Back to Journals » Research and Reports in Urology » Volume 11
Fexapotide Triflutate Induces Selective Prostate Glandular Pharmaco-Ablation in the Rat
Authors Averback P ![]() , Gohal R, Fuska M, Prins K, Wang P
, Gohal R, Fuska M, Prins K, Wang P
Received 17 September 2019
Accepted for publication 11 December 2019
Published 20 December 2019 Volume 2019:11 Pages 343—350
DOI https://doi.org/10.2147/RRU.S231334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Paul Averback, Rajna Gohal, Marta Fuska, Kathleen Prins, Ping Wang
Nymox Corporation, Montreal, QC, Canada
Correspondence: Paul Averback
Nymox Corporation, 9900 Cavendish Blvd, Suite 206, St. Laurent, QC H4M 2V2, Canada
Tel +1 514 332 3222
Fax +1 514 332 2227
Email [email protected]
Introduction: A clinical challenge for interventional prostate treatments for localized prostate cancer has been to elicit cancer tissue eradication which can avoid undesirable toxicities and irreparable damage to adjacent structures. Fexapotide triflutate (FT) has been shown in human clinical trials to be a well-tolerated pharmaco-ablative agent with therapeutic benefit in patients with prostate enlargement and low-grade prostate cancer.
Methods: Studies were undertaken in vitro and in the normal male rat to characterize and quantify selective ablation of prostate glandular cells exposed to fexapotide triflutate (FT) injections. N=371 2-month-old Sprague Dawley rats received direct intraprostatic injections under ether anesthesia with laparotomy (n=268 given 0.3 mL FT 0.1–2.0 mg/mL at varied schedules, and n=103 controls), and were sacrificed at intervals of 24 hr-12 months, with measurements of prostate volume, assessments of apoptosis, prostatic nerve structures, connective tissue stroma, and vasculature. In vitro prostate cell lines treated with FT were studied by electron microscopy and RNA quantification.
Results: Evidence shows that FT leads to prostate glandular cell loss not found in controls, by apoptosis within 24–72 hrs that is highly selective for achieving near-total loss of glandular epithelium at 6 to 12 months, without any adverse microscopic effects to adjacent periprostatic nerves, vascular elements, and stroma.
Conclusion: Histological studies in the rat demonstrate that FT ablative effect is selective for prostate glandular epithelium, sparing adjacent tissues and structures in the prostate including nerves, vasculature, and stroma.
Keywords: ablation, hyperplasia, cancer, BPH, urology
Introduction
Removal of prostate tissue, both benign and/or malignant, is commonly required in many prostatic disease conditions. Prostate cancers are removed by surgical means and/or radiation, thermoablation, or endoscopic strategies. In benign prostatic hyperplasia (BPH), obstructive urinary symptoms may develop from the enlarged transition zone due to glandular hyperplasia and may require ablation by surgical resection, or by laser, microwave, high-intensity ultrasound, thermal needle placement, steam, or other methods of transition zone tissue destruction.1–5 In ablation methods that destroy tissue, the zones of tissue destruction are microscopically non-selective, which can be attributed to the non-selective forces (high energy transduction, radiation) which cause the necrosis. Therefore, a traditional major challenge for treatment has been to promote or to directly produce tissue destruction that is structurally selective at the microscopic (histological) level, in order to avoid undesirable toxicities and irreparable damage to key adjacent structures. For example, transurethral resection, high energy laser extirpations and other methods may damage prostatic nerves and peri-urethral musculature, with the consequent occurrences of ejaculatory disorders, sexual dysfunction and/or incontinence.6–8
Fexapotide triflutate (FT) induces apoptosis in prostatic glandular epithelial cells and is targeted to the transition zone to help to decompress the urethral lumen to improve LUTS. Studies were undertaken in Sprague Dawley rats in order to define the histological structural vulnerabilities and differential cellular susceptibilities in order to determine the extent of FT safety when used as an injectable into the prostate. This report describes the histopathological effects in rats of FT intraprostatic injection. Selective apoptotic destruction of prostate glandular epithelial cells which spares the nerves of the prostate and other adjacent tissues is described. As far as we are aware, this is the first demonstration of a molecular treatment that can produce structurally significant and focally targeted destruction of prostate epithelial gland growth combined with complete or near-complete preservation of key nerves and structural elements in intimate structural proximity to the foci of ablation.
Materials and Methods
Experiments were designed in order to investigate tissue selectivity and susceptibilities at the histological level. All protocols were done in accordance with applicable national regulations, and carried out by individuals with training in animal handling and with anesthetic and other techniques to ensure humane treatment of animals at all times. The Animal Care Committee (ACC) of Nymox Corp approved the studies which were done in accordance with the principles described in the Guide for the Care and Use of Experimental Animals of the Canadian Council on Animal Care. Two-month-old Sprague Dawley rats (n=268) weighing 200 to 300 g, housed in groups of 2–5 per cage at room temperature (24–26°C), with standard unrestricted diet and water, were anesthetized with ether, and received intraprostatic injections visualized by laparotomy, using sterile precautions and sterile techniques, without antibiotics, of 0.3 mL of FT 0.1–2.0 mg/mL in phosphate-buffered saline (PBS) pH 7.4, administered by #26-gauge sterile needles attached to sterile syringes. Control animals (n=103) were injected with 0.5 mL solutions of a. PBS vehicle alone; b. HCl in water pH 3.0–5.0; c. inactive synthetic peptides (n=8) in PBS pH 7.4; or d. no injection. Animals were observed daily and were painlessly sacrificed after post-treatment intervals of 24 hrs to 12 months under ether anesthesia. Sub-groups of rats received repeated injections (2X-8X, on a once-weekly basis). Prostate glands were removed, bisected and immersed in 10% formalin solution, and subsequently embedded in paraffin, sectioned and stained with a. hematoxylin-eosin (H&E); b. Bielschowsky silver method for nerve fibers; c. immunohistochemical TUNEL staining. TUNEL (Terminal deoxynucleotidyl transferase (dUTP) nick end labeling) detects DNA fragmentation by labeling the 3′-hydroxyl termini in the double-strand DNA breaks generated during apoptosis. Apoptosis was evaluated microscopically in H&E stained sections, including all rats sacrificed after 24, 48, 72 hrs; 4–8 days; and 1, 3, 6, and 12 months. All sections from FT-treated rats were examined by two separate observers who tabulated extent of atrophy and apoptosis, nerve presence or absence, and nerve histological normality or abnormality, in each section. TUNEL staining was assessed in 9 animals sacrificed at 72 hrs post-treatment with FT 1 mg/mL and one PBS-treated control rat. Prostate volume (calculated by approximation to a sphere using the mean of 8 perpendicular diameters (2 per section at 90 degrees; on four sections) and calculations of 4/3 π (D/2)3) were assessed in all animals and all controls. Tangentially cut blocks and sections were excluded from measurements. Qualitative ultrastructural examination (Paragon Bioservices, Baltimore, MD, USA) of pellets from prostate cell lines PC3 and LNCAP-treated with FT 2.5 mg/mL in vitro was done on pellets at baseline, 12, 24, and 48 hrs (Analytical Biological Services, Wilmington, DE, USA). Total RNA of the treated pellets and untreated baseline controls was assayed at 8, 24, and 48 hrs post treatment with FT 2.5 mg/mL. RNA from each sample was isolated using Qiagen RNAeasy Kit with an on-column DNAase digestion, and was quantified spectrophotometrically (A260/A280) and by agarose gel electrophoresis. Additional independent safety studies were undertaken in beagle dogs under sodium pentothal or propofol anesthesia using the transabdominal route of administration with ultrasound guidance. A total of 12 dogs received intraprostatic FT 0.28–1.6 mg/kg and 18 control dogs received either FT administered to non-prostatic (non-P) adjacent tissues (N=12; bladder injection N=4; rectal injection N=4; urethral injection N=4) or PBS pH 7.4 into non-P adjacent tissues (N=6). The dogs were examined at necropsy 14 days post injection after painless sacrifice either with sodium pentothal or propofol and prostate glands were weighed (Nucro-Technics, Scarborough, ON, Canada, with protocol approvals from ACC of Nucro-Technics).
Results
Histological results in control rats showed occasional examples (6/92 control rats) with recognizable needle insertion tracts. Two (2/12) rats injected with HCl pH 3.0–5.0 had focal ischemic or hemorrhagic infarctions and necrosis involving <5% of the cross-sectional area. Other HCl pH 3.0–5.0-treated animals had microscopic foci (<2% of cross-sectional area) with focal necrosis. There were no other examples of injection-induced hematoma >5% of the cross-sectional area. All controls exhibited nerve presence. Controls did not show the histological features described below in FT-treated rat prostate. Apoptotic figures in untreated controls were sparse (<1 per 100X field). Glandular epithelium showed no significant lasting changes in untreated controls or in any controls treated with vehicle alone or with inactive peptides in PBS. PBS injected prostates were swollen at time intervals <72 hrs. At time intervals >7 days in saline-injected rat prostates there was no further swelling detectable.
FT-treated animals showed the following histological changes not found in controls. 1. Apoptotic changes (Figure 1A–F) consisting of large areas with very prominent cellular changes of hyperchromatic pyknotic convoluted nuclei progressing to the appearance of smaller roundish broken nuclei and apoptotic bodies, with cellular dissolution with pallor, cell ghosts and cell disappearance at 24, 48, 72 hrs, 1 week, and to a lesser extent in the ensuing weeks. At 6 months and 1 year, apoptotic changes were infrequent or no longer seen. 2. TUNEL positivity (Figure 1D–F): dark brown immunoperoxidase TUNEL staining is seen in the areas of the apoptotic changes described above in animals at 72 hrs. 3. Normal appearing nerves at all time points including 6 months and 1 year (Figure 2A–E). 4. Atrophy (Table 1 and Figure 3) consisting of significantly reduced overall prostatic volume. Histologically, glandular epithelium is initially disrupted, and then progressively fragmented and diminished, and gradually disappears (Figure 1A–E). After 6 months–1 year, there is near-complete to complete loss of glandular epithelium throughout the prostate (Figure 3). Stromal connective tissue remains, and nerves and blood vessels are intact at all time intervals.
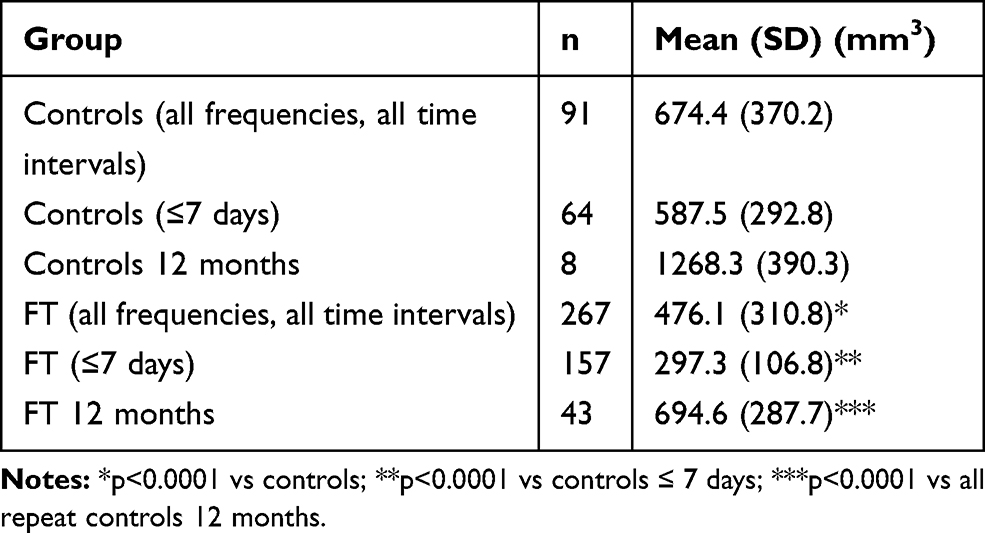 |
Table 1 Prostate Volume in FT-Treated Rats and Controls |
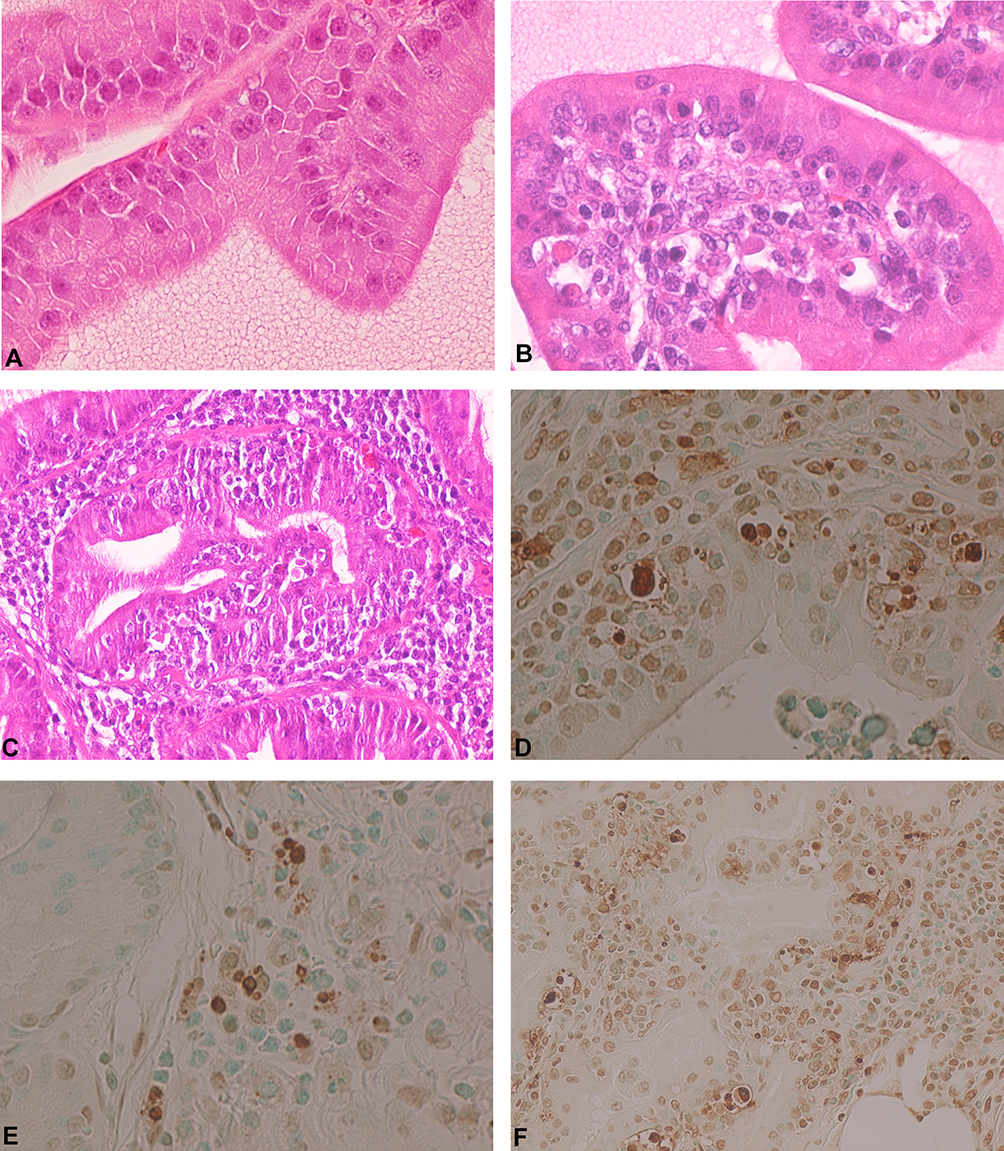 |
Figure 1 Prostate changes after FT administration. (A) Normal rat prostate. H&E ×400 original magnification. (B) Rat prostate 72 hr post FT 1 mg/mL 300µL intraprostatic, showing apoptotic changes in glandular cells. H&E ×400 original magnification. (C) Rat prostate 72 hr post FT 1 mg/mL 300 µL intraprostatic, showing severe diffuse apoptotic changes throughout the field. H&E ×200 original magnification. (D) Rat prostate 72 hr post FT 1mg/mL 300 µL intraprostatic, showing apoptotic changes in glandular cells. TUNEL positive cells stain dark brown. TUNEL ×400 original magnification. (E) Rat prostate 72 hr post FT 1 mg/mL 300 µL intraprostatic administered once daily for 3 days, showing apoptotic changes in glandular cells. TUNEL positive cells stain dark brown. TUNEL ×400 original magnification. (F) Rat prostate 72 hr post FT 1 mg/mL 300 µL intraprostatic, showing widespread apoptotic changes in glandular cells. TUNEL positive cells stain dark brown. TUNEL ×200 original magnification. |
 |
Figure 2 Normal nerves (arrows) in rat prostate after FT administration. (A) Normal nerve in atrophied rat prostate 12 months post FT 2 mg/mL 300 µL intraprostatic administered once weekly for first month, H&E ×400 original magnification. (B) Normal nerve in atrophied rat prostate 12 months post FT 1mg/mL 300 µL intraprostatic administered once weekly for first month, H&E ×400 original magnification. (C) Normal nerve in atrophied rat prostate 12 months post FT 1 mg/mL 300 µL intraprostatic administered once weekly for first month, Bielschowsky silver stain, ×200 original magnification. (D) Normal nerve in atrophied rat prostate 12 months post FT 1 mg/mL 300 µL intraprostatic administered once weekly for 1st month, higher power view of Figure 3C. Bielschowsky silver stain, ×400 original magnification. (E) Normal nerve in atrophied rat prostate 12 months post FT 2 mg/mL 300 µL intraprostatic administered once weekly for 2 months, Bielschowsky silver stain, ×600 original magnification. |
 |
Figure 3 Prostate atrophy after FT administration. Atrophic rat prostate with near total loss of glandular epithelium throughout gland 12 months post FT 2 mg/mL 300 µL intraprostatic administration. H&E ×20 original magnification. |
Ultrastructural changes found in vitro after 24–48 hrs consist of nuclear changes (hyperconvoluted electron-dense nuclei with prominent invaginations and foldings; nuclear membrane disruptions and eventually prominent nuclear blebs (Figure 4)); organellar disruptions with vesicular swelling and disruption; and progressive cell disruption, fragmentation, and disappearance into debris. Cell culture pellets showed RNA depletion with >40% reduction at 8 hrs compared to baseline, and no RNA present at 24 hrs and 48 hrs post treatment with FT.
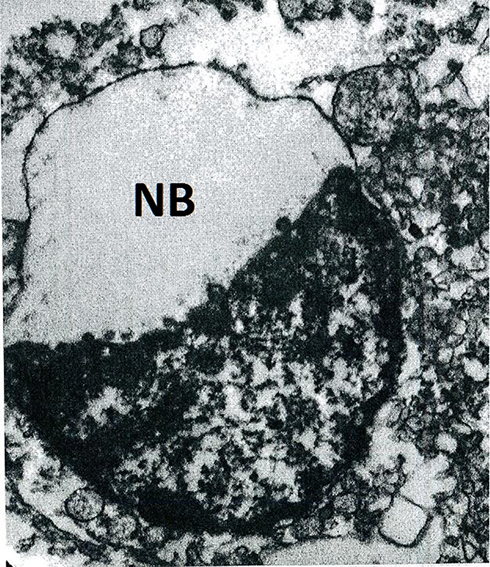 |
Figure 4 Massive apoptotic nuclear bleb (NB) in LNCAP prostate cancer cell line in vitro 24 hrs post treatment with FT 2.5 mg/mL. Electron microscopy, ×20,000. |
Mean prostate volume (MPV) of FT-treated rats at all frequencies, concentrations and time intervals (n=267) was 476.8 mm3 (SD 310.3), compared to MPV of controls (n=91) 717.3 (SD 402.4) (p<0.0001, CI −317.62 to −163.38, t test). The MPV of all FT-treated rats at all concentrations <7 days post-treatment (n=157) was 297.3 mm3 (SD 106.9), compared to the MPV of controls <7 days (n=64) 587.5 (SD 292.8) (p<0.0001, CI −343.15 to −237.31, t test) (Table 1, Figure 5A and B). All adequately powered individual time point matched values were statistically significantly reduced in FT-treated rats compared to vehicle control-injected animals, with no consistent quantitative differences in volume reductions in single-dose concentrations in the 0.5–5.0 mg/mL range, nor between singly and multiply injected rats in the 1 mg/mL or 2 mg/mL dosages. The mean prostate weights in the dog injection studies were decreased in the intraprostatic FT group (mean 5.21g, SD 1.8) compared to control groups FT non-P (mean 8.40g SD 3.73, p<0.01, 95% CI −5.3206 to −1.05954) and vs all controls (mean 8.38g SD 3.6, p<0.01, 95% CI −5.1247 to −1.2153). In the dog safety studies standard plasma biochemical parameters, hematology measurements, necropsy studies and clinical safety assessments were all within normal range in both FT-treated and control animals.
 |
Figure 5 Mean prostate volume (mm3) vs time in FT-treated animals and controls. (A) Mean prostate volume (mm3) vs time in FT 1 mg/mL-treated rats vs vehicle-alone-treated rats, 24 hrs to 7 days, showing significant reductions at all time points. (B) Mean prostate volume (mm3) vs time in FT 1 mg/mL and 2 mg/mL-treated rats vs vehicle-alone-treated rats, 0 to 12 months, showing significant reductions at all time points (6-month control value was not done). |
Discussion
In rat prostate, FT selectively causes loss of cell membrane integrity, mitochondrial metabolic arrest, depletion of RNA, DNA lysis and aggregation, and cell fragmentation and cell loss. The apoptotic process leads to typical ultrastructural progressive changes of membranous disruption and swelling, progressively deepening nuclear invaginations9 with eventual nuclear bleb formations (Figure 4 Reference [10]) and cell death and fragmentation into apoptotic bodies. Histologically, typical apoptotic changes with positive immunohistochemical staining of markers for apoptosis are found throughout the injected areas for up to several weeks after treatment.
FT has been extensively tested in patients with BPH and in men with low-grade (ISUP Gleason Group 1) prostate cancer. The compound and placebo controls have been administered by the transrectal route in over 1700 procedures in 9 human clinical trials. Phase 3 trials showing long-term benefits without molecular adverse effects have been presented in detail.9–11 In these large long-term clinical trials in men with BPH, there were no instances in any patients of significant sexual adverse events attributed to the drug, and no clinical evidence of any damage or toxicity to any nerve structures, or urethra, bladder, rectum, or adjacent periprostatic tissues. Semen analysis and plasma testosterone measurements showed no difference from controls in the above human clinical studies, and sexual function questionnaire values were improved long-term in prior treatment-naive patients treated with FT compared to placebo patients where there was worsening.9 In independent toxicology studies done using administration of intravenous (IV) dosages of FT in dogs, rabbits and rats, there were no clinical, hematological, biochemical or histological signs of toxicity after IV dosages as high as 25 mg/kg and in toxicology studies done with intraprostatic injections, there was no extraprostatic toxicity.
The studies detailed in the present report demonstrate that FT leads to apoptosis in rat prostate glandular epithelium and to widespread but selective gland epithelial cell loss and atrophy. The reduction in prostate volume in the rat studies and the prostate weight reduction in the dog studies reported here were in the −30 to −50% range compared to controls. The rat dosage in the studies reported here involved a volume infusion approximately equal to the volume of the rat prostate allowing for the FT to reach all or nearly all of the gland acinar epithelial cell populations. The rat prostate is highly cellular compared to the human BPH gland, the latter which is up to 50% stromal in structure. Furthermore, the human BPH prostate weighs up to 70–100 g or more and the FT volume (10 mL dose) per prostate volume dosage in humans is proportionally smaller compared to the rat per prostate volume experimental dosage. In the human the combination of i. FT dosage that is 10–20% of gland volume, and ii. glandular epithelial target of approximately 50% of tissue, implies a percentage of atrophy that will be considerably less than the rat – the latter where the normal gland is predominantly cellular and the volume infused was ≥ the total gland volume. Therefore, the high percentage of atrophy in the rat is not linearly comparable to the human. In human BPH FT trials the gland shrinkage per single dose (allowing for untreated 5% per year enlargement in BPH subjects)12 has been in the 5–10% range, as compared to the data from injections in normal rat prostate presented here, showing ≥30% shrinkage, which is consistent with the above considerations.
Repeated dosages did not add to response in terms of observable atrophy. This is very likely attributable to saturation of effect as the entire rat gland is exposed to the dosage given in these studies. This is further reinforced by the histological findings showing that single-dose FT 1 mg/mL in the rat leads to total or near-total depletion of glandular acinar epithelium after 12 months, thereby indicating that there were relatively few or no further cell targets remaining to kill after the first dosage. In the human studies, it has been clearly shown that repeat dosage leads to added clinical benefit,9 which may be related to there being remaining cells to target, which is consistent with quantitative considerations discussed above.
These studies were undertaken in normal rats and did not utilize any rat models of BPH induced by hormones or other means.13,14 The purpose was to explore and document over time the effects in a natural context treating normal prostate cells. Typical BPH histologically affects up to half of men over 50, and perhaps 90% of men by age 80–90.1–5 There are many well-documented mechanisms and abnormalities relevant to lower urinary tract symptoms (LUTS) caused by BPH, and testing of FT in other relevant animal models of BPH remains to be done. FT-proven effectiveness in typical human cases of BPH indicates that the normal rat prostate growth observed longitudinally over time is a reasonable model, amongst others, to test the effect on nerves, gland volume, apoptosis, and other factors relevant to BPH and LUTS.
There are inherent limitations to the quantitative analysis of histological findings. The main results of the reported studies are that FT leads to extensive prostate glandular epithelial apoptosis and selective cell loss within the prostate, and there is sparing of nerves, vasculature, stroma and adjacent tissues. Gland-specific molecular ablation of overgrown prostatic glands in the transition zone in the prostate with nerve sparing is a novel mechanism of action for a prostate therapeutic which has important benefits. The prostate gland performs vital male reproductive functions and is situated in intimate proximity to many important pelvic structures (urethra, bladder, rectum, seminal vesicles). Non-specific ablation in some percentage of patients inevitably leads to irreparable damage to those structures with resultant functional deficits. A review of all the ablative devices and agents and their collateral damage toxicities is beyond the scope of this report; however, in general prostatic nerve damage commonly leads to sexual deficit (ejaculatory dysfunction, impotence, loss of libido); urethral damage commonly leads to retrograde ejaculation and/or strictures; and rectal or bladder damage can result in incontinence, fistulae, strictures, and/or dysfunction. The specificity of FT avoids this large spectrum of adverse events from non-specific ablation-related damage to other structures. The extensive well-known toxic effects of non-specific ablation are documented in the device studies literature and device labels for high energy transduction ablation techniques (laser; needle ablations; microwave; cryotherapies; high-intensity ultrasound), radiation (external beam; brachytherapy seeds); and in the literature for non-specific injectable ablatives (carbolic acid; alcohol, etc.). In all of the aforementioned and other methods, there is non-specific ablation and inevitable risk of permanent damage to some degree of clinically relevant adjacent structures.
These studies in the rat have shown that FT intraprostatic administration consistently leads to significant and selective prostate glandular epithelial apoptotic cell loss and gland shrinkage, with the absence of discernible damage to adjacent and surrounding tissues including nerves, blood vessels and other important structures. Gland-specific targeted molecular ablation of overgrown prostatic glands in the transition zone in the prostate with nerve sparing is a novel mechanism of action for a prostate therapeutic which has important benefits. The nerve and stromal sparing for peri-prostatic tissues provides an objective underlying basis for the observed safety of FT treatment in human BPH studies.
Conclusion
A major challenge for prostate treatments has been to produce or promote beneficial targeted gland destruction that is structurally selective at the microscopic tissue level in order to avoid undesirable toxicities and irreparable damage to important adjacent structures. Fexapotide triflutate (FT) has been shown in human clinical trials to be a well-tolerated pharmaco-ablative agent with therapeutic benefit in patients with prostate enlargement and low-grade prostate cancer. Evidence from experimental animal studies shows that FT leads to prostate glandular cell loss not found in controls, by apoptosis that is highly selective with sparing of nerves, vascular elements and stroma, and near-total loss of glandular epithelium at 12 months.
Acknowledgments
The authors gratefully acknowledge Dr Kresimir Pucaj and colleagues (Nucro-Technics, Scarborough, ON) who performed the cited toxicology studies. The authors thank Dr Neal Shore for kindly reviewing the report and for his helpful suggestions.
Disclosure
Dr Paul Averback owns stock in Nymox Corp and is employed and funded by Nymox Corp. In addition, Dr Averback has a patent PCT WO 2016120807A1. Ms Kathleen Prins and Mrs Rajna Gohal are employed by Nymox Corp. Mrs Marta Fuska and Dr Ping Wang are former Nymox Corp employees. The authors report no other conflicts of interest in this work.
References
1. Bushman W. Etiology, epidemiology, and natural history of benign prostatic hyperplasia. Urol Clin North Am. 2009;36(4):403–415.
2. Jacobsen SJ, Girman CJ, Lieber MM. Natural history of benign prostatic hyperplasia. Urology. 2001;58(6Suppl 1):
3. Gravas S, Bach T, Bachmann A, et al. Guidelines on the management of non-neurogenic male lower urinary tract symptoms (LUTS), incl benign prostatic obstruction (BPO). European Association of Urology; 2015. Available from: www.uroweb.org/guidelines.
4. McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–1803. doi:10.1016/j.juro.2011.01.074
5. Gratzke C, Bachmann A, Descazeaud A. EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2015;67:1099–1109. doi:10.1016/j.eururo.2014.12.038
6. Zong HT, Peng XX, Yang CC, et al. The impact of transurethral procedures for benign prostate hyperplasia on male sexual function: a meta-analysis. J Androl. 2012;33(3):427–434. doi:10.2164/jandrol.111.013490
7. Rassweiler J, Teber D, Kuntz R, et al. Complications of transurethral resection of the prostate (TURP): incidence, management, and prevention. Eur Urol. 2006;50(5):
8. Malaeb BS, Yu X, McBean AM, et al. National trends in surgical therapy for benign prostatic hyperplasia in the United States (2000–2008). Urology. 2012;79(5):1111–1116. doi:10.1016/j.urology.2011.11.084
9. Shore N, Tutrone R, Efros M, et al. Fexapotide triflutate: results of long‑term safety and efficacy trials of a novel injectable therapy for symptomatic prostate enlargement. World J Urol. 2018;36(5):801–809. doi:10.1007/s00345-018-2185-y
10. Shore N, Tutrone R, Roehrborn CG. Efficacy and safety of Fexapotide triflutate in outpatient medical treatment of male lower urinary tract symptoms associated with benign prostatic hyperplasia. Ther Adv Urol. 2019;11:1–16. doi:10.1177/1756287218820807
11. Shore N. NX-1207: a novel investigational drug for the treatment of benign prostatic hyperplasia. Expert Opin Investig Drugs. 2010;19(2):305–310. doi:10.1517/13543780903555196
12. Loeb S, Kettermann A, Carter HB, et al. Prostate volume changes over time: results from the Baltimore longitudinal study of aging. J Urol. 2009;182:1458–1462. doi:10.1016/j.juro.2009.06.047
13. Scolnik MD, Servadio C, Abramovici A. Comparative study of experimentally induced benign and atypical hyperplasia in the ventral prostate of different rat strains. J Androl. 1994;15:287–297.
14. Julia-Guilloteau V, Mevel K, Oudot A, et al. Prostate hypertrophy induced by testosterone: effect of oxybutynin in an experimental model of overactive bladder in conscious rats. Eur Urol Suppl. 2006;5(2):119. doi:10.1016/S1569-9056(06)60394-1
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.