Back to Journals » International Medical Case Reports Journal » Volume 17
Fluoroquinolone-Associated Tendinopathy: An Important Complication of Cyst Infection Management in Polycystic Kidney Disease
Authors Kaneko M, Akimoto T ![]() , Nagata D
, Nagata D ![]()
Received 1 April 2024
Accepted for publication 13 August 2024
Published 6 September 2024 Volume 2024:17 Pages 777—781
DOI https://doi.org/10.2147/IMCRJ.S471718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Miwa Kaneko, Tetsu Akimoto, Daisuke Nagata
Division of Nephrology, Department of Internal Medicine, Jichi Medical University, Tochigi, Japan
Correspondence: Tetsu Akimoto, Division of Nephrology, Department of Internal Medicine, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke-Shi, Tochigi, 329-0498, Japan, Tel +81-285-58-7346, Fax +81-285-44-4869, Email [email protected]
Abstract: A 68-year-old man on hemodialysis treatment for end-stage kidney disease secondary to autosomal dominant polycystic kidney disease (ADPKD) complained of right ankle pain that impaired walking ability two weeks after the initiation of intravenous levofloxacin as a treatment for concomitant liver cyst infection. A systemic workup led us to conclude that our patient had a fluoroquinolone-associated tendon injury. Such a disease condition has been recognized as a serious adverse event resulting from the receipt of fluoroquinolones in various clinical settings. Fluoroquinolones have received focus as standard therapeutic agents for liver and/or renal cyst infection because of their lipophilic properties that lead to good penetration into infected cysts. However, reports on fluoroquinolone-associated tendinopathy in patients with ADPKD associated with cyst infection are sparse. We believe the current report illustrates the pitfalls associated with managing patients with ADPKD who are subjected to the administration of fluoroquinolones due to infectious complications.
Keywords: ADPKD, renal failure, cyst, infection, fluoroquinolone-associated tendon injuries
Introduction
Patients with autosomal dominant polycystic kidney disease (ADPKD) may present with several symptoms, such as a fever and abdominal pain, because of liver and/or renal cyst infection.1,2 Due to their pharmacodynamic nature characterized by favorable penetration into cysts, lipid-soluble antibiotics, such as fluoroquinolones, have received focus as standard therapeutic agents for the disease.1 On the other hand, fluoroquinolone-associated tendon injuries have gained increased attention and reports on this topic are modestly but steadily accumulating;3–5 however, literatures on this subject among patients with ADPKD are lacking.
We herein report one such case in an end-stage kidney disease patient with ADPKD complicated by hepatic cyst infection.
Case Report
A 68-year-old anuric male patient undergoing regular hemodialysis (HD) treatment for end-stage kidney disease secondary to ADPKD was admitted to our hospital because of recurrent upper right flank pain. He had been suffering from a hepatic cyst in the context of the disease. At 38 years old, he was diagnosed with ADPKD based on a positive family history. His grandfather had a history of subarachnoid hemorrhage. He was subjected to the creation of an autogenous arteriovenous fistula in his forearm eight years prior, at which point regular HD treatment three times per week was commenced. The course of HD, which required heparinization for anticoagulation, was uneventful, and his casual blood pressure, including the HD session, was well controlled at approximately 120/70 mmHg with amlodipine besilate 5 mg/day and telmisartan 40 mg/day. He also underwent treatment for hyperphosphatemia with calcium carbonate 3000 mg/day, thereby leading to phosphorus levels ranging from 4.0 to 5.5 mg/dL, while his serum levels of calcium and intact parathyroid hormone (PTH) had been maintained at approximately 9.0 mg/dL and 90 pg/mL, respectively. His medical history also included insomnia, for which he received sporadic medical care. He had a 24-pack-year history of cigarette smoking and no exposure to a specific environment or activity. The patient denied any history of allergies.
Three months prior to this admission, he had developed hepatic cyst infection due to Klebsiella pneumoniae, which was detected in the blood culture. At that time, the patient had right-sided abdominal pain, an intermittent fever with chills, and reduced appetite. Elevated serum levels of C-reactive protein (CRP) of 17.52 mg/dL and procalcitonin (PCT) 2.48 ng/mL were also noted. Although initial management with empirical intravenous meropenem achieved limited disease control, the patient was favorably managed with a 5-week course of intravenous cefotaxime (2 g, daily) combined with oral metronidazole (500 mg, thrice daily), which led to a consequent decrease in CRP to 0.9 mg/dL, under multidisciplinary collaboration involving surgeons and infectious disease specialists. Four weeks after quitting treatment, he started to complain of abdominal symptoms again; thus, he was admitted to our hospital.
At the time of admission (clinical day 0), his body temperature was 37.1 °C. A laboratory evaluation revealed the following results: white blood cell count (WBC), 4300/µL; hemoglobin, 11.3 g/dL; platelet count, 10.4 × 104/µL; serum creatinine, 6.69 mg/dL; aspartate aminotransferase, 19 U/L; alanine aminotransferase, 9 U/L; lactate dehydrogenase, 210 U/L; gamma-glutamyl transferase, 118 U/L; alkaline phosphatase, 517 U/L; CRP, 5.17 mg/dL; and PCT, 0.432 ng/mL. After confirming the patient’s clinical presentation, we reintroduced the same therapeutic regimen. However, a generalized pruritic erythematous rash involving his chest, abdomen, trunk, arms, and lower extremities became remarkable four days after resuming treatment; thus, he was suspected of having a drug allergy. Both cefotaxime and metronidazole were discontinued and substituted with intravenous levofloxacin (500 mg, every 48 h). While investigations at that time revealed an elevated CRP level of 4.59 mg/dL, the right flank pain as well as the itching subsided, and the CRP level decreased to 0.57 mg/dL two weeks later when the patient developed right ankle pain impairing his walk ability despite bed rest without any physical activity.
Magnetic resonance (MR) imaging of the right ankle indicated the presence of inflammation in the soft tissue around the right Achilles tendon (Figure 1); therefore, the patient was suspected to have fluoroquinolone-associated tendinopathy. We decided to switch the levofloxacin to oral doxycycline (200 mg/day) and alleviate the strain to the tendon. Three weeks later, his leg symptoms improved, and walking resumed without difficulty, while his serum CRP levels fluctuated ranging from 3.7 to 4.5 mg/dL. The patient did not complain of right flank pain or pruritic rash and was discharged (Figure 2).
 |
Figure 1 MR imaging findings of the ankles. Axial (A) and coronal (B) T2-weighted short inversion time inversion recovery images show a high signal intensity (arrows), a finding suggestive of an edematous change due to inflammation, in the anterior region of the right Achilles tendon (an asterisk in panel (A) surrounded by the soleus, flexor digitorum longus, and peroneus brevis muscles. |
 |
Figure 2 The time course of the patient. After making a diagnosis of fluoroquinolone-associated tendinopathy, levofloxacin was discontinued and oral doxycycline was commenced. Over the next three weeks, the patient’s right leg manifestations gradually subsided without any exacerbation of abdominal symptoms despite the absence of significant improvement in his serum CRP levels. Abbreviation: MRI, MR imaging. |
During the next two months, the patient did not experience recurrence of right ankle pain; however, he died of fatal cerebral bleeding despite the fact that periodic intracranial screening with MR angiography had not detected any structural vascular abnormalities, such as aneurysms. Oral antibiotic treatment was continued until two weeks before he passed away.
Discussion
Tendinopathy has been recognized as a serious adverse event resulting from the receipt of fluoroquinolones in various clinical settings.3–5 One may therefore argue that the clinical scenario of the present patient may simply be too common to have been described in the literature; however, the significance of our experience should be evaluated carefully given the paucity of case reports describing this pathology in patients with ADPKD, despite the current therapeutic trends preferring quinolone-based regimens over using water-soluble antibiotics for concomitant cyst infections.1,2,6–8
Fluoroquinolone administration appears to result in development of the disease within a few weeks, with an estimated incidence ranging from 0.14% to 0.4% in the general population.3–5 However, such disorders may occur up to several months after the initiation of the treatment and even after quitting the agents.3 Although there is a predilection for the Achilles tendon, other body parts, including the shoulder and hands, can be affected as well.5 An abrupt onset and spontaneous acute pain upon walking and/or palpation can help distinguish the disease from other forms of tendinopathy.9 Occasionally, substantial swelling at the dependent portion, which mimics phlebitis, can be noted, but the symptoms can be bilateral, partial, or complete, and the injury may be located 2 to 3 cm above a poorly vascularized region.10
The pathogenic basis for the link between quinolones and tendon injury remains to be delineated; however, numerous potential sources have been proposed, including an ischemic vascular process, direct toxicity to collagen oxidative damage, and structural specificity of quinolone molecules.4,10,11 Although abnormal extracellular matrix production is one of the hallmarks of ADPKD,12 no relevant data indicating a link between such an abnormality and the onset of tendon injury are currently available. To date, several factors have been recognized as risk factors for this pathology (Table 1), with advanced age, concomitant steroid use and renal insufficiency being the most common.3–5,10 Several studies have demonstrated that the risk of tendon injury varies depending on the fluoroquinolone type; however, most tenotoxic agents remain to be delineated since a lack of consensus exists in the literature.3,5,11,13,14 While the diagnosis of fluoroquinolone-associated tendinopathy is commonly based on clinical manifestations and a physical examination, MR imaging has received focus as a useful investigative tool for detecting and monitoring pathogenic changes during the observation period.5,10,15,16 This was also the case in the present patient, making the diagnostic process straightforward. We acknowledged that patients undergoing regular HD treatment with uncontrolled high PTH levels have a high risk of tendon rupture and bone fracture;17,18 however, we believe that the role of such a disorder for the onset of tendinopathy in the present patient would be marginal considering the patient’s laboratory findings. The prompt relief of leg symptoms after the discontinuation of levofloxacin should support our conclusion.
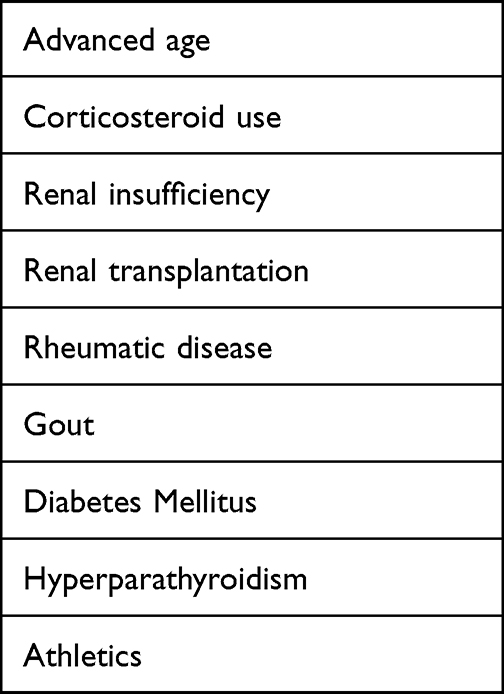 |
Table 1 Risk Factors for Fluoroquinolone-Associated Tendinopathy |
The development of liver and/or renal cysts, which may be associated with various complications, including intracystic bleeding, gross hematuria, and cyst infections, is the most characteristic feature of ADPKD.1,2 The diagnostic and therapeutic managements of liver and/or renal cyst infections remain clinical challenges, and no evidence-based strategy for how to address these disease states has been established.2,6 As a matter of course, the choice of antibiotic to use in treating infected cysts is an issue of debate.19 In ordinary clinical settings, fluoroquinolones and third-generation cephalosporins seem to be selected as the standard therapeutic agents for cyst infections in patients with ADPKD,2 although the former may be preferred over the latter because of their bactericidal activity against Gram-negative enteric pathogens and their lipophilic properties that lead to good penetration into infected cysts.1,2
At present, why information on fluoroquinolone-associated tendinopathy among patients with ADPKD is lacking is unclear. This disease state may simply be underreported. Otherwise, the use of fluoroquinolones may not necessarily be selected as therapeutic agents for infectious complications in usual clinical practice. Nevertheless, we believe the current report illustrates the pitfalls associated with managing patients with ADPKD who are subjected to the administration of fluoroquinolones due to infectious complications. Fluoroquinolone-associated tendinopathy should always be included in the list of causes of painful joint disorders in the lower extremities, although its involvement in other body regions has also been reported,3,5,9,10 thereby leading to an increased index of suspicion and prompt recognition of this pathology. Educating patients regarding the signs and/or manifestations of tendinopathy on commencing treatment with fluoroquinolones would allow us to recognize such disease states in a timely manner. Needless to say, careful weighing of the risks and benefits of fluoroquinolone use on a case-by-case basis is essential, and we may otherwise need to consider adopting other antibiotic agents. Furthermore, some subsets of patients may benefit from the concomitant use of antioxidant agents as well as avoiding sunlight and/or ultraviolet exposure.20 Alternatively, or in addition, we must bear in mind that no patients receiving this kind of agent are free from tendon toxicity, since a case of Achilles tendinitis in a man who exhibited no known predisposing factor has been shown anecdotally.5,21 Finally, evaluating the clinical benefits of using third-generation fluoroquinolones among patients with ADPKD complicated by cyst infections in detail may be useful, as the reduced risk for Achilles tendinopathy has been shown when using these agents instead of first- and second-generation fluoroquinolones.11
Consent
Written informed consent was obtained from the patient to publish this case report and any accompanying images. Clinicians at our university are not required to obtain institutional review board approval for case reports of a single patient.
Funding
This study was supported in part by a Grant-in-Aid for Research on Advanced Chronic Kidney Disease, Practical Research Project for Renal Diseases from the Japan Agency for Medical Research and Development (AMED) and by a grant from Private University Research Branding Project from the Ministry of Education, Science and Culture, Japan.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Suwabe T. Cyst infection in autosomal dominant polycystic kidney disease: our experience at Toranomon Hospital and future issues. Clin Exp Nephrol. 2020;24:748–761. doi:10.1007/s10157-020-01928-2
2. Sallée M, Rafat C, Zahar JR, et al. Cyst infections in patients with autosomal dominant polycystic kidney disease. Clin J Am Soc Nephrol. 2009;4:1183–1189. doi:10.2215/CJN.01870309
3. Khaliq Y, Zhanel GG. Fluoroquinolone-associated tendinopathy: a critical review of the literature. Clin Infect Dis. 2003;36:1404–1410. doi:10.1086/375078
4. Takeda S, Imai T, Chaki Y, Kusano E. Four consecutive cases of Achilles tendon disorders associated with levofloxacin treatment in hemodialysis patients. Clin Exp Nephrol. 2012;16:977–978. doi:10.1007/s10157-012-0716-1
5. Bidell MR, Lodise TP. Fluoroquinolone-associated tendinopathy: does levofloxacin pose the greatest risk? Pharmacotherapy. 2016;36:679–693. doi:10.1002/phar.1761
6. Lantinga MA, Geudens A, Gevers TJ, Drenth JP. Systematic review: the management of hepatic cyst infection. Aliment Pharmacol Ther. 2015;41:253–261. doi:10.1111/apt.13047
7. Shimano S, Tsuda M, Fuyuno S, Arimura Y, Nanishi F. Liver cyst infection after colon endoscopic mucosal resection in a patient with autosomal dominant polycystic kidney disease on maintenance hemodialysis. Intern Med. 2018;57:219–222. doi:10.2169/internalmedicine.8784-16
8. Bernts LHP, Wallenburg E, de Jonge HJM, et al. Ciprofloxacin penetration into infected hepatic cysts in autosomal dominant polycystic kidney disease: a case report. J Antimicrob Chemother. 2019;74:829–830. doi:10.1093/jac/dky456
9. Harrell RM. Fluoroquinolone-induced tendinopathy: what do we know? South Med J. 1999;92:622–625. doi:10.1097/00007611-199906000-00014
10. Gold L, Igra H. Levofloxacin-induced tendon rupture: a case report and review of the literature. J Am Board Fam Pract. 2003;16:458–460. doi:10.3122/jabfm.16.5.458
11. Chinen T, Sasabuchi Y, Matsui H, Yasunaga H. Association between third-generation fluoroquinolones and achilles tendon rupture: a self-controlled case series analysis. Ann Fam Med. 2021;19:212–216. doi:10.1370/afm.2673
12. Zhang Y, Reif G, Wallace DP. Extracellular matrix, integrins, and focal adhesion signaling in polycystic kidney disease. Cell Signal. 2020;72:109646. doi:10.1016/j.cellsig.2020.109646
13. Stephenson AL, Wu W, Cortes D, Rochon PA. Tendon Injury and Fluoroquinolone Use: a Systematic Review. Drug Saf. 2013;36:709–721. doi:10.1007/s40264-013-0089-8
14. Lewis T, Cook J. Fluoroquinolones and tendinopathy: a guide for athletes and sports clinicians and a systematic review of the literature. J Athl Train. 2014;49:422–427. doi:10.4085/1062-6050-49.2.09
15. Gillet P, Blum A, Hestin D, et al. Magnetic resonance imaging may be an asset to diagnose and classify fluoroquinolone-associated Achilles tendinitis. Fundam Clin Pharmacol. 1995;9:52–56. doi:10.1111/j.1472-8206.1995.tb00265.x
16. Kato A, Ishigaki S, Yasuda H. Levofloxacin-associated Achilles tendinitis in a patient with chronic kidney disease stage 5. Clin Exp Nephrol. 2011;15:318–319. doi:10.1007/s10157-011-0417-1
17. Jones N, Kjellstrand CM. Spontaneous tendon ruptures in patients on chronic dialysis. Am J Kidney Dis. 1996;28:861–866. doi:10.1016/S0272-6386(96)90386-8
18. Koh KH, Arimuthu DA. Association of incidence rate of spontaneous tendon rupture and renal bone disease in end-stage renal disease patients’ cohort. Semin Dial. 2023;36:462–467. doi:10.1111/sdi.13145
19. Gibson P, Watson ML. Cyst infection in polycystic kidney disease: a clinical challenge. Nephrol Dial Transplant. 1998;13:2455–2457. doi:10.1093/ndt/13.10.2455
20. Kaleagasioglu F, Olcay E. Fluoroquinolone-induced tendinopathy: etiology and preventive measures. Tohoku J Exp Med. 2012;226:251–258. doi:10.1620/tjem.226.251
21. Durey A, Baek YS, Park JS, et al. Levofloxacin-induced Achilles tendinitis in a young adult in the absence of predisposing conditions. Yonsei Med J. 2010;51:454–456. doi:10.3349/ymj.2010.51.3.454
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.