Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Fixation by Autogenous Cortical Plate Technique on Sites of Subtrochanteric Shortening Osteotomy Contributes to Early Bone Union in Total Hip Arthroplasty for Crowe Type IV Developmental Dysplasia of the Hip
Authors Liu Y, Zhang S, Li C, Ma M ![]() , Yang M
, Yang M ![]() , Guo R
, Guo R ![]() , Kong X, Chai W
, Kong X, Chai W
Received 18 July 2022
Accepted for publication 6 October 2022
Published 29 November 2022 Volume 2022:18 Pages 1059—1067
DOI https://doi.org/10.2147/TCRM.S381885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Yubo Liu,1,2,* Shuai Zhang,2,3,* Chao Li,2,4,* Mingyang Ma,2,3 Minzhi Yang,1,2 Renwen Guo,2,3 Xiangpeng Kong,2,4 Wei Chai2,4
1School of Medicine, Nankai University, Tianjin, 300071, People’s Republic of China; 2Senior Department of Orthopedics, the Fourth Medical Center of PLA General Hospital, Beijing, 100048, People’s Republic of China; 3Medical School of Chinese People’s Liberation Army, Beijing, 100853, People’s Republic of China; 4National Clinical Research Center for Orthopaedics, Sports Medicine & Rehabilitation, Beijing, 100853, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangpeng Kong; Wei Chai, Email [email protected]; [email protected]
Aim: Subtrochanteric shortening osteotomy (SSO) is often applied during total hip arthroplasty (THA) in high hip dislocations. The aim of the present paper was to evaluate the results of fixation by autogenous cortical plate technique on sites of SSO in THA for patients with Crowe type IV developmental dysplasia of the hip (DDH).
Methods: We conducted a historical prospective cohort study and reviewed 67 patients (82 THAs) with SSO performed between March 2016 and May 2020. Thirty-nine patients (48 hips) obtained stability by intramedullary pressure provided by the S-ROM modular prostheses and with or without prophylactic binding by stainless-steel wire after osteotomy and before stem implantation (group A). Twenty-eight patients (34 hips) were fixed with autogenous cortical plate technique and stainless-steel wire or cables (group B). Time of operations, complications, radiographic results and clinical scores were compared.
Results: One intraoperative fracture and a dislocation occurred, while component loosening, ectopic ossification and osteolysis were not observed. Group B had a higher union rate at the 4th month than group A (P = 0.015) while there were no significant differences of union rates at the 8th (P = 0.811) and the 12th month (P = 0.722) and of the average healing time (P = 0.181). No significant differences were found in hip function scores (HHS and WOMAC Osteoarthritis Index) between two groups.
Conclusion: Fixation with autogenous cortical plate from the cylinder of femoral bone contributes to early bone union of osteotomy ends in Crowe type IV DDH patients compared to those who do not apply the technique. Besides of application of autogenous cortical strut grafts, relevant measures are as well recommended to prevent nonunion after SSO.
Keywords: developmental dysplasia of the Hip, subtrochanteric shortening osteotomy, autogenous cortical plate technique, bone union, total Hip arthroplasty
Introduction
Developmental dysplasia of the hip (DDH) may result in pain in adjoining structures and functional disability due to failed mechanics.1 Patients with DDH end up with total hip arthroplasty (THA) when pain becomes unbearable or the abnormal gait impacts life seriously.
Crowe classified DDH from type I to type IV based on the degree of superior migration of the femoral head.2 With its severest form, quality of life is seriously affected by high-ride dislocation of the hip and apparent leg-length discrepancy (LLD), along with limping and pain.3 When THA is performed in these patients, the aims are not only to restore the center of rotation of the hip but correcting the length of the leg and normalizing gait. For these patients, the acetabular cup should be introduced to the true acetabulum and modular implants are recommended to accommodate the femur abnormality in order to achieve optimal biomechanics and to decrease the joint reaction force and increase the lever arm of the abductor musculature.4,5 However, restoration of the anatomical hip center in these patients will inevitably lead to limb lengthening, which will lead to potential complications, such as palsy of the sciatic and femoral nerves and injuries to arteries.6,7 As a result, to manage joint reduction of the femoral head to the true acetabulum and avoid neurovascular injuries, subtrochanteric shortening osteotomy (SSO) is often applied during THA.
A transverse osteotomy is relatively easy to perform and decreases the surgical time considerably.8 However, studies have indicated that the inherent instability of a transverse osteotomy has the potential to cause healing problems at the osteotomy site.8,9 Osteotomy nonunion is not uncommon compared with other complications, such as postoperative dislocation and neurovascular injury. Nonunion of osteotomy sites need to be paid attention to, not only because early union of the osteotomy sites indicates an ideal healing condition of the whole body postoperatively, but provides guidance for early exercise and rehabilitation.
It has been recommended in literatures that an extramedullary device, such as strut grafts, cerclage wires or plate and screws can be used after transverse osteotomy to facilitate healing.10–12 Previous studies have also shown that fixation with a cable attached to the osteotomized segment is faster and results in more rapid union time when compared to plate osteosynthesis at the osteotomy site.1 The possible underlying mechanism might be the delaying effect of periosteal damage that takes place during a plate application. Here, we integrate the applications of both autogenous grafts and plate fixation concept and acquire autogenous cortical plate technique. Good immediate fixation demonstrated during surgery, its effect on the healing of the fracture ends is unknown yet.
This study aimed to explore whether fixation by autogenous cortical plate technique at the osteotomy site attributes to bone healing. We hypothesize that the technique is beneficial to bone union compared to those who do not apply or accepted sole prophylactic cable fixation before inserting the prosthesis to prevent iatrogenic splitting of the proximal femur in THA with SSO in patients with Crowe type IV DDH.
Patients and Methods
Patients
Based in our institute, the study is a single center historical prospective cohort study. We reviewed and recruited a total of 67 patients (82 hips) with Crowe type IV DDH who underwent THA with SSO between March 2016 and May 2020. For group A, we reviewed 39 patients (48 hips) who only obtained stability by intramedullary pressure provided by the S-ROM modular prostheses and with or without prophylactic binding by stainless steel wire after osteotomy and before stem implantation. For group B, we have recruited 28 patients (34 hips) who were applied with autogenous cortical plate technique and supplemented with stainless-steel wire or cables since the beginning of 2019, at which time the surgeon mastered the technique through academic exchange and learning. The inclusion criteria for both groups required patients with (1) anteroposterior (AP) and lateral pelvic radiographs preoperatively, 4th, 8th and 12th month postoperatively; (2) no past surgical history of the operative hip; (3) complete clinical data, including Harris Hip Scores (HHS) preoperatively, and both HHS and Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index at the 4th, 8th and 12th month postoperatively. The enrollment flow-chart is shown in Figure 1.
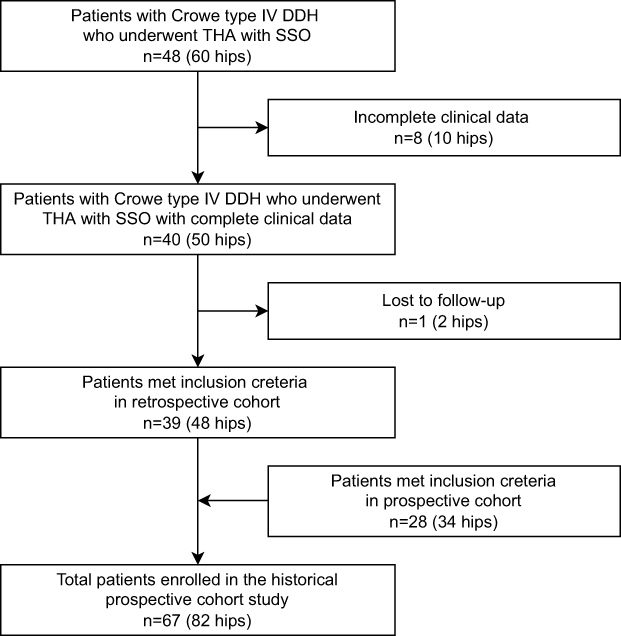 |
Figure 1 Enrollment flow-chart of patients. |
Surgical Technique
All operations were performed by one senior surgeon in our hospital with the patient in the lateral decubitus position. The preoperative surgical plans were prepared using OrthoView software (Version 6.6.1, Materialise, Leuven, Belgium). The planning system is simple and practicable, as many other similar applications have been widely reported.13,14 The process can be summarized as follows: (1) Scaling: Orientating the X-ray with the Image Manipulation Tools and establish the type of X-ray and calibrate the image. (2) Analyzing: Placing tools on images to make measurements and positioning templates on acetabulum and femur. (3) Templating: To get detailed information about size recommendations and change template options. So far, the preoperative prosthesis planning has been completed, while it does not actually guide the planning of SSO length.
All patients received general anesthesia, a posterolateral approach and similar technique of transverse subtrochanteric shortening osteotomy as previous studies described.12,15 Acetabular components were placed at the level of the true acetabulum and were inserted at 15°±10° of anteversion and 40°±10° of inclination. The osteotomy line is located 1.5 to 2.0 cm below the lesser trochanter to maintain the integrity of the trochanter area and to ensure adequate structural strength. The software templating results provided references and intraoperative measurement of lower-limb parameters presented solid evidence, collectively determining the actual reduction of length by SSO, which approximately equaled the distance between the true acetabular center and the femoral head center during the trial reduction. Before the cuts, a proximal vertical line was made parallel to the longitudinal axis of the femur and with the electric knife to serve as a rotational alignment marker. In the same way, a distal vertical line was made parallel to the longitudinal axis of the femur. Femoral anteversion was adjusted while applying fixation after osteotomy. In group A, stability was obtained only by intramedullary pressure provided by the S-ROM modular prostheses and with or without prophylactic binding by stainless steel wire after osteotomy and before stem implantation, which is to prevent iatrogenic splitting of the proximal and distal femur (Figure 2A). In group B, the autogenous bone segments resected from the proximal femur were split longitudinally, separated like an open book and covered at the osteotomy sites. One or two titanium control cables surrounded and pulled tight by a guider were applied to reinforce the structure for each femur (Figure 2B–E).
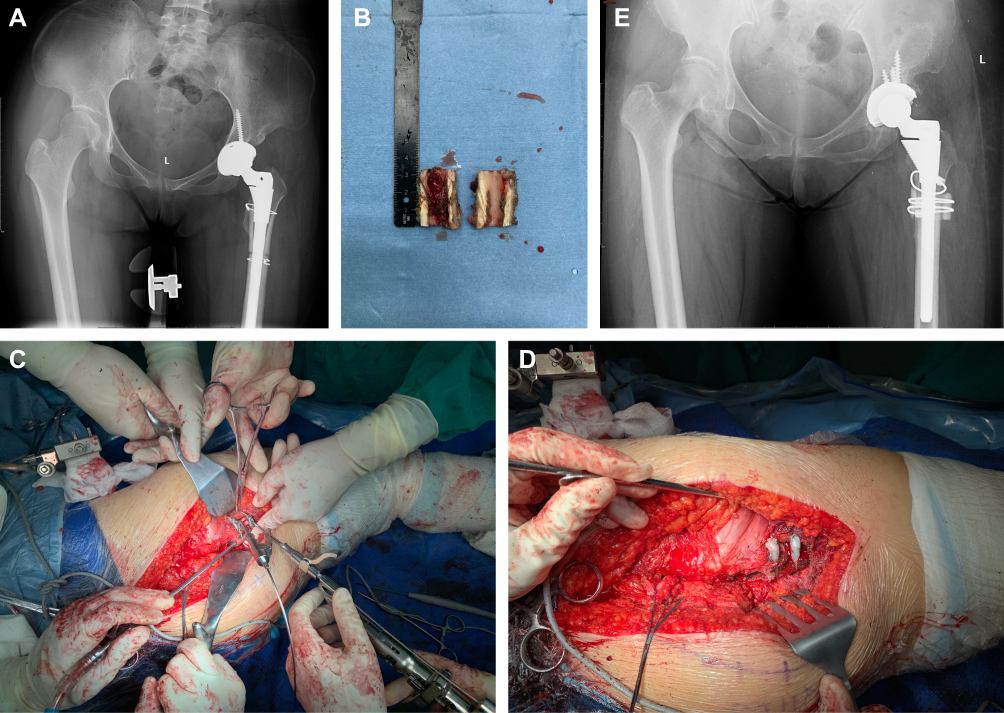 |
Figure 2 Two different methods of fixation of sites of SSO. (A) Stability obtained only by intramedullary pressure provided by S-ROM modular prostheses. 4th month follow-up shows nonunion of the osteotomy ends. (B) Autogenous bone segments resected from the femur and split longitudinally, which will then covered at the osteotomy sites. (C) Control cables were surrounded and pulled tight by a guider. (D) The structure of the femur was reinforced by application of the control cables. (E) Fixation with autogenous cortical strut grafts on sites of SSO. 4th month follow-up shows osteotomy site union. |
Pinnacle cementless acetabular components and modular S-ROM femoral stems (DePuy, Warsaw, IN, USA) were used in all hips. Binding of the autogenous cortical strut grafts and the prophylactic fixation before prothesis inserting are achieved by Cable-Ready cable grip system (Zimmer Biomet, Warsaw, IN, USA).
Clinical Evaluation
Clinical evaluations were performed preoperatively, postoperatively and at each clinical visit, which was routinely scheduled at the 4th, 8th and 12th month postoperatively. Clinical scores were derived using HHS system and WOMAC Osteoarthritis Index.
The intraoperative conditions, such as time of operations, were obtained from the patients’ medical records. Intraoperative and postoperative complications, defined as fractures, prosthesis loosening, dislocations, periprosthetic infections and ectopic ossifications were paid attention and recorded during operations and each follow-up. Follow-ups were performed by outpatient visits and phone interviews. The follow-up time at which fracture union was found was considered as the healing time.
Radiographic Measurements
A standard AP and lateral hip radiograph were obtained preoperatively, immediately after surgery, 4th, 8th and 12th month postoperatively. All radiographic measurements were analyzed twice, by 2 independent investigators who had not participated in the surgery and this research. If consensus is not reached, then ask for a senior investigator’s opinion.
Bone healing at the osteotomy site was determined using the criteria proposed by Masonis et al,16 which included (i) callous at the osteotomy site, (ii) restoration of cortical continuity between the proximal and distal fragments on the anteroposterior or lateral radiograph, and (iii) no progressive migration or gapping at the osteotomy site on serial radiographs.
Acetabular component position and loosening was defined with shift of component >2 mm in vertical, medial or lateral plane or radiolucent line of both A-P and lateral radiographs according to the method of Sutherland et al.17 Subsidence of the femoral component >3 mm was considered meaningful, and the femoral component was considered to have loosened if there was varus or valgus angle change of more than 2° or if there was complete radiolucent line around the femoral implant.18,19 The presence of ectopic ossification was determined by the method of Brooker et al.20
Statistical Analysis
The measurement data were normally distributed and expressed as mean ± standard deviation. Categorical data were described as rates and compared using a chi-squared test. One-way ANOVA was used for comparison of operation time and healing time between groups. Repeated measures ANOVA was used for inter-group comparison of HHS and WOMAC. If Mauchly’s test of sphericity was not met, Greenhouse-Geisser method was used for correction. Bonferroni method was used for inter-group comparison at different follow-up time, and multi-factor ANOVA was used for comparison of groups at the same follow-up time.
All tests were performed using SPSS 25.0 (IBM Corp, Armonk, NY. USA). A p-value <0.05 was considered significant in all the analyses.
Results
Demographic and Clinical Characteristics of Patients in Two Groups
There were 7 males and 75 females in total and 2 males and 46 females in group A and 5 males and 29 females in group B. The mean age of all patients was 38.1±11.7 years (range 21–66 years), and were 36.1±10.5 years (range 21–66 years) and 40.8±13.0 years (range 24–66 years) for 2 groups, respectively (t=−1.738, P = 0.087). The mean body mass index (BMI) was 22.2±3.1 kg/m2 (range, 16.4–29.3 kg/m2), and were 21.6±3.1 kg/m2 (range 16.4–29.3 kg/m2) and 23.0±2.9 kg/m2 (range 17.6–27.8 kg/m2), respectively (t=−2.081, P = 0.041). The mean follow-up time was 2.7±1.2 years (range 1.0–5.5 years) and 3.2±1.1 years (range 1.5–5.5 years) and 1.9±0.9 years (range 1.0–5.5 years).
Intraoperative and Early Postoperative Conditions
The mean time of operations was 139.7±40.3 minutes (range 80–332 minutes) and were 140.3±38.5 minutes (range 85–265 minutes) and 139.0±43.2 minutes (range 80–332 minutes), respectively (t = 0.145, P = 0.885). Intraoperative fracture of distal femur occurred in one hip in group A. No special treatment was given to her except delayed weight-bearing exercises. Dislocation occurred in one hip 2 months postoperatively due to a fall in group B, who underwent a reduction operation under general anesthesia. Neurological deficiency and acetabular and femoral component loosening were not observed in the early postoperative follow-up.
Radiographic Results
For group A, 24 out of 48 sites of subtrochanteric osteotomy achieved bone union at the 4-month follow-up, 43 out of 48 sites achieved bone union at the 8-month follow-up and 46 out of 48 achieved bone union at the 12-month follow-up. For group B, 26 out of 34 sites of subtrochanteric osteotomy achieved bone union at the 4-month follow-up, 31 out of 34 sites achieved bone union at the 8-month follow-up and 32 out of 34 sites achieved bone union at the 12-month follow-up.
At the 4-month follow-up, the bone healing rate was significantly higher in group B than group A (χ2=5.861, P = 0.015). But it was not significantly different between 2 groups at the 8-month (χ2=0.057, P = 0.811) and 12-month (χ2=0.126, P = 0.722) follow-up (Table 1).
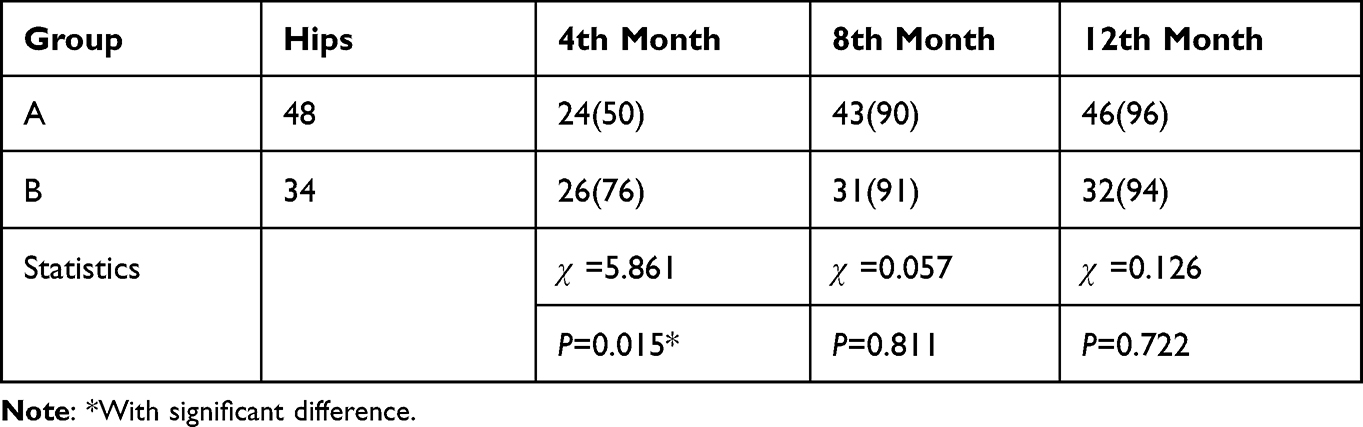 |
Table 1 Comparison of Osteotomy Healing Rates at Each Follow-Up (%) |
At each follow-up, acetabular and femoral component loosening were not observed according to radiograph data. Osteointegration of the stems in both groups was satisfactory. Ectopic ossification was not observed. No radiolucency, osteolysis, or migration was observed in association with acetabular and femoral components.
Clinical Outcomes
The mean healing time of the two groups was 6.4±2.9 months (range 4–15 months) and 5.5±3.1 months (range 4–15 months), respectively (t = 1.349, P = 0.181). The hip function scores of the two groups were significantly different at different follow-up time points (F = 234.687, P = 0.000 and F = 344.579, P = 0.000) respectively, indicating excellent therapeutic and functional improvement effects of both methods (Figure 3A and B). The main effect of hip function scores showed no significant differences in HHS (F = 1.518, P = 0.222) and WOMAC Osteoarthritis Index (F = 3.313, P = 0.072). And there were no significant differences in interaction effects (F = 0.652, P = 0.491 and F = 0.344, P = 0.614, respectively) that may cause potential false positives (Table 2). The result suggests that patients in 2 groups had the same good functions and subjective feelings at each follow-up postoperatively.
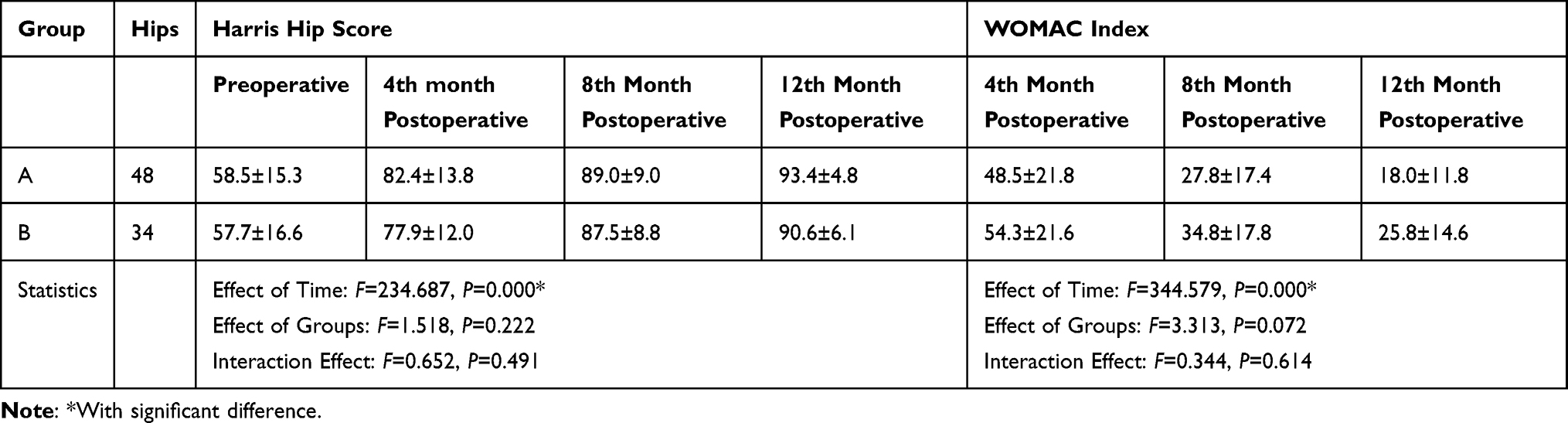 |
Table 2 Comparison of Hip Function Scores Between 2 Groups Among Follow-Ups |

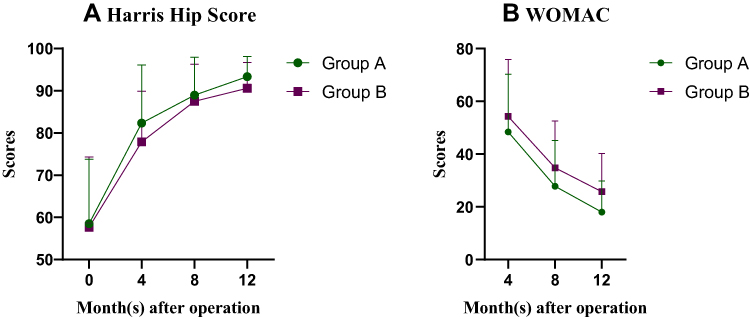 |
Figure 3 Trend of Hip function scores preoperative and at each follow-up. (A) Harris Hip Score. (B) WOMAC index. |
Except intraoperative fracture in one hip and one dislocation due to a fall 2 months postoperatively, complications such as neurological deficiency, prosthesis loosening and deep-seated infection were not observed during our follow-ups.
Discussion
In the setting of Crowe type IV DDH, femoral shortening osteotomy may be necessary to safely reduce the hip to the true acetabulum, mitigate hip soft-tissue contractions, and protect the neurovascular structures.21,22 According to literature reports, the nonunion rate of transverse osteotomy range from 1.3~20%.23 To avoid the potential possibility of reoperation, influence factors of delayed union and relevant surgical measures to promote healing should be taken into account. The factors that may cause delayed union of osteotomy ends are so far not clear. In our study, autogenous cortical plate technique, achieved by the form of strut graft, however, can provide extramedullary fixation in addition to intramedullary fixation acquired by S-ROM modular prothesis. By our surgical technique, it is considered to enhance the stability of the osteotomy site and to potentiate biologic healing when affixed around the osteotomy site.15,24,25 Although it showed no difference of healing rate and time between the two groups at the 8th, 12th months and the endpoints of the follow-ups, higher union rate of group B was shown at the first follow-up (4-month) postoperatively than group A. Yet, no significant difference in average union time and complication rate between the two groups were found.
According to literature reports, several reasons for the occurrence of nonunion are as follows. Firstly, Congruence of the interface and canal diameters between proximal and distal femoral segments may affect the union.25 Mismatched sizes of anastomosis interface and uneven surfaces of the osteotomy ends are likely to prolong healing time. Secondly, counterrotating between the proximal and distal femoral parts may lead to delayed healing at the osteotomy ends. Satisfactory torsional stability can be provided by S-ROM when the splines and flutes bite into the cortex.26,27 However, modulus mismatch or the incomplete matching of the round stem and the malformed femoral medullary elliptical cavity may reduce the resistance to torque and cause a delaying effect of healing. Thirdly, bone healing can be affected by underlying biological mechanisms. Stripping of circumferential periosteum during the preparation, and high local temperature of the saw for osteotomy may damage the osteoblastic activity of the periosteum, resulting in nonunion after the technique.23,25,28 What is more, embedding of soft tissue in the osteotomy sites and premature load or improper activity were also believed to affect bone union.23
As a result, the following suggestions can be carried out at the very least to prevent unexpected nonunion. First, ensure that the contact surface of the osteotomy ends close and the diameter of the medullary cavities match. Second, to select a large and sufficiently long distal femoral stem to prevent rotation. Third, during the operation, excessive stripping of periosteum at the osteotomy ends should be refrained to ensure the blood supply. Fourth, to reduce embedding of soft tissue during and after implantation. Fifth, to avoid postoperative premature loading and inappropriate exercises. Sixth, attention should also be paid to the decision of the height of the osteotomy site. If the osteotomy line is too high, which lies in the region that the femur becoming narrower, the matching area of the medullary cavity between the proximal and distal ends will be smaller, and the risk of instability will be increased. If the osteotomy line is too low and far from the epiphysis, the relatively poor blood supply and poor fixation due to weak compression of the distal end of the S-ROM modular prosthesis are not conducive to healing of osteotomy sites. Granger et al29 found that the cortical strut grafts add rigidity to the femur, potentially reducing the difference in structural rigidity between the native femur and the implant and, as a result, reduce the stresses transferred to the femur and the resulting pain. In the similar way, for patients underwent THA with SSO, cortical strut grafts help in balancing rigidity of the overall structure and virtually promote osteotomy sites healing.
There are also reports that stressed the effect of the cable of higher risk of osteolysis around the fixation and the femoral and acetabular components when used for reattachment following a transtrochanteric approach.30 Higher rate of nonunion of the greater trochanter has been also found and considered as a result of metal debris generation caused by fretting of the cables, which induces local inflammation and osteolysis.30–32 Higher infection rate with cables than with wires has also been observed by some authors.30,33,34 Kelley et al34 suggested that cable debris might facilitate bacterial seeding and thus lead to a higher infection rate; and this might be related to reduced phagocytosis in the presence of cobalt ions,35,36 as approximately 60% of the Dall Miles cable alloy (Vitallium, Stryker Howmedica) is made of cobalt.30 Nevertheless, in our study, control cables were made of titanium and placed around the bone grafts rather than the femur and components, which to some extent osteolysis and infection might be effectively avoided.
In conclusion, for patients with Crowe type IV DDH who require THA with SSO, application of autogenous cortical strut grafts recycled from osteotomized femoral segments together has a promoting effect on bone healing from the following aspects. i) The extramedullary fixation can provide additional stability, cooperated with the internal fixation provided by S-ROM prosthesis. ii) In case of modulus mismatch and uneven surfaces of anastomosis interface, covering of bone grafts can prevent embedding of soft tissue in the osteotomy sites. iii) The medial wall of grafts supports more contact around the femoral osteotomy site, which potentiate healing under some biological mechanism.
Our study has a number of limitations. First, this is a single-center historical prospective cohort study. In this way more attention was likely to be given to group B to avoid early weight bearing and improper activities, etc. Second, the sample size is relatively small. A larger number of patients of both groups should be included in our future study. Finally, the evaluation of osteotomy ends union needs more precise means. The method of visual judgment lacks objectivity. Therefore, the results of this study could not absolutely prove the superiority of application of autogenous cortical strut grafts from the cylinder of femoral bone on osteotomy sites. There is still a need for further multicenter and diversified clinical trials with more samples and clinical data.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author Wei Chai on reasonable request.
Ethics Statement
The study protocol has been approved by the Ethics Committee of First Medical Center of Chinese PLA General Hospital, and all the participating patients were fully informed and participated in the study voluntarily. We have obtained informed consents from all the study participants prior to study commencement. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The study was funded by: (1) National Key R&D Program of China (2021YFC2401303) (2) National Key R&D Program of China (2021YFC2401304) (3) Beijing Municipal Natural Science Foundation (M22016). (4) 2022 Major Scientific Problems And Medical Technology Problems Project of China Medicine Education Association (2022KTZ006).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Çatma M, Ünlü S, Öztürk A, Aksekili A, Ersan Ö, Ateş Y. Femoral shortening osteotomy in total Hip arthroplasty for severe dysplasia: a comparison of two fixation techniques. J Int Orthop. 2016;40:2271–2276. doi:10.1007/s00264-016-3144-0
2. Crowe JF, Ranawat CS. Total Hip replacement in congenital dislocation and dysplasia of the Hip. J Bone Joint Surg Am. 1979;61:15–23. doi:10.2106/00004623-197961010-00004
3. Kong X, Chai W, Chen J, Yan C, Shi L, Wang Y. Intraoperative monitoring of the femoral and sciatic nerves in total Hip arthroplasty with high-riding developmental dysplasia. Bone Joint J. 2019;101-B:1438–1446. doi:10.1302/0301-620X.101B11.BJJ-2019-0341.R2
4. Wang S, Zhou Y, Ma H, Du Y, Piao S, Wu W. Mid-term results of total hip replacement with subtrochanteric osteotomy, modular stem, and ceramic surface in Crowe iv Hip dysplasia. J Arthroplasty Today. 2018;4:363–369. doi:10.1016/j.artd.2017.07.003
5. Yoder S, Brand R, Pedersen D, O’Gorman T. Total Hip acetabular component position affects component loosening rates. J Clin Orthop Relat Res. 1988;228:79–87.
6. Rogers B, Garbedian S, Kuchinad R, Backstein D, Safir O, Gross A. Total hip arthroplasty for adult Hip dysplasia. J Bone Jt Surg. 2012;94:1809–1821. doi:10.2106/JBJS.K.00779
7. Shi X, Li C, Han Y, Song Y, Li S, Liu J. Total Hip arthroplasty for Crowe type iv Hip dysplasia: surgical techniques and postoperative complications. J Orthop Surg. 2019;11:966–973. doi:10.1111/os.12576
8. Muratli K, Karatosun V, Uzun B, Celik S. Subtrochanteric shortening in total Hip arthroplasty: biomechanical comparison of four techniques. J Arthroplasty. 2014;29:836–842. doi:10.1016/j.arth.2013.09.004
9. Reikeraas O, Lereim P, Gabor I, Gunderson R, Bjerkreim I. Femoral shortening in total arthroplasty for completely dislocated hips: 3–7 year results in 25 cases. J Acta orthopaedica Scandinavica. 1996;67:33–36. doi:10.3109/17453679608995605
10. Çağlar Ö, Özdemir E, Tokgözoğlu A, Atilla B. Use of proximal humerus plates for the fixation of the subtrochanteric femoral shortening osteotomy during total Hip arthroplasty for Crowe type iv developmental dysplasia of the Hip patients. J Joint Dis Relat Surg. 2020;31:306–311. doi:10.5606/ehc.2020.73078
11. Togrul E, Ozkan C, Kalaci A, Gülşen M. A new technique of subtrochanteric shortening in total Hip replacement for Crowe type 3 to 4 dysplasia of the Hip. J Arthroplasty. 2010;25:465–470. doi:10.1016/j.arth.2009.02.023
12. Yasgur D, Stuchin S, Adler E, DiCesare P. Subtrochanteric femoral shortening osteotomy in total hip arthroplasty for high-riding developmental dislocation of the Hip. J Arthroplasty. 1997;12:880–888. doi:10.1016/S0883-5403(97)90157-1
13. Chernchujit B, Tharakulphan S, Prasetia R, Chantarapanich N, Jirawison C, Sitthiseripratip K. Preoperative planning of medial opening wedge high tibial osteotomy using 3d computer-aided design weight-bearing simulated guidance: technique and preliminary result. J Orthop Surg. 2019;27:2309499019831455. doi:10.1177/2309499019831455
14. Pruksakorn D, Chantarapanich N, Arpornchayanon O, Leerapun T, Sitthiseripratip K, Vatanapatimakul N. Rapid-prototype endoprosthesis for palliative reconstruction of an upper extremity after resection of bone metastasis. Int J Comput Assist Radiol Surg. 2015;10:343–350. doi:10.1007/s11548-014-1072-2
15. Krych A, Howard J, Trousdale R, Cabanela M, Berry D. Total Hip arthroplasty with shortening subtrochanteric osteotomy in Crowe type-iv developmental dysplasia: surgical technique. J Bone Jt Surg. 2010;92:176–187. doi:10.2106/JBJS.J.00061
16. Masonis J, Patel J, Miu A, et al. Subtrochanteric shortening and derotational osteotomy in primary total Hip arthroplasty for patients with severe Hip dysplasia: 5-year follow-up. J Arthroplasty. 2003;18:68–73. doi:10.1054/arth.2003.50104
17. Sutherland C, Wilde A, Borden L, Marks K. A ten-year follow-up of one hundred consecutive müller curved-stem total Hip-replacement arthroplasties. J Bone Jt Surg. 1982;64:970–982. doi:10.2106/00004623-198264070-00002
18. Kim Y, Kim J, Oh S, Kim J. Comparison of porous-coated titanium femoral stems with and without hydroxyapatite coating. J Bone Jt Surg. 2003;85:1682–1688. doi:10.2106/00004623-200309000-00005
19. Lim S, Moon Y, Eun S, Park Y. Total Hip arthroplasty using the s-rom modular stem after joint-preserving procedures for osteonecrosis of the femoral head. J Arthroplasty. 2008;23:495–501. doi:10.1016/j.arth.2007.05.026
20. Brooker A, Bowerman J, Robinson R, Riley L. Ectopic ossification following total Hip replacement. Incidence and a method of classification. J Bone Jt Surg. 1973;55:1629–1632. doi:10.2106/00004623-197355080-00006
21. Du Y, Sun J, Ma H, Wang S, Ni M, Zhou Y. Leg length balance in total Hip arthroplasty for patients with unilateral Crowe type iv developmental dysplasia of the Hip. J Orthop Surg. 2020;12:749–755. doi:10.1111/os.12667
22. Greber E, Pelt C, Gililland J, Anderson M, Erickson J, Peters C. Challenges in total Hip arthroplasty in the setting of developmental dysplasia of the Hip. J Arthroplasty. 2017;32:S38–S44. doi:10.1016/j.arth.2017.02.024
23. Gong S, Xu W, Wang R, et al. The causes and management of nonunion of femoral subtrochanteric shortening osteotomy in a THA patient: a case report. J BMC Musculoskelet Disord. 2019;20:203. doi:10.1186/s12891-019-2612-2
24. Becker DA, Gustilo RB. Double-chevron subtrochanteric shortening derotational femoral osteotomy combined with total hip arthroplasty for the treatment of complete congenital dislocation of the hip in the adult. Preliminary report and description of a new surgical technique. J Arthroplasty. 1995;10:313–318. doi:10.1016/S0883-5403(05)80180-9
25. Wang D, Li L, Wang H, Pei F, Zhou Z. Long-term results of cementless total hip arthroplasty with subtrochanteric shortening osteotomy in Crowe type iv developmental dysplasia. J Arthroplasty. 2017;32:1211–1219. doi:10.1016/j.arth.2016.11.005
26. Ma H, Lu Q, Sun J, et al. One-stage total Hip arthroplasty with modular s-rom stem for patients with bilateral Crowe type iv developmental dysplasia. J Orthop Surg. 2020;12:1913–1922. doi:10.1111/os.12843
27. Ma H, Sun J, Du Y, et al. Model to predict need for subtrochanteric shortening osteotomy during total hip arthroplasty for Crowe type iv developmental dysplasia. J Med Sci Monit. 2020;26:e926239.
28. Wang D, Li D, Li Q, et al. Subtrochanteric shortening osteotomy during cementless total Hip arthroplasty in young patients with severe developmental dysplasia of the hip. J BMC Musculoskelet Disord. 2017;18:491. doi:10.1186/s12891-017-1857-x
29. Granger L, Bankes M, Sandiford N. Cortical strut graft for enigmatic thigh pain in uncemented total hip replacement. J Cureus. 2020;12:e8233.
30. Berton C, Puskas G, Christofilopoulos P, Stern R, Hoffmeyer P, Lübbeke A. Comparison of the outcome following the fixation of osteotomies or fractures associated with total hip replacement using cables or wires: the results at five years. J Bone Jt Surg. 2012;94:1475–1481. doi:10.1302/0301-620X.94B11.29687
31. Bauer T, Ming J, D’Antonio J, Morawa L Abrasive three-body wear of polyethylene caused by broken multifilament cables of a total hip prosthesis. A report of these cases. J Bj Surg. 1996;78:1244–1247.
32. Hop J, Callaghan J, Olejniczak J, Pedersen D, Brown T, Johnston R; The frank stinchfield award. Contribution of cable debris generation to accelerated polyethylene wear. J Clin Orthop Relat Res. 1997;20–32.
33. Altenburg A, Callaghan J, Yehyawi T, et al. Cemented total hip replacement cable debris and acetabular construct durability. J Bone Jt Surg. 2009;91:1664–1670. doi:10.2106/JBJS.G.00428
34. Kelley S, Johnston R. Debris from cobalt-chrome cable may cause acetabular loosening. J Clin Orthop Relat Res. 1992;285:140–146.
35. Daou S, El Chemaly A, Christofilopoulos P, Bernard L, Hoffmeyer P, Demaurex N. The potential role of cobalt ions released from metal prosthesis on the inhibition of hv1 proton channels and the decrease in staphylococcus epidermidis killing by human neutrophils. J Biomaterials. 2011;32:1769–1777. doi:10.1016/j.biomaterials.2010.11.016
36. Rae T. The action of cobalt, nickel and chromium on phagocytosis and bacterial killing by human polymorphonuclear leucocytes; its relevance to infection after total joint arthroplasty. J Biomaterials. 1983;4:175–180. doi:10.1016/0142-9612(83)90006-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.