Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Fentanyl vs fentanyl-dexmedetomidine in lumbar foraminotomy surgery
Authors Abdul Hadi B ![]() , Sbeitan SM, Shakya AK
, Sbeitan SM, Shakya AK ![]()
Received 18 November 2018
Accepted for publication 10 March 2019
Published 15 July 2019 Volume 2019:15 Pages 885—890
DOI https://doi.org/10.2147/TCRM.S195108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Bushra Abdul Hadi,1 Saleh M Sbeitan,2 Ashok K Shakya1
1Faculty of Pharmacy and Medical Sciences, Al-Ahliyya Amman University, Amman 19328, Jordan; 2Intensive Care Unit, Specialty Hospital, Amman 19328, Jordan
Aim: Lumbar foraminotomy surgery requires a potent opioid with short duration and rapid onset of action. In the present study we intended to compare the efficacy of fentanyl alone vs the combination of dexmedetomidine and fentanyl during lumbar foraminotomy surgery.
Methods: The duration and requirements for first postoperative analgesics, hemodynamic stability, and respective side effects were studied. A prospective, randomized, double blind study of 40 patients (fentanyl group [Fen group] and fentanyl-dexmedetomidine group [Fen-Dex group], n=20 each) scheduled for lumbar foraminotomy surgery under pharmaceutical care intervention was carried out. Patients were classified as class I or II, according to the American Society of Anesthesiologists physical status classification. Patients received intraoperative propofol, sevoflurane, atracurium, and either fentanyl loading dose of 1.0 μg/kg and maintenance infusion dose of 0.2 μg/kg/h in both groups. The patients of the Fen group received normal saline (0.9%) placebo, while the patients of the Fen-Dex group received dexmedetomidine infusion (0.5 μg/kg/h) along with the fentanyl infusion. Postoperative morphine doses were given. Hemodynamic stability, pain, postoperative analgesia requirement, side effects of drugs, and other effects were monitored.
Results: In the Fen-Dex group, the pain score was significantly less than in the Fen group (p<0.05). The time to first postoperative analgesia request was prolonged in the Fen-Dex group compared to the Fen group. On the other hand, requirement of morphine, and postoperative symptoms and episodes of nausea and vomiting were significantly greater in the Fen group than in the Fen-Dex group (p<0.05).
Conclusion: The present study suggests the addition of dexmedetomidine during lumbar foraminotomy surgery at different levels would be beneficial to reduce morphine consumption and any adverse drug reaction.
Keywords: dexmedetomidine, foraminotomy surgery, fentanyl, postoperative analgesics, hemodynamic stability, adverse drug reactions
Introduction
The most common therapeutic problems after surgeries are postoperative pain and nausea and vomiting side effects.1–3 In lumbar foraminotomy surgery, patients usually experience more severe postoperative pain than in other common surgeries.4 Dexmedetomidine is an active dextrorotatory isomer of medetomidine and a highly selective α2-adrenoceptor agonist5 commonly used in anesthesia and emergency care. Activation of the receptors inhibits neuronal firing causing sedation, analgesia, hypotension, and bradycardia.6 Termination of pain signals is generally controlled by pre-synaptic activation of the α2-adrenoceptor which inhibits the release of norepinephrine,7 while decrease in blood pressure (BP) and heart rate (HR) is due to the postsynaptic activation of α2-adrenoceptors in the central nervous system which inhibits sympathetic activity.8 It has analgesic, sedative, and anesthetic sparing effect along with cardiovascular stabilizing effects.9,10 It reduces sympathetic tone and attenuates the stress responses to anesthesia and surgery. It increases respiratory stability, decreases opioid need, helps with early postoperative recovery, and maintains hemodynamics by blocking sympathetic overactivity.11 In recent years, perioperative continuous dexmedetomidine infusion has been used for sedative purposes in cardiac surgery and outpatient operations, in particular those performed with local anesthesia.12 Dexmedetomidine effectively attenuated sympathomimetic stimulation during intubation, but does not completely stop the heart and cardiovascular system response.13 However, there have not been sufficient studies on the usage of continuous dexmedetomidine infusion in general anesthesia for induction and maintenance of anesthesia.
In this study, we investigated the time to first postoperative request for analgesic agent, the total morphine consumption (postoperatively), severity of postoperative pain using the visual analog scale (VAS) score, and nausea and vomiting side effects.
We carried out this study by conducting a clinical pharmacist intervention during lumbar foraminotomy surgery in different anesthetics stages.1,2,14
The formal permission for this study to be conducted was obtained from the Human Investigation Section of the Institutional Review Board of the Hospital (Specialty Hospital, Amman, Jordan), and informed consent was obtained from each patient.
Materials and methods
Adult patients up to the age of 55 years presenting for surgery in Jordan were enrolled. After obtaining written informed consent before surgery, each patient was evaluated. This study adhered to the Declaration of Helsinki guidelines. All patients were initially assessed in a systematic way for the following clinical parameters: age, gender, duration of the complaint, associated systemic conditions, and family history.
Clinical pharmacist’s role
An independent clinical pharmacist, who was just involved in the therapeutic regimen, created the experimental protocol. The pharmacist provided the patients with some information about the disease and drug use pre-, intra-, and postoperatively. They attempted to allay patients’ fears and apprehensions to minimize the consequences of the painful surgical experience, furthermore they checked patients’ wellbeing and health condition, and monitored all prescribed medication prior to the surgery, if appropriate. The clinical pharmacist investigated and recorded all the details of potential drug allergic responses and major side effects if appropriate, and analyzed the results. In addition, they instructed the patients on how to use the face pain scale.
Technique of anesthesia
To detect a reduction in VAS score of 0.82 units, which is similar to other studies with a two-sided 5% significance level and a power of 80%, a sample of 20 patients in each group was necessary, given an anticipated dropout rate of 5%. Total number of patients were 40, they were divided randomly in two groups (20 patients in each group), disregarding their gender and age. The established uniform operative procedures for the two groups who were treated by the same surgical team were carried out.15
A prospective randomized double blind study was conducted with 40 patients between the ages of 48–55 years, patients were classified as class I or II, according to the American Society of Anesthesiologists physical status classification. Patients were educated and able to use the patient-controlled analgesia technique. Patients who developed bleeding or hyper-sensitivity to any medication were excluded from the final study using current protocol. None of the patients were pre-medicated nor alcoholic. Patient data were collected and recorded before and during the operation: gender (male or female), age (years), body mass (kg), HR (beats/min), and mean arterial blood pressure (MAP) (mmHg). All patients were free of any systemic diseases after performing pre-operative test and were considered fit to be operated on. The drug history of each patient did not display any major differences between individuals and the data indicated that all patients were considered suitable for the trial. We excluded all patients with major systemic diseases, or those taking chronic narcotic analgesics.
Half an hour prior to surgery, patients of both groups received midazolam (0.25 mg/kg po) as a pre-medication. The anesthesia was induced in the operating theater using propofol (2 mg/kg) bolus intravenous (iv) injection, followed by atracurium (0.6 mg/kg) and sevoflurane/nitrous oxide mixture.
Fentanyl (1 μg/kg) bolus iv injection followed by a fentanyl infusion (0.2 μg/kg/h) was used as analgesic agent for both groups. On the other hand, the patients of the fentanyl-dexmedetomidine group (Fen-Dex) group received dexmedetomidine (loading dose of 0.5 μg/kg and maintenance dose of 0.2 μg/kg/h) infusion for the first 24 hours after surgery. The patients received normal saline as needed during surgery and postoperatively. Quantitative measurements during the operation and analgesic assessment postoperatively were carried out. All the data were collected blindly. Hemodynamic parameters were recorded for all patients (HR, as beats/min and MAP, in mmHg). The postoperative pain (during 24 hours) was recorded at the post-anesthesia care unit (PACU) using VAS.
During the first 24 hours after surgery, the severity of postoperative pain was measured by using the VAS with 0 as no pain and 10 as the highest measurable pain. Whenever the pain score was more than 4 on VAS, morphine was given intravenously in the PACU until the pain score was reduced. The morphine was given using morphine infusion pump which can deliver morphine solution at the rate of 1 mg/mL/h. The total requirement for morphine (mg) and VAS scores were monitored and signs of nausea and vomiting were documented.
Statistical analysis
Sigma Plot Version 12 and Graph Pad Version 5, were used for the statistical analyses. Values are expressed as mean ± SD or median (interquartile range) (range). Categorical data are expressed as number of patients/observations. Mann-Whitney U test (either numerical or ordinal) and the χ2 test (categorical) were used for comparison.
Results
The two experimental groups were found to be comparable in regard to gender, age, and body mass.
There were 25 lumber level 5 and sacral 1 (L 5 – S 1) patients, ten lumber level 2 and 3 (L 2 – L 3) patients, and five L 5 – S 1 and L 2 – L 3 patients, all with unilateral level and no other spinal pathology.
No statistically significant differences between the two groups (Table 1) were observed. The time to first postoperative request for analgesic agent in PACU, total morphine consumption, VAS score, MAP, and HR were observed over the first 24 hours after surgery. These parameters were significantly different between the two groups (p<0.001). The morphine requirement in the patients of Fen-Dex group was significantly reduced compared to the fentanyl group (Fen group) (p=0.001). The first request for analgesic agent during the treatment at PACU was also significantly (P=0.001) reduced. The VAS value was also significantly (P=0.001) reduced in Fen-Dex group compared to the Fen group. On the other hand, the hemodynamic measurements were satisfactory and normal, showing no significant differences between the two groups (MAP [p=0.339] and HR [p=0.767]) (Figure 1, Table 2). Patients in the Fen-Dex group experienced fewer episodes of nausea and vomiting than the patients of Fen group (Table 3). None of the patients were excluded from the study due to any complications.
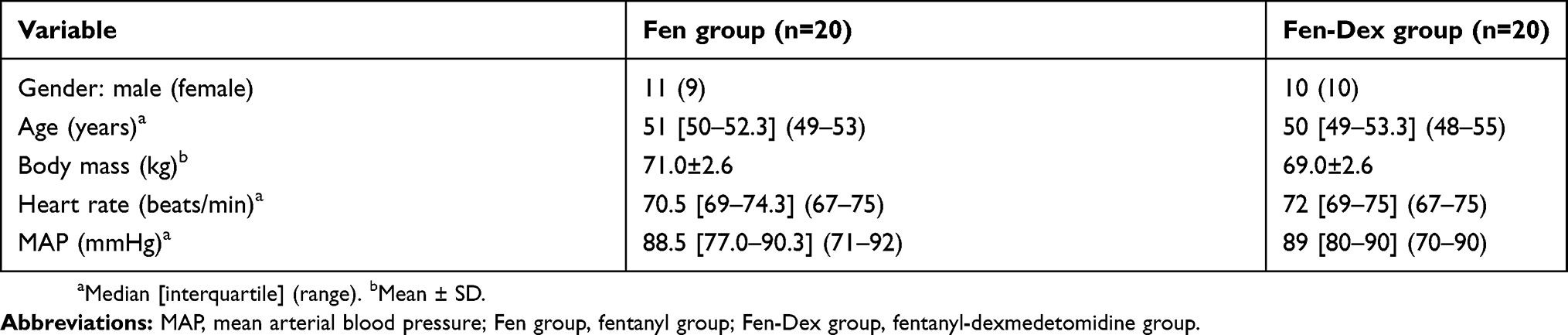 |
Table 1 Demographic parameters of groups of patients |
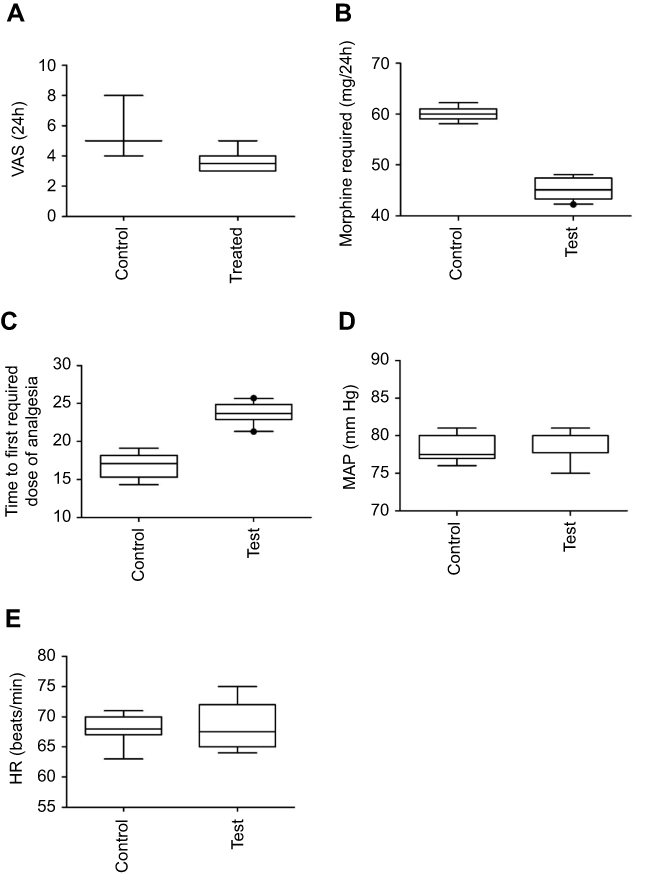 |
Figure 1 Effect of treatment (Fen [control] and Fen-Dex [test]) on: (A) visual analog scale (VAS) score (p=0.001), (B) morphine requirement (p=0.001), (C) time to first request for analgesia (minutes) (p=0.001), (D), mean arterial blood pressure (MAP) (p=0.339) and (E), heart rate (HR) (p=0.767). Abbreviations: Fen group, fentanyl group; Fen-Dex group, fentanyl-dexmedetomidine group. |
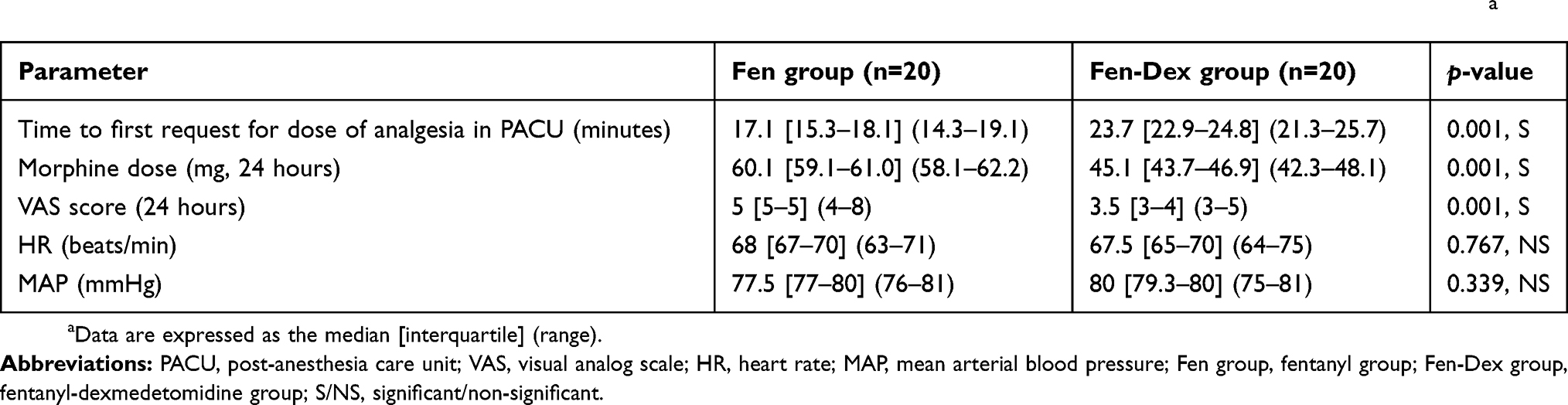 |
Table 2 Time to first request for analgesia in PACU, the cumulative requested doses of morphine, VAS score, HR, and MAPa |
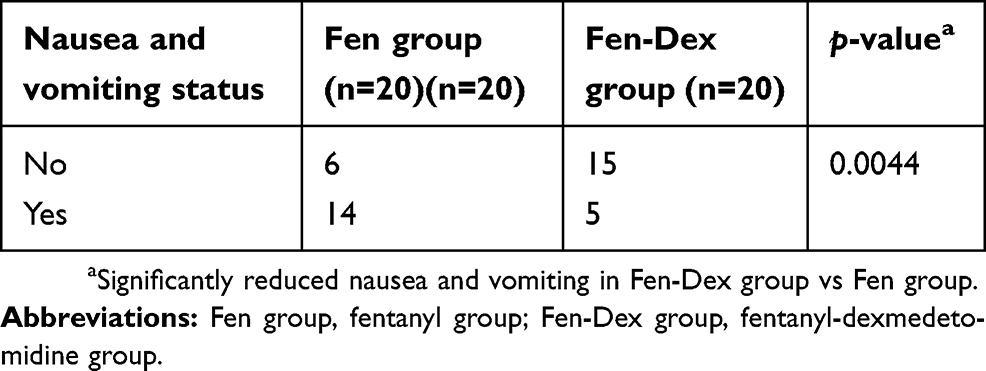 |
Table 3 Nausea and vomiting over the first 24-hour postoperative period |
Discussion
Worldwide, literature on clinical pharmacist interventions in the “operating room” is still limited. This research applied a pharmaceutical care intervention to lumbar foraminotomy surgery. Earlier studies have suggested more pharmacist intervention during surgery in conjunction with anesthesiologists.16 Newer studies have applied clinical pharmacy intervention program in the operating room.1,2
Feld et al17 have studied various alternative methods for analgesia in bariatric surgery. The results indicate that dexmedetomidine provided better hemodynamic stability preoperatively and postoperative analgesia, which accordingly reduces the use of morphine or morphine derivatives postoperatively in comparison to fentanyl. As compared to Feld et al,17 we had the same results concerning hemodynamic stability and postoperative analgesics consumption.
Hemodynamic and recovery profile of patients treated with dexmedetomidine and fentanyl in intracranial supratentorial surgeries were studied by Tripathi et al.18 Better hemodynamic control was observed with dexmedetomidine in comparison to fentanyl. A recent study was carried out by Goyal et al,19 which has confirmed that dexmedetomidine can be used as suitable alternative to fentanyl in breast cancer surgeries due to better hemodynamic stability, anesthetic sparing effects, and better recovery profile. Lehnen et al20 and Cepeda et al21 have mentioned that nausea and vomiting are the most common adverse effects of opioids during surgeries. Previous studies tested the effects of ketamine on the consumption of morphine and associated side effects like nausea and vomiting in after tonsillectomy. Their results showed a significant reduction in total morphine consumption and its side effects.2 On the other hand, opioid consumption was reduced during intraoperative period and in the PACU when dexmedetomidine was used for different surgeries.3,9,22 In the current study, dexmedetomidine in lumbar foraminotomy surgery at all levels, had the same effects on morphine consumption and side effects.
Liang et al22 indicated that dexmedetomidine showed superiority to placebo, but not to all other anesthetic agents in terms of post-anesthesia nausea and vomiting, and this efficacy may be related to a reduced consumption of intraoperative opioids. These observations were similar to the current findings. Our study showed a significant reduction in the consumption of analgesic agents in the Fen-Dex group compared to the Fen group postoperatively (Figure 1, Tables 2 and 3). Turgut et al23 have reported that patients of Fen group required additional analgesia earlier than Dex group. Dexmedetomidine can be used safely for pain reduction, which may help to reduce intraoperative opioid requirements, as it is evident from previous studies.24
Conclusion
Adding dexmedetomidine to fentanyl in lumbar foraminotomy surgery at different levels, could be a supplementary therapy to maintain hemodynamic level and ensure postoperative analgesic control whilst reducing the consumption of postoperative morphine, thereby minimizing nausea and vomiting side effects.
Interventions of clinical pharmacists have an efficient role in improving and recovering the total outcomes of lumbar foraminotomy surgery.
Acknowledgments
The authors are grateful to Prof. Dr. Ghaleb A Oriquat, Dean, Faculty of Pharmacy and Medical Sciences, and Dean, Scientific Research, Al-Ahliyya Amman University, Amman, 19328, Jordan, for providing facilities.
The authors would also like to thank Prof. Dr. Sari Hamdan, President, Al-Ahliyya Amman University, Amman, Jordan, for encouragement and constant motivation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hadi BA, Daas R, Zelko R. A randomized, controlled trial of a clinical pharmacist intervention in microdiscectomy surgery–low dose intravenous ketamine as an adjunct to standard therapy. Saudi Pharm J. 2013;21(2):169–175. doi:10.1016/j.jsps.2012.08.002
2. Hadi BA, Sbeitan SM. Clinical pharmacy intervention post tonsillectomy: a randomized control trial. Int J Clin Pharm. 2015;37(1):133–138. doi:10.1007/s11096-014-0051-6
3. Hadi BA, Sbeitan SM, Shakya AK. Dexmedetomidine infusion prevents significant postoperative pain in the first 24 hrs after myomectomy laparoscopic surgery. Acta Pol Pharm Drug Res. 2018;75(1):183–188.
4. Madhavan K, Chieng LO, McGrath L, Hofstetter CP, Wang MY. Early experience with endoscopic foraminotomy in patients with moderate degenerative deformity. Neurosurg Focus. 2016;40(2):E6. doi:10.3171/2015.11.FOCUS15511
5. Keers RN, Williams SD, Cooke J, Walsh T, Ashcroft DM. Impact of interventions designed to reduce medication administration errors in hospitals: a systematic review. Drug Saf. 2014;37(5):317–332. doi:10.1007/s40264-014-0152-0
6. Srivastava VK, Mishra A, Agrawal S, Kumar S, Sharma S, Kumar R. Comparative evaluation of dexmedetomidine and magnesium sulphate on propofol consumption, haemodynamics and postoperative recovery in spine surgery: a prospective, randomized, placebo controlled, double-blind study. Adv Pharm Bull. 2016;6(1):75–81. doi:10.15171/apb.2016.012
7. Walwyn WM, Chen W, Kim H, et al. Sustained Suppression of Hyperalgesia during Latent Sensitization by μ-, δ-, and κ-opioid receptors and α2A Adrenergic Receptors: role of Constitutive Activity. J Neurosci. 2016;36(1):204–221. doi:10.1523/JNEUROSCI.1751-15.2016
8. Özütürk B, Ersoy A, Altan A, Uygur LM. Comparison of the effects of remifentanil and dexmedetomidine infusions on hemodynamic parameters and thyroid hormones. Turk J Anaesthesiol Reanim. 2013;41(6):206–210. doi:10.5152/TJAR.2013.39
9. Kimura M, Sakai A, Sakamoto A, Suzuki H. Glial cell line‐derived neurotrophic factor‐mediated enhancement of noradrenergic descending inhibition in the locus coeruleus exerts prolonged analgesia in neuropathic pain. Br J Pharmacol. 2015;172(10):2469–2478. doi:10.1111/bph.13073
10. Naaz S, Ozair E. Dexmedetomidine in current anaesthesia practice-a review. J Clin Diagn Res. 2014;8(10):GE01–GE04.
11. Cruickshank M, Henderson L, MacLennan G, et al. Alpha-2 agonists for sedation of mechanically ventilated adults in intensive care units: a systematic review. Health Technol Assess (Rockv). 2016. doi:10.3310/hta20400
12. Chen Q, Wu W, Zhang GC, et al. Dexmedetomidine attenuates hypoxemia during palliative reconstruction of the right ventricular outflow tract in pediatric patients. Medicine. 2014;93(13):e69. doi:10.1097/MD.0000000000000069
13. Kunisawa T, Nagata O, Nagashima M, et al. Dexmedetomidine suppresses the decrease in blood pressure during anesthetic induction and blunts the cardiovascular response to tracheal intubation. J Clin Anesth. 2009;21(3):194–199. doi:10.1016/j.jclinane.2008.08.015
14. Mendes MB, Da Silva-Filho JC, Sabino CK, et al. Pharmacological evidence of α2-adrenergic receptors in the hypotensive effect of Platonia insignis mart. J Med Food. 2014;17(10):1079–1085. doi:10.1089/jmf.2013.0151
15. Sekhon L. Foraminotomy: posterior cervical, surgical technique, risks and recovery. Available from: https://www.spineuniverse.com/treatments/surgery/cervical/foraminotomy-posterior-cervical.
16. Gordon PC. Wrong drug administration errors amongst anaesthetists in a South African teaching hospital. South Afr J Anaesth Analg. 2004;10(2):7–8. doi:10.1080/22201173.2004.10872353
17. Feld JM, Hoffman WE, Stechert MM, Hoffman IW, Ananda RC. Fentanyl or dexmedetomidine combined with desflurane for bariatric surgery. J Clin Anesth. 2006;18(1):24–28. doi:10.1016/j.jclinane.2005.05.009
18. Tripathi M, Kumar V, Malviya D, Singh M, Kumar MTyagi A. Hemodynamic and recovery profile with dexmedetomidine and fentanyl in intracranial supratentorial surgeries: a comparative study. IOSR J Pharm. 2015;5(11):43–48.
19. Goyal S, Gupta KK, Mahajan V. A comparative evaluation of intravenous dexmedetomidine and fentanyl in breast cancer surgery: a prospective, randomized, and controlled trial. Anesth Essays Res. 2017;11(3):611–616. doi:10.4103/0259-1162.206860
20. Lehnen N, Heuser F, Sağlam M, et al. Opioid-induced nausea involves a vestibular problem preventable by head-rest. PLoS One. 2015;10(8):e0135263. doi:10.1371/journal.pone.0135263
21. Cepeda MS, Farrar JT, Baumgarten M, Boston R, Carr DB, Strom BL. Side effects of opioids during short‐term administration: effect of age, gender, and race. Clin Pharmacol Ther. 2003;74(2):102–112. doi:10.1016/S0009-9236(03)00152-8
22. Liang X, Zhou M, Feng JJ, et al. Efficacy of dexmedetomidine on postoperative nausea and vomiting: a meta-analysis of randomized controlled trials. Int J Clin Exp Med. 2015;8(6):8450–8471.
23. Turgut N, Turkmen A, Gokkaya S, Altan A, Hatiboglu MA. Dexmedetomidine-based versus fentanyl-based total intravenous anesthesia for lumbar laminectomy. Minerva Anestesiol. 2008;74(9):469–474.
24. Shukla U, Prabhakar T, Malhotra K, Srivastava D. Dexmedetomidine versus midazolam as adjuvants to intrathecal bupivacaine: a clinical comparison. J Anaesthesiol Clin Pharmacol. 2016;32(2):214–219. doi:10.4103/0970-9185.182105
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.