Back to Journals » Risk Management and Healthcare Policy » Volume 14
Food Safety Knowledge, Handling Practices and Associated Factors Among Food Handlers Working in Food Establishments in Debre Markos Town, Northwest Ethiopia, 2020: Institution-Based Cross-Sectional Study
Authors Alemayehu T, Aderaw Z, Giza M ![]() , Diress G
, Diress G ![]()
Received 6 December 2020
Accepted for publication 6 March 2021
Published 17 March 2021 Volume 2021:14 Pages 1155—1163
DOI https://doi.org/10.2147/RMHP.S295974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Tadege Alemayehu,1 Zewdie Aderaw,2 Mastewal Giza,3 Gedefaw Diress3
1East Gojjam Zone Health Department, Debre Markos, Ethiopia; 2Public Health Department, College of Medicine and Health Science, Debre Markos University, Debre Markos, Ethiopia; 3Public Health Department, College of Health Sciences, Woldia University, Woldia, Ethiopia
Correspondence: Gedefaw Diress PO box: 400 Tel +251913756945
Email [email protected]
Purpose: Foodborne illness is a major public health problem worldwide. The supply of safe and healthy food is crucial to prevent foodborne illness. However, evidence regarding food safety knowledge and handling practice is limited in Ethiopia. Therefore, this study aimed to assess food safety knowledge, handling practice, and its associated factors among food handlers in Debre Markos Town, North West Ethiopia.
Patients and Methods: An institutional-based cross-sectional study was conducted on 408 randomly selected food handlers at Debre-Markos town. A structured questionnaire and an observational checklist were used to collect relevant data. The main outcome of interest was food safety and handling practice. Multivariable logistic regression analysis was used to identify the factors significantly associated with food safety knowledge and food handling practice. Data were analyzed using SPSS version 25.
Results: In this study, only 34.1% of food handlers had good food safety knowledge and nearly 54% of food handlers had good food handling practice. Level of education (AOR = 0.23 (0.14– 0.57)), training on food safety (AOR = 5.13 (3.57– 7.82)), and favorable attitudes towards food safety (AOR=2.54 (1.52– 4.25)) were the factors associated with knowledge of food safety. Similarly, training (AOR=2.05, 95% CI=1.31– 3.19), a good level of knowledge (AOR: 1.68, 95% CI: 1.40, 3.17), and work experience (AOR = 1.24, 95% CI: 1.10– 2.81) were positively associated with good food handling practice.
Conclusion: In this study, the level of food safety knowledge and handling practices were relatively low. Therefore, the concerned bodies should work on the identified factors to improve food handlers’ knowledge of food safety and practice level. Continuous training for food handlers should be given.
Keywords: knowledge, practice, food safety, food establishment, Ethiopia
Introduction
Now a day’s food safety is the primary public health concern for many countries. According to World Health Organization (WHO), food safety is defined as the conditions and measures that are necessary during the production, processing, storage, distribution, and preparation of food to ensure that it is safe, sound, and wholesome, and fit for human consumption.1–3 Food safety is essential to prevent foodborne illness and enhance the well-being of humans.4 Globally, foodborne related illnesses have increased over the years and negatively affected the health and economic well-being of many developing and developed countries.5 Nowadays, lack of food safety measures is a major public health problem in many parts of the world.6,7
There is growing evidence that food safety has been neglected in developing countries.8 In developing countries, particularly in Africa, foodborne diseases may be an important contributor to gastrointestinal disease, and poor hygienic practices during food preparation, handling, and storage are one of the commonest causes of morbidity.5,8 In Sub-Saharan Africa, evidence indicates that morbidity and mortality related to lack of food safety are a constant threat to public health organizations.9,10 In Malaysia, by 2014, more than 50% of the total food poisoning cases were attributed to improper food handling by food handlers.11
In Ethiopia, around 70% of diarrheal disease is associated with the consumption of contaminated food.12 Approximately 10 to 20% of food-borne disease outbreaks are due to contamination by the food handler.13 The Federal Ministry of Health of Ethiopia acknowledges the depth of the problem by stating that communicable diseases, particularly diarrheal diseases and intestinal parasites, are the leading causes for outpatient attendance and causes of hospitalization most of which are attributed to poor food safety. Furthermore, many reported cases of food-borne viral diseases have been attributed to infected food-handlers involved in catering services.14,15
In Ethiopia, particularly in urban settings, eating and drinking in food establishments (hotels, restaurants, and snack bars) is common. These food establishments prepare, handle, and serve large quantities of food to large groups of people within a short period of time and implying a possible risk of contamination. Food handlers seem to be a major source and means of food contamination.4
Assessing and improving food-handlers knowledge on food safety and handling practice play a dominant role in ensuring strict adherence to food safety principles. Several cross-sectional studies on food safety knowledge and practices of food-handlers were conducted in the country.16–19 However, there is substantial heterogeneity in their finding. The magnitude of good food safety knowledge varied from 24.5% in Godey Town, East Ethiopia20 to 75.9% in Debarq Town, Northwest Ethiopia.16 Similarly, the magnitude of good food handling practice varied across the countries; 32.5% in Arbaminch, South Ethiopia,21 and 52.4% in Diredawa, East Ethiopia.22 Additionally, there are limited studies that used observation to investigate food handling practices. The majority of previous studies used self‐reported practices which may introduce bias in the study findings.
Therefore, in countries like Ethiopia, assessing food handlers’ level of food safety knowledge, handling practices and its determinants enable regulatory authorities to take evidence derived measures toward the provision of safe food to the consumer. Such studies will also offer a well understanding of the relations of essential food safety knowledge, attitudes, and practices of food handlers. Besides, there is no available evidence on the knowledge and practice of food handlers in food establishments in the northwest region of Ethiopia, particularly in Debre Markos town. Therefore, this study aimed to assess food safety knowledge, attitude, handling practice, and its associated factors among food handlers of food establishments in Debre Markos Town, North West Ethiopia.
Patients and Methods
Study Design, Period, and Setting
An institution-based cross-sectional study was conducted in Debre Markos town from September 2019 to October 2019. Debre Markos town is found in the Northwest of Ethiopia and located between 10°17′00′′ to 10°21′30′′ N Latitudes and 37°42′00′′ to 37°45′30′′ E longitude. It is 300 Kilometers far from Addis Ababa (the capital city of Ethiopia) and 265 Kilometers from Bahir Dar (the capital of Amhara National Regional State). The town consists of 11 Keble’s with 125,636 projected populations from the 2008 census; of which 66,832 are female and 58,804 male. There are 147 food establishments in the town with 3123 food handlers currently working in food establishments.23
Population and Eligibility Criteria
The source populations were all food handlers working in food establishments of Debre Markos Town. The study populations were food handlers currently working in selected food establishments in Debre Markos Town. Food handlers age ≥14—65 years working in preparation, cleaning and service areas of food establishments at the time of the study regardless of their sex and employment status were included in the study. However, Food handlers generally those who cannot answer due to serious illness (rather than food-related) at the time of intervention were excluded from the study.
Sample Size and Sampling Procedure
The required sample size was determined by using a single population proportion formula with the following assumption: 95% CI, 5% margin of error, and 80% power. We tried to calculate the sample size for each main objective by taking a proportion of good knowledge on food safety 90%, favorable attitude 93%, and good food handling practice 40.1% from previous studies.18,24 Finally, by considering 10% for non-response rate the required sample size is found to be 408.
The list of existing food establishments and the number of food handlers currently working in food establishments was obtained from the Federal Democratic Republic of Ethiopia private employee social security agency Debre-Markos branch. Based on social security agency data, in 2019, there are 147 food establishments and 3123 food handlers in Debre Markos town. Initially, of a total of 147 food establishments, we randomly selected 44 food establishments. Study participants were proportionately allocated to each selected food establishment based on the number of food handlers. Then, the sampling frame was prepared for each selected food establishment using the updated list of food handlers. Finally, study participants were selected using a simple random method (computer-generated) from each establishment.
Data Collection Tools and Procedures
Data were collected using a structured standard questionnaire and an observational checklist. A questionnaire consisting of close-ended questions pertaining to knowledge on food safety, attitude, and observed practices on food safety. The questioner was adapted and modified from previously published studies.2,15,25–27 The questionnaire was structured into four distinctive parts; demographic (11 questions), knowledge (9 questions), attitude (5 statements), and practices (18 statements).
Food safety knowledge was assessed using 9 closed-ended questions with two possible answers; “yes” or “No”. The questions mainly focus on the personal hygiene of food handlers, temperature control, cross-contamination, food storage, and equipment hygiene. In assessing knowledge, one point was given for every correct answer and zero points for incorrect answers or unanswered questions. Then, the responses to these questions were added together to generate a knowledge score ranging from 0 to 9. Food-handlers that obtained a total score ≥ mean (4.82) were considered to have “Good knowledge” and those that had scores < mean were considered to have “Insufficient knowledge”28
The attitude of food handlers’ towards food safety was measured using 5 questions that required five Likert scales response (1=strongly disagree, 2=disagree, 3=neutral, 4 =agree and 5=strongly agree). The scores for attitude were normally distributed. Therefore, we add all scores together and divide by the number of scores to obtain the mean. Finally, food-handlers that answered ≥ mean (13.17) correctly were measured to have a “favorable attitude”, whereas those that responded < mean statements/questions correctly were measured to have an “unfavorable attitude”29
Food handling practice was assessed by using an observational checklist during serving (working). These practices were also scored and one mark was given for every standard practice and zero for every unhygienic practice. Food-handlers that obtained total score ≥ mean were considered to have “safe practice” and those that had scores < mean were considered to have “unsafe practice” (20).
The data were collected by four diploma nurses and the overall data collection processes were supervised by two environmental health professionals after two-days of training. A pre-test was done on 5% of the sample in Dembecha town. Accordingly, all the necessary modifications were made.
Data Processing and Analysis
The data were entered into Epi data version 4.3 and transported to SPSS version 25.0 for further analysis. The results were presented in tables and texts using descriptive statistics such as mean, standard deviation and percentage to describe the study population in relation to relevant variables. Multivariable logistic regressions were employed to identify the independent factors associated with knowledge and practice of food safety. The strength of the association between independent variables and outcome variables was measured using an odds ratio (OR) with a 95% confidence interval. All variables with a p-value <0.25 at bivariable logistic regression analysis were included in the final regression model. In multivariable logistic regression analysis variables with a p-value <0.05 were used to declare statistical significant association. To measure internal consistency, Cronbach’s Alpha was done for both knowledge and attitude items of questions. Cronbach’s Alpha was 0.773 for knowledge and 0.758 for attitude measurement.
Operational Definitions
Food safety: is the assurance that food would not cause any harm to the consumers when it is prepared and/or consumed according to its intended use.15
Food handler- Person who contact directly with food, or with any equipment or utensil used in food handling.
Food establishment-establishments engaged in the work of providing food and drink services to large groups of customers in the form of breakfast, lunch, dinner, or drinks. These establishments are hotels, restaurants, cafeterias, and snack houses.30
Results
Socio-Demographic Characteristics of Study Participants
In this study, a total of 408 study participants participated with a response rate of 100%. Out of the total participants, 56.3% were female and almost all (99.8%) of food handlers were Orthodox Christian religious followers. The mean age of respondents was 22.5 years (SD± 3.55). More than three-fourths (75.7%) of the respondents were single and nearly two-thirds have completed secondary education. The majority of food handlers (84.3%) did not receive any training on food safety (Table 1).
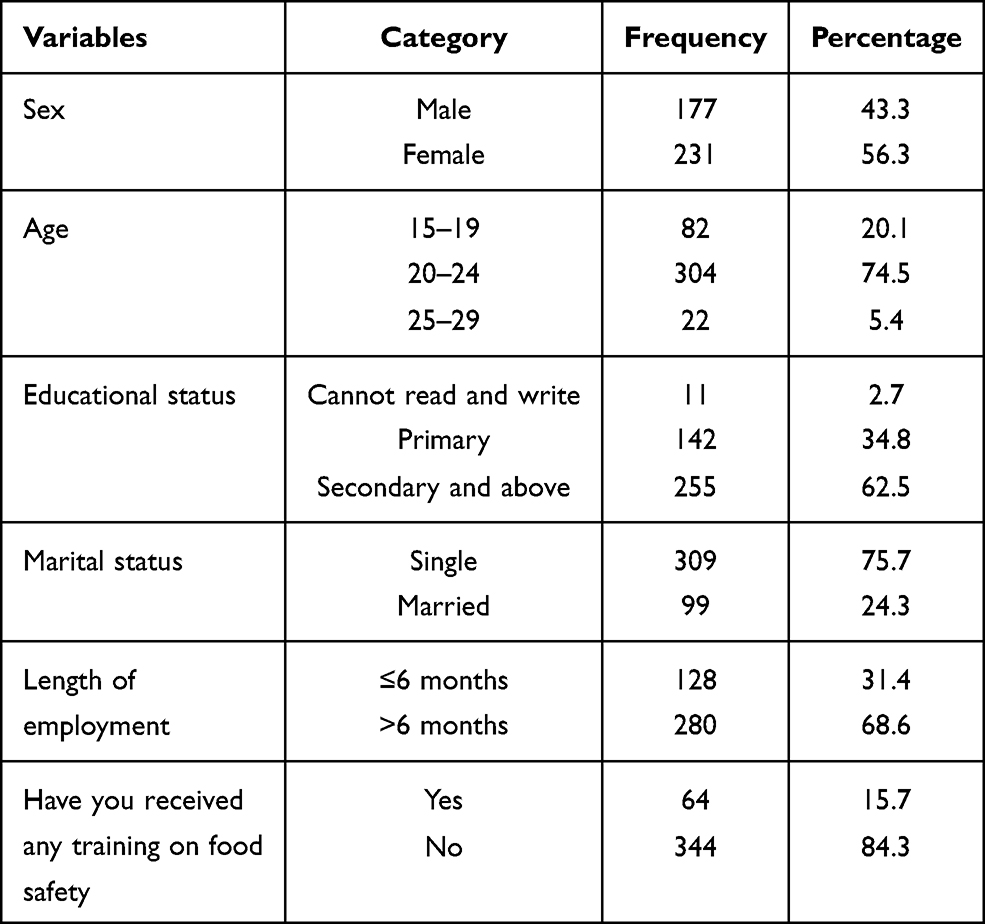 |
Table 1 Socio-Demographic Characteristics of Food Handlers Working in Food Establishments in Debre Markos Town, October 2019 (n=408) |
Characteristics of Food Establishments
In this study, food handlers were selected from 44 food establishments. All food establishments had private pipe water and toilet within the establishment. Out of 44 food establishments, 27 (61.4%) had disposed of liquid waste into a latrine and 2 food establishments dispose liquid wastes into open space (Table 2).
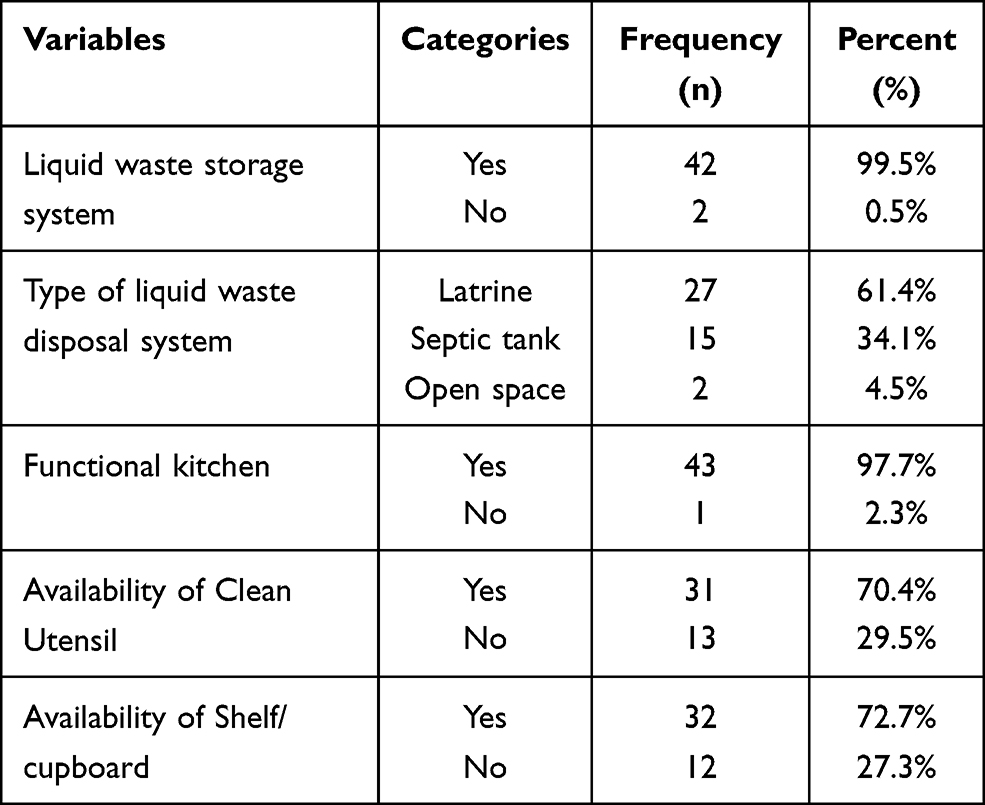 |
Table 2 Institutional Characteristics of Food Establishments in Debre Markos Town, Northwest Ethiopia, 2019 (n = 44) |
Food Safety Knowledge and Handling Practice
From the total participants, nearly half of the participants (52.2%) responded that contaminated foods always have some change in color, odor, or taste. Similarly, 45.6% of food handlers responded that cooked foods do not have microbes. Of the total food handlers, 157 (38.5%) responded that use of jewels such as rings, watches, wearing in food handling cause food contamination. Overall, only 34.1% (n=139) of food handlers had adequate knowledge of food safety. The majority (65.9%) of food handlers had inadequate knowledge. More than three-fourths (74.6%) of food handlers had a favorable attitude towards food safety but only 53.7% of food handlers had good handling practice (Table 3).
 |
Table 3 The Response of the Food Handlers About the Food Safety Knowledge Statements |
Factors Associated with Food Safety Knowledge
During bivariable regression analysis, levels of education, sex, length of employment, and attitude of the respondents were significantly associated with food safety knowledge. In the final regression model, level of education, training on food safety, and attitude were significantly associated with food safety knowledge.
Food handlers who did not attain any formal education were 77.0% less likely to have good food safety knowledge as compared to those food handlers who had completed secondary educational level (AOR=0.23, 95% CI= 0.14–0.57). Similarly, food handlers who had completed primary education were 73.0% less likely to have good knowledge of food safety than secondary school and above (AOR: 0.27, 95% CI =0.09–0.45). Trained food handlers were 5 times more likely to have good knowledge of food safety than non-trained food handlers (AOR: 5.13, 95% CI=3.57–7.82). The odds of having good knowledge of food safety among food handlers who had a favorable attitude towards food safety was nearly three folds higher as compared to those food handlers who had an unfavorable attitude (AOR = 2.54; 95% CI: 1.52–4.25) (Table 4).
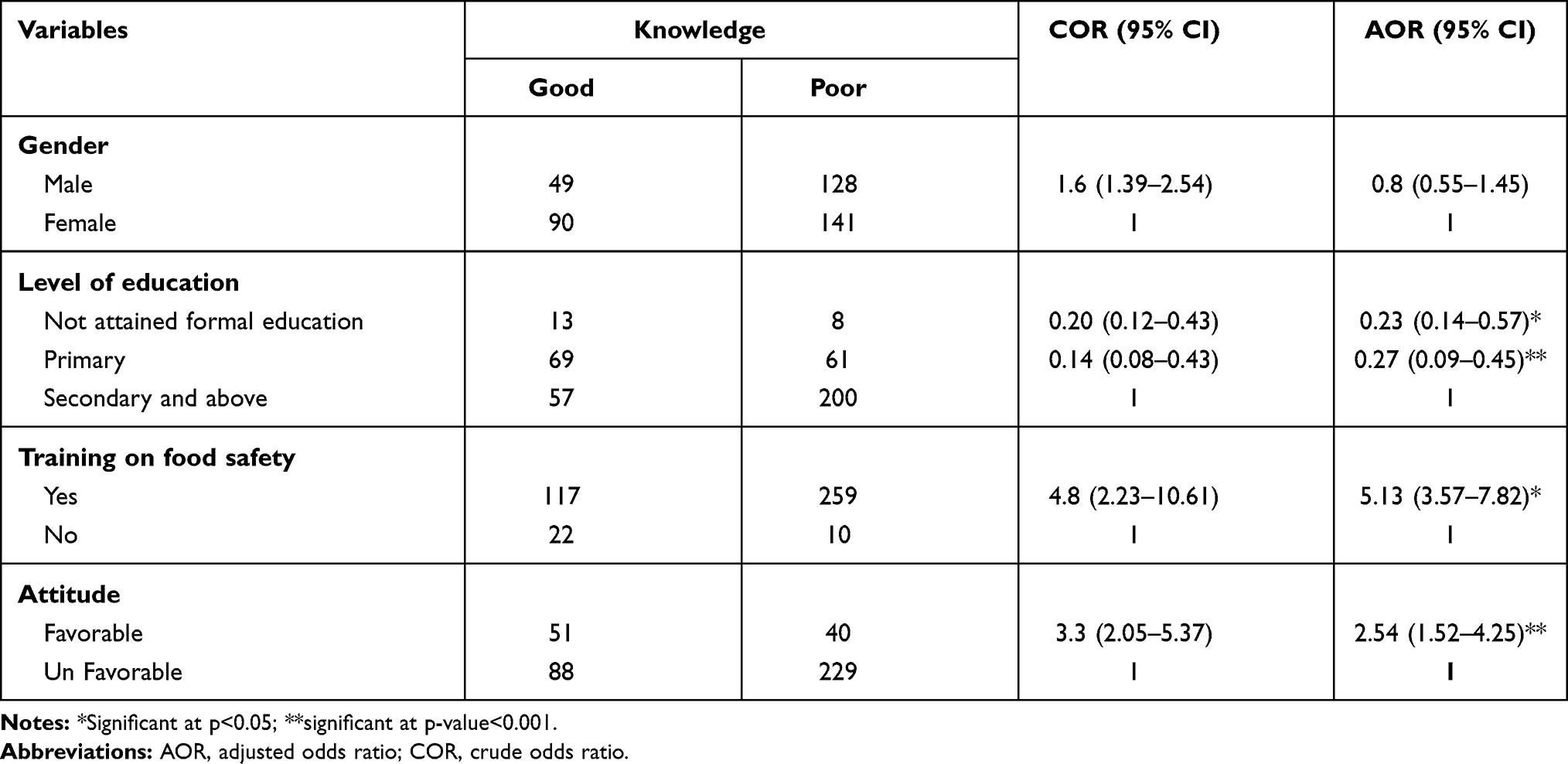 |
Table 4 A Bivariable and Multivariable Logistic Regression Analysis Output of Associated Factors with Knowledge on Food Safety in Debre Markos Town, Northwest Ethiopia, 2019 (n = 408) |
Factors Associated with Food Handling Practices
During bivariable logistic regression analysis, educational status, work experience, food safety training, and marital status were significantly associated with food handling practice. While running the final multivariable analysis model, only food safety training, knowledge of food safety, and work experience remains significant.
Trained food handlers were two times more likely to have good food safety practices than non-trained food handlers (AOR=2.05, 95% CI=1.31–3.19). Knowledgeable food handlers were 1.68 times more likely to practices good food safety than non-knowledgeable (AOR: 1.68, 95% CI: 1.40, 3.17). Similarly, the odds of having good food safety practices among food handlers who had work experience greater than the attitude towards food safety were 24.0% higher when compared to their counterparts (AOR = 1.24, 95% CI: 1.10–2.81) (Table 5).
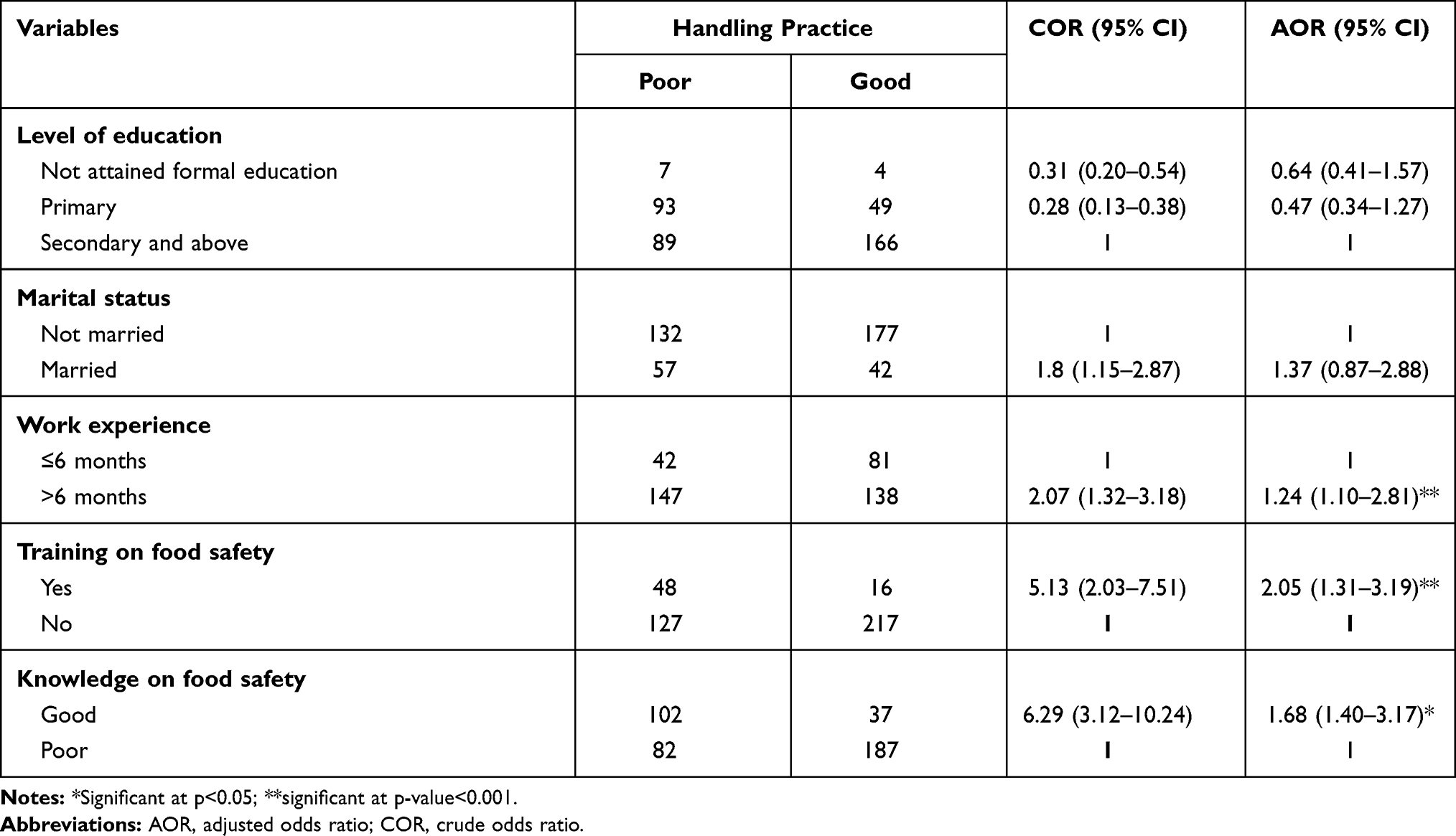 |
Table 5 A Bivariable and Multivariable Logistic Regression Analysis Output of Associated Factors with Food Handling Practice in Debre Markos Town, Northwest Ethiopia, 2019 (n = 408) |
Discussion
Lack of knowledge on food safety and poor food handling practice are the major contributors for food-borne disease and diarrheal related morbidity in Ethiopia. To overcome these public health problems, the governments of Ethiopia should give emphasis on the knowledge of food handlers on food safety and food handling practice. Therefore, this study gives information on the level of knowledge and food handling practice in northwest Ethiopia.
In the current study, only 34.1% of food handlers had good knowledge of food safety. This is consistent with studies done in northern Ethiopia,31 eastern Ethiopia,29 and India.32 In this study, nearly one-fourth (23.7%) of food handlers did not know that healthy people can cause illness by carrying germs to food. Similarly, 61.5% of the food handlers did not know that the use of jewels such as rings, watches, wearing in food handling can cause food contamination and 54.3% did not know that food handlers with a disease such as diarrhea, flu, and sore throat poses a risk of food contamination. This is supported with a study done in the central part of Ethiopia that reported more than half of food handlers were not heard about the food-borne disease, causes, and mode of transmission of food-borne disease and reason for food contamination.27
This study also revealed that only 53.7% of food handlers had safe food handling practices. The finding is nearly similar to studies done in northern Ethiopia (31) and Malaysia.33,34 However, this study is higher than a study conducted in Nigeria (36.5%),35 Gondar, Ethiopia (30.3%),36 Arba-Minch (32.6%),21 and Somali (20.9%).29 But, the finding is lower than other studies conducted in Jordan and Malaysia.24,37 The discrepancy might be due to variation in institutions where study participants were selected. For example, the study done in Jordan was conducted in a hospital setting which might have better resources and a suitable setup for food handling practice which might improve food handlers’ practice.
The odds of having good knowledge of food safety were lower among food handlers who did not attain any formal education and who have primary educational status as compared to those who have completed secondary education. The potential justification for this might be due to the fact that education might help food handlers to get better information regarding food safety as compared to non-educated. Besides, educated food handlers’ will also be able to read additional written messages on food safety from a different source of information such as leaflets, posters, or fliers and which in turn could positively affect food handlers knowledge on food safety.38
The odds of having good knowledge of food safety were 5 times higher among food handlers who received food safety-related training as compared to their counterparts. This finding is supported by a previous study.38 This is due to the fact that training could help them to acquire a better knowledge of food safety. Similarly, in the current study, a good attitude towards food safety is positively associated with food safety knowledge.
There is a significant positive association between work experience and food handling practice. The odds of performing good handling practice increased with prolonged work experience. This is possibly due to experience might help food handlers to gain good knowledge and abilities regarding food handling practice. Likewise, the odds of practicing good handling practices were higher among trained food handlers as compared to their counterparts. This is due to the fact that training could help them to acquire a better knowledge of food safety.
Knowledge is the key element to influence food handling practices among the food handlers. Similar to previous studies in different parts of Africa,39–41 this study revealed that the odds of having good handling practice was nearly two times higher among food handlers who had good food safety knowledge than those who have poor knowledge.
This study has several limitations. First, due to the cross-sectional nature of the study, it is impossible to declare a causal relationship between independent variables and the outcome of interest. Second, the study might be liable to social desirability. Finally, parasitic and microbiological laboratory analyses were not considered in this study.
Conclusion
The current study reveals that the level of good food safety knowledge and good handling practice was relatively low. Therefore it still needs further intervention and investigation. Food handlers’ level of education, training on food safety, and attitude were identified as the factors associated with food safety knowledge. Similarly, food safety training, knowledge of food safety, and work experience were identified as the factors associated with food handling practice. To improve food handling practice, concerned bodies need to enhance food handlers’ knowledge of food safety. Food safety-related training should be given continuously. The government of Ethiopia should give special attention to food handlers in food establishments in order to bring a better outcome in the future.
Abbreviation
AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; SPSS, Statistical Package for Social Sciences.
Data Sharing Statement
The data can be available from the corresponding author.
Ethical Approval and Consent to Participate
The study was conducted following the Declaration of Helsinki. Initially, ethical clearance was obtained from Debre Markos University ethical review committee (Reference number: DMU/RCS/078/2019). Then the detailed purpose of the study was explained to all study participants and written informed consent was taken from every participant. For study participants under the age of 18, the legal guardian of the participants provides informed consent on behalf of the participants. All information collected from the respondents was treated as confidential in that no name was recorded on the questionnaire and the collected data were kept using a computer password.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Dora-Liyana AL, Mahyudin NA, Ismail‐Fitry MR, et al. Food safety and hygiene knowledge, attitude and practices among food handlers at Boarding Schools in the Northern Region of Malaysia. Int J Acad Res Bus Soc Sci. 2018;8(17).
2. Getachew F. An Assessment of the hygienic and food handling practices in selected hospitals in Addis Ababa-Ethiopia. Unpublished master’s thesis, Addis Ababa University; 2010.
3. Organization WH. WHO estimates of the global burden of foodborne diseases: foodborne disease burden epidemiology reference group 2007–2015. World Health Organization; 2015.
4. Kambhampati LLA. Improving food safety through prevention: CDC’s Food Safety Prevention Status Report. CDC Environ Health Serv Branch. 2013;79(2).
5. Admasu M, Kelbessa W. Food safety knowledge, handling practice and associated factors among Food Handlers of Hotels/Restaurants in Asosa Town, North Western Ethiopia. SM J Public Health Epidemiol. 2018;4(1):1051.
6. Fung F, Wang H-S, Menon S. Food safety in the 21st century. Biomed J. 2018;41(2):88–95. doi:10.1016/j.bj.2018.03.003
7. Borchers A, Teuber SS, Keen CL, Gershwin ME. Food safety. Clin Rev Allergy Immunol. 2010;39(2):95–141. doi:10.1007/s12016-009-8176-4
8. Grace D. Food safety in developing countries: an overview; 2015.
9. Nguz K. Assessing food safety system in sub-Saharan countries: an overview of key issues. Food Control. 2007;18(2):131–134. doi:10.1016/j.foodcont.2005.09.003
10. Aworh OC. Food safety issues in fresh produce supply chain with particular reference to sub-Saharan Africa. Food Control. 2020;107737.
11. Lee HK, Abdul Halim H, Thong KL, Chai LC. Assessment of food safety knowledge, attitude, self-reported practices, and microbiological hand hygiene of food handlers. Int J Environ Res Public Health. 2017;14(1):55. doi:10.3390/ijerph14010055
12. Tegegne H, Phyo H. Food safety knowledge, attitude and practices of meat handler in abattoir and retail meat shops of Jigjiga Town, Ethiopia. J Prev Med Hyg. 2017;58(4):E320. doi:10.15167/2421-4248/jpmh2017.58.4.737
13. Organization WH. WHO global strategy for food safety; 2002. Available from: https://apps.who.int/iris/handle/10665/42559.
14. Abera K, Kalkidan G, Helina W, et al. The sanitary conditions of public food and drink establishments in the district town of Zeway, Southern Ethiopia. Original article. Ethiopian J Health Develop. 2001.
15. Dora-Liyana AL, Mahyudin NA. Food safety and hygiene knowledge, attitude and practices among Food Handlers at Boarding Schools in the Northern Region of Malaysia. Acad Res Bus Soc Sci. 2018;8(17).
16. Dagne H, Raju RP, Andualem Z, Hagos T, Addis K. Food safety practice and its associated factors among Mothers in Debarq Town, Northwest Ethiopia: community-Based Cross-Sectional Study. Biomed Res Int. 2019;2019:1549131. doi:10.1155/2019/1549131
17. Azanaw J, Gebrehiwot M, Dagne H. Factors associated with food safety practices among food handlers: facility-based cross-sectional study. BMC Res Notes. 2019;12(1):683. doi:10.1186/s13104-019-4702-5
18. Chekol FA, Melak MF, Belew AK, Zeleke EG. Food handling practice and associated factors among food handlers in public food establishments, Northwest Ethiopia. BMC Res Notes. 2019;12(1):20. doi:10.1186/s13104-019-4047-0
19. Yenealem DG, Yallew WW, Abdulmajid S. Food safety practice and associated factors among Meat Handlers in Gondar Town: a Cross-Sectional Study. J Environ Public Health. 2020;2020:7421745. doi:10.1155/2020/7421745
20. Baraki N. Egata G. Food Safety Practice and AssociatedFactors among Food Handlers in Public Food Establishments of Godey Town. Somali Region, Eastern Ethiopia, HaramayaUniversity, Dire Dawa, Ethiopia; 2018.
21. Legesse D, Tilahun M, Agedew E, Haftu D. Food handling practices and associated factors among food handlers in arba minch town public food establishments in Gamo Gofa Zone, Southern Ethiopia. Epidemiology. 2017;7(302):2161–1165.1000302. doi:10.4172/2161-1165.1000302
22. Getachew M. Food safety practice and associated factors among food handlers in selected types of food establishments of Dire Dawa, Ethiopia. New York: FAO; 2016:41.
23. office DMtAms. Debre Markos town Administrative mayor’s office 2018 profile data; 2018.
24. Rosnani AH, Son R, Mohhidin O. Assessment of knowledge, attitude and practices concerning food safety among Restaurant Workers in Putrajaya, Malaysia. Food Sci Qual Manage. 2014;32.
25. Akabanda F, Hlortsi EH, Owusu-Kwarteng J. Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health. 2017;17(40).
26. Geta K. Microbiological safety of fruit juices consumed in cafes and restaurants of debre-markos town, North Western Ethiopia; 2015.
27. Neme K, Hailu B, Belachew T. Assess Sanitary Condition and Food Handling Practices of Restaurants in Jimma Town, Ethiopia: implication for Food Born Infection and Food Intoxication. Food Sci Qual Manage. 2017;60.
28. Kibret M, Abera B. The sanitary conditions of food service establishments and food safety knowledge and practices of food handlers in Bahir Dar town. Ethiop J Health Sci. 2011;22(1).
29. Mussama M. Food safety practice and associated factors among food handlers in public food establishments of Godey Town. Somali Region, Eastern Ethiopia; 2018.
30. Abate M, Tesfa M, Adere A. The sanitary conditions of food and drink establishments in Woldia town, Northeastern Ethiopia. Ethiop J Health Dev. 2016;32(3).
31. Tessema AG, Gelaye KA, Chercos DH. Factors affecting food handling Practices among food handlers of Dangila town food and drink establishments, North West Ethiopia. BMC Public Health. 2014;14(1):571. doi:10.1186/1471-2458-14-571
32. Kubde SR, Pattankar J, Kokiwar PR. Knowledge and food hygiene practices among food handlers in food establishments. Int J Community Med Public Health. 2016;251–256. doi:10.18203/2394-6040.ijcmph20151572
33. Zain MM, Naing NN. Sociodemographic characteristics of food handlers and their knowledge, attitude and practice towards food sanitation: a preliminary report. Southeast Asian j Trop Med Public Health. 2002;33(2):410–417.
34. Havelaar AH, Cawthorne A, Angulo F, et al. WHO initiative to estimate the global burden of foodborne diseases. Lancet. 2013;381:S59. doi:10.1016/S0140-6736(13)61313-6
35. Iwu AC, Uwakwe KA, Duru CB. Knowledge, attitude and practices of food hygiene among food vendors in Owerri, Imo State, Nigeria. Occup Dis Environ Med. 2017;5(11):11–25. doi:10.4236/odem.2017.51002
36. Gizaw ZGM, Teka Z. Food safety practice and associated factors of food handlers working in substandard food establishments in Gondar Town, Northwest Ethiopia, 2013/14. Food Sci Nutr Diet. 2014;3(7).
37. Ma’moun A, Al-Shakhsheer F, Al-Ababneh MM. Restaurant employees’ food handling practices in Irbid City, Jordan. Tourism Hospitality Manage. 2017;5(1).
38. Addo-Tham R, Appiah-Brempong E, Vampere H, Acquah-Gyan E, Gyimah Akwasi A. Knowledge on food safety and food-handling practices of street food vendors in Ejisu-Juaben Municipality of Ghana. Adv Public Health. 2020;2020:4579573. doi:10.1155/2020/4579573
39. Ncube F, Kanda A, Chijokwe M, Mabaya G, Nyamugure T. Food safety knowledge, attitudes and practices of restaurant food handlers in a lower‐middle‐income country. Food Sci Nutr. 2020;8(3):1677–1687. doi:10.1002/fsn3.1454
40. Akabanda F, Hlortsi EH, Owusu-Kwarteng J. Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health. 2017;17(1):40. doi:10.1186/s12889-016-3986-9
41. Yenealem D, Yallew W, Abdulmajid S. Food safety practice and associated factors among meat handlers in Gondar Town: a Cross-Sectional Study. J Environ Public Health. 2020;2020:1–7.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.