initial conservative management, and the absence of marked systemic inflammatory response, raised concern for alternative etiologies. Differential considerations included unresolved pneumonia, obstructive pneumonitis, or an endobronchial lesion. Diagnostic bronchoscopy was therefore indicated to exclude airway obstruction or neoplastic pathology.
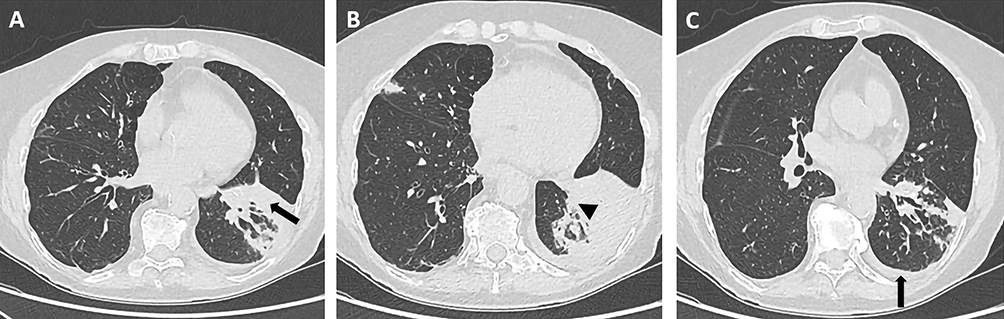 |
Figure 2 Initial chest CT scan prior to bronchoscopy. (A–C) Representative axial CT images at different thoracic levels. (A) Focal consolidation in the left lower lobe (arrow). (B) Near-complete endobronchial obstruction of the basal segmental bronchus of the left lower lobe (arrowhead). (C) Small left-sided pleural effusion (arrow). |
Flexible bronchoscopy was performed under sedation at the Institute for Pulmonary Diseases of Vojvodina, a tertiary care center in Serbia. Inspection of the larynx, trachea, carina, and right bronchial tree was unremarkable, as was evaluation of the left main bronchus and segmental bronchi of the left upper lobe. However, in the left lower lobe, a whitish-yellow cauliflower-like endobronchial mass was observed within the basal segmental bronchus, consistent with an aspirated foreign-body of biological origin. The lesion resulted in near-complete distal bronchial obstruction. Using endobronchial forceps, nearly the entire mass was mechanically extracted. The specimen was submitted for histopathological examination. After the extraction of the endobronchial mass and opening of the distal bronchial segments, copious amounts of purulent material began to drain from the periphery of the left lower lobe. Complete aspiration of purulent material was performed, followed by bronchoalveolar lavage. Bronchial aspirates were collected for microbiological analysis. After clearance, the underlying bronchial mucosa appeared markedly erythematous, edematous, and friable, without evidence of active bleeding.
Histopathological examination of the extracted material revealed mucopurulent exudates containing small bacterial colonies and food particles most likely of plant origin.
Microbiological Findings
Bronchial aspirate obtained immediately after foreign-body extraction was submitted for microbiological analysis. Direct Gram staining of the bronchial aspirate demonstrated abundant polymorphonuclear leukocytes and Gram-negative rods. The specimen was subsequently cultured on 5% sheep blood agar, chocolate agar, and MacConkey agar and incubated at 35–37°C in a CO2-enriched atmosphere. Routine mycological cultures showed no fungal growth, and mycobacterial cultures remained negative after 8 weeks of incubation. Dedicated anaerobic cultures are not routinely performed for bronchial aspirates in our laboratory practice.
After 24 hours of incubation, pinpoint-sized colonies appeared on blood agar. Quantitative culture demonstrated pure growth exceeding 105 CFU/mL. Gram staining revealed Gram-negative rods. Following an additional 24 hours of incubation, the colonies developed a dry, gray, translucent, non-hemolytic appearance, becoming rough, flat to slightly convex, with round-to-irregular margins. The colonies emitted a characteristic hypochlorite-like odor and were oxidase-positive and catalase-negative. These phenotypic features were consistent with E. corrodens.6 Final identification was performed using VITEK MS Prime (bioMérieux, France), a matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) system, which provided reliable species-level identification.7
Antimicrobial susceptibility results could not be interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) standards routinely applied in our microbiology laboratory, as EUCAST does not provide specific clinical breakpoints for E. corrodens. Therefore, susceptibility testing was performed and interpreted according to the CLSI M45 guidelines for infrequently isolated or fastidious organisms. Beta-lactamase production was assessed using a nitrocefin-based method and was not detected. The isolate was susceptible to all tested beta-lactams (penicillin, ampicillin, amoxicillin–clavulanic acid, ceftriaxone, and cefotaxime), fluoroquinolones (ciprofloxacin and levofloxacin), co-trimoxazole, and tetracycline and resistant to azithromycin.8
Given the bacteriological findings, the patient’s clinical status, and laboratory parameters, including mildly elevated inflammatory markers (CRP 16.6 mg/L, fibrinogen 7.4 g/L) without leukocytosis, suggesting a mild to moderate systemic inflammatory response, rather than severe acute infection, empiric dual antimicrobial therapy with levofloxacin and metronidazole was initiated to provide broad coverage for aspiration-associated pneumonia. Following microbiological identification of E. corrodens, an organism intrinsically resistant to metronidazole, metronidazole was discontinued and definitive therapy with levofloxacin (500 mg once daily) was continued based on in vitro susceptibility results. Probiotic supplementation and de-obstructive therapy were maintained. Given prompt source control through bronchoscopic removal and rapid clinical improvement, a 7-day course of therapy was considered adequate.
A follow-up chest CT performed six weeks after bronchoscopy, compared with the previous CT scan, demonstrated a significantly smaller area of consolidation in the left lower lobe and partial regression of the pleural effusion (Figure 3). The previously described borderline enlarged mediastinal lymph nodes persisted but were slightly smaller than those on the initial examination.
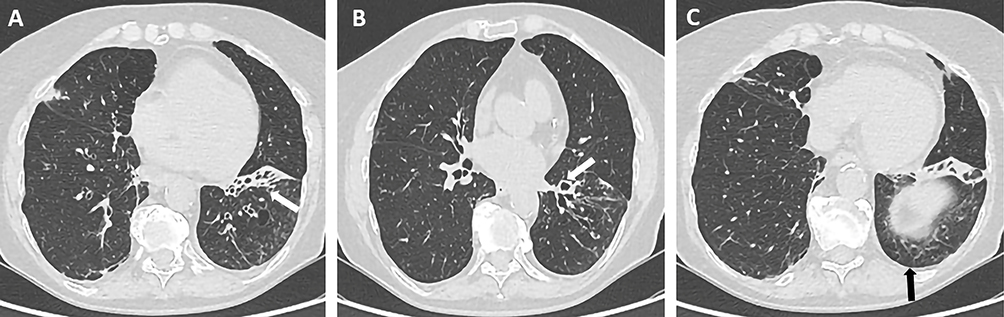 |
Figure 3 Follow-up chest CT scan six weeks after bronchoscopy. (A–C) Representative axial CT images at corresponding thoracic levels. (A) Marked reduction of left lower lobe consolidation (arrow). (B) Re-expansion of the previously obstructed basal segmental bronchus (arrow). (C) Partial regression of the left-sided pleural effusion (arrow). |
Discussion
Eikenella corrodens, a member of the HACEK group, is a fastidious organism that rarely causes pulmonary infection. Lower respiratory tract infections are uncommon and typically occur in the presence of predisposing factors such as aspiration, immunosuppression, or airway obstruction.9–12
Isolation of E. corrodens in the setting of foreign-body aspiration is infrequently reported, particularly in adults. Only two pediatric cases of complicated pneumonia following foreign-body aspiration have identified E. corrodens as the causative pathogen.13 In older adults diagnosed with pneumonia, age-related alterations in swallowing mechanics may be present, but remain clinically unrecognized. The frequent occurrence of microaspiration of saliva, together with the overlap between oropharyngeal and pulmonary microbiota, supports aspiration as a common and often underappreciated pathogenic mechanism.14 Subtle swallowing dysfunction and recurrent microaspiration may therefore contribute to such clinical presentations.
A limitation of this case is the absence of a clearly documented choking episode or witnessed aspiration event. Foreign-body aspiration in older adults may occur silently, particularly in the presence of subtle, clinically unrecognized swallowing dysfunction. The patient’s history of recurrent pneumonia likely reflects an underlying predisposition to intermittent microaspiration or repeated aspiration events. Furthermore, the subtle pleural effusion and early left lower lobe abnormalities observed on the initial chest radiograph could represent an early manifestation of the same aspiration-related process, although it remains uncertain whether these findings preceded or resulted from the aspiration event. A formal swallowing assessment was not performed in this patient. Nevertheless, evaluation for dysphagia may be warranted in similar presentations to better assess aspiration risk.
These considerations are particularly relevant in the present case, in which E. corrodens was isolated in pure culture from a bronchial aspirate obtained immediately after foreign-body extraction. This sampling approach substantially reduces the likelihood of oropharyngeal contamination and supports the diagnosis of true lower respiratory tract infection.
Although E. corrodens is part of the normal oropharyngeal microbiota, several findings in the present case support its etiological role rather than colonization or contamination. The organism was isolated in pure culture with significant quantitative growth (>105 CFU/mL) from a specimen obtained immediately after foreign-body extraction, minimizing the possibility of upper airway contamination. No additional bacterial species were isolated on standard aerobic media, and routine mycological and mycobacterial testing were negative. Direct Gram staining demonstrated Gram-negative rods consistent with the subsequent culture results, supporting microbiological concordance. Importantly, radiologic imaging showed focal consolidation distal to near-complete bronchial obstruction, and purulent secretions were observed at the site of obstruction during bronchoscopy. The concordant clinical and radiologic improvement following both mechanical source control and directed antimicrobial therapy strengthens the interpretation of E. corrodens as the causative pathogen in this setting. Moreover, mechanical obstruction by plant-derived material likely contributed to localized airway injury and impaired mucociliary clearance, thereby facilitating bacterial proliferation and a localized inflammatory response.15
This case highlights the importance of considering occult foreign-body aspiration in adults with persistent or unexplained pulmonary symptoms, particularly when fastidious or atypical organisms are recovered from the lower respiratory tract samples. In such settings, bronchoscopy is indispensable and plays both diagnostic and therapeutic roles.
Advances in diagnostic methodologies, particularly the implementation of MALDI-TOF mass spectrometry, have significantly improved the accuracy and speed of identification of fastidious organism such as E. corrodens. Despite these advances, standardized antimicrobial susceptibility testing remains limited. EUCAST does not currently provide specific clinical breakpoints for E. corrodens, whereas CLSI M45 offers guidance for susceptibility testing of infrequently isolated or fastidious organisms.8 Additionally, beta-lactamase-producing E. corrodens strains have been reported, and intrinsic resistance to clindamycin and metronidazole has been documented, underscoring the importance of appropriate antimicrobial selection.16,17 These resistance patterns are particularly relevant in aspiration-associated infections, where empirical anaerobic coverage may be ineffective against E. corrodens.
Given the limited number of cases and absence of standardized susceptibility testing guidelines, further studies are needed to better define the clinical spectrum, optimal diagnostic approach, and evidence-based management strategies for pulmonary infections caused by E. corrodens.
Conclusion
This case report describes an uncommon presentation of E. corrodens aspiration pneumonia associated with endobronchial foreign-body retention in an elderly adult patient without known immunosuppressive conditions. Nonspecific clinical and imaging findings may lead to diagnostic delays, particularly in the absence of a witnessed aspiration event or other obvious risk factors. The case emphasizes the diagnostic and therapeutic value of bronchoscopy in persistent focal pneumonia and underscores the clinical significance of isolating E. corrodens in pure culture from lower respiratory specimens. Careful interpretation of microbiological findings is essential to distinguish true lower respiratory infection from oropharyngeal colonization and to prompt evaluation for aspiration or airway obstruction.
Ethical Approval
Ethical approval for the publication of this case report was obtained from the Ethics Committee of the Institute for Pulmonary Diseases of Vojvodina, Sremska Kamenica, Serbia (Approval No. 40-10/2; date: December 2, 2025).
Informed Consent
The patient provided written informed consent for publication of their medical care details and associated images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any funding agencies or sponsors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li L, Shi YB, Weng XB. Eikenella corrodens infections in humans: report of six cases and review of literature. J Clin Lab Anal. 2022;36(2):e24230. doi:10.1002/jcla.24230
2. Khaledi M, Sameni F, Afkhami H, et al. Infective endocarditis by HACEK: a review. J Cardiothorac Surg. 2022;17(1):185. doi:10.1186/s13019-022-01932-5
3. Liang ZC, Ouyang H, Song XJ, et al. Eikenella corrodens isolated from pleural effusion: a case report. World J Clin Cases. 2024;12(18):3596–7. doi:10.12998/wjcc.v12.i18.3596
4. Jasin Mansur F, Takahara S, Yamamoto M, et al. Purification and characterization of hemolysin from periodontopathogenic bacterium Eikenella corrodens strain 1073. Biosci Biotechnol Biochem. 2017;81:1246–1253. doi:10.1080/09168451.2017.1295807
5. Kara K, Ozdemir C, Tural Onur S, Satici C, Tokgoz Akyil F, Nedime Sokucu S. Late diagnosis of foreign body aspiration in adults: case series and review of the literature. Respir Care. 2024;69(3):317–324. doi:10.4187/respcare.10723
6. Mühlhauser M. Eikenella corrodens. Rev Chilena Infectol. 2013;30(2):152–157. doi:10.4067/S0716-10182013000200007
7. Couturier MR, Mehinovic E, Croft AC, Fisher MA. Identification of HACEK clinical isolates by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol. 2011;49(3):1104–1106. doi:10.1128/JCM.01777-10
8. Clinical and Laboratory Standards Institute. Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria; Approved Guideline. Wayne, PA: CLSI; 2015. CLSI document M45-A3.
9. Goldstein EJ, Kirby BD, Finegold SM. Isolation of Eikenella corrodens from pulmonary infections. Am Rev Respir Dis. 1979;119(1):55–58. doi:10.1164/arrd.1979.119.1.55
10. Hsu CY, Liu LL, Luh KT. Lung abscess caused by Eikenella corrodens: report of a case. Taiwan Yi Xue Hui Za Zhi. 1989;88(8):828–831.
11. Easow JM, Joseph NM, Tuladhar R, Shivananda PG. Empyema caused by Eikenella corrodens. J Glob Infect Dis. 2011;3(3):309–311. doi:10.4103/0974-777X.83546
12. Hu L, Lin J, Li J, Cao Y, Lin L. Lung abscess secondary to lung cancer with Eikenella corrodens and Streptococcus anginosus: a case report. BMC Infect Dis. 2020;20(1):165. doi:10.1186/s12879-020-05054-y
13. Joseph L, Assous M, Dreifuss K, Goldberg S, Picard E. Complicated pediatric pneumonia with Eikenella caused by foreign body aspiration: institutional and literature review. Case Rep Infect Dis. 2025;2025:2857930. doi:10.1155/crdi/2857930
14. Yoshimatsu Y, Melgaard D, Westergren A, Skrubbeltrang C, Smithard DG. The diagnosis of aspiration pneumonia in older persons: a systematic review. Eur Geriatr Med. 2022;13(5):1071–1080. doi:10.1007/s41999-022-00689-3
15. Sane SM, Faerber EN, Belani KK. Respiratory foreign bodies and Eikenella corrodens brain abscess in two children. Pediatr Radiol. 1999;29(5):327–330. doi:10.1007/s002470050600
16. Lacroix JM, Walker C. Characterization of a beta-lactamase found in Eikenella corrodens. Antimicrob Agents Chemother. 1991;35(5):886–891. doi:10.1128/AAC.35.5.886
17. Goldstein EJ, Citron DM, Merriam CV, Warren YA, Tyrrell KL, Fernandez H. In vitro activities of a new des-fluoroquinolone, BMS 284756, and seven other antimicrobial agents against 151 isolates of Eikenella corrodens. Antimicrob Agents Chemother. 2002;46(4):1141–1143. doi:10.1128/AAC.46.4.1141-1143.2002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.