Back to Journals » Open Access Journal of Contraception » Volume 11
Focused Family Planning Counseling Increases Immediate Postpartum Intrauterine Contraceptive Device Uptake: A Quasi-Experimental Study
Authors Wayessa MB ![]() , Abebe TW
, Abebe TW ![]() , Habtewold EM
, Habtewold EM ![]() , Adlo AM
, Adlo AM ![]() , Teklu AM
, Teklu AM ![]() , Abeya SG, Negero WO
, Abeya SG, Negero WO
Received 17 January 2020
Accepted for publication 10 April 2020
Published 21 August 2020 Volume 2020:11 Pages 91—102
DOI https://doi.org/10.2147/OAJC.S246341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Muleta Befkene Wayessa,1– 3 Tilaye Workineh Abebe,1– 3 Ephrem Mannekulih Habtewold,1– 3 Abebe Megerso Adlo,2 Alula M Teklu,2,3 Sileshi Garoma Abeya,2 Wakgari Olijira Negero1– 3
1Department of Gynecology and Obstetrics, Adama Hospital Medical College, Adama, Ethiopia; 2Department of Public Health, Adama Hospital Medical College, Adama, Ethiopia; 3Center for International Reproductive Health and Training Center at Michigan University, Addis Ababa, Ethiopia
Correspondence: Muleta Befkene Wayessa Tel +251 91 788-6932
Email [email protected]
Purpose: The aim of the study was to assess the effectiveness of focused family planning counseling (FFPC) in increasing postpartum intrauterine contraceptive device (PPIUCD) uptake among mothers who gave birth in the public health facilities of the towns of Adama and Olenchiti from April 1 to May 30, 2017.
Methods: A quasi-experimental study design was employed, taking a sample of 726 postpartum mothers: 484 in the non-intervention group (NIG) and 242 in the intervention group (IG). Focused family planning counseling was given to the IG using a newly designed cue card adapted from World Health Organization (WHO) guidelines and developed based on the constructs of the health belief model. Counseling based on a routine counseling approach was given to the NIG. The interviewer administered a semi-structured questionnaire for data collection. Data were analyzed using SPSS software, version 20. Descriptive statistics were used to characterize the study participants. The difference in the proportion of PPIUCD uptake in the two groups was tested using an independent Z-test at an alpha level of 0.05. Binary logistics regression was used to identify factors associated with the odds of taking IUCD. The significance of association was declared for P-values less than 0.05.
Results: The proportion of PPIUCD uptake in the IG [12.4%; 95% CI: 8.6, 17.4] was significantly higher than in the NIG [4.8%; 95% CI: 2.9, 6.7] with a P-value = 0.000. The odds of IUCD uptake among the IG was about 6 times higher (AOR: 5.92; 95% CI: 2.79, 12.60) than in the NIG. In addition, being unmarried women (AOR: 12.96; 95% CI: 4.30, 34.56), having higher education (AOR: 3.07; 95% CI: 1.13, 8.36), grand multiparity (AOR: 3.76; 95% CI: 1.58, 8.95), making a mutual decision (AOR: 0.16, 95% CI: 0.07, 0.38) and having a better knowledge of family planning (AOR: 5.92, 95% CI: 2.79, 12.60) were factors associated with uptake.
Conclusion: Providing FFPC immediately increases PPIUCD uptake. The uptake was also associated with marital status, education, parity, decision and knowledge on family planning.
Keywords: Adama, Ethiopia, IUCD, Olenchiti, Oromia, quasi-experimental
Introduction
Globally, family planning (FP) is recognized as a key life-saving intervention for mothers and their children. In particular, postpartum family planning (PPFP) is a method of preventing unintended pregnancy and closely spaced pregnancies throughout the 12 months following childbirth. PPFP is a strategy to reduce the unmet need for FP among postpartum women that have the greatest unmet need for FP. PPFP is also used to support longer birth intervals or reduce unintended pregnancies and their consequences. It is also used to allow those who wish to have children in the future to space their birth intervals and reach their desired family size (referred to as “spacers”) and those who wish to avoid future pregnancies (“limiters”).1
The postpartum period is a critical period when the probability of an unintended pregnancy happens. On the other hand, it is also typically a time of breastfeeding. Hence, this stage requires an FP method that both satisfies the need to prevent unplanned pregnancy and is appropriate for breastfeeding. In this regard, WHO recommends the lactational amenorrhea method (LAM) for mothers who exclusively breastfeed for 6 months and a copper-bearing intrauterine contraceptive device (IUCD) that can be inserted immediately or up to 48 hours after birth, or at any point after 4 weeks postpartum.2
A report from the Demographic and Health Surveys (DHS) of 43 countries that represent 61% of developing countries showed that postpartum women are more likely to use an injectable method or the lactational amenorrhea method for FP and less likely to use the female sterilization method. PPFP use was not strongly related to the age of the mother, parity, or the wanted status of the last birth. PPFP use was positively related to a mother’s urban location, wealth, education level, achievement of the desired family size, and current fertility desires and negatively related to her number of children under age 5.3
The use of modern FP methods during the postpartum period plays a key role in reducing the unmet need for FP4. About 10% of infant mortality and 20% of under-5-year child mortality can be prevented by increasing birth intervals. A longer birth interval can also protect mothers from obstetric-related complications5,6 PPFP has the potential to reduce 71% (53 million) of global unwanted pregnancies annually: 22 million unplanned births, 25 million induced abortions and 7 million fewer miscarriages.7 Analysis from 172 countries showed that without the use of FP, maternal mortality would be 1.8 times higher (equivalent to 614 000 deaths), meaning that its use eliminates 44.3% of maternal mortality.8
In Ethiopia, overall FP coverage and modern contraceptive use are the key indicators of maternal and child health, and they remain low (29% and 27%, respectively)6 Despite the demand for PPFP, many postpartum women do not access the FP information or services they need to delay or prevent subsequent pregnancies in sub-Saharan Africa. The extended postpartum (EPP) period is critical for addressing the unmet need for FP because it is a time women frequently encounter the health system.9,10
Women’s interest in avoiding pregnancies, especially in the first year postpartum, is well documented. Ross and Winfrey’s analysis of 27 DHSs found that only 3% of postpartum women wanted another baby within 2 years.11,12
A meta-analysis study demonstrated that after full-term or preterm delivery, an inter-pregnancy interval <12 months or <60 months (5 years) is associated with an increased risk of poor perinatal and maternal outcomes. Clearly meeting women’s desired spacing will also have public health effects. Studies from different settings in sub-Saharan Africa have indicated that postpartum abstinence is a common practice.13,14
Hence, the postpartum period requires optimization of a woman’s PPFP choices so she can choose the appropriate one for her. Especially in our setting, where the postpartum period is a challenging time in that the mother has less access to any FP method for reasons of distance, transportation, finances and cultural inconvenience. So, it is necessary to optimize an FP method that can be used for a longer period to prevent unplanned pregnancies and that is appropriate for breastfeeding. Standard counseling immediately after delivery and the use of an IUCD will better solve the unmet need for FP during this time. The study aimed to differentiate whether standard counseling can affect the use of an IUCD during the postpartum period because of its appropriateness.
Methods
The Aim, Design and Setting of the Study
The study aimed to assess whether the implementation of a newly designed focused family planning counseling approach can increase the immediate postpartum uptake of IUCD. A quasi-experimental study design was employed. The study was conducted among women who gave birth in public health facilities (hospital and health centers) of the city of Adama and town of Olenchiti in the Oromia region, of Ethiopia from April 1 to May 30, 2017. Adama is located about 100 km southeast of the capital city, Addis Ababa, on the rail line to Djibouti. Adama has a total population of more than 250 000, according to the 2007 Central Statistical Agency (CSA) report. In Adama, there are one governmental and four private hospitals. In addition, there are seven health centers that provide FP services. Nine gynecologists and 30 midwives provide FP service in Adama’s health facilities.
The town of Olenchiti is located 25 km east of Adama. The town has a total population of 23 924, of whom 5 294 are women of reproductive age. The town has one public health hospital and one health center. There are also eight private clinics, five drug stores and one pharmacy. Concerning health professionals, the town has about 16 general practitioners, 3 integrated emergency surgeons and obstetricians, and 14 midwives. The hospital in the town is a referral center for the Boset woreda’s population of more than 142 112.
Study Participants
All pregnant women who gave birth in the public health facilities of Adama and Olenchiti were considered the source population. The women who gave birth in selected public health facilities were considered the study population for the current study.
Intervention and Non-Intervention Groups
Intervention Group
The intervention group consisted of women who gave birth in selected public health facilities of Adama (Adama Hospital Medical College [AHMC] and Adama Health Center) and counseled for an IUCD based on the newly designed counseling tool or cue card. This cue card was focused and developed based on the four constructs of the health belief model (HBM): perceived susceptibility, perceived seriousness, perceived benefits and barriers. These four constructs were considered during the preparation of the content of the cue card and procedures for providing counseling service, as was the WHO cue FP guideline. Counseling was provided by midwives, who were trained on the new cue card before performing the intervention. In the intervention setting, about three counselors were trained in the newly designed counseling. Three health professionals were also trained in data-collection tools and procedures. The counseling was organized into 4 main sessions, each of which lasts about 9 minutes. The 4 sessions are sessions for introduction and rapport-building (1 minute), exploration (3 minutes), and a decision on the options (2 minutes). Implementation sessions last 2 minutes (see Annex 1).
Non-Intervention Group
The non-intervention group (NIG) consisted of women who gave birth at Olenchiti Hospital. For a woman in this group, counseling was provided based on the routine national FP counseling approach. The guideline is not focused, which can be challenging for the providers in terms of the time required for its implementation. Currently, due to increased numbers of clients in the study settings, there is insufficient time to implement the routine counseling approach. In this group, counseling was provided by midwives who had previous training on the routine national FP counseling approach. Even though the routine counseling approach is longer and lacks focus, the counselors at non-intervention sites were oriented regarding the research and how counseling procedures should be implemented per the guideline. In the non-intervention setting, about five health professionals were trained on the data-collection tools and procedures.
Inclusion Criteria
Pregnant women who came to the selected public health facilities for delivery service and those who gave birth in other health facilities and then came to the postnatal units of the selected health facilities during their immediate postpartum period were included in the study.
Exclusion Criteria
Excluded from the study were mothers who had achieved their ideal family size and opted for a permanent FP method, those who had intrapartum fetal loss (optional, based on their number of living children and desire to participate) and women with contraindications for an IUCD.
Sample Size and Sampling Procedure
The sample size was calculated using a formula designed to test the difference between two population proportions in experimental study designs.15 In determining the sample size for the two groups, the required statistical assumptions (a 95% level of confidence, 80% power, proportion of IUCD uptake in the NIG [ ],16 the hypothesized proportion of IUCD uptake in the IG (
],16 the hypothesized proportion of IUCD uptake in the IG ( ) and a 2:1 ratio of the NIG to the IG) were considered. Accordingly, 484 women from the NIG (n1) and 242 women from IG (n2) were sampled for the current study. Since the attendance of women for the service was assumed to be random, they were consequently selected for the study in their respective groups.
) and a 2:1 ratio of the NIG to the IG) were considered. Accordingly, 484 women from the NIG (n1) and 242 women from IG (n2) were sampled for the current study. Since the attendance of women for the service was assumed to be random, they were consequently selected for the study in their respective groups.
Data Collection
The first women who fulfilled the inclusion criteria were identified by data collectors. After requesting a woman’s consent, data regarding her socio-demographic, obstetric and other characteristics were collected using an interview-administered questionnaire. Then, women in the IGs were counseled on FP options based on the newly designed cue card; women in the NIGs, however, were counseled per the routine counseling approach. Finally, the woman’s decision to accept a contraceptive method and her choice were asked. Woman’s decision and the type of contraceptive method were recorded on decision form (Annex 2). Interviewer administered structured questionnaire and decision form were used for data collection. The questionnaire and decision form were first prepared in English, then translated into the Afan Oromo and Amharic languages, which are commonly spoken in the study setting. To check for consistency of the translation, the questionnaire and decision form were translated back into English. Midwives holding at least a diploma who spoke Afan Oromo or Amharic were assigned to collect data. Before data collection, training was given on the overall data-collection procedures. The questionnaire was pretested and checked for clarity and a logical sequence on 5% of the sample before actual data collection began. The log book was also reviewed to retrieve important data for the study. Two supervisors (one for intervention and one for the non-intervention area) were recruited and trained to supervise the data-collection process. Data were assessed by trained supervisors for completeness and consistency during the data-collection period.
Study Variables
Dependent Variables
IUCD uptake (grouped into Yes or No)
Independent Variables
- Socio-demographic variables: mother’s age, residence, marital status, occupation, education, partner’s education, monthly income
- Obstetric variables: age at first marriage, gravidity, history of abortion, number of living children, children’s sex composition at household level, preference for sex of child, plan to have more children
- Other variables: decision-makers in choice to have children, level of knowledge, attitude toward IUCD
Analysis
The collected data were coded and entered into SPSS software, version 20. Data-processing tasks, such as data cleaning, categorizing and transforming, were then performed to ready the data for analysis. Descriptive analysis was performed to explore the characteristics of the study participants in each group across their different socio-demographic, obstetric and other variables. The difference in the proportion of IUCD uptake in the IGs and NIGs was tested using an independent Z-test statistics at alpha 5%  17 Accordingly, the null hypothesis that the proportion of IUCD uptake in the IGs and NIGs would be similar was rejected due to the corresponding P-value for the test statistics being less than 0.05. Binary logistic regression analysis was next used to identify the determinants of postpartum IUCD uptake. The predictive model was developed using a standard model-building approach. In the process of building the model, first, a simple logistic regression analysis was performed to screen candidate variables that had a crude association with postpartum IUCD uptake at alpha = 0.25.18 The selected candidate variables were then subjected to a multiple logistic regression model to estimate their adjusted effects on postpartum IUCD uptake. The statistical significance of independent variables in the final predictive model of postpartum IUCD uptake was declared at alpha <0.05. Model adequacy assessment was performed before declaring the potential determinants of postpartum IUCD uptake using different model diagnosis statistics. The final fitted model was assessed for multicollinearity using Variance Inflation Factor (VIF)19 and goodness of fit using Hosmer and Lemeshow tests.18 Accordingly, the mean VIF value was found to be 1.62, indicating the absence of multicollinearity among the covariates in the fitted regression model. The corresponding p-value for the Hosmer and Lemeshow tests’ statistics indicated that the model was well fitted, with P-value = 0.16. The model’s ability to correctly classify those subjects who experienced outcomes of interest and those who did not was assessed using a Receiver Operating Characteristics (ROC) curve.18,19 Accordingly, the diagnosis revealed that the area under the ROC curve was 84.16%. This indicated that the fitted model was correctly classified for about 84.16% of the subjects. The parsimonious model that best explained the data with a minimum of free parameters was selected using Akaike Information Criteria (AIC).20 Finally, the magnitude of association between the independent variables and postpartum IUCD uptake was estimated using an odds ratio with a 95% confidence interval.
17 Accordingly, the null hypothesis that the proportion of IUCD uptake in the IGs and NIGs would be similar was rejected due to the corresponding P-value for the test statistics being less than 0.05. Binary logistic regression analysis was next used to identify the determinants of postpartum IUCD uptake. The predictive model was developed using a standard model-building approach. In the process of building the model, first, a simple logistic regression analysis was performed to screen candidate variables that had a crude association with postpartum IUCD uptake at alpha = 0.25.18 The selected candidate variables were then subjected to a multiple logistic regression model to estimate their adjusted effects on postpartum IUCD uptake. The statistical significance of independent variables in the final predictive model of postpartum IUCD uptake was declared at alpha <0.05. Model adequacy assessment was performed before declaring the potential determinants of postpartum IUCD uptake using different model diagnosis statistics. The final fitted model was assessed for multicollinearity using Variance Inflation Factor (VIF)19 and goodness of fit using Hosmer and Lemeshow tests.18 Accordingly, the mean VIF value was found to be 1.62, indicating the absence of multicollinearity among the covariates in the fitted regression model. The corresponding p-value for the Hosmer and Lemeshow tests’ statistics indicated that the model was well fitted, with P-value = 0.16. The model’s ability to correctly classify those subjects who experienced outcomes of interest and those who did not was assessed using a Receiver Operating Characteristics (ROC) curve.18,19 Accordingly, the diagnosis revealed that the area under the ROC curve was 84.16%. This indicated that the fitted model was correctly classified for about 84.16% of the subjects. The parsimonious model that best explained the data with a minimum of free parameters was selected using Akaike Information Criteria (AIC).20 Finally, the magnitude of association between the independent variables and postpartum IUCD uptake was estimated using an odds ratio with a 95% confidence interval.
Results
Socio-Demographic Characteristics of Subjects
In this study, 726 postpartum mothers who delivered in the public health facilities of Olenchiti and Adama were included. We sampled 246 women as the IG and 484 as the NIG from the 2 study settings. Our analysis revealed that about 105 (44.3%) women in the IG and 175 (37%) in the NIG were aged 25–29 years. The result indicated that about 115 (47.5%) women in the IGs and 246 (51.2%) in the NIGs followed the Orthodox religion. Regarding educational status, 33 (13.7%) women in the IG and 70 (14.5%) in the NIG had no formal education. About 227 (94.6%) of women in the IG and 463 (96.5%) in the NIG were married. Regarding occupational status, 47 (19.4%) of the IG and 78 (16.3%) in the NIG were employed, while 80 (33.1%) in the IG and 330 (68.9%) in the NIG were homemakers. One hundred and ten (45.5%) women in the IG and 309 (65.2%) in the NIG were urban residents. Ninety (38.1%) in the IG and 159 (33.1%) in the NIG had male partners who had completed high school. Seventy-seven (32%) of the IG and 157 (34.1%) of the NIG had an employed partner (Table 1).
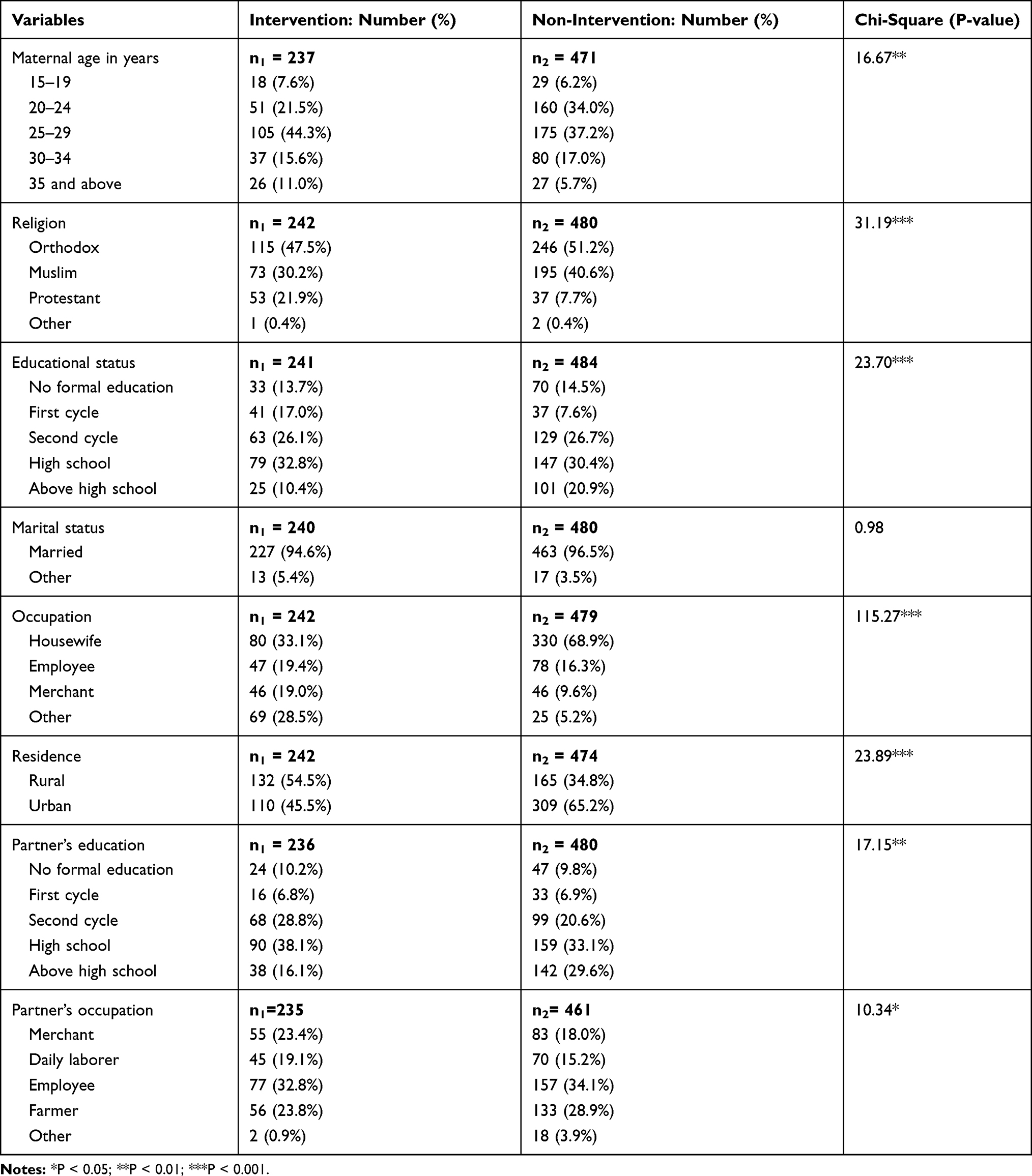 |
Table 1 Socio-Demographic Characteristics of Women Who Delivered at AHMC and Olenchiti Hospital, 2017 |
Obstetric Characteristics of Women
The study found that 120 (54.5%) in the IG and 248 (54%) in the NIG were first married between 19 and 24 years old. One hundred and eleven (46.1%) women in the IG and 247 (51%) in the NIG had a history of 2 to 4 pregnancies. Forty-two (17.6%) in the IG and 89 (18.6%) in the NIG had a history of abortion. One hundred and sixty-two (67.8%) of women in the IG and 347 (72.7%) in the NIG had up to 2 children at home. The proportion of women who did not have a sex preference for their child were 134 (55.8%) in the IG and 170 (35.7%) in the NIG. One hundred and ninety-one (82%) in the IG and 323 (68.1%) in the NIG planned to have more children. Regarding who made decisions about having children, 194 (81.5%) women in the IG and 218 (47.1%) in the NIG played a role in decision-making along with their partners. Per the result of the current study, 92 (38.2%) in the IG and 202 (41.8%) in the NIG had relatively higher knowledge, and the women who had a relatively good attitude numbered 183 (76.2%) in the IG and 292 (61.5%) in the NIG (see Table 2).
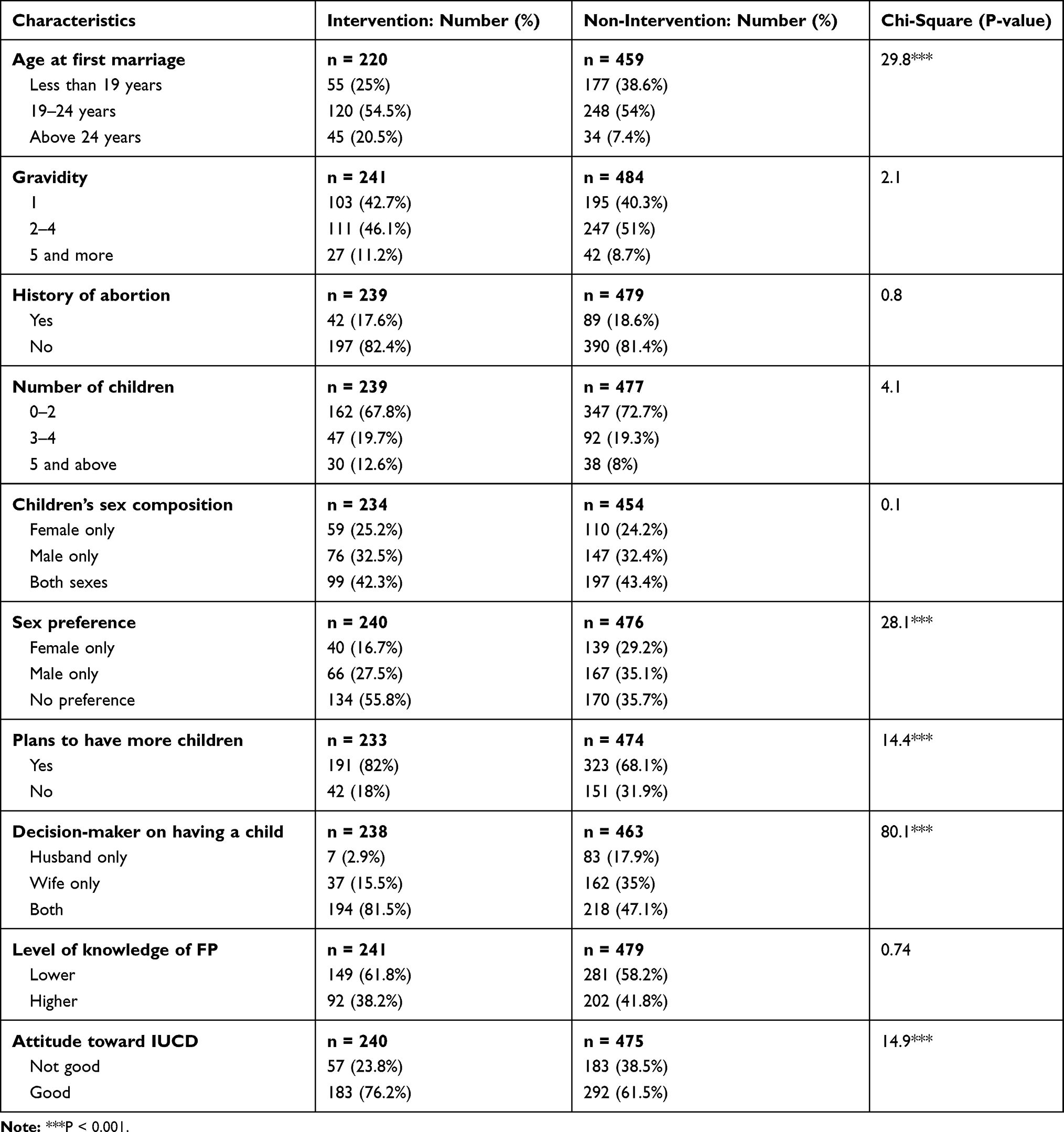 |
Table 2 Obstetric Characteristics of Women Delivering at AHMC and Olenchiti Hospital, 2017 |
Uptake of PPIUCD in Intervention and Non-Intervention Groups
The proportion of mothers who received an IUCD was 12.4% (95% CI: 8.6, 17.4) in the IG and 4.8% (5% CI: 2.9, 6.7) in the NIG. The difference in IUCD uptake in the two groups was tested using Z-test statistics at alpha = 0.05. According to the result of analysis, there was a statistically significant difference in the proportion of IUCD uptake between the women in the two groups (P-value <0.05). We observed that the proportion of mothers who received an IUCD in the IG was significantly higher than in the NIG. Similarly, we tested the difference in postpartum IUCD uptake in the IG against the hypothesized proportion of 5.3%. Accordingly, the proportion of mothers who received an IUCD in the IG was significantly higher (12.4%; 95% CI: 8.6, 17.4) compared to the hypothesized proportion of postpartum IUCD uptake (P-value <0.05).
Socio-Demographic and Economic Factors Associated with Postpartum IUCD Uptake
Factors associated with postpartum IUCD uptake were identified using binary logistic regression analysis. First, a simple logistic regression analysis was used to identify candidate variables for a multiple logistic regression model. At this level, the designed counseling cue card for intervention, maternal age, marital status, occupation, partner’s level of education, gravidity, number of children, children’s sex composition, plans to have more children, decision-making on having a child and level of knowledge were selected as candidate variables at P-value <0.25.
All selected candidate variables were subjected to multiple logistic regression models to estimate their adjusted effect on postpartum IUCD uptake after controlling for all possible confounding variables. Accordingly, after adjusting for all possible confounders, the designed counseling for intervention was found to be a significant predictor of IUCD uptake. Besides marital status, education, gravidity, decision-making on having a child and level of knowledge of FP were significantly associated with postpartum IUCD uptake.
The current study revealed that intervening using the designed FP counseling cue card was associated with odds 5.92 (AOR = 5.92; 95% CI: 2.79, 12.60) times higher of using postpartum IUCD compared to the intervening routine counseling approach. This study also showed that being an unmarried woman was associated with odds 12.19 (AOR = 12.96; 95% CI: 4.30, 34.56) times higher of using an IUCD compared to married women. Compared to having no formal education, women who attained a high school education were associated with odds 77% (AOR = 0.23; 95% CI: 0.06, 0.94) lower of using an IUCD, while women who had attained higher education were associated with odds 3.07 (AOR = 3.07; 95% CI: 1.13, 8.36) times higher of using IUCD in the postpartum period (see Table 3).
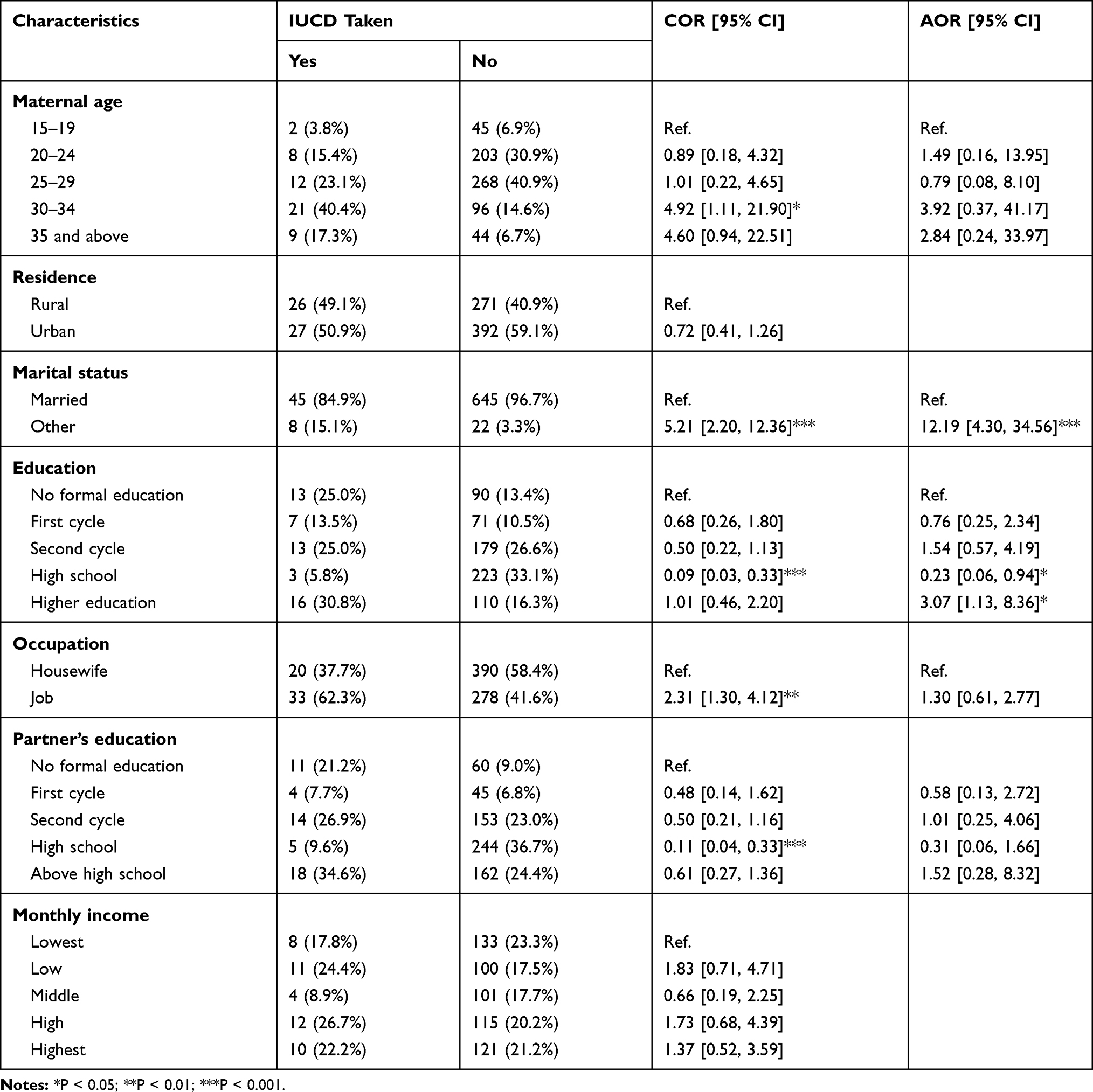 |
Table 3 Socio-Demographic and Economic Factors Associated with Postpartum IUCD Uptake Among Women Who Delivered at AHMC and Olenchiti Hospital, 2018 |
Obstetric and Knowledge-Related Factors Associated with Postpartum IUCD Uptake
This study showed that woman who had five or more previous pregnancies had odds 3.76 (AOR = 3.76; 95% CI: 1.58, 8.95) times higher of using an IUCD, and women who had 2 to 4 previous pregnancies had odds 7.78 (AOR = 7.78; 95% CI: 2.76, 21.93) times higher of using an IUCD compared to women who had only 1 previous pregnancy. Per the current study’s findings, women who were solely responsible for the decision to have a child were associated with 90% (AOR = 0.010; 95% CI: 0.03, 0.33) lower odds of using an IUCD than women whose partners were solely responsible; those who made the decision together with their partners were associated with 84% (AOR = 0.16; 95% CI: 0.07, 0.38) lower odds. Women with higher knowledge of FP had odds of using an IUCD 5.92 (AOR = 5.92; 95% CI: 2.79, 12.60) times greater than women who had a lower level of knowledge (see Table 4).
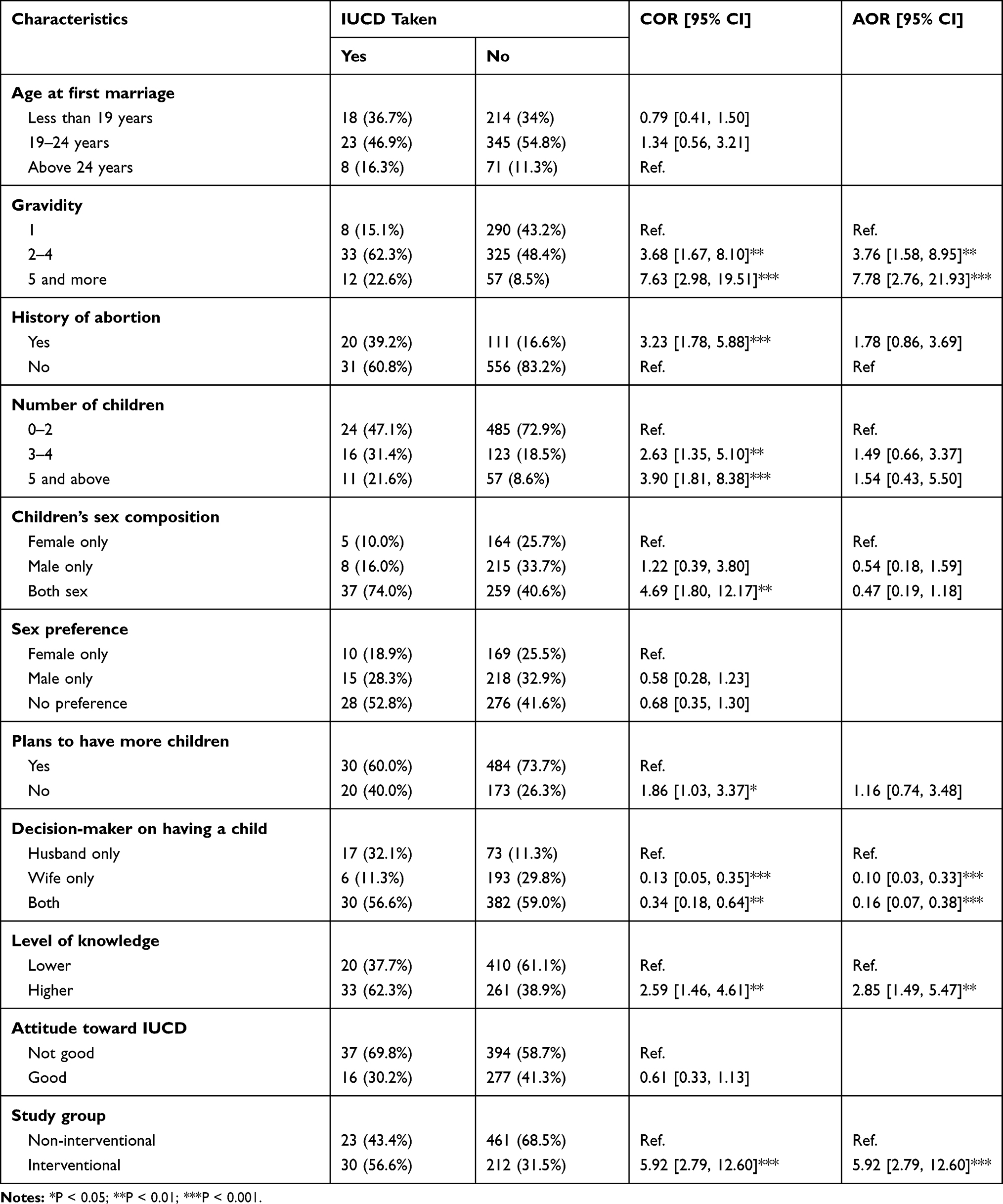 |
Table 4 Obstetric and Knowledge-Related Factors Associated with Postpartum IUCD Uptake Among Women Who Delivered at AHMC and Olenchiti Hospital, 2018 |
Discussion
The current study aimed to test whether the intervention of the newly designed focused FP counseling approach would increase postpartum IUCD uptake compared to the routine FP counseling approach. The study revealed that the proportion of postpartum IUCD uptake was significantly higher among women who were counseled by the newly designed FP counseling approach than among those counseled by the routinely implemented approach. It was also observed that the odds of using IUCD during the postpartum period were almost 6 times higher among the women counseled with the new approach than among those counseled with the routinely implemented approach. These findings may be attributable to the organization of counseling procedures and the time required to implement them. The procedures in the newly designed approach were organized based on the basic constructs of the health belief model: the most widely used model to study health service use, specifically to explain why people do not use health services.21 The integration of this model perspective in the counseling approach is helpful for identifying exhaustively why IUCD is not used during the postpartum period and addresses these reasons accordingly.
Furthermore, the newly designed approach takes significantly less time to implement than the routine approach. The provision of FP counseling using the routine approach may be challenged by time constraints as a result of a high patient load per a health service provider in the current study settings. With this consideration, the new counseling approach was designed to be implemented within a short time: only 9 minutes. Being focused and more practical in the current context of the health service delivery system, the newly designed counseling may be more efficient at persuading women to use an IUCD during the postpartum period within the intended time.
The current study also observed higher odds of postpartum IUCD uptake among women with more education. This association was also observed in studies done in Nigeria and Uganda.22,23 Postpartum IUCD uptake was also higher among women who had good knowledge of FP, similar to findings from a study in Ghana.24 Education can play a significant role in women’s use of a long-acting contraceptive method in general and IUCD in particular. Having more education creates opportunities for women to be employed and engage most of their time in a job in addition to responsibilities they have in their families. Even if they have basic reproductive health rights as a result of their expected responsibilities in their workplace, they may be prevented from having more closely spaced pregnancies. Furthermore, educated women may have more access to information regarding the obstetric consequences of closely spaced pregnancies and the benefits of using long-acting FP methods immediately after a pregnancy. Education can also give women a good level of knowledge about FP, which helps them analyze the comparative advantages of using contraceptive methods and makes them more likely to make informed decisions compared to women with a low level of knowledge.25
The current study observed that having a larger number of previous pregnancies was associated with higher odds of using an IUCD during the postpartum period. This finding is in line with a study done in Nigeria.22 This association may be explained by a reduced pregnancy desire among women with a larger number of previous pregnancies. Based on their experiences with previous pregnancies and with the sacrifices required for their growing children, women of multigravidities may have less desire for additional pregnancies.
According to the current study’s findings, contrary to the male partner being the sole decision-maker on family issues, the likelihood of women’s using an IUCD during the postpartum period was lower when they made the decision either alone or together with their partners; a similar observation was found in a study done with African American women.26 This may be due to husbands’ remaining highly autonomous in deciding whether or not the woman should use an IUCD or be pregnant rather than their mutual or the women’s sole interest.
Our study revealed that many potential clients in SSA lack information or have misconceptions about long-acting and permanent contraception methods.27 As this study concerns FP, it may be necessary to control social desirability bias to some extent, especially among mothers from rural areas. Except for this minimum limitation, this study will serve as a set of baseline information for government organizations working in the health sector and for other stakeholders, as well as for decision-makers related to FP, particularly IUCD.
Conclusion
Based on the current study’s findings, keeping constant other factors, such as education, marital status, level of knowledge about FP, number of previous pregnancies and who makes decisions on family issues, the counseling approaches significantly determined the highest odds of women adopting IUCD during their postpartum period. Therefore, along with improving women’s education, empowering them and increasing their knowledge about FP, the currently implemented counseling approaches should be revised so that they can be efficiently integrated and implemented in the existing context of the health service delivery system.
Abbreviations
AHMC, Adama Hospital Medical College; ANC, Antenatal Care; AOR, Adjusted Odds Ratio; CI, Confidence Interval; CIRHT, Center for International Reproductive Health Training, University of Michigan; COR, Crude Odds Ratio; CSA, Central Statistical Agency; DHS, Demographic and Health Survey; EDHS, Ethiopian Demographic and Health Survey; FP, Family Planning; IUCD, Intrauterine Contraceptive Device; KM, Kilometer; LAFP, Long-Acting Family Planning; NGO, Non-Government Organization; PPFP, Postpartum Family Planning; SD, Standard deviation; WHO, World Health Organization.
Data Sharing Statement
The data for the current study were obtained from the study participants and, with a formal request, can be obtained from the principal investigator Dr. Muleta Befkene Wayessa.
Ethics Approval and Informed Consent
Ethical clearance was obtained from the Institutional Ethics Review Board of Adama Hospital Medical College. All concerned officials were notified about the purpose of the study. The study was conducted in accordance with the Declaration of Helsinki. The consent process outlined in Annex 3 was approved by the Ethics Review Board of Adama Hospital Medical College. Since significant numbers of women in the study setting were unable to read or write, informed consent was obtained verbally from each study participant before data were collected. The data’s confidentiality was assured by using code as identification; the mothers’ names were not recorded (see Annex 3).
Consent for Publication
Not applicable.
Acknowledgments
We would like to express our gratitude to Adama Hospital Medical College for its support in accomplishing this proposal. Our particular appreciation goes to the Center for International Reproductive Health Training at the University of Michigan (CIRHT) for its financial and technical support to conduct this study. We would like to extend our appreciation to Adama city and Olenchiti town Health Office staff and leaders for their support to realize data collection. Finally, we are grateful to the study participants for their time and cooperation in conducting this study.
Author Contributions
All authors contributed to data analysis and drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. WHO. Programming Strategies for Postpartum Family Planning; 2019b.
2. WHO. Meeting the Family Planning Need of Postpartum Women; 2009.
3. Winfrey W, Rakesh K Use of family planning in the postpartum period. DHS Comparative Report 36. ICF International, USAID, 2014;September.
4. Shastri VD. Family planning needs during the extended postpartum period in a high fertility state “Bihar” in Northern India. SSRN Electronic J. 2012. doi:10.2139/ssrn.2579228
5. Bakamjian LCS, Cianci S, Malandrino C, et al. Programming strategies for postpartum family planning. Eur J Obstet Gynecol Reprod Biol. 2013;13:23.
6. Central Statistical Agency, ICF International. International Ethiopia Demographic and Health Survey. Ethiopia and Calverton, MD: Addis Ababa;2012.
7. WHO. Packages of Interventions for Family Planning, Safe Abortion Care, Maternal, Newborn and Child Health; 2010.
8. Ahmed S, Li Q, Liu L, Tsui AO. Maternal deaths averted by contraceptive use: an analysis of 172 countries. Lancet. 2012;380(9837):111–125. doi:10.1016/S0140-6736(12)60478-4
9. WHO, World Bank. Trends in Maternal Mortality:1990 to 2010; 2012.
10. Lauro D. Abortion and contraceptive use in sub-Saharan Africa: how women plan their families. Afr J Reprod Health. 2011;15(1):13–23.
11. Eleje GU, Ezebialu IO, Eke NO. Inter-Pregnancy interval (IPI): what is the ideal? Afrimedic J. 2011;2(1):36–38.
12. DaVanzo J, Hale L, Razzaque A, Rahman M. Effects of interpregnancy interval and outcome of the preceding pregnancy on pregnancy outcomes in Matlab, Bangladesh. BJOG. 2007;114(9):1079–1087. doi:10.1111/j.1471-0528.2007.01338.x
13. Rossier C, Hellen J. Traditional birthspacing practices and uptake of family planning during the postpartum period in Ouagadougou: qualitative results. Int Perspect Sex Reprod Health. 2014;40(2):87–94. doi:10.1363/4008714
14. Adeyemi A, Ijadunola K, Orji E, Kuti O, Alabi M. The unmet need for contraception among Nigerian women in the first year post-partum. Eur J Contracept Reprod Health Care. 2005;10(4):229–234. doi:10.1080/13625180500279763
15. Wittes J. Sample size calculations for randomized controlled trials. Epidemiol Rev. 2002;24(1):39–53. doi:10.1093/epirev/24.1.39
16. [Ethiopia], CSA. Ethiopia Mini Demographic and Health Survey. Ethiopia: Addis Ababa; 2014.
17. Daniel WW, Cross CL. Biostatistics a Foundation for Analysis in the Health Sciences.
18. Hosmer DW, Lemeshow S. Applied Logistic Regression.
19. Forthofer RN, Lee ES, Hernandez M. Biostatistics: A Guide to Design, Analysis, and Discovery.
20. Burnham KP, Anderson DR. Model Selection and Multimodel Inference.
21. Glanz K. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health. 2010;31:399–418. doi:10.1146/annurev.publhealth.012809.103604
22. Eluwa GI, et al. Success providing postpartum intrauterine devices in private-sector health care facilities in Nigeria: factors associated with uptake. Global Health. 2016;4(2):276–283.
23. Rutaremwa G, et al. Predictors of modern contraceptive use during the postpartum period among women in Uganda: a population-based cross sectional study. BMC Public Health. 2015;15(1):262. doi:10.1186/s12889-015-1611-y
24. Robinson N, et al. Barriers to intrauterine device uptake in a rural setting in Ghana. Health Care Women Int. 2016;37(2):197–215. doi:10.1080/07399332.2014.946511
25. Pasha O, et al. Postpartum contraceptive use and unmet need for family planning in five low-income countries. Reprod Health. 2015;12(2):S11. doi:10.1186/1742-4755-12-S2-S11
26. Weston MR, et al. Factors influencing uptake of intrauterine devices among postpartum adolescents: a qualitative study. Am J Obstet Gynecol. 2012;206(1):40,e140,e7. doi:10.1016/j.ajog.2011.06.094
27. Nalwadda G, et al. Persistent high fertility in Uganda: young people recount obstacles and enabling factors to use of contraceptives. BMC Public Health. 2010;10(1):530. doi:10.1186/1471-2458-10-530
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.