Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Financial Burden and Catastrophic Health Expenditure Associated with COVID-19 Hospitalizations in Kerala, South India
Authors Thomas R ![]() , Jacob QM, Raj Eliza S, Mini M, Jose J, A S
, Jacob QM, Raj Eliza S, Mini M, Jose J, A S
Received 15 March 2022
Accepted for publication 23 June 2022
Published 4 July 2022 Volume 2022:14 Pages 439—446
DOI https://doi.org/10.2147/CEOR.S365999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Ronnie Thomas,1 Quincy Mariam Jacob,1 Sharon Raj Eliza,2 Malathi Mini,1 Jobinse Jose,3 Sobha A1
1Department of Community Medicine, Government Medical College Kottayam, Kottayam, Kerala, India; 2Department of Community Medicine, Pushpagiri Institute of Medical Sciences and Research Centre, Thiruvalla, Kerala, India; 3Department of Community Medicine, Kasturba Medical College, Mangalore, India
Correspondence: Ronnie Thomas, Department of Community Medicine, Government Medical College Kottayam, Kottayam, Kerala, India, Tel +91 9947014747, Email [email protected]
Introduction: Catastrophic health expenditure during COVID-19 hospitalization has altered the economic picture of households, especially in low resource settings with high rates of COVID-19 infection. This study aimed to estimate the out of pocket (OOP) expenditure and the proportion of households that incurred catastrophic health expenditure due to COVID-19 hospitalization in Kerala, South India.
Materials and Methods: A cross-sectional study was conducted among a representative sample of 155 COVID-19 hospitalized patients in Kottayam district over four months, using a pretested interview schedule. The direct medical and non-medical costs incurred by the study participants during hospitalization and the total monthly household expenditure were obtained from the respective COVID-19 affected households. Catastrophic health expenditure was defined as direct medical expenditure exceeding 40% of the household’s capacity to pay.
Results: From the study, median and mean OOP expenditure was obtained as USD 93.57 and USD 502.60 respectively. The study revealed that 49.7% of households had catastrophic health expenditure, with 32.9% having incurred distress financing. Multivariate analysis revealed being below poverty line, hospitalization in private healthcare facility, and presence of co-morbid conditions as significant determinants of catastrophic health expenditure.
Conclusion: High levels of catastrophic health expenditure and distress financing revealed by the study have unveiled major unaddressed challenges in the road to universal health coverage.
Keywords: COVID-19, financial burden, catastrophic health expenditure, distress financing, Kerala
Introduction
The second wave of COVID-19 in India was a humanitarian and public health crisis which has overwhelmed the country’s healthcare system.1 The newly emerged Delta B.1.617 variant with increased transmissibility and pathogenicity was behind the devastating turn the pandemic took in April 2021 in India.2,3 As of October 1, India had reported more than 3.37 million confirmed COVID-19 cases and 448,605 deaths.4 COVID-19 continues to spread across the southern state of Kerala with significant health consequences and mortality.5,6 In addition to the direct effects of COVID-19, the economic and social disruption associated with the pandemic has had a substantial impact on the livelihood of the population and has exposed the healthcare disparities existing in socially disadvantaged communities.7,8 COVID-19 patients from such communities disproportionately experienced financial burden due to hospitalizations.7 The immediate apparent reason for this healthcare disparity is the underlying economic inequality.
Inadequate financial risk protection leads to high out-of-pocket (OOP) expenditure on healthcare. The OOP expenditure contribution reaches almost three-quarters of total expenditure on health in India and some South Asian countries with similar per capita income.9 The Twelfth Five Year Plan of India had reduction of OOP expenditure as one of the measurable targets.10 NITI Aayog’s report on the need for health insurance coverage states that the increased reliance on the private healthcare sector, makes the population vulnerable to increasing out of pocket payments.11 Evidence on OOP expenditure is important to protect vulnerable, poor households from catastrophic health expenditures (CHE) by providing appropriate financial risk protection. Health spending is considered to be catastrophic when a household must reduce its basic expenditure over a period of time to cope with health costs.12 Catastrophic healthcare spending is considered as an indicator of financial protection under Universal Health Coverage for the Sustainable Development Goals.13,14 In Africa and Asia the number of people incurring catastrophic payments increased in the last decade.14 As pointed out by Xu et al, policy makers need a better understanding of any socioeconomic, cultural or demographic characteristics that make people more vulnerable to catastrophic payments.12 Furthermore, the economic weakening of a household as a result of health care expenses can lead to distress financing manifesting as borrowing money, mortgaging gold, and selling of assets. Indicators like CHE do not consider the economic impact of health conditions like COVID-19 beyond the health sector.15 As suggested by Wagstaff et al, health care-seeking has an opportunity cost beyond the direct medical costs in the form of productivity losses.14 This is especially important in the context of COVID-19 pandemic as the income loss can either be due to temporary reasons such as quarantine or job absenteeism and permanent causes like mortality or disability.
To the best of our knowledge, no study from India has systematically examined the financial burden of COVID-19 patients who required in-patient care. Evidence on the scale of hospitalization expenditures would enable decision-makers to optimize the allocation of scarce healthcare resources. With this background we conducted a cross-sectional study to primarily estimate the OOP expenditure and the proportion of catastrophic health expenditures (CHE) among hospitalized patients with COVID-19. Secondly we assessed the proportion of households facing impoverishment or distress financing due to catastrophic payments.
Materials and Methods
Study Sample
Kerala, a southern state of India, has the highest Human Development Index (inequality adjusted HDI of 0.520), in the country with a per capita income of INR 149,563.16,17 The study population included patients of all age groups and genders diagnosed with COVID-19 who required in-patient care in Kottayam district of Kerala from May to August 2021. The sampling frame was a line-list of patients containing the data on hospital admissions in the district for the same period. The inclusion criteria were: patients of any age and gender with or without co-morbid conditions, diagnosed with COVID-19 using either RT-PCR or rapid antigen test and admitted to any private hospitals, COVID second line treatment centers (CSLTC) or designated government COVID hospitals in Kottayam district. The authors performed systematic random sampling for selecting study participants from the line-list. The line-list also included patients who had expired at the time of data collection for whom details were collected from the next of kin. The investigators collected the data using a pre-tested structured interview schedule. Verbal informed consent was obtained from all study participants. Verbal informed consent was acceptable and approved by the Institutional Review Board, Government Medical College Kottayam. Pregnant patients were excluded and in cases of multiple hospital admissions for a single patient, the last hospital of admission was considered for study. The minimum sample size required was calculated to be 149.18 This study complies with the Declaration of Helsinki and was approved by the Institutional Review Board, Government Medical College Kottayam.
Estimation of Costs
As participants in household surveys are generally reluctant to reveal their total income, we used monthly household final consumption expenditure as the proxy for monthly effective income and the food expenditure as a proxy for household subsistence expenditure as explained by Xu et al.19 Expenditure data were collected as reported by the participants and the hospitalization expenditures of participants who were admitted in private hospitals were verified by the copies of available hospital bills sent electronically through Whatsapp or email. The investigators calculated the direct medical costs per COVID-19 patient as the sum of the inpatient cost in each category namely room/ICU rent, physician consultations, nursing services, drugs, medical consumables, imaging, electrocardiography, laboratory services, invasive and non-invasive ventilation, blood products transfusion and other procedures or interventions like hemodialysis. The direct non-medical costs for each COVID-19 patient was calculated as the sum of expenses incurred for food, travel, and accommodation for the patients and the bystanders. OOP expenditure was taken as the sum of direct medical and direct non-medical expenses paid by the house-hold at the time of hospitalization for COVID-19 after deducting for the aid received for financial risk protection. For defining catastrophic health expenditure we used the threshold and approach reported by Xu et al.12 This approach uses the household’s capacity to pay which is a measure of the non-subsistence income of the household calculated as effective income minus subsistence income. As per the definition we used, a household is said to incur catastrophic health expenditures when out-of-pocket spending on COVID-19 hospitalization exceeds 40% of the household’s capacity to pay.12 Distress financing was said to occur when the household is forced to borrow money or to take a personal loan or sell/mortgage land, gold or other assets to meet healthcare expenditure during hospitalization for COVID-19.20 The lost productivity was quantified only for the earning members of the household. In addition to income loss due to death, disability, and job absenteeism, we included income loss due to isolation, quarantine or patient care for any earning member of the household for quantifying the indirect costs.21 The friction period for estimating loss of income from permanent loss of productivity was fixed at 3 months.
Data Analysis
The outcome measures were the median OOP expenditure, proportion of households incurring catastrophic health expenditure, proportion of households experiencing distress financing, and the proportion of households facing temporary and permanent productivity losses. The households were divided into income tertiles based on the effective income. We used the Mann Whitney U-test and the Kruskal–Wallis test for nonparametric analyses of OOP expenditures. To evaluate the correlates of catastrophic health spending we created a binary logistic regression model. Variables were introduced into the regression model if they were found to be associated with CHE at p < 0.20. All statistical analyses were conducted using the statistical software SPSS version 20.0 (IBM Corp, Armonk, NY). We used a conversion rate of USD 1 = 74.9 INR.
Results
The authors interviewed 179 patients or next of kin, of whom 155 fulfilled the inclusion criteria. The mean age of the study participants was 55.45 ±19.93 years with a female predominance (55.5%). The average household size was 4.21±1.57 persons. Among the study participants, 38.7% belonged to households with per capita income below the international poverty line and 12.3% were unemployed. The mean duration of hospitalization was 11.35±10.75 days.
The present study found that the median (IQR) total OOP expenditure among the study participants was INR 7010 (1500–38,150), USD 93.57. The median (IQR) OOP expenditure for inpatient treatment of COVID-19 in public and private hospitals were INR 2980 (825–8850), USD 39.78 and INR 38,100 (10,237.5–63,625), USD 508.67, respectively.
Our analysis revealed that a total of 49.7% (95% CI 41.9, 58.1) of households incurred catastrophic health expenditure due to COVID 19 hospitalization. For the patients who underwent treatment in public sector institutions, 37.6% of households experienced catastrophic health expenditures. Whereas, for private sector hospitalizations the health expenditure was catastrophic for 64.3% households. As shown in Table 1, the median OOP expenditure was found to be significantly higher in patients with advancing age, comorbidities, severe disease and bad clinical outcomes. Significant variation of OOP expenditure was observed across the different income tertiles for COVID hospitalizations.
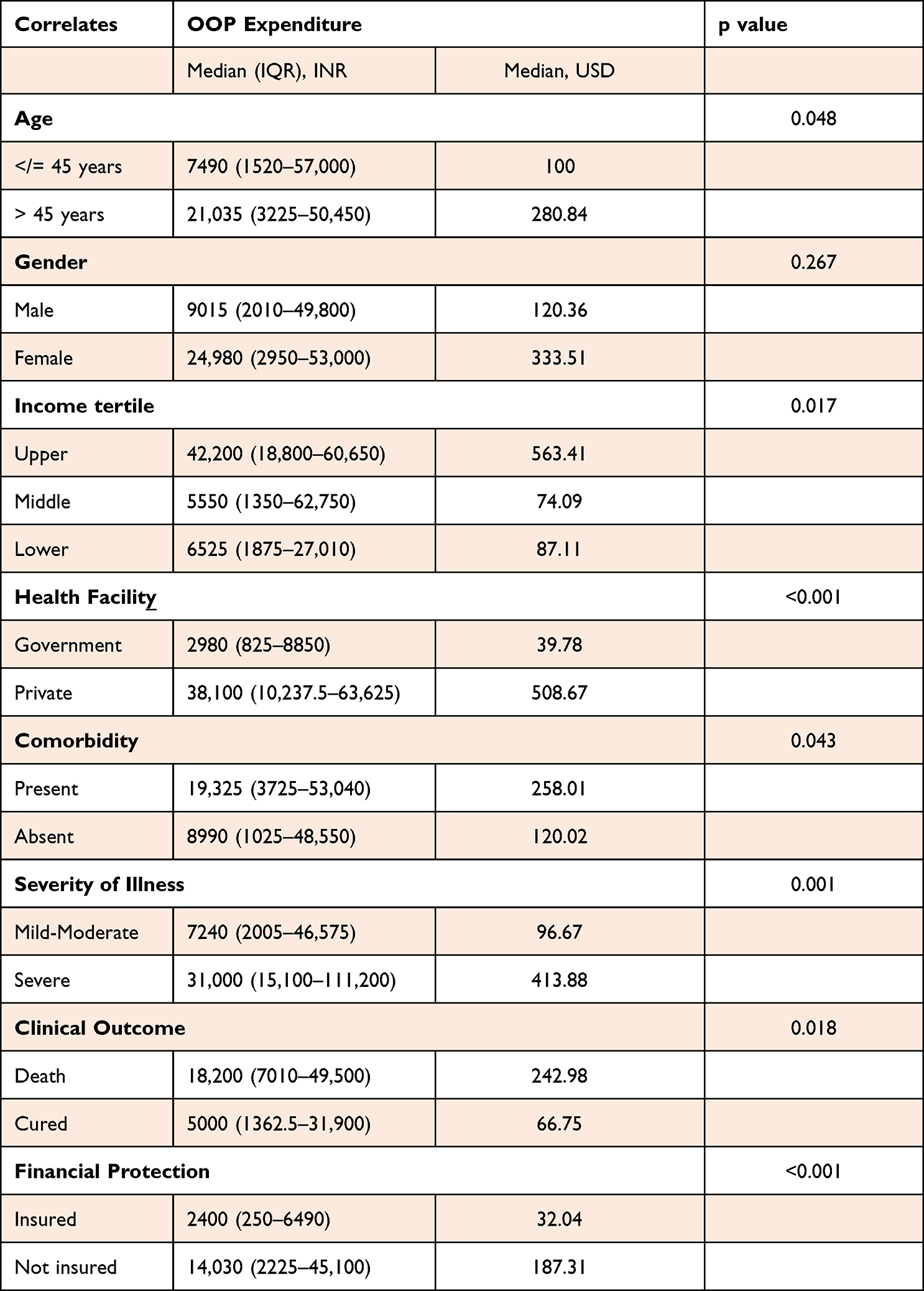 |
Table 1 The Median (IQR) Out of Pocket (OOP) Expenditures Grouped According to Correlates |
The median out-of-pocket costs for COVID-19 admissions were similar regardless of gender, educational status and occupational categories. In approximately one third of the hospitalizations (32.9%), patient costs were covered through borrowing, gold loans or sale of assets. Only 27 (17.4%) participants reported utilizing health insurance plans. The significant findings with regard to the odds of catastrophic health expenditure associated with COVID-19 hospitalizations are summarized in Table 2.
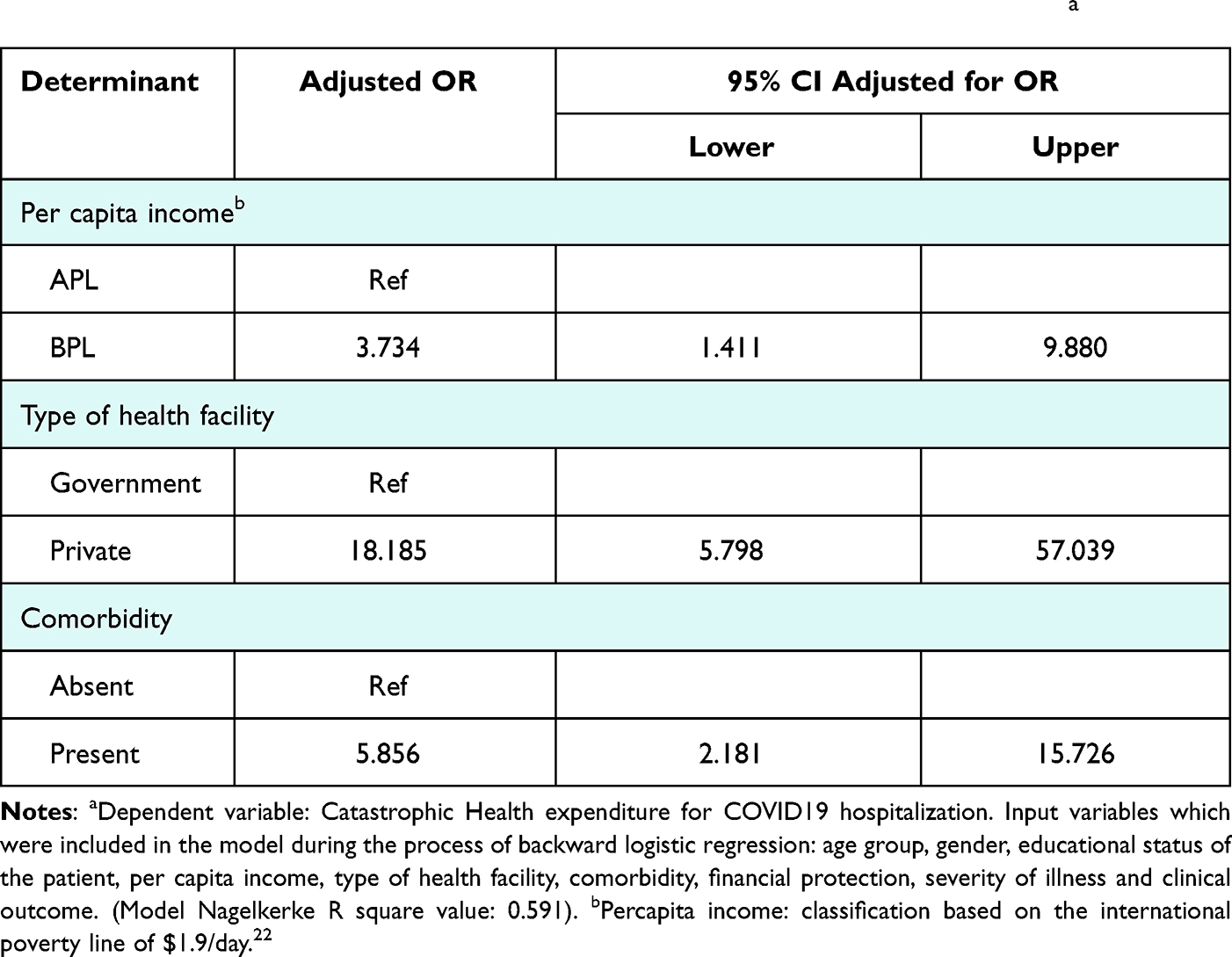 |
Table 2 Binary Logistic Regression Results of Significant Determinants of CHEa |
A total of 98 (63.2%) households reported productivity loss, of which the majority (48.4%) reported temporary income loss. 14.8% of the households reported permanent income loss for at least one member. The mean indirect expenditure for the study participants was found to be INR 18,830.9 ± 29,424.
Discussion
In the present study we report the healthcare expenditure data on COVID-19 hospitalizations as the median OOP expenditures, the proportion of households facing CHE, and the proportion of households where OOP expenditure was sourced by distress financing. The overall median (IQR) OOP expenditures on COVID-19 hospitalizations in central Kerala were INR 7010 (1500–38,150), USD 93.57. This was the lowest reported OOP expenditure for in-patient care compared to those reported elsewhere. Evidence on costs of COVID-19 hospitalizations to date has been drawn from high income countries. According to a report on the COVID-19 hospitalization cost from Spain, the mean cost per patient was USD 12,108.23 Analysis based on co-payments data from the United States found the mean total out-of-pocket spending to be USD 3840 for privately insured patients and USD 1536 for patients with medicare services.24 The estimates from China puts the medical cost as USD 6827 per treated case while the mean daily hospitalization cost per patient for COVID-19 care in Saudi Arabia was reported to be USD 1384.57.25,26
We observed that the median OOP expenditure was nearly ten times higher (INR 38100, USD 508.67) in private as compared to the public sector (INR 2980, USD 39.78). COVID-19 has a wide spectrum of clinical presentations and the OOP expenditure was found to vary across severity categories. It was also observed that the median OOP expenditure payments for severely ill patients and patients who died were significantly higher. This was in agreement with the European Centre for Disease Prevention and Control country summary data which, when adjusted for the GDP income category, showed a positive association between OOP expenditure for COVID hospitalizations and mortality.8 When comparing the results of the present study with the costs incurred during hospitalization for other respiratory infections in India, it was observed that the out of pocket costs were substantially higher for Covid care.27 This observation was in contrast to findings from studies reported elsewhere. An analysis based on the administrative claims data among patients admitted for pneumonia between 2016 and 2019 in the United States estimates the mean out-of-pocket spending as USD1961.28 A systematic review on the health care costs of influenza-like illness in high income countries range from US$19 in Korea to US$323 in Germany.29 Though the expenses associated with general illness are not comparable with COVID-19, studies based on the National Sample Survey data report the mean OOP expenditure expenses on hospitalization for all causes to be INR 19,210.30
We found that a total of 77 (49.7%) out of the 155 eligible households studied incurred catastrophic health expenditure due to hospitalization for COVID-19. Wagstaff et al reported the global incidence of catastrophic expenditure, at a threshold of 10% income, as 11·7% in the year 2010.14 A multi-country analysis on the magnitude and distribution of OOP expenditure payments by van Doorslaer et al estimates the incidence of catastrophic payments in India, defined at 25% of non-food expenditures, to be nearly 10% in the year 2007.9 There are considerable variations observed in the CHE estimates from national surveys done across India.31 Research work based on the National Sample Survey data done in 2014 demonstrated that 24.9% of Indian households incurred CHE.32 This survey reports an increase of 17.0% in CHE from that in 2004. The World Health Survey (WHS) done in the year 2003 reported that 33.9% of households in India suffered CHE. These variations are attributed to the differences in the survey methodologies used.31 The results of our regression analyses highlight the link between CHE and per capita income. This finding further substantiates the importance of addressing the problem of income inequality which can only be resolved by providing universal health coverage and social security benefits intended to protect households from income loss associated with hospitalization. But with the government health spending standing at 1·28% of GDP, inadequate public expenditure is going to be the greatest challenge in achieving universal health care.33,34 Our study also demonstrates a robust relationship between the type of health facility where the patient sought care and CHE. A report published in the year 2021 claims that more than half of Kerala’s population rely on the public sector for episodes of acute illness.35 The state government made a policy decision to offer publicly financed decentralized medical care services to overcome the financial barriers to accessing COVID-19. This approach taken by the state government led to the establishment of district level first line and second line covid care centers which provided free treatment and accommodated a major share of hospitalizations. Our finding is consistent with the observations in other studies that found a similar healthcare seeking pattern. The 75th round of National Sample Survey (NSS) carried out in the year 2017 reports the average medical expenditure incurred during hospitalization was seven fold more in a private hospital than in a government hospital.36 The analysis from the present study adds to a group of studies that have established that comorbid conditions are significantly associated with increasing medical costs for hospitalizations for COVID-19.23,24,37 Even though the existing body of evidence from low and middle income countries emphasizes the role of health insurance in protecting households from catastrophic health costs, the present study did not identify such an association in the regression model.38 Recent research has demonstrated that coverage under the public health insurance programs for those below poverty line had no significant influence on decreasing OOP expenditure payments.39 The majority of the participants with financial protection in the study sample were privately insured. We observed a low utilization rate for Ayushman Bharath, the largest publicly financed health insurance scheme, with only 4 participants reporting using the service. This could be attributed to the slow enrollment rate and relatively lower number of registered private hospitals for the scheme in the state.
The estimation of the proportion of distress financing in the study population is imperative in understanding the sources of OOP expenditure payments for COVID-19. The present study demonstrates that one-third of the study participants (32.9%) resorted to borrowing money, private gold loans, and selling assets to meet the hospitalization expenses. This is in line with peer-reviewed evidence from India. Joe et al found that distress financing accounted for 58% and 42% share of the total OOP expenditure payments for hospitalized care in rural and urban India, respectively.20 Among the people suffering from the burden of cancer in India, distress financing occurred in 43% of the population.30 This is consistent even in the case of maternal services in India. In spite of the cash incentives for institutional delivery since the implementation of the National Health Mission, a recent study found that one in four mothers in India resorted to borrowing money or selling assets to meet the OOP expenditure expenses on institutional delivery.40
Our study has several limitations. Firstly it was not possible for us to correctly analyze the cost components in the OOP expenditure expenses, as patients who sought care in public health facilities were not provided a hospital bill or expenditure statement. Secondly, recall bias may have affected the retrospective assessment of the expenditures. Thirdly, the approach of calculating the monthly household income based on total expenditure may have underestimated the actual household income. Notwithstanding these limitations, the study provides key information that will enable policy makers to prioritize interventions to ensure health equity and universal health coverage.
Conclusion
The present study provides insight into the extent to which COVID-19 hospitalizations have disrupted household economies. Though the study population had one of the lowest reported OOP expenditure payments for COVID-19 hospitalizations worldwide in terms of absolute value, nearly half of them suffered catastrophic expenditures which led to impoverishment in approximately a third. From the study findings, it is plausible that catastrophic payments would prevent patients under home isolation for COVID-19 from seeking necessary health care. Given the current situation, the government should make an effort to scale up coverage and implementation of social health insurance programs to extend the social safety net. The findings from the study reiterated the need for such major reforms in health financing systems. Further research on the wider economic consequences of the COVID-19 pandemic would be essential for the attainment of universal health coverage in the context of unforeseen health crises across the world in the years to come.
Abbreviations
CHE, catastrophic health expenditure; CSLTC, COVID-19 second line treatment centres; GDP, gross domestic product; ICU, intensive care units; INR, Indian National rupee; LMIC, lower-middle income countries; NSS, national sample survey; OOP expenditure, out of pocket expenditure; RT-PCR, real time polymerase chain reaction; USD, United States dollar.
Data Sharing Statement
Data will be made available by the corresponding author upon request.
Ethical Approval
Institutional Review Board, Government Medical College Kottayam, Kerala No.- 94/2021 dated 11.11.2021. IRB certificate issued on 28.12.2021
Acknowledgments
The authors hereby declare that they did not receive any monetary assistance. The authors thank the following individuals for their expertise and assistance throughout all aspects of our study. 1. Mr Unnikrishnan U.G, 2. Dr. Geethadevi M, 3. Dr. Suresh Bhat, 4. Mrs Treesa Sebastian.
Disclosure
All authors declare no financial relationships or any conflicts of interest with any organizations that might have an interest in the submitted work in the previous three years.
References
1. Asrani P, Eapen MS, Hassan MI, Sohal SS. Implications of the second wave of COVID-19 in India. Lancet Respir Med. 2021;9(9):e93–e94. doi:10.1016/S2213-2600(21)00312-X
2. Cherian S, Potdar V, Jadhav S, et al. SARS-CoV-2 spike mutations, L452R, T478K, E484Q and P681R, in the second wave of COVID-19 in Maharashtra, India. Microorganisms. 2021;9(7):1542. doi:10.3390/microorganisms9071542
3. Thangaraj JWV, Yadav P, Kumar CG, et al. Predominance of delta variant among the COVID-19 vaccinated and unvaccinated individuals, India, May 2021. J Infect. 2021;84(1):94–118. doi:10.1016/j.jinf.2021.08.006
4. IndiaFightsCorona. #IndiaFightsCorona COVID-19 in India, vaccination, dashboard, corona virus tracker. Available from: https://www.mygov.in/covid-19/.
5. Thomas R, John BM, Koothapally JT, et al. Clinical and epidemiological spectrum of coronavirus disease 2019 in Central Kerala: a retrospective case series. Int J Community Med Public Health. 2021;8(3):1503–1507. doi:10.18203/2394-6040.ijcmph20210852
6. Ellis-Petersen H; The Guardian. Why Kerala is still in the grip of India’s second wave of Covid; 2021. Available from: https://www.theguardian.com/world/2021/sep/15/why-kerala-is-still-in-the-grip-of-indias-second-wave-of-covid.
7. Liao TF, De Maio F. Association of social and economic inequality with coronavirus disease 2019 incidence and mortality across US counties. JAMA Netw Open. 2021;4(1):e2034578. doi:10.1001/jamanetworkopen.2020.34578
8. El-Khatib Z, Otu A, Neogi U, Yaya S. The association between out-of-pocket expenditure and COVID-19 mortality globally. J Epidemiol Glob Health. 2020;10(3):192–193. doi:10.2991/jegh.k.200725.001
9. van Doorslaer E, O’Donnell O, Rannan-Eliya RP, et al. Catastrophic payments for health care in Asia. Health Econ. 2007;16(11):1159–1184. doi:10.1002/hec.1209
10. India, ed. Twelfth Five Year Plan (2012–2017). SAGE Publications; 2013.
11. Sarwal R, Kumar A. Health insurance for India’s missing middle. Open Science Framework; 2021. doi:10.31219/osf.io/s2x8r.
12. Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, Murray CJL. Household catastrophic health expenditure: a multicountry analysis. Lancet. 2003;362(9378):111–117. doi:10.1016/S0140-6736(03)13861-5
13. SDG Indicators. SDG Indicators. Available from: https://unstats.un.org/sdgs/indicators/indicators-list/.
14. Wagstaff A, Flores G, Hsu J, et al. Progress on catastrophic health spending in 133 countries: a retrospective observational study. Lancet Glob Health. 2018;6(2):e169–e179. doi:10.1016/S2214-109X(17)30429-1
15. Boccuzzi SJ. Indirect health care costs. In: Weintraub WS, editor. Cardiovascular Health Care Economics. Contemporary Cardiology. Humana Press; 2003:63–79. doi:10.1007/978-1-59259-398-9_5.
16. Economic Review 2017. State planning board, Thiruvananthapuram, Kerala, India; 2017. Available from: https://spb.kerala.gov.in/economic-review/ER2017/web_e/foreword.php.
17. Suryanarayana MH, Agrawal A, Prabhu S. Inequality adjusted Human Development Index for India’s States 2011. United Nations Development Programme; 2003. Available from: htpps://www.undp.org/content/dam/india/docs/inequality_adjusted_human_development_index_for_indias_state1.pdf.
18. Ghaffari Darab M, Keshavarz K, Sadeghi E, Shahmohamadi J, Kavosi Z. The economic burden of coronavirus disease 2019 (COVID-19): evidence from Iran. BMC Health Serv Res. 2021;21(1):1–7. doi:10.1186/s12913-021-06126-8.
19. Xu K, Klavus J, Kawabata K, et al. Household health system contributions and capacity to pay: definitional, empirical, and technical challenges. In: Health Systems Performance Assessment: Debates, Methods and Empiricism. 2003:124.
20. Joe W. Distressed financing of household out-of-pocket health care payments in India: incidence and correlates. Health Policy Plan. 2015;30(6):728–741. doi:10.1093/heapol/czu050
21. Jo C. Cost-of-illness studies: concepts, scopes, and methods. Clin Mol Hepatol. 2014;20(4):327–337. doi:10.3350/cmh.2014.20.4.327
22. World Bank. Principles and practice in measuring global poverty. Available from: https://www.worldbank.org/en/news/feature/2016/01/13/principles-and-practice-in-measuring-global-poverty.
23. Carrera-Hueso FJ, Álvarez-Arroyo L, Poquet-Jornet JE, et al. Hospitalization budget impact during the COVID-19 pandemic in Spain. Health Econ Rev. 2021;11:43. doi:10.1186/s13561-021-00340-0
24. Chua KP, Conti RM, Becker NV. Assessment of out-of-pocket spending for COVID-19 hospitalizations in the US in 2020. JAMA Netw Open. 2021;4(10):e2129894. doi:10.1001/jamanetworkopen.2021.29894
25. Khan AA, AlRuthia Y, Balkhi B, et al. Survival and estimation of direct medical costs of hospitalized COVID-19 Patients in the Kingdom of Saudi Arabia (Short title: COVID-19 survival and cost in Saudi Arabia). Int J Environ Res Public Health. 2020;17(20):7458. doi:10.3390/ijerph17207458
26. Li XZ, Jin F, Zhang JG, et al. Treatment of coronavirus disease 2019 in Shandong, China: a cost and affordability analysis. Infect Dis Poverty. 2020;9(1):78. doi:10.1186/s40249-020-00689-0
27. Kumar H, Misra S, Awasthi S. Estimation of medical expenditure of initial various treatment regimes in hospitalized cases of severe community acquired pneumonia in children under 5 years of age in North India. Clin Epidemiol Glob Health. 2019;7(1):41–45. doi:10.1016/j.cegh.2017.12.007
28. Eisenberg MD, Barry CL, Schilling CL, Kennedy-Hendricks A. Financial risk for COVID-19–like respiratory hospitalizations in consumer-directed health plans. Am J Prev Med. 2020;59(3):445–448. doi:10.1016/j.amepre.2020.05.008
29. Federici C, Cavazza M, Costa F, Jommi C. Health care costs of influenza-related episodes in high income countries: a systematic review. PLoS One. 2018;13(9):e0202787. doi:10.1371/journal.pone.0202787
30. Kastor A, Mohanty SK. Disease-specific out-of-pocket and catastrophic health expenditure on hospitalization in India: do Indian households face distress health financing? PLoS One. 2018;13(5):e0196106. doi:10.1371/journal.pone.0196106
31. Raban MZ, Dandona R, Dandona L. Variations in catastrophic health expenditure estimates from household surveys in India. Bull World Health Organ. 2013;91(10):726–735. doi:10.2471/BLT.12.113100
32. Pandey A, Kumar GA, Dandona R, Dandona L. Variations in catastrophic health expenditure across the states of India: 2004 to 2014. PLoS One. 2018;13(10):e0205510. doi:10.1371/journal.pone.0205510
33. Bang A. Health insurance, assurance, and empowerment in India. Lancet. 2015;386(10011):2372–2373. doi:10.1016/S0140-6736(15)01174-5
34. NHA_Estimates_Report_2015–16_0.pdf. Available from: https://main.mohfw.gov.in/sites/default/files/NHA_Estimates_Report_2015–16_0.pdf.
35. AvailDistribUtilisationHSKerala.pdf. Available from: https://spb.kerala.gov.in/sites/default/files/inline-files/AvailDistribUtilisationHSKerala.pdf.
36. KI_Health_75th_Final.pdf. Available from: http://mospi.nic.in/sites/default/files/publication_reports/KI_Health_75th_Final.pdf.
37. Miethke-Morais A, Cassenote A, Piva H, et al. COVID-19-related hospital cost-outcome analysis: the impact of clinical and demographic factors. Braz J Infect Dis. 2021;25(4):101609. doi:10.1016/j.bjid.2021.101609
38. Huffman MD, Rao KD, Pichon-Riviere A, et al. A cross-sectional study of the microeconomic impact of cardiovascular disease hospitalization in four low- and middle-income countries. PLoS One. 2011;6(6):e20821. doi:10.1371/journal.pone.0020821
39. Sinha RK. Impact of publicly financed health insurance scheme (Rashtriya Swasthya Bima Yojana) from equity and efficiency perspectives. Vikalpa. 2018;43(4):191–206. doi:10.1177/0256090918804390
40. Mishra S, Mohanty SK. Out-of-pocket expenditure and distress financing on institutional delivery in India. Int J Equity Health. 2019;18(1):99. doi:10.1186/s12939-019-1001-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.