Back to Journals » Clinical Interventions in Aging » Volume 12
Five-year durability of stand-alone interspinous process decompression for lumbar spinal stenosis
Authors Nunley PD ![]() , Patel VV, Orndorff DG, Lavelle WF, Block JE
, Patel VV, Orndorff DG, Lavelle WF, Block JE ![]() , Geisler FH
, Geisler FH
Received 8 June 2017
Accepted for publication 18 July 2017
Published 6 September 2017 Volume 2017:12 Pages 1409—1417
DOI https://doi.org/10.2147/CIA.S143503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Pierce D Nunley,1 Vikas V Patel,2 Douglas G Orndorff,3 William F Lavelle,4 Jon E Block,5 Fred H Geisler6
1Spine Institute of Louisiana, Shreveport, LA, 2The Spine Center, University of Colorado Hospital, Denver, CO, 3Spine Colorado, Mercy Regional Hospital, Durango, CO, 4Upstate Bone and Joint Center, East Syracuse, NY, 5Independent Consultant, San Francisco, CA, 6Independent Consultant, Chicago, IL, USA
Background: Lumbar spinal stenosis is the most common indication for spine surgery in older adults. Interspinous process decompression (IPD) using a stand-alone spacer that functions as an extension blocker offers a minimally invasive treatment option for intermittent neurogenic claudication associated with spinal stenosis.
Methods: This study evaluated the 5-year clinical outcomes for IPD (Superion®) from a randomized controlled US Food and Drug Administration (FDA) noninferiority trial. Outcomes included Zurich Claudication Questionnaire (ZCQ) symptom severity (ss), physical function (pf), and patient satisfaction (ps) subdomains, leg and back pain visual analog scale (VAS), and Oswestry Disability Index (ODI).
Results: At 5 years, 84% of patients (74 of 88) demonstrated clinical success on at least two of three ZCQ domains. Individual ZCQ domain success rates were 75% (66 of 88), 81% (71 of 88), and 90% (79 of 88) for ZCQss, ZCQpf, and ZCQps, respectively. Leg and back pain success rates were 80% (68 of 85) and 65% (55 of 85), respectively, and the success rate for ODI was 65% (57 of 88). Percentage improvements over baseline were 42%, 39%, 75%, 66%, and 58% for ZCQss, ZCQpf, leg and back pain VAS, and ODI, respectively (all P<0.001). Within-group effect sizes were classified as very large for four of five clinical outcomes (ie, >1.0; all P<0.0001). Seventy-five percent of IPD patients were free from reoperation, revision, or supplemental fixation at their index level at 5 years.
Conclusion: After 5 years of follow-up, IPD with a stand-alone spacer provides sustained clinical benefit.
Keywords: interspinous spacer, lumbar spinal stenosis, Superion, neurogenic claudication, decompression
Introduction
Within 10 years, it is estimated that 64 million older adults will be afflicted with lumbar spinal stenosis, making it the most common indication for spine surgery in individuals older than 65 years.1,2 This expanding population of patients requires a greater range of treatment options throughout the continuum of care, particularly in the elderly who may not be appropriate candidates for open surgical procedures with the associated risks of general anesthesia.3 Interspinous process decompression (IPD) is a minimally invasive procedure that can be performed under monitored anesthesia care in an ambulatory surgery center and has been shown to provide comparable clinical performance to decompressive laminectomy for management of symptoms of spinal stenosis.4,5
Neurogenic claudication is the cardinal clinical feature of lumbar spinal stenosis, as it limits patients’ walking ability and causes a major impact on their quality of life.6 Intermittent neurogenic claudication is defined as unilateral or bilateral radicular pain during walking or standing that is relieved by sitting down or flexing the lumbar spine.7 Stenotic arthritic degeneration of the lumbar spine causes bony and ligamentous compression of neural structures axially and laterally. Indeed, constriction and impingement of nerves traversing the lateral recess and exiting the foraminal aperture are highly contributory to the most pronounced and aggravating radicular symptoms of stenosis.8
IPD employs a stand-alone spacer that functions as an extension blocker to minimize the extent of compression of neural elements, particularly in the lateral recess and foramina.9 Importantly, insertion of the spacer is performed percutaneously without surgical removal of tissue adjacent to the dura or exiting nerves. There is only one Food and Drug Administration (FDA)-approved stand-alone spacer commercially available in the USA. Herein, we provide the 5-year clinical outcomes for patients with moderate lumbar spinal stenosis treated with this IPD device.
Materials and methods
Clinical outcomes at the 5-year follow-up interval were obtained from the Superion® (VertiFlex, Inc., Carlsbad, CA, USA) treatment arm of a randomized controlled FDA noninferiority trial comparing two interspinous spacers. Methodological details of the study have been published previously.10,11 This multicenter trial evaluated the use of stand-alone IPD in the treatment of subjects aged 45 or older with moderate symptoms of intermittent neurogenic claudication, secondary to a diagnosis of moderate degenerative lumbar spinal stenosis at one or two contiguous levels from L1 to L5. Three hundred ninety-one subjects met the trial eligibility criteria and were randomized to treatment. The comparative effectiveness of these two spacers and the FDA-approved indications for use for IPD have been reported previously.12 The current 5-year analysis was restricted exclusively to the Superion arm of the trial.
This trial complied with all US regulatory requirements and was approved by the Institutional Review Board at each participating site (Table S1), and patients provided written informed consent before any study-related procedures were performed. The trial was prospectively registered at ClinicalTrials.gov (NCT00692276).
At the 5-year follow-up interval, 127 patients were free from reoperation (n=48) and/or epidural steroid injection (n=33), and there were 6 deaths, leaving 121 (64%) spacer patients actively participating in the post-market period of this study. Eighty-eight of 121 active spacer patients (73%) provided complete 5-year clinical outcome assessments by the Zurich Claudication Questionnaire (ZCQ), leg and back pain severity by visual analog scale (VAS), and the Oswestry Disability Index (ODI).
Clinical outcome data were analyzed in several ways. Success rates were calculated based on a priori definitions of the minimal clinically important difference: ≥0.5-point change for ZCQ symptom severity (ss) and physical function (pf), ≤2.5 points for ZCQ patient satisfaction (ps), ≥20 mm for pain VAS, and ≥15% points for ODI. Additionally, we computed the percentage improvement in each outcome measure at 5 years compared to preoperative values and displayed these results graphically.
The within-group effect sizes at the 5-year postoperative interval were computed and compared to baseline for each clinical outcome separately using Cohen’s formula and thresholds.13,14 Effect sizes were reported in the range from 0.0 (no effect) to >1.0 (very large effects) with the following thresholds: 0.2 (small effect), 0.5 (medium effect), 0.8 (large effect), and >1.0 (very large effect).
Results
Five years after the index procedure, 74 of 88 patients (84%) demonstrated clinical success on at least two of three ZCQ domains. The success rates for the individual ZCQ domains were 75% (66 of 88), 81% (71 of 88), and 90% (79 of 88) for ZCQss, ZCQpf, and ZCQps, respectively. For leg and back pain VAS, the success rates were 80% (68 of 85) and 65% (55 of 85), respectively, and the rate was 65% (57 of 88) for ODI.
There was substantial improvement at each annual follow-up interval compared to baseline for the ZCQ (Figure 1), leg and back pain VAS (Figure 2), and ODI (Figure 3). Spacer patients demonstrated percentage improvements over baseline of 42%, 39%, 75%, 66%, and 58% for ZCQss, ZCQpf, leg and back pain VAS, and ODI, respectively (all P<0.001), as shown in Figure 4. Within-group effect sizes were classified as very large for four of five clinical outcomes (ie, >1.0): 1.35, 1.40, 1.32, 0.97, and 1.37 for ZCQss, ZCQpf, leg and back pain VAS, and ODI, respectively (all P<0.0001), as shown in Figure 5.
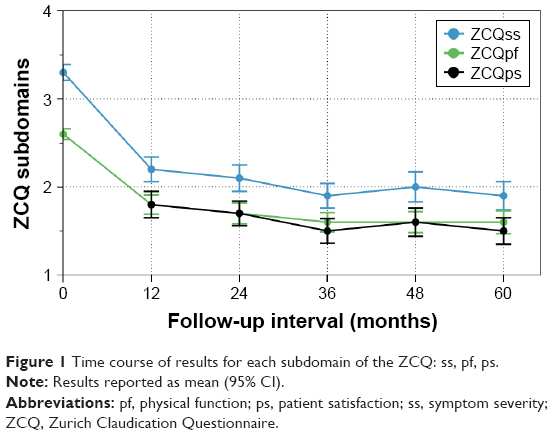 | Figure 1 Time course of results for each subdomain of the ZCQ: ss, pf, ps. |
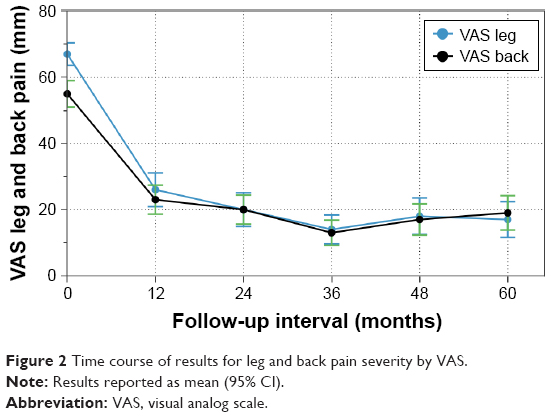 | Figure 2 Time course of results for leg and back pain severity by VAS. |
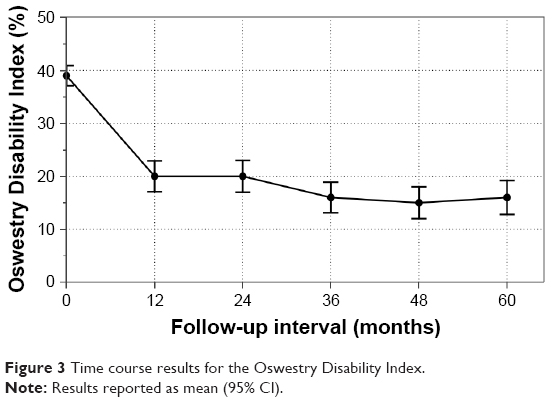 | Figure 3 Time course results for the Oswestry Disability Index. |
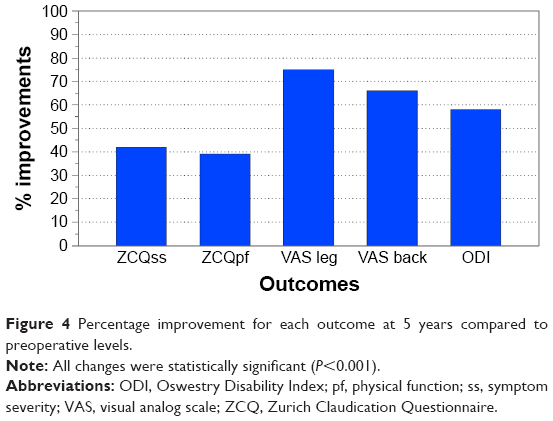 | Figure 4 Percentage improvement for each outcome at 5 years compared to preoperative levels. |
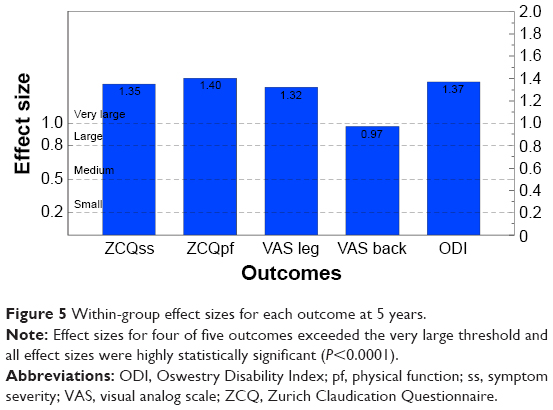 | Figure 5 Within-group effect sizes for each outcome at 5 years. |
Of the 190 patients randomized to receive treatment, 142 (75%) were free from reoperation, revision, or supplemental fixation at their index level at 5 years. Notably, there was a discernible trend toward decreasing risk of reoperation over time with the majority of revisions occurring during the initial 2 years of observation with annual percentage increments as follows: 27 (14.2%), 11 (5.8%), 3 (1.6%), 6 (3.2%), and 1 (0.5%) during years 1, 2, 3, 4, and 5, respectively.
Discussion
It has been estimated that ~40% of patients with lumbar spinal stenosis become refractory to conservative care and will ultimately require decompression surgery within 10 years to manage persistently worsening symptoms.15 Moreover, while laminectomy effectively decompresses the offended neural elements providing symptom relief, it can destabilize the spine, eventually leading to re-emergence of symptoms requiring reoperation with instrumented fusion. A recent randomized controlled trial reported that one-third of laminectomy patients required reoperation with fusion within 4 years.16 This rate of reoperation rate after laminectomy is comparable to a 28% rate reported from a large Washington state administrative database.17 Treatment of recalcitrant symptoms of neurogenic claudication with an interspinous spacer may significantly delay or obviate completely the need for decompressive laminectomy as well as the downstream risk of revision surgery with instrumented fusion.
This is the first report to document the long-term clinical durability of stand-alone interspinous spacer decompression for lumbar spinal stenosis through 5 years of monitored follow-up. For the 75% of spacer patients who have remained free of reoperation with an intact implant, the clinical results continue to be impressive, with almost 85% of patients achieving success on at least two of three ZCQ domains. Leg pain symptom amelioration remains most notable with an average improvement of 75% at 5 years over preoperative values. This suggests that the spacer continues to offer sufficient indirect decompression of neural structures in the lateral recesses and foramina to suppress claudicant and radicular symptoms.
Thirty-eight of 48 (79%) spacer patients underwent reoperation within the initial 2 years of postoperative observation. Of the remaining 10 reoperations, only 1 occurred during the fifth year of observation, suggesting a decreasing risk of revision surgery with time. This implies that patients who demonstrate early clinical improvement with spacer implantation will maintain that benefit over time. Clinical failures after spacer treatment can be identified early in the postoperative time course and these patients can be offered other surgical options. In contrast, reoperation rates after laminectomy tend to increase with time.16 Consequently, early clinical success may not be sustained in the long term, as outcomes eventually deteriorate due to the untoward effects of laminectomy-induced spinal instability, necessitating a complex instrumented fusion procedure to provide stabilization.
Because the IPD implantation procedure is performed in a minimally invasive fashion and causes only minor anatomic disruption, the full range of surgical options remains available if a revision becomes necessary to manage re-emergence of symptoms. Thus, with simplicity of the operative procedure, rapid patient recovery, low surgical risk of complications, and long-term clinical durability, IPD remains a viable treatment option for stenosis patients.
Conclusion
After 5 years of postoperative follow-up, IPD with a stand-alone spacer provides sustained clinical benefit. Its use is indicated for patients with intermittent neurogenic claudication associated with moderate lumbar spinal stenosis.
Acknowledgments
The authors wish to thank Greg Maislin for data management support and for conducting all statistical analyses. Graphical support was provided by Terry Meredith. Financial support for this work was provided by VertiFlex, Inc. (Carlsbad, CA, USA).
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
JB is an independent advisor to VertiFlex. The authors report no other conflicts of interest in this work.
References
Deyo RA. Treatment of lumbar spinal stenosis: a balancing act. Spine J. 2010;10(7):625–627. | ||
Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010;303(13):1259–1265. | ||
Li G, Warner M, Lang BH, Huang L, Sun LS. Epidemiology of anesthesia-related mortality in the United States, 1999–2005. Anesthesiology. 2009;110(4):759–765. | ||
Lauryssen C, Jackson RJ, Baron JM, et al. Stand-alone interspinous spacer versus decompressive laminectomy for treatment of lumbar spinal stenosis. Expert Rev Med Devices. 2015;12(6):763–769. | ||
Nunley PD, Shamie AN, Blumenthal SL, Orndorff D, Block JE, Geisler FH. Interspinous process decompression: expanding treatment options for lumbar spinal stenosis. Biomed Res Int. 2016;2016:3267307. | ||
Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol. 2010;24(2):253–265. | ||
Katz JN, Harris MB. Clinical practice. Lumbar spinal stenosis. N Engl J Med. 2008;358(8):818–825. | ||
Jenis LG, An HS. Spine update. Lumbar foraminal stenosis. Spine (Phila Pa 1976). 2000;25(3):389–394. | ||
Loguidice V, Bini W, Shabat S, Miller LE, Block JE. Rationale, design and clinical performance of the superion® Interspinous Spacer: a minimally invasive implant for treatment of lumbar spinal stenosis. Expert Rev Med Devices. 2011;8(4):419–426. | ||
Patel VV, Whang PG, Haley TR, et al. Superion interspinous process spacer for intermittent neurogenic claudication secondary to moderate lumbar spinal stenosis: two-year results from a randomized controlled FDA-IDE pivotal trial. Spine (Phila Pa 1976). 2015;40(5):275–282. | ||
Patel VV, Whang PG, Haley TR, et al. Two-year clinical outcomes of a multicenter randomized controlled trial comparing two interspinous spacers for treatment of moderate lumbar spinal stenosis. BMC Musculoskelet Disord. 2014;15:221. | ||
Patel VV, Nunley PD, Whang PG, et al. Superion(®) InterSpinous Spacer for treatment of moderate degenerative lumbar spinal stenosis: durable three-year results of a randomized controlled trial. J Pain Res. 2015;8:657–662. | ||
Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting changes in health status. Med Care. 1989;27(3 Suppl):S178–S189. | ||
Sullivan GM, Feinn R. Using effect size-or why the P value is not enough. J Grad Med Educ. 2012;4(3):279–282. | ||
Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine (Phila Pa 1976). 2005;30(8):936–943. | ||
Ghogawala Z, Dziura J, Butler WE, et al. Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. N Engl J Med. 2016;374(15):1424–1434. | ||
Martin BI, Mirza SK, Comstock BA, Gray DT, Kreuter W, Deyo RA. Reoperation rates following lumbar spine surgery and the influence of spinal fusion procedures. Spine (Phila Pa 1976). 2007;32(3):382–387. |
Supplementary material
 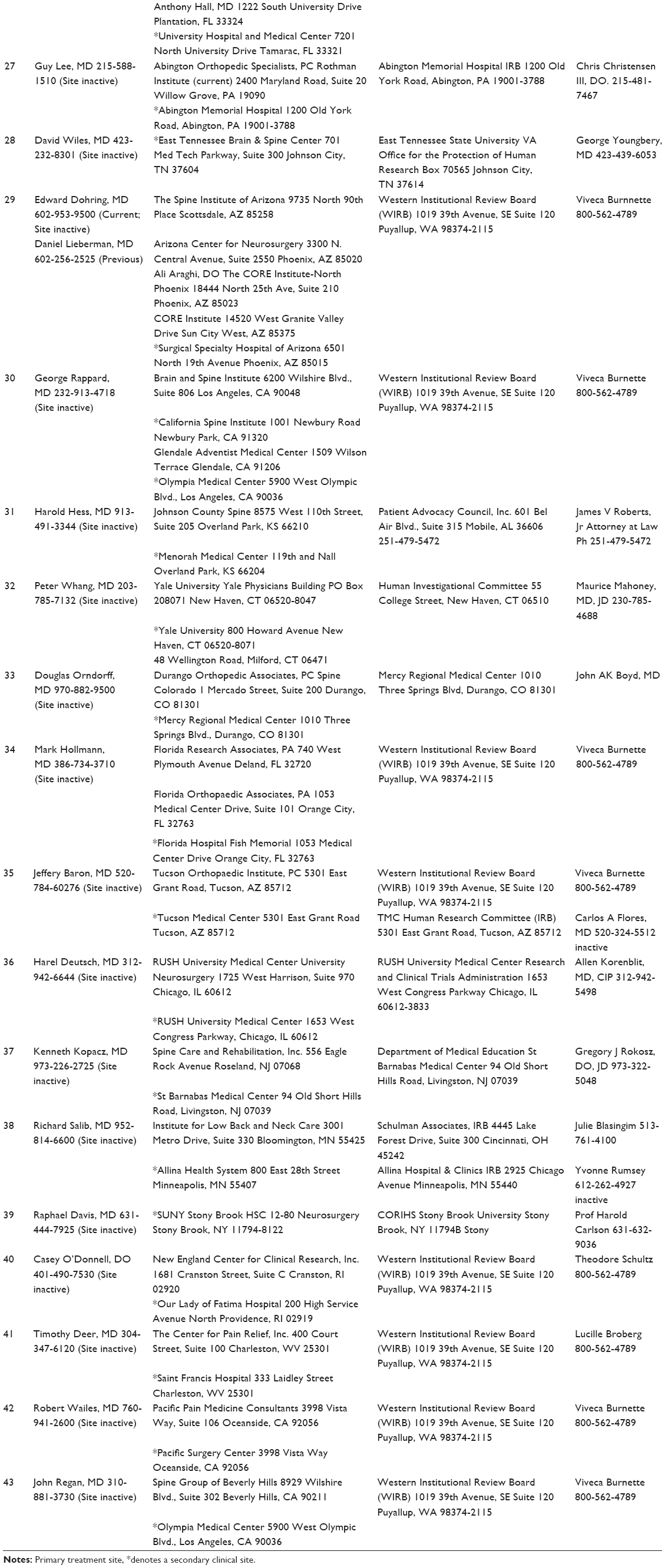 | Table S1 Site list of institutional review board (IRB) information |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.