Back to Journals » International Journal of Women's Health » Volume 17
Fetal Interventricular Septum Volume Evaluated by Four-Dimensional Ultrasound Using Spatiotemporal Image Correlation (STIC) and Virtual Organ Computer-Aided Analysis (VOCAL) in Fetuses from Gestational Diabetes Mellitus Pregnant Women Compared to Fetuses from Healthy Pregnant Women
Authors Rachatakarn R ![]() , Luangdansakul W, Kanjanasingh T, Bhamarapravatana K, Suwannarurk K
, Luangdansakul W, Kanjanasingh T, Bhamarapravatana K, Suwannarurk K ![]()
Received 12 September 2025
Accepted for publication 9 December 2025
Published 16 December 2025 Volume 2025:17 Pages 5479—5486
DOI https://doi.org/10.2147/IJWH.S564359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Rachata Rachatakarn,1 Wiyada Luangdansakul,1 Teenat Kanjanasingh,1 Kornkarn Bhamarapravatana,2 Komsun Suwannarurk3
1Department of Obstetrics and Gynecology, Bhumibol Adulyadej Hospital, Royal Thai Air Force, Bangkok, Thailand; 2Department of Preclinical Sciences, Faculty of Medicine, Thammasat University, Pathumthani, Thailand; 3Department of Obstetrics and Gynecology, Faculty of Medicine, Thammasat University, Pathumthani, Thailand
Correspondence: Wiyada Luangdansakul, Department of Obstetrics and Gynecology, Bhumibol Adulyadej Hospital, Royal Thai Air Force, Bangkok, 10220, Thailand, Tel +66839928978, Email [email protected]
Purpose: To evaluate fetal interventricular septum (IVS) volume in pregnant women with gestational diabetes mellitus (GDM) and compare it with that of healthy pregnant women using 4D ultrasound with spatiotemporal image correlation (STIC) and virtual organ computer-aided analysis (VOCAL) methods.
Patients and Methods: This prospective cross-sectional study was conducted at Bhumibol Adulyadej Hospital, Royal Thai Airforce, Bangkok, Thailand, from November 2024 to March 2025. Pregnant women with a gestational age (GA) between 29 and 34 weeks were enrolled and divided into two groups: GDM and healthy controls. Fetal IVS volume was measured using 4D ultrasonography with STIC and VOCAL. Maternal, fetal, and demographic data were collected and analyzed.
Results: A total of 111 participants were included: 63 in the GDM group and 48 in the control group. The GDM group was significantly older (33.0 vs 27.9 years) and had a higher BMI (31.1 vs 26.8 kg/m2). Mean fetal IVS volume was significantly greater in the GDM group (347.1 mm3 vs 221.5 mm3). Adverse neonatal outcomes were comparable. The cut-off fetal IVS volume for predicting neonatal hyperbilirubinemia (HBB) and respiratory distress syndrome (RDS) was 419.8 mm3. Sensitivity for predicting HBB and RDS was 55.0 and 56.0%, with negative predictive values of 94.0 and 95.2%, respectively.
Conclusion: Fetal IVS volume was significantly higher in GDM pregnancies. A cut-off value of 419.8 mm3 may be useful in predicting HBB and RDS risk, with high negative predictive value, suggesting its potential as a screening tool during the early third trimester.
Keywords: fetal interventricular septum, diabetes mellitus, pregnancy, four-dimensional ultrasonography
Introduction
Diabetes mellitus (DM) in pregnancy included both DM that was diagnosed before pregnancy and DM that occurred during pregnancy known as gestational diabetes mellitus (GDM). In Thailand, there were more than 6.5 million DM patients in 2024 and the trend kept on rising.1 At Bhumibol Adulyadej Hospital (BAH), the prevalence of DM in pregnancy in 2024 was 24.7%.
DM in pregnancy causes various adverse pregnancy outcomes effecting both mother and fetus, for example, pregnancy induced hypertension (PIH), preterm birth, hyperbilirubinemia (HBB) of newborn and large for gestational age.2,3 Diabetes in pregnancy was also associated with fetal heart structural anomalies and functional impairment, including septal defects and cardiac hypertrophy.4–7 Maternal and fetal hyperglycemia induced fetal hyperinsulinemia. Insulin was cardiomyotrophic hormone. Increment of cardiac septum volume was its consequence.4–7 Fetal echocardiography can be used to evaluate these anomalies. Fetal cardiac hypertrophy was reported to be an important etiology of dead fetus in utero (DFIU) as it was an important risk for heart failure in utero.8 Poorly controlled DM may result in adverse neonatal outcomes such as neonatal intensive care unit (NICU) admission, stillbirth and neonatal death.8–10
Traditionally, myocardial thickness was assessed by measuring interventricular septum (IVS) thickness using M-mode and 2-dimensional (2D) ultrasound. However, the 2D ultrasonography technique might have limited sensitivity, especially for mild cardiac hypertrophy cases. The 4-dimensional (4D) ultrasound, which includes spatiotemporal image correlation (STIC) and the virtual organ computer-aided analysis (VOCAL) method, provides better identification of fetal heart ventricular wall edges.11 Measurements of the fetal IVS could be done with higher accuracy. Earlier diagnosis of fetal cardiac hypertrophy would be achieved with 4D ultrasonography.11
This study aimed to evaluate the fetal IVS volumes in GDM and healthy pregnant women using 4D ultrasound with STIC and VOCAL methods. Correlations between abnormal fetal IVS volume and adverse pregnancy outcomes were also studied.
Materials and Methods
The study protocol was approved by Bhumibol Adulyadej Institutional Review Board (BAIRB) (IRB registration Number 62/67) In June 2024. The clinical trial registration number was TCTR20241016006. Consent forms were obtained from all the participants. This study was a prospective cross-sectional study to assess fetal IVS volumes in fetuses of GDM and healthy pregnant women using 4D ultrasound with STIC and VOCAL methods.
Singleton pregnant women were recruited from the antenatal care clinic (ANC) of the department of obstetrics at the BAH, Royal Thai Air Force, Bangkok, Thailand, between November 2024 and March 2025. The population was divided into two groups: the GDM group and the healthy group. The inclusion criterion was singleton pregnancies with gestational age (GA) from 29 to 34 weeks. The GA was based on the last menstrual period (LMP) as confirmed by an ultrasound examination performed before 20 weeks of gestation. All pregnant women had their ANC and were delivered at BAH. The exclusion criterions were fetuses with concurrent cardiac anomalies or chromosomal abnormalities and overt or pre-gestational DM mother.
DM screening was offered to all pregnant women. Overt or pre-gestational DM was diagnosed when hemoglobin-A1c was greater than 6.5%, random blood sugar during the first trimester or at mother’s first ANC visit that exceeded 200 mg/dL and a fasting blood sugar greater than 126 mL/dL. Overt DM was excluded. A 75-g oral glucose tolerance test (OGTT) was used as a diagnostic test for GDM with a cut-off of ≥92 mg/dL fasting blood sugar, ≥180 mg/dL after one hour, ≥153 mg/dL after two-hours.
All pregnant women included in this study were examined once using the Voluson E8 and Voluson E10 apparatus (General Electric Medical System, Zipf, Austria) with a convex and volumetric (RAB 4–8 L) probes. The acquisition angle was 30 to 40 degrees with an acquisition time of 10 to 15 seconds. Fetal echocardiograms were performed by multiple specialists of our maternal and fetal medicine department.
The ultra-sonographic study was initially performed by systematic evaluation of the fetal heart using 2D ultrasound. Then the probe was then positioned to obtain a four-chamber view of fetal heart. 4D cardiac volumes were acquired using STIC method during fetal rest and maternal apnea. The 4D cardiac volume images were obtained three times, respectively. Only one of the three 4D cardiac volume images, selected by the examiner for the best quality, was analyzed offline.
The axial plane of the multiplanar mode was selected to perform the off-line measurements of the fetal IVS volume using the viewpoint program version 6.0 (General Electric Medical System, Zipf, Austria). The IVS was measured at the ventricular ends of both ventricles during the diastolic phase of the cardiac cycle, which is the widest period of the ventricles. The 4D cardiac volume image was rotated around the horizontal view to position the apex of the fetal heart to 12 o’clock. The VOCAL method was then used to manually draw a figure around the ventricular septal edge (Figure 1). The 4D cardiac image was then rotated 30 degrees around the horizontal axis. This process was repeated six times. The software then automatically calculated the fetal IVS volume. The intraclass correlation coefficient was calculated. The values were 0.97 and 0.98 for single and average measurement, respectively.
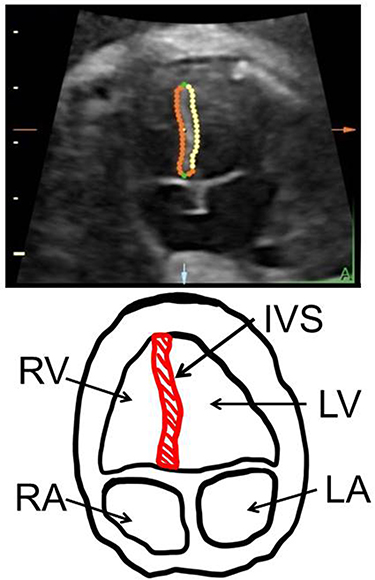 |
Figure 1 Axial plane of fetal interventricular septum measurements. Abbreviations: LV, left ventricle; RV, right ventricle; RA, right atrium; LA, left atrium; IVS, fetal interventricular septum. |
Sample size calculation was calculated based on Bravo-Valenzuela’s work.12 Fetal IVS volume of GDM and control groups in Bravo-Valenzuela’s work was 0.3 ± 0.2 and 0.2 ± 0.1 cubic centimetre.12 Study and control groups’ ratio were 1/1. The alpha and beta error rates were set at 0.05 and 0.15, respectively. The minimum number of cases per group was at least 45. Due to long period of follow up, healthy group has high possibility to deliver at other hospital. Fifty percent compensation was added. The total sample size in both the study and healthy groups was 67 cases per group.
Clinical variables such as maternal age, parity, body mass index (BMI), GA at the time of ultrasound examination were collected. Others clinical outcomes, namely as preterm delivery, low Apgar score, NICU admission, length of stay, neonatal birth weight, neonatal hypoglycemia, neonatal hyperbilirubinemia (HBB), respiratory distress syndrome of new born (RDS), stillbirth, birth injury and PIH were then collected by medical document review.
Data analysis was conducted using Statistical Package for the Social Sciences (SPSS), version 20 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means with standard deviations. While categorical data were summarized as frequencies and percentages. To compare the two groups, t-test and chi-square were applied. Analysis of covariance (ANCOVA) was used to control for differences between the two groups. A p-value less than 0.05 was considered statistically significant.
Results
A total of 111 singleton pregnancies were included as shown in Figure 2. Sixty three and 48 patients with GDM and healthy patients were included, respectively. Participants in the study group were older (33.0 vs 27.9 years) and had a higher BMI (31.1 vs 26.8 kg/m2) than those in the healthy group, with statistically significant differences. Other demographic data, namely GA and parity in both groups were comparable. Mean fetal IVS volume of the study group was significantly higher than that of the healthy group (347.1 vs 221.5 mm3). After age and BMI adjustment by ANCOVA, IVS volume of the study group was still higher than that of the healthy group (p-value = 0.003). Other adverse neonatal outcomes, namely preterm birth, RDS, HBB, PIH and NICU admission of both groups were comparable as presented in Table 1. There were no cases of low Apgar scores or stillbirths in this study. Only one case of a forceps mark on the newborn’s face was reported in the healthy group.
 |
Table 1 Clinical and Ultra-Sonographic Characteristics of the Healthy and GDM Pregnant Woman (n = 111) |
 |
Figure 2 Flow chart of study of fetal interventricular septum measurement between DM and control groups. Abbreviations: STIC, spatio-temporal image correlation; GDM, gestational diabetes mellitus; OGTT, oral glucose tolerance test. |
Table 2 presented the predictive values of fetal IVS volume for predicting adverse neonatal outcomes namely HBB and RDS. The cut-off point of fetal IVS volume to predict HBB and RDS was 419.8 mm3 (Figure 3). The sensitivities of fetal IVS volume to predict HBB and RDS were 55.0 and 56.0%, respectively. The negative predictive values (NPVs) of fetal IVS volume were 94.0 and 95.2%, respectively.
 |
Table 2 Cut Points Level of Fetal Interventricular Septum (IVS) Volume to Predict Hyperbilirubinemia (HBB) and Respiratory Distress Syndrome (RDS) of Newborn |
 |
Figure 3 Receiver operative curves (ROC) of fetal IVS volume to predict HBB and RDS. Abbreviations: HBB, hyperbilirubinemia of newborn; RDS, respiratory distress syndrome of newborn; AUC, area under curve; NPV, negative predictive value. |
Discussion
During the study period, a high percentage of healthy subjects delivered at other hospitals. One-quarter (19 out of 67) of the healthy group returned to their hometowns for delivery. Bhumibol Adulyadej Hospital (BAH) is located in the northern part of Bangkok. Many participants who worked and lived in this area originally came from rural regions. After delivery patients usually raise their babies with their own parents in their home town. Subjects in the study group were aware of their disease and the risk of their babies. Only a few of them (4 out of 67) returned to their hometown hospital to deliver their babies.
Participants in the GDM group were older (33.0 vs 27.9 years), more obese (31.1 vs 26.8 kg/m2), and had higher fetal IVS volume (347.1 vs 221.5 mm3) than those in the healthy group, with statistically significant differences. After adjusting for age and BMI, the fetal IVS volume in the study group remained higher than in the healthy group. Compared to previous studies, Simjak, Söylemez, Samath, and Turgut reported that the fetal IVS thickness in diabetic subjects was significantly higher than in the healthy group.13–16 Sapanont from Thailand reported that the fetal IVS thickness of the overt DM subjects and GDM was similar.17 All Simjak’s, Söylemez’s, Samath’s and Turgut’s studies, subjects’ age of DM and healthy groups were comparable.13–16 However, Sapanont’s study revealed higher age of GDM pregnant woman than those of overt DM pregnant woman.17 The IVS thickness of the diabetic and control groups in Sapanont’s study was similar.17 Bravo-Valenzuela’s study from Brazil in 2022 reported that fetal IVS by volume measurement of overt DM pregnant woman was higher than those of the healthy group even though the overt was younger than appeared healthy.12 In the current study, the age of participants in the study group was significantly higher than that of participants in the control group. Their fetal IVS volume was higher than that of the control group and remained higher after adjusting for age. We suggested that age was not the dependent factor for fetal IVS and recommended that IVS volume measurement to be used for prediction of adverse neonatal outcomes among GDM mothers.
In the studies by Simjak, Söylemez, and the current study, the BMI of participants with diabetes was higher than that of the healthy group.13,14 Fetal IVS measurement from both thickness and volume technique in diabetic subjects were significantly higher than values from the control group.13,14 In the current study, after adjusting for BMI in both groups, the fetal IVS volume of the study group remained higher than that of the healthy group. Compared those former works to Sapanont’s study, subjects in Sapanont’s were only GDM and overt DM, the investigators reported comparable BMI between GDM and overt DM groups.17 Sapanont concluded that the fetal IVS thickness was similar between the two types of DM.17 From the current study, fetal IVS by volumetric measurement of diabetic group was higher than that of healthy group. In this study, BMI was not found to be a dependent factor for fetal IVS volume. Comparison of the current to the previous study were summarized and presented in Table 3. Differences of population and methodology of the previous studies, deeper exploration of differences of the present to the previous studies were difficult.
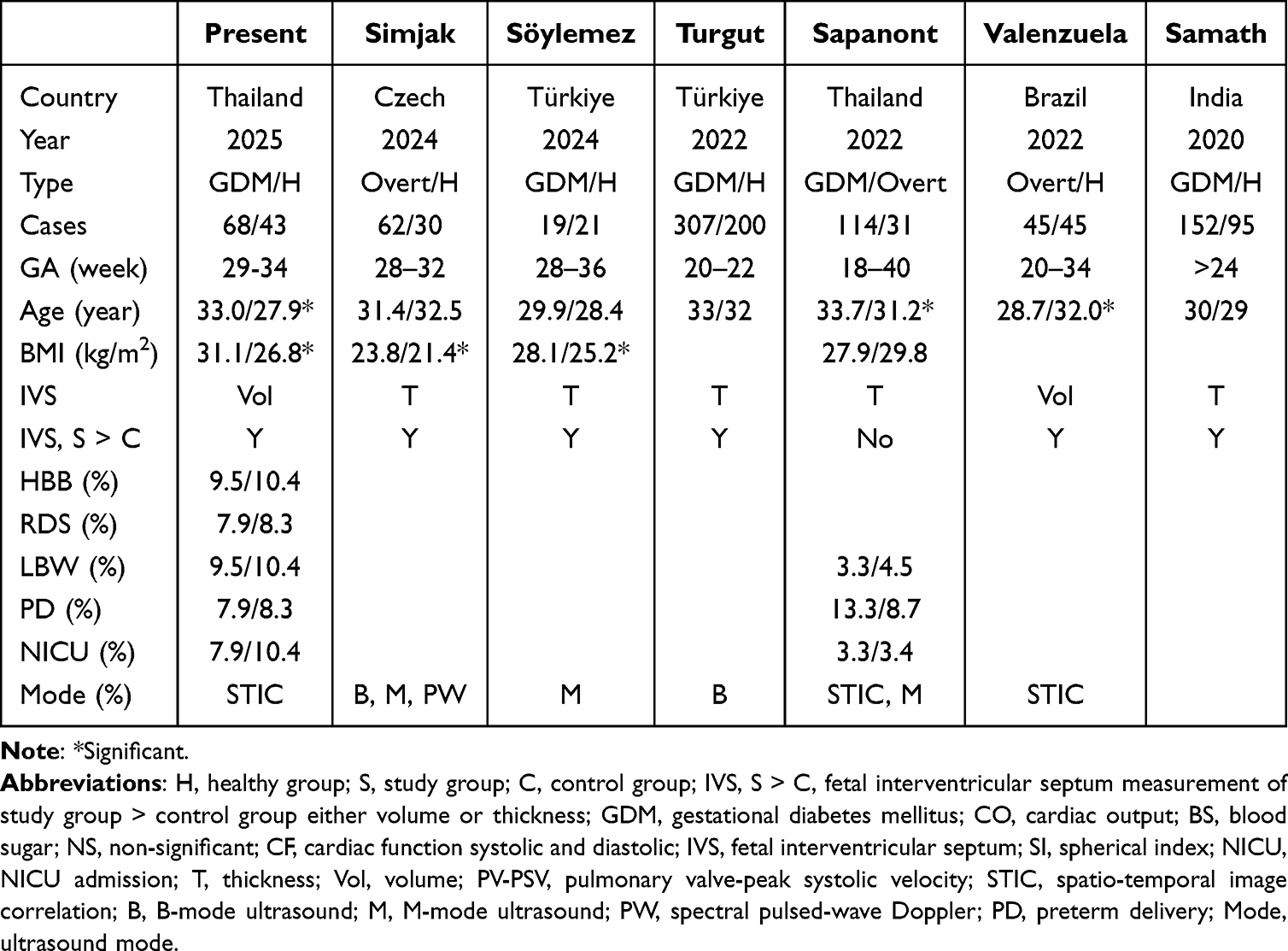 |
Table 3 Comparisons of Interventricular Septum Measurements Study of the Current to the Previous Studies |
According to Table 2, participant with fetal IVS volume less than 419.8 mm3 has less possibility to develop HBB and RDS at birth with NPV at 94.0 and 95.2%, respectively. The high NPV could ensure the pregnant woman and attending physician that her baby has low possibilities to develop RDS and HBB within the next three months. The sensitivity of fetal IVS volume measurement was only 55 and 56% for HBB and RDS, respectively. Positive predictive values (PPV) of fetal IVS volume were very low at 21.4 and 17.9% for HBB and RDS prediction. The benefit of measuring fetal IVS volume was its high NPV, which helps ensure a low risk of the neonate developing HBB and RDS. If the fetal IVS volume exceeds the threshold of 419.8 mm3, the attending physician can be alerted to the possibility of early detection of HBB and RDS. HBB can be detected at birth through a small amount of neonatal blood testing, while RDS can only be diagnosed by close observation after birth. We suggest that fetal IVS volume measurement be performed in pregnant women with GDM during the early third trimester (29–34 weeks). The unexpected case loss might be the limitation of this study. The identical 419.8 mm3 cutoff for both HBB and RDS, with near-identical predictive metrics, might be another limitation of study from overfitting or arbitrary ROC selection that needed the more number of subjects in the next study.
In conclusion, fetal IVS volume measured during the early third trimester in pregnant women with GDM was higher than that measured in healthy pregnant women. The cut off value of fetal IVS volume from the current study was 419.8 mm3 for HBB and RDS prediction. A high NPV (94.0 and 95.2%) of fetal IVS volume was observed. We suggest that fetal IVS volume measurement be performed routinely in pregnant women with GDM during the early third trimester to help identify those at low risk for HBB and RDS or to raise early alert for their occurrence and compensation of low sensitivity of this test.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restriction.
Ethics Approval
This study was approved by the Bhumibol Adulyadej Institutional Review Board (BAIRB) (registration number 62/67). The present study was conducted in accordance with the Declaration of Helsinki. All information and data were encrypted and confidential. All participants provided informed consent. All samples were handled and processed strictly, as stipulated by an approved local review board protocol.
Author Contributions
Rachata Rachatakarn: Data procurer; data analysis; data interpretation; conception; writing; study design; review and editing. Wiyada Luangdansakul: Data procurer; investigation; data interpretation; supervision; study design. Teenat Kanjanasingh: Data procurer; data interpretation. Kornkarn Bhamarapravatana: writing; review and editing. Komsun Suwannarurk: Investigation; data interpretation; writing; supervision. All authors made substantial contributions to the design and conception of the study, and acquisition, analysis and interpretation of data, and took part in either drafting or revising the manuscript. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research was financially supported by Bhumibol Adulyadej Hospital research fund.
Disclosure
The authors declare no conflict of interest. The authors are grateful to all the patients, investigators, nurses, and colleagues who participated in this study.
References
1. Thai Department of Disease Control. Introduction. In: Thailand National Plan for the Prevention and Control of Non-Communicable Diseases (2023-2027). Bangkok: Thai Department of Disease Control; 2023:1–2.
2. Berger H, Melamed N, Davis BM, et al. Impact of diabetes, obesity and hypertension on preterm birth: population-based study. PLoS One. 2020;15:e0228743. doi:10.1371/journal.pone.0228743
3. Hay WW. Care of the infant of the diabetic mother. Curr Diab Rep. 2012;12(1):4–15. doi:10.1007/s11892-011-0243-6
4. Depha AL, De Wit L, Steenhuis TJ, et al. Effect of maternal diabetes on fetal heart function on echocardiography: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2021;57:539–550. doi:10.1002/uog.22163
5. Simone RM, Devine OJ, Marcinkevage JA, et al. Diabetes and congenital heart defects: a systematic review, meta-analysis, and modeling project. Am J Prev Med. 2015;48:195–204. doi:10.1016/j.amepre.2014.09.002
6. Lisowski LA, Verheijen PM, Copel JA, et al. Congenital heart disease in pregnancies complicated by maternal diabetes mellitus. An international clinical collaboration, literature review, and meta-analysis. Herz. 2010;35:19–26. doi:10.1007/s00059-010-3244-3
7. Han SS, Wang G, Jin Y, et al. Investigating the mechanism of hyperglycemia-induced fetal cardiac hypertrophy. PLoS One. 2015;10:e0139141. doi:10.1371/journal.pone.0139141
8. Lynch TA, Westen E, Li D, Katzman PJ, Malshe A, Drennan K. Stillbirth in women with diabetes: a retrospective analysis of fetal autopsy reports. J Matern Fetal Neonatal Med. 2022;35:2091–2098. doi:10.1080/14767058.2020.1779213
9. Bhorat I, Pillay M, Reddy T. Determination of the fetal myocardial performance index in women with gestational impaired glucose tolerance and to assess whether this parameter is a possible prognostic indicator of adverse fetal outcome. J Matern Fetal Neonatal Med. 2018;31:2019–2026. doi:10.1080/14767058.2017.1334047
10. Ye W, Luo C, Huang J, Li C, Liu Z, Liu F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022;377:e067946. doi:10.1136/bmj-2021-067946
11. Rolo LC, Santana EF, da Silva PH, et al. Fetal cardiac interventricular septum: volume assessment by 3D/4D ultrasound using spatio-temporal image correlation (STIC) and virtual organ computer-aided analysis (VOCAL). J Matern Fetal Neonatal Med. 2015;28:1388–1393. doi:10.3109/14767058.2014.955005
12. Bravo-Valenzuela NJ, Peixoto AB, Mattar R, Araujo Júnior E. Fetal interventricular septum volume evaluated by three-dimensional ultrasound using spatiotemporal image correlation and virtual organ computer-aided analysis in fetuses from pre-gestational diabetes mellitus pregnant women. J Cardiovasc Imaging. 2022;30:125–134. doi:10.4250/jcvi.2021.0170
13. Simjak P, Anderlova K, Smetanová D, Kršek M, Mráz M, Haluzík M. Glucose control during pregnancy in patients with type 1 diabetes correlates with fetal hemodynamics: a prospective longitudinal study. BMC Pregnancy Childbirth. 2024;24:264. doi:10.1186/s12884-024-06462-7
14. Söylemez E, Sağol S. Effects of gestational diabetes mellitus on fetal cardiac morphology. Med Sci. 2024;12:73.
15. Samanth J, Vasudeva A, Raghavendra SD, et al. Myocardial hypertrophy in fetuses of women with gestational diabetes. J Appl Pharm Sci. 2020;10:105–110.
16. Turgut E, Turan G, Özdemir H, Aktulum F, Bayram M, Karcaaltincaba D. Fetal cardiac morphology and geometry in pregnancies with class A1 and A2 gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2022;35:1023–1027. doi:10.1080/14767058.2022.2035712
17. Sapanont K, Luangdansakul W, Pleankong M, Smanchat B, Bhamarapravatana K, Suwannarurk K. Incidence of fetal myocardial hypertrophy in mother with diabetes mellitus by using cardio-spatiotemporal image correlation (STIC) M-mode. Int J Womens Health. 2023;15:703–710. doi:10.2147/IJWH.S410697
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.