Back to Journals » Risk Management and Healthcare Policy » Volume 13
Food Hygiene Practices and Associated Factors Among Food Handlers Working in Food Establishments in the Bole Sub City, Addis Ababa, Ethiopia
Authors Abdi AM ![]() , Amano A
, Amano A ![]() , Abrahim A, Getahun M, Ababor S, Kumie A
, Abrahim A, Getahun M, Ababor S, Kumie A
Received 20 June 2020
Accepted for publication 29 August 2020
Published 1 October 2020 Volume 2020:13 Pages 1861—1868
DOI https://doi.org/10.2147/RMHP.S266342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Ahmed Mohammed Abdi,1 Abdella Amano,2 Abadir Abrahim,3 Mulusew Getahun,4 Sabit Ababor,5 Abera Kumie6
1Department of Public Health Emergency Management, Ethiopian Public Health Institute, Gulele Sub City, Addis Ababa, Ethiopia; 2Department of Public Health, Hawassa University, Hawassa, SNNPR, Ethiopia; 3Department of Business Administration, Jimma University, Jimma, Oromia Regional State, Ethiopia; 4Department of Immunology and Hematology, Ethiopian Public Health Institute, Gulele Sub City, Addis Ababa, Ethiopia; 5Department of Public Health, Ethiopian Public Health Institute, Gulele Sub City, Addis Ababa, Ethiopia; 6Department of Preventive Medicine, Addis Ababa University, Lideta Sub City, Addis Ababa, Ethiopia
Correspondence: Ahmed Mohammed Abdi
Department of Public Health Emergency Management, Ethiopian Public Health Institute, P.O. Box 102249, Gulele Sub City, Addis Ababa, Ethiopia
Tel +251911910058
Email [email protected]
Background: Consumers’ health would be at risk unless food preparation and handling hygiene is ensured by food establishments. Literature indicates that poor food handling and sanitation practices are more common among food handlers in developing countries resulting in food-borne illness. Hence, food handlers can play a significant role in ensuring food hygiene. To this end, the paper aims to assess the level of food hygiene practices and its associated factors of food handlers working in food establishments in Bole sub-city, Addis Ababa, Ethiopia.
Methods: Through across-sectional study design, a total of 394 food handlers selected randomly from food establishments have participated in the study. The data were collected between July and December 2017, through interview and observation. Percentage, cross tabulations, and logistic regressions were used to analyze the data.
Results: The findings show that among 394 study subjects only 27.4% (i.e., 108 food handlers), were found to have good food hygiene practices. In other words, majority of food handlers observed were poor in maintaining food hygiene. Food hygiene practices were highly influenced by level score of favorable attitude (AOR = 3.9, 95% CI = 1.93, 7.87), extensive knowledge towards food hygiene (AOR= 3.33, 95% CI= 1.93, 5.76) and availability of water storage equipment at food establishments (AOR= 2.67, 95% CI= 1.38, 5.15).
Conclusion: Food handlers had poor food hygiene practices in the study area. Shortages of a continuous water supply at food establishments, poor knowledge, and unfavorable attitude of food handlers towards food hygiene practice were all contributing factors associated with poor food hygiene practice. However, these can be improved through health education programs and environmental health services, such as periodic inspections, effective enforcement of food safety regulations, and enhancing the capacity of food hygiene regulators.
Keywords: food hygiene, food handlers, Addis Ababa Ethiopia
Background
The gradual increase in urbanization, industrialization, expansion of the tourism industry and economic globalization have typically led to a significant rise in the number of food establishments across the world.1,2,6,11 This is also true in Ethiopia, especially Addis Ababa, the capital city where the number of food establishments are growing at an increasing rate. This might compromise food hygiene as hygiene regulators might not keep up with expansion and, in some cases, lack proper mandates to ensure food hygiene. In such a situation, food establishments may see an increase in food-borne diseases. Food-borne diseases are common in both developed and developing countries because of the prevailing poor food hygiene and sanitation practice.3,4,9,14,29,31,32
Food is the basic need for all living organisms and it can be contaminated in different ways. The three main risk factors responsible for food-borne disease are: 1) poor personal hygiene, 2) improper food handling, and 3) contaminated food surfaces and equipment.6,10 Food handling practice is one of the main sources of food contamination. Empirical data indicates that poor food handling practices by food handlers were responsible for 10–20% of food-borne diseases.4,7,16 When it comes to specific cases in the US, improper food handling practices contribute to 97% of food-borne illness in food establishments as well as in private homes.5 Furthermore, observational studies show that errors in food handling were also more common among the food handlers. This indicates that food handlers play a major role in ensuring food hygiene throughout the chain of food processing.7,12
Food hygiene practices are worse in developing countries, especially in Ethiopia, according to previous studies conducted in this area. For example, in Addis Ababa only 50% of food handlers have maintained a satisfactory hygiene practice in handling food in studied food establishments.8 Considering the KAP more needs to be done on sanitary condition of food establishment throughout the developing countries.7,9,16,30 Unless hygienic food handling and preparation is ensured in food establishments, consumers’ health and well-being could be at risk.
Some studies suggested that a lack of knowledge may result in poor hygiene practices among food handlers.10 To the contrary, some published studies in developing countries revealed that food handlers seldom follow food handling procedure despite their awareness and knowledge of food hygiene.9,10 Many factors, including individual, institutional, and socioeconomic, are reported to have an influence on the ability of food handlers to prepare and handle food hygienically.5,11,12
In Ethiopia, there are a numbers of destination points for food-borne diseases; groups susceptible to this risk are groups such as travelers, economically better-off people, refugees and immigrants. Among these, Bole sub-city is one of the main destination points and residential area for these people.
Although tremendous efforts have been made to improve public health problems in Ethiopia, including in the capital, the safety of food hygiene practices and procedures by food handlers remains a challenge.13 Though the problem is significant little has been done to ensure food hygiene in parts of Ethiopia, including in Addis Ababa.5,14,30 Therefore, in the study area the status of food hygiene practices and its associated factors among food handlers were unknown. Hence, this study aimed at determining the level of food hygiene practices, and its associated factors among food handlers in the Bole sub-city (home to Ethiopians, travelers, refugees, and immigrants). This is crucial to provide baseline information valuable for environmental health interventions.
Methods
A community-based cross-sectional study was conducted in Bole sub-city, Addis Ababa, Ethiopia, between July and December 2017. Bole sub-city is one of eight sub-cities found in Addis Ababa, the capital of Ethiopia.
Participants of the study were food handlers who worked in different food establishments such as Hotels below star level, café and restaurants, bar and restaurants, restaurants, bar snacks and ‘Menafesha bet.’ Study participants were selected using simple random sampling technique by taking the roster as sampling frame. One participant was interviewed per food establishment.
The sample size was determined using a single population proportion formula which took the following assumptions in to consideration: level of food hygiene practice of food handlers 20.65%,12 (p = 0.2065); 5% level of significance (α = 0.04); 4% marginal error. The final sample size was adjusted by adding 5% non-response rate. Thus, the sample size used in the study was t 414 food handlers.
Using standardized questionnaire and observational checklist developed data was collected through face to face interview and observation. There was a discrepancy between self-reported practice and actual practice. For this reason the observations are a more reliable means of collecting practices data as food handlers tend to overestimate their actual behaviors, there by introducing social desirability bias.15 The questionnaire was adopted from previous literature8,14 is based on a 5-point Likert scale ranging from 0 to 4. The range of scales represents respectively options from high to low; always, most of the times, sometimes, rarely and never. The five scales further categorized in dichotomy as negative and positive. Responses below or scores less than 3 were categorized as a negative while scores 3 and 4 were categorized as a positive response. Those study participants who have scored 80% and above out of the total items related to food hygiene practice questions were classified as good food hygiene practice. Data were collected by trained female data collectors and supervised by environmental health officers. Women in Ethiopia considered it taboo to discuss cooking activities to men. Because of this reason female data collectors were considered for data collection. In order to assure the quality of this study, a pre-test of data collection instrument was carried out on 5% of study population. In addition, training was given for data collectors and supervisors.
Data entry was done by using EPI Info version 3 and exported to SPSS version 20.0 software package for analysis. Binary logistic regression was used to determine the effect of various factors on the outcome variable and to control confounding effects. The results were presented in the form of tables and text using frequencies and summary statistics such as mean, standard deviation, and percentage to describe the study population in relation to relevant variables. The strength of association between independent and dependent variables was made using odds ratio with 95% CI.
Operational Definition
Food hygiene practices: a process carried out by food handlers to protect food from contamination and ensure a safe supply of food for the consumer.
Food hygiene practice level: respondents who scored less than 80% of their response to the total food hygiene practice-related questions were considered as having poor level of practices. Those who scored equal to or more than 80% were considered as having a good level of practice.
Food hygiene knowledge level: respondents who scored less than 80% of their responses to the total food hygiene knowledge-related questions were considered as having a poor level of knowledge. Those who scored equal to or more than 80% were considered as having a good level of knowledge.
Food hygiene attitude level: the respondents who scored less than 80% of their responses to the total food hygiene attitude-related questions were considered as having a negative level of attitude. Those who scored equal to or more than 80% were considered as having a positive level of attitude.
Results
Socio-Demographic Characteristics of Food Handlers
In this study a total of 394 food handlers participated with a response rate of 394 (95.17%). The majority (371; 94.2%) of the participants were female. More than half of the food handlers, (244; 61.9%) were found to be above 20 years of age. Of the total, (347; 88.1%) has completed primary education and above. However, only 64 (32.7%) of food handlers took formal training about food hygiene principles in the past year. Nearly all (364; 92.7%) of food handlers had less than 5 years of services in food establishment. The study assessed a total of 394 food establishments, which includes 8 (2%) hotels below star level, 36 (9.2%) bar and restaurants, 64 (16.2%) cafe and restaurants, 17 (4.3%) restaurants, 220 (55.8%) bar snack, and 49 (12.5%) others (Table 1).
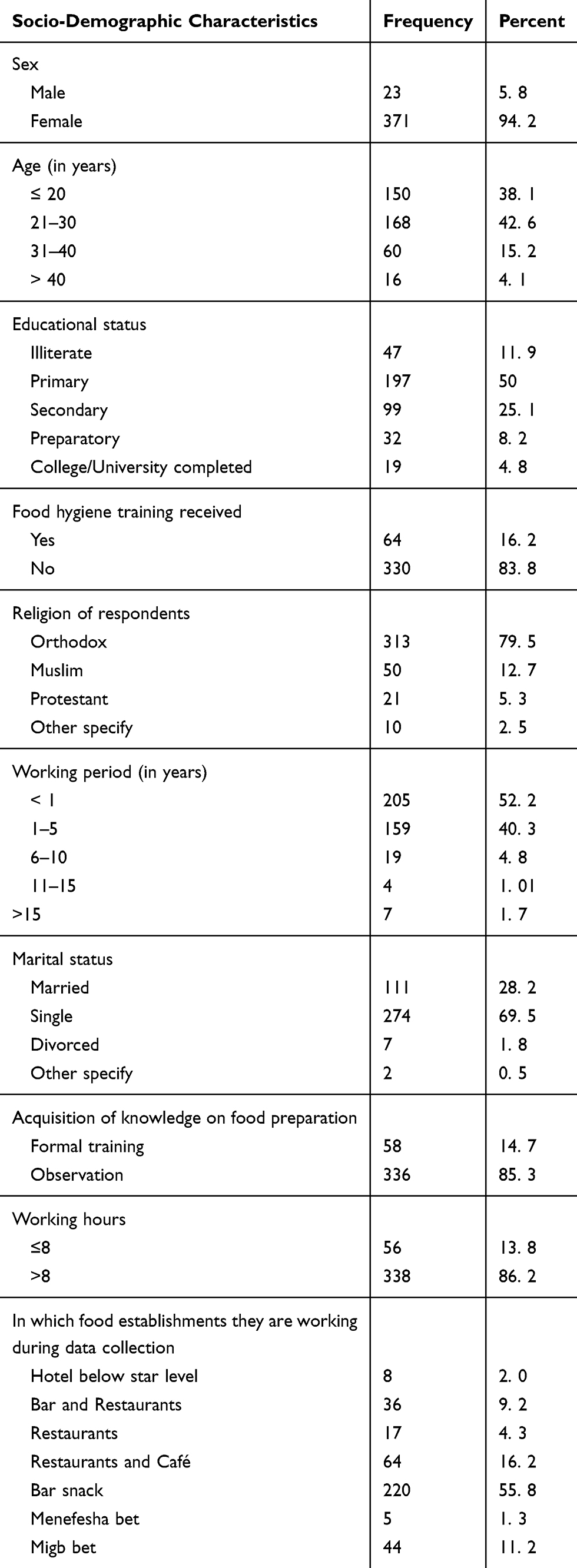 |
Table 1 Socio-Demographic Profile of Food Handlers in Bole Sub-City, 2017 (n= 394) |
Knowledge and Attitude of Food Handlers
One hundred ten (28%) and 121 (31%) of study participants were found to have good knowledge and positive attitude towards food hygiene practices respectively.
Food Handlers’ Practice
Food hygiene practices were found to be poor in the majority of the food handlers. In general, among the 394 food handlers who participated in the study, 108 (27.4%) 95% CI, 27 (23.1, 32.2) had demonstrated good food hygiene practices.
Food Handlers’ Self-Reported Practices on Food Hygiene
Improper food hygiene practices is main route of food-borne diseases. Less than half (190; 48.3%) and 143 (36.2%) of the study participants reported that they maintained safe practices on hand washing and personal hygiene respectively. Similarly, less than two-thirds (177; 44.9%) of the food handlers in our study reported that they followed proper safe practices regarding cross-contamination. In addition to that approximately one-third (129; 32.7%) of food handlers reported that they kept and cooked food at safe temperature., Furthermore, only 97 (24.6%) food handlers stated that they were engaged in food handling by ensuring good health practices. More than half (250; 63.45%) of respondents stated that they had cleaned and sanitized equipment and/or utensils and workstation by using proper procedures and detergents. Finally, nearly all (359, 91.1%) of food handlers reported that they utilized safe water and materials in food preparation chains (Table 2).
 |
Table 2 Food Handlers’ Self-Reported Practices on Food Hygiene in Bole Sub-City, 2017 (n= 394) |
Observed Food Hygiene Practices and Availability of Sanitary Facilities
Observed Food Hygiene Practices
Poor personal hygiene, cross-contamination, and time–temperature abuse are main causes of food-borne illness. These factors should be controlled regularly for safe food hygiene and sanitation practices in food establishments. During the study period, among the study participant, 85 (21.6%) of the food handlers followed safe practices of personal hygiene, and 90 (22.8%) of food handlers were observed using appropriate hand washing procedures. In addition, 114 (28.9%) of study participants adhered to safe practices regarding cross-contamination, while 101 (25.6%) of food handlers cooked food and kept at safe temperature. Similarly, about 120 (30.45%) of respondents maintained good hygiene of equipment, utensils and work stations, and also more than two-thirds (290; 73.5%) of respondents adhered to good health practices to reduce risk to consumers. Finally less than one-third 97 (24.6%) of participants had utilized safe water and materials (Table 3).
 |
Table 3 Food Handlers’ Observed Practices on Food Hygiene in Bole Sub-City, 2017 (n= 394) |
Availability of Sanitary Facilities
More than half of food handlers, 264 (67.0%) were working in an establishments which had private pipe. Similarly, approximately 86 (22%) and 118 (30%) of food handlers handled food in an establishment having water storage equipment and functional hand washing facility near the toilet area respectively. Of the establishments which had hand washing facility near the toilet area, approximately half (48.0%) of hand washing facilities were without any detergents or soap for hand washing purpose. However, all 394 (100%) of food handlers handled food in institution where there were no hand washing facilities near the kitchen area (Table 3).
Factors Associated with Food Hygiene Practices
Multi-variable logistic regression analysis reported that good knowledge, positive attitude and presence of water storage equipment for continues water supply in food establishments were statistically associated factors with food hygiene practices.
The odds of performing good hygiene practice among food handlers who had good knowledge towards good food hygiene practices were 3 times higher than compared to their counterparts (AOR= 3.33, 95% CI= 1.93, 5.76).
Similarly, the likelihood of performing good food hygiene practices among food handlers who had a positive attitude towards good food hygiene practices was 4 times higher when compared to those food handlers who had no positive attitude towards food hygiene practices (AOR= 3.9, 95% CI= 1.93, 7.87).
Furthermore, food handlers who were working in an establishment which had water storage equipment were 2.7 times more likely to have good food hygiene practices when compared to those food handlers who were working in an establishment without water storage equipment (AOR= 2.67, 95% CI = 1.38, 5.15) (Table 4).
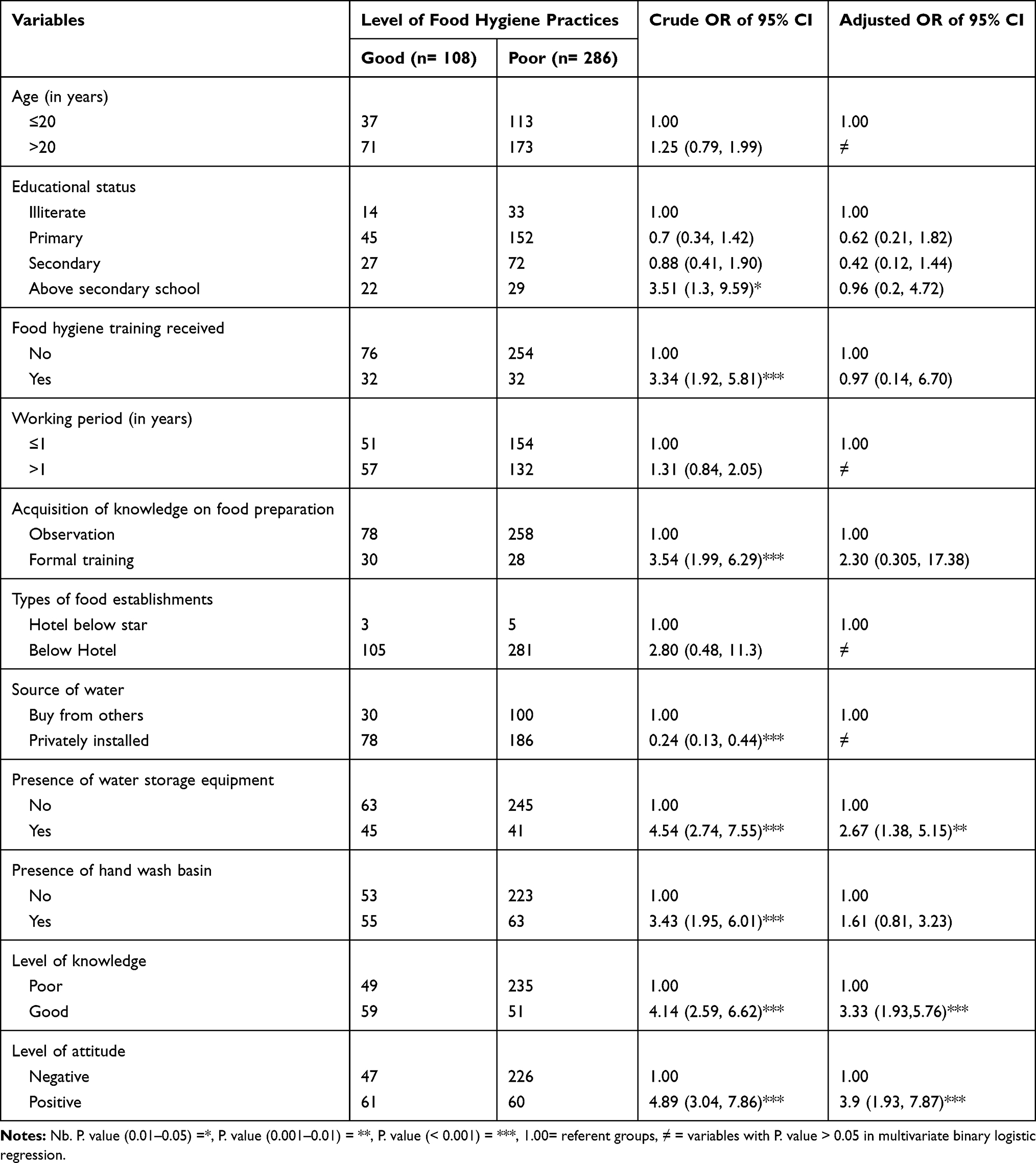 |
Table 4 Selected Socio-Demographic Determinants of Food Hygiene Practice in Bole Sub-City, 2017 (n= 394) |
Discussion
Poor hygiene and sanitation practice is one of the major routes of food-borne disease transmission. To reduce/prevent the burden of food-borne diseases due attention is expected from concerned bodies on the improvement of food hygiene and sanitation practices. For that reason, this study provides an understanding on the status of food hygiene practice among food handlers working in study setting. This study shows that good food hygiene practice was 27.4% (95% CI 23.1, 32.2). The result is consistent with the study conducted in Gondar (30.3%).17
However, the finding is lower than other studies conducted in Saudi Arabia (80.29%),18 Indonesia (90%),19 Jordan (89.4%),20 and Malaysia (59.3%).21 The discrepancy may be due to study area context and a difference in study population (food handlers). The studies in Saudi Arabia and Malaysia were conducted on the universities' campuses, while studies conducted in Indonesia and Jordan were conducted in health care facilities. In fact, these facilities might have sufficient resources and appropriate arrangement for hygienic practices as compared to this study area. Similarly, the educational status of food handlers might contribute for this variation. In our study only 38.1% of study participants attended secondary school and above education.
Furthermore, the result of this study is also lower than studies conducted in Mekelle (63.9%),8 Dangla (52.5%),22 Dire Dawa (52.4%)23 and Gamogofa (32.6).24 The difference might be due to study setting, sensitive environment, and educational status of respondents. The study in Mekelle was conducted on the university campus. The institution might have enough resources and better infrastructure which enhancwhen good food hygiene practices as compared to this study area. Sensitivity of food to the warm environment in Diredawa might make food handlers curious while handling23 because foods may become easily perishable.
According to the previous studies many factors such as time pressure, equipment and resource availability, food hygiene emphasis by management and co-workers, food hygiene education and training, and environmental health services have an influence on the ability of food handlers to prepare food hygienically.12 The above factors have a leaner relationship on the improvement of food hygiene knowledge, attitude and food hygiene practice towards food hygiene principles.1,25 In relation to the above information, a recent study reported that good knowledge, positive attitude, and presence of water storage equipment that provided a continuous water supply in food establishments were positively associated variables with food hygiene practices.
Accordingly, the odds of performing good hygiene practices among the study participants who had good knowledge towards good food hygiene practice was 3 times higher as compared to their counterparts. Those who have good knowledge are assumed to have positive attitude which is key elements for practice. This finding is in line with other studies conducted in Mekelle5 and Dangila.22
Similarly, the odds of performing good hygiene practices among food handlers who had positive attitude towards good food hygiene practice was 4 times higher when compared to their counterparts. Those who have meaningful knowledge and positive attitude towards food hygiene practice display positive behaviors.15,19,26 This result is corroborated in the studies carried out in Turkey,27 Gondar,17 Dire Dawa,23 and also elsewhere by Yarrow et al.28
Food handlers who were working in an establishment which had water storage equipment were 2.7 times more likely to have good food hygiene practices compared to those who were working in an establishment which did not have water storage equipment. The reason for this finding might be those study participants working in food establishments which had a continuous water supply might have better personal hygiene and sanitation practice.12
Limitation
The limitations of this work are that some socio-demographic variables such as income of the food handlers, supervision, inspection, and detailed sanitary practices in the establishments have not been considered. In addition, enumeration of bacteria and other enteric pathogens were not included in this research.
Conclusions
In conclusion more than two-thirds of study participants had poor food hygiene practices in our study area. Poor knowledge and unfavorable attitude towards food hygiene practices and shortage of a continuous water supply in the facilities were contributing factors for food hygiene practice. The concerned body or relevant program manager can use this study to improve the identified gaps through health education program and environmental health services, such as periodic inspections, effective enforcement of food safety regulations, and enhancing the capacity of an authorized body.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author and will submit on reasonable request.
Ethics Approval and Consent
Study protocol was approved by joint Ethical Review Board of Addis Continental Institute of Public Health and University of Gondar. Similarly, the ethical clearance was obtained from Ethic and Research committee established under Addis Ababa Regional Health Bureau. In addition, Permission was obtained from Bole sub-city administration, Bole sub-city health office, and all Woreda administration. The verbal informed consent was accepted and approved by the institutions mentioned above. A verbal informed consent was obtained from each study participant after the purpose of study was explained for them. The data collectors informed them that thet information obtained was not disclosed to any third party. Study participants who were not volunteer to continue from the beginning or at any moment of the interview were respected to do so. Privacy and strict confidentiality were maintained during the interview process. Name and personal identifiers of participants had not been included in order to maintain anonymity.
Acknowledgment
The authors would like to thank University of Gondar, Addis Continental Institute of Public Health, and Addis Ababa Regional Health Bureau for their ethical approval and valuable comments on research project. In general study participants and Bole Sub-city Administration offices are thankful for their cooperation during data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors had no funding support or funding to report.
Disclosure
All authors declare that they have no competing interest.
References
1. Getachew F. An assessment of the hygienic and food handling practices in selected hospitals in Addis Ababa- Ethiopia (Unpublished data); 2010.
2. WHO. The Role of Food Safety in Health and Development. World Health Organization Technical Report Series No 705. Geneva; 1984.
3. FAO/WHO Regional Conference on Food Safety for Africa. National Food Safety System in Ethiopia, a Situation Analysis. Zimbabwe, Harare; October 3–6, 2005.
4. WHO. Global Strategy for Food Safety. Geneva; 2002.
5. Nigusse D, Kumie A. Food hygiene practices and prevalence of intestinal parasites among food handlers working in Mekelle university student’s cafeteria, Mekelle. Glob Adv Res J Social Sci. 2012;1(4):065–071.
6. Akabanda F, Hlortsi EH, Owusu-Kwarteng J. Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health. 2017;17(1):40. doi:10.1186/s12889-016-3986-9
7. Zain MM, Naing NN, Janecharat T, Ukong S. Sociodemographic characteristics of food handlers and their knowledge, attitude and practice towards food sanitation: a preliminary report. Southeast Asian J Trop Med Public Health. 2002;33(Suppl 3):2.
8. Zeru K, Kumie A. Sanitary conditions of food establishments in Mekelle town, Tigray, north Ethiopia. Ethiop J Health Dev. 2007;21:3–11.
9. World Health Organization. Food Borne Disease Outbreaks: Guidelines for Investigation and Control. Geneva; 2008.
10. Tan SL, Cheng PL, Soon HK, et al. A qualitative study on personal hygiene knowledge and practices among food handlers at selected primary schools in Klang valley area, Selangor, Malaysia. Int Food Res J. 2013;20(1):71–76.
11. Kibret M, Abera B. The sanitary conditions of food service establishments and food safety knowledge and practices of food handlers in Bahirdar town. Ethiop J Health Sci. 2012;22(1):27–35.
12. Patah MO, Issa ZM, Nor KM. Food safety attitude of culinary arts based students in Public and Private Higher Learning Institutions (IPT). Int Educ Stud. 2009;2(4):168–178.
13. Guteta D. Sanitary survey of food and drinking establishments in Ambo Town West Showa Zone Oromia Region. (unpublished); 2007.
14. Haileselassie M, Taddele H, Adhana K. Source (s) of contamination of ‘raw’ and ‘ready-to-eat’ foods and their public health risks in Mekelle City, Ethiopia. Asian J Food Agric Sci. 2012;2(2):20–29.
15. Thelwell-Reid MA Food Safety Knowledge and Self-Reported Practices of Food Handlers in Jamaica. Walden: Walden University Scholar Works; 2014:188.
16. Smith SI, Agomo CO, Bamidele M, et al. Survey of food handlers in bukas (a type of local restaurant) in Lagos, Nigeria about typhoid fever. Health. 2010;2(08):951–956
17. Gizaw Z, Gebrehiwot M, Teka Z. Food safety practice and associated factors of food handlers working in substandard food establishments in Gondar Town, North West Ethiopia, 2013/14. Int J Food Sci Nutr Diet. 2014;3(7):138–148.
18. Sharif L, Al-Malki T, Knowledge, attitude and practice of Taif University students on food poisoning. Food Control. 2010;21(1):55–60. doi:10.1016/j.foodcont.2009.03.015
19. Daru L, Husodo AH, Iravati S, et al. Safe food handling knowledge, attitude and practice of food handlers in Hospital Kitchen. Int J Publ Health Sci. 2017;6(4):324–330.
20. Sharif L, Obaidat MM, Al-Dalalah M-R, et al. Food hygiene knowledge, attitudes and practices of the food handlers in the military hospitals. J Food Nutr Sci. 2013;4:245–251. doi:10.4236/fns.2013.43033
21. Nee S, Sani NA. Assessment of knowledge, attitudes and practices (KAP) among food handlers at residential colleges and canteen regarding food safety. J Sains Malays. 2011;40(4):403–410.
22. Tessema AG, Gelaye KA, Chercos DH. Factors affecting food handling Practices among food handlers of Dangila town food and drink establishments, North West Ethiopia. BMC Public Health. 2014;14(1):571. doi:10.1186/1471-2458-14-571
23. Getachew M. Food Safety Practice and Associated Factors Among Food Handlers in Selected Types of Food Establishments of Dire Dawa, Ethiopia. New York: FAO; 2016:41.
24. Legesse D, Tilahun M, Agedew E, Haftu D. Food handling practices and associated factors among food handlers in arba minch town public food establishments in Gamo Gofa Zone, Southern Ethiopia. Epidemiology. 2017;7:2.
25. Annor GA, Ekua Anamoaba B, et al. Evaluation of food hygiene knowledge attitudes and practices of food handlers in food businesses in Accra, Ghana. J Sci Res Food Nutr. 2011;2:830–836.
26. Rutter D, Quine L. Changing Health Behaviour: Intervention and Research with Social Cognition Models.Buckingham: Open University Press; 2002:224.
27. Sanlier N, Konaklioglu E. Food safety knowledge, attitude and food handling practices of students. Br Food J. 2012;114(4):469–480. doi:10.1108/00070701211219504
28. Yarrow L, Remig VM, Higgins MM. Food safety educational intervention positively influences college students food safety attitudes, beliefs, knowledge, and self-reported practices. J Environ Health. 2009;71(6):30–35.
29. Kasturwar NB, Shafee M. Knowledge, practices and prevalence of MRSA among food handlers. Int J Biol Med Res. 2011;2(4):889–894.
30. Abera K, Genete K, Worku H, et al. The sanitary conditions of public food and drink establishments in the district town of Zeway, Southern Ethiopia. Ethiop J Health Dev. 2002;16:95–104.
31. Ansari MA, Khan Z. An evaluation of health education intervention on hygienic status of food handlers in Aligarh - a three year experience. J Community Med Health Educ. 2012;2(4):15. doi:10.4172/2161-0711.1000142
32. World Health Organization Initiative to Estimate the Global Burden of Food Borne Diseases, First Formal Meeting of the Foodborne Diseases Burden Epidemiology Reference Group (FERG). Geneva; November 26–27, 2007.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.