Back to Journals » International Medical Case Reports Journal » Volume 19
Fentanyl-Induced Chest Wall Rigidity Causing Recurrent Ventilator Dyssynchrony in the Intensive Care Unit: A Case Report
Authors Hussein AM ![]() , Yusuf FY
, Yusuf FY ![]()
Received 8 January 2026
Accepted for publication 4 March 2026
Published 9 March 2026 Volume 2026:19 590626
DOI https://doi.org/10.2147/IMCRJ.S590626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Abdiwali Mohamed Hussein,1 Fathi Yasin Yusuf1,2
1Department of ICU, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia; 2Faculty of Medicine and Health Science SIMAD University, Mogadishu, Somalia
Correspondence: Abdiwali Mohamed Hussein, Email [email protected]
Background: Fentanyl-induced chest wall rigidity represents an important and often overlooked cause of ventilator dyssynchrony in mechanically ventilated patients. Its clinical presentation overlaps with bronchospasm and ventilator malfunction which delays diagnosis and appropriate management.
Case Presentation: A 75-year-old male, mechanically ventilated with pneumonia and asthma exacerbation developed ventilator desynchrony, characterized by sudden-onset hypercarbia, decreased lung compliance, and episodic breath-holding. Escalation of bronchodilators, corticosteroids, and sedation failed to improve ventilation. Recurrent episodes of poor ventilation responded only transiently to neuromuscular blockade. After exclusion of dynamic hyperinflation, pneumothorax, and progression of pneumonia; fentanyl-induced chest wall rigidity was suspected. Reduction of the fentanyl infusion resulted in improved lung compliance and resolution of desaturation episodes.
Conclusion: While fentanyl remains a valuable for pain management in the ICU, this case highlights fentanyl-induced chest wall rigidity as a reversible cause of refractory ventilator dyssynchrony that should be suspected when sudden reductions in lung compliance and ineffective ventilation occur without identifiable pulmonary or mechanical causes, particularly in patients receiving continuous opioid infusions. Early recognition and opioid adjustment restore effective ventilation and prevent unnecessary diagnostic or therapeutic interventions.
Keywords: fentanyl, chest wall rigidity, ventilator dyssynchrony, Intensive care unit, Somalia
Introduction
Fentanyl is widely used in intensive care units (ICUs) for analgesia and sedation due to its rapid onset, potent analgesic effect, and hemodynamic stability. Although its common adverse effects are well described, including respiratory depression, bradycardia and hypotension. Fentanyl rarely causes chest wall rigidity, leading to acute ventilatory compromise. While historically described in anesthesia and perioperative settings, this complication remains underrecognized in routine ICU practice.1,2
Chest wall rigidity has been reported after rapid administration or high cumulative doses of fentanyl, particularly in operative and postoperative settings3 However, studies suggest that this complication is not limited to high doses alone. Several case reports have demonstrated that chest wall rigidity occurred following low doses and intermittent bolus administration.3,4 Because its clinical presentation overlaps with more common causes of respiratory deterioration in the ICU and lacks objective diagnostic criteria, fentanyl-induced chest wall rigidity is often diagnosed late.
No previous case reports from Somalia have described fentanyl-induced chest wall rigidity, despite widespread fentanyl use in intensive care units. We present a case of fentanyl-induced chest wall rigidity occurring during routine ICU, emphasizing the diagnostic challenge and the importance of early recognition of this reversible complication.
Case Report
A 75-year-old man presented with a 5-days history of fever, productive cough with purulent sputum, and progressive dyspnea. His medical history included bronchial asthma, hypertension, type 2 diabetes mellitus, and prior ischemic stroke. On admission, his vital signs were: temperature 37.8°C, heart rate 96 beats/min, blood pressure 138/82 mmHg, respiratory rate 26 breaths/min, and oxygen saturation (SpO2) 88% on room air, improving to 94% on 5 L/min oxygen via nasal cannula. Chest auscultation revealed bilateral coarse crackles without wheezing.
Initial arterial blood gas (ABG) analysis on supplemental oxygen showed: pH: 7.34, PaCO2: 48 mmHg, PaO2: 72 mmHg and HCO3−: 25 mmol/L. Despite treatment with intravenous antibiotics, bronchodilators, and corticosteroids, the patient developed worsening respiratory distress with SpO2 declining to 85% on FiO2 0.5 via face mask and progressive hypercapnia (PaCO2 55 mmHg), necessitating endotracheal intubation and ICU admission.
Mechanical ventilation was initiated using volume-controlled mode with the following settings: Tidal volume: 480 mL (8 mL/kg predicted body weight), Respiratory rate: 16 breaths/min, FiO2: 50%, PEEP: 5 cm H2O, Peak airway pressure was 22 cm H2O and plateau pressure was 18 cm H2O. Sedation and analgesia were maintained using: Midazolam infusion: 4 mg/h, and Fentanyl infusion: 30 µg/h. ABG analysis following stabilization showed: pH: 7.36, PaCO2: 42 mmHg, PaO2: 92 mmHg and SpO2: 97%. Serial arterial blood gas measurements throughout the ICU course are summarized in Table 1. The patient showed progressive improvement in oxygenation and ventilation. Sedation was discontinued on ICU Day 3, and he was successfully extubated on day 5. He was transitioned to noninvasive ventilation with SpO2 maintained at 95% on FiO2 0.4.
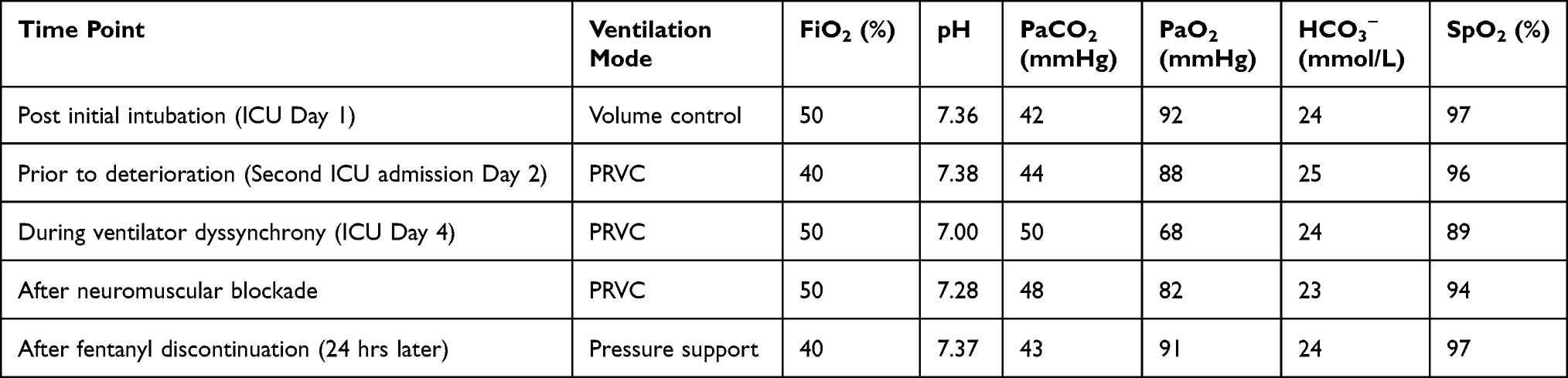 |
Table 1 Serial Arterial Blood Gas Analysis During ICU Course |
Seven days later, the patient developed progressive respiratory fatigue and hypercapnia, with SpO2 declining to 88% on noninvasive ventilation and ABG showing: pH: 7.31, PaCO2: 58 mmHg and PaO2: 68 mmHg. He was reintubated and readmitted to the ICU. Mechanical ventilation was initiated using pressure-regulated volume control mode: Tidal volume: 450 mL, Respiratory rate: 18 breaths/min, FiO2: 50%, and PEEP: 5 cm H2O. Peak airway pressure was 24 cm H2O and plateau pressure was 19 cm H2O. Sedation and analgesia were provided using: Fentanyl infusion: 30 µg/h and Ketamine infusion: 40 mg/h. ABG analysis showed: pH: 7.38, PaCO2: 44 mmHg, PaO2: 88 mmHg, and SpO2: 96%.
On ICU Day 4, increasing agitation required escalation of sedation: Fentanyl infusion increased to 80–90 µg/h and Ketamine infusion increased to 100 mg/h. The timeline of sedation, analgesia, and neuromuscular blockade during the ICU course is summarized in Table 2. Within hours of fentanyl dose escalation, the patient developed severe ventilator dyssynchrony characterized by breath-holding, paradoxical respiratory effort, and reduced chest wall movement. Ventilator parameters demonstrated: Tidal volume: 55–95 mL, Peak airway pressure: >45 cm H2O, Plateau pressure: 13–22 cm H2O, Minute ventilation: 2.0–2.5 L/min, and SpO2 declined to 89% despite FiO2 0.5. Detailed ventilator parameters during key clinical events are presented in Table 3. ABG analysis revealed severe respiratory acidosis: pH: 7.00, PaCO2: 50 mmHg, PaO2: 68 mmHg, and SpO2: 89%. Vital signs during deterioration were: Heart rate: 110 beats/min, Blood pressure: 148/86 mmHg and Respiratory rate (ventilator): 22 breaths/min. Changes in vital signs during key clinical events are summarized in Table 4.
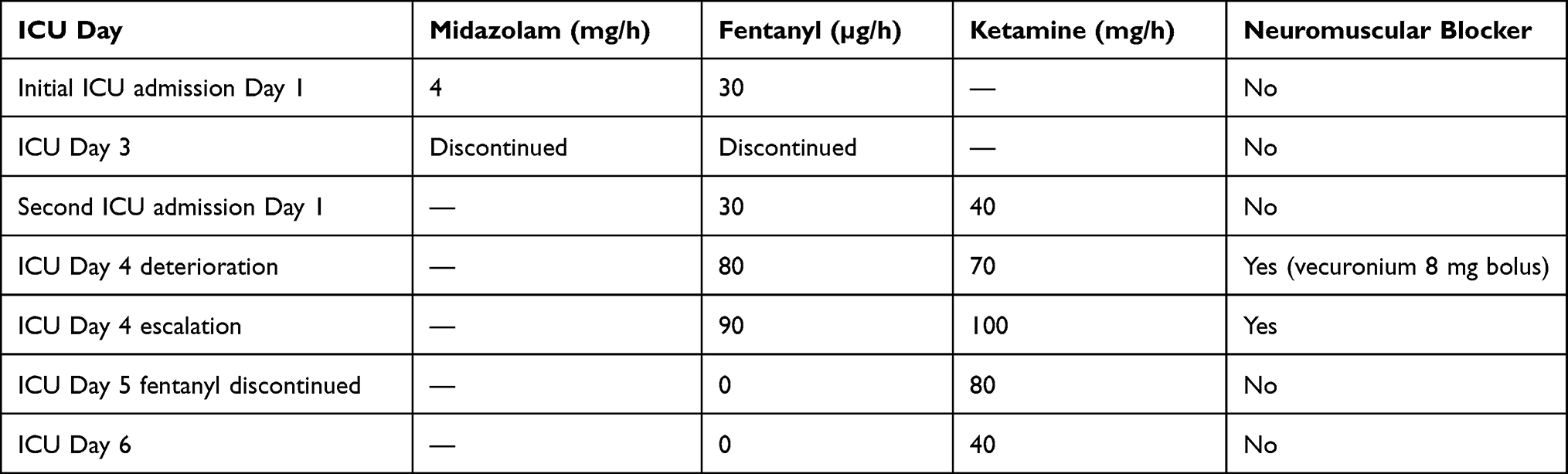 |
Table 2 Sedation and Analgesia Timeline |
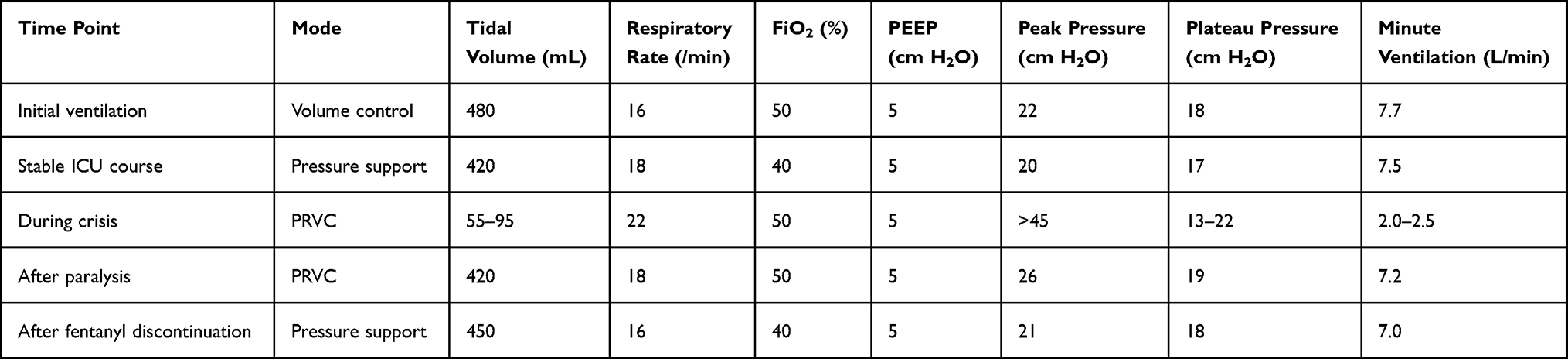 |
Table 3 Ventilator Parameters During Critical Events |
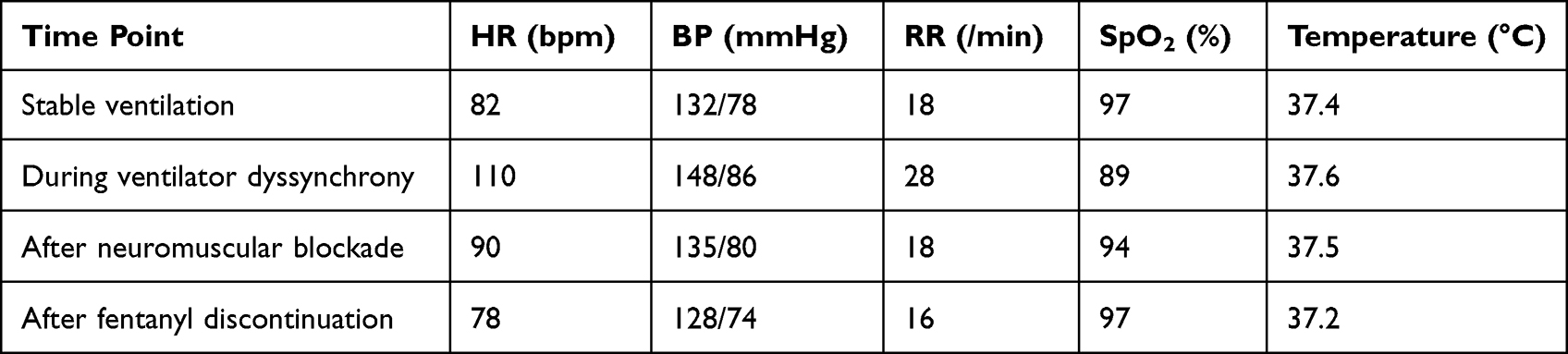 |
Table 4 Vital Signs During Key Events |
Endotracheal tube obstruction was excluded by direct inspection and suctioning. Chest radiography showed no pneumothorax, atelectasis, or progression of pneumonia. Auscultation revealed no wheezing. Bronchodilator therapy produced no improvement. Ventilator malfunction was excluded by replacing the ventilator without improvement in tidal volume or airway pressure. The differential diagnoses considered and the evaluations performed to exclude them are summarized in Table 5. Neurological causes were excluded by normal brain magnetic resonance imaging. Administration of intravenous neuromuscular blockade (vecuronium 8 mg bolus) resulted in immediate normalization of ventilatory parameters: Tidal volume increased to 420 mL; Peak airway pressure decreased to 26 cm H2O and SpO2 improved to 94%.
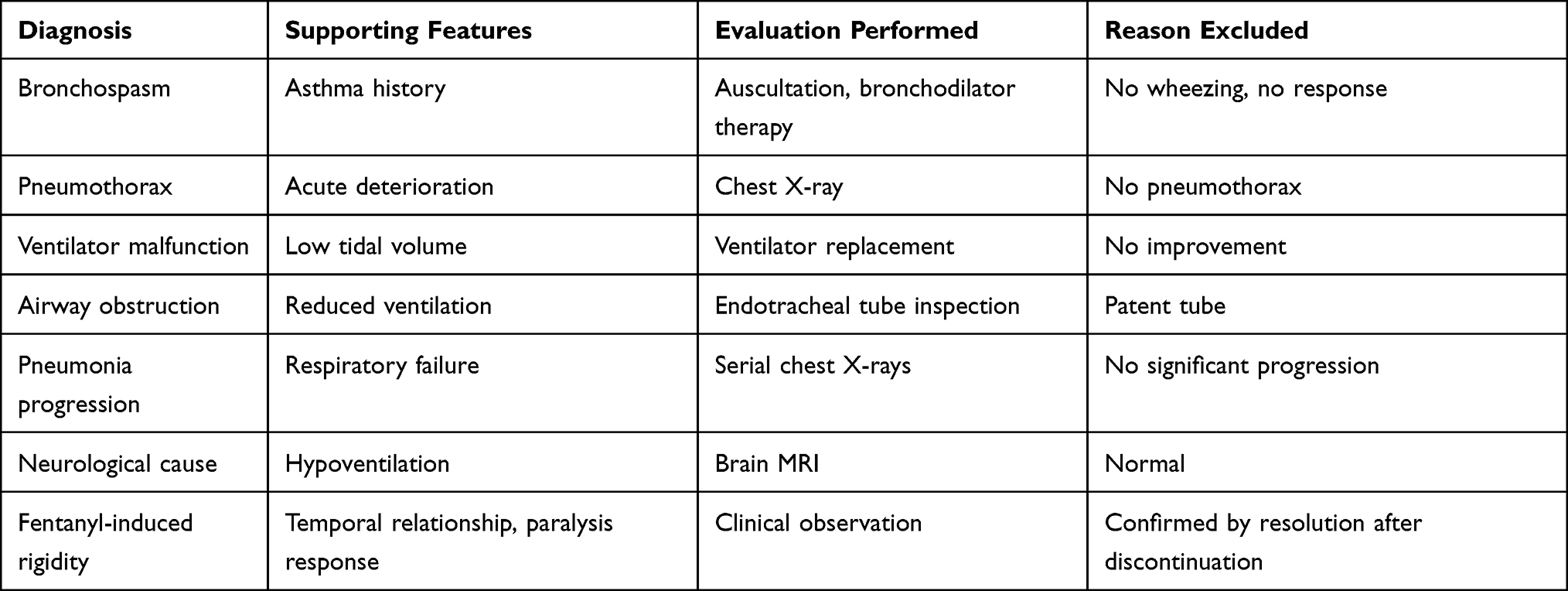 |
Table 5 Differential Diagnosis and Exclusion |
Based on the temporal relationship between fentanyl dose escalation and ventilatory dyssynchrony, preserved plateau pressure, and immediate response to neuromuscular blockade, fentanyl-induced chest wall rigidity was suspected. Fentanyl infusion was discontinued while ketamine infusion was continued at 80 mg/h. Within 24 hours, ventilatory function normalized: Tidal volume: 450 mL, Peak airway pressure: 21 cm H2O, and SpO2: 97%. ABG showed: pH: 7.37, PaCO2: 43 mmHg and no further episodes of ventilator dyssynchrony occurred.
The patient was successfully transitioned to pressure support ventilation and subsequently weaned from mechanical ventilation. He was eventually liberated from ventilatory support and discharged from the ICU in stable condition on day 10.
Discussion
Opioid-induced chest wall rigidity, commonly referred to as wooden chest syndrome (WCS), is a rare but clinically significant adverse effect of potent synthetic opioids, particularly fentanyl. The phenomenon was first described in the mid-twentieth century in the context of opioid-related respiratory depression and has since been reported predominantly during anesthetic induction with rapid intravenous administration of high-dose opioids.5,6 In contrast, occurrence during continuous sedation in mechanically ventilated intensive care unit (ICU) patients remains uncommon and under-recognized.7–9 This case highlights recurrent ventilator dyssynchrony attributable to fentanyl-induced chest wall rigidity during ICU management, emphasizing the importance of early recognition in critically ill patients.
The proposed mechanism involves central activation of μ-opioid receptors within the central nervous system. Experimental data suggest that stimulation of these receptors modulates dopaminergic transmission within the basal ganglia and related extrapyramidal pathways, resulting in increased skeletal muscle tone. Fentanyl’s high lipophilicity facilitates rapid penetration across the blood–brain barrier, leading to pronounced central effects. Increased rigidity of thoracic and abdominal musculature reduces chest wall compliance and increases elastance, thereby impairing both spontaneous and assisted ventilation. Laryngeal muscle involvement may further contribute to airflow limitation. In mechanically ventilated patients, these changes manifest as elevated peak inspiratory pressures, ventilator dyssynchrony, and difficulty with manual ventilation despite an otherwise patent airway. The rapid onset of dyssynchrony following fentanyl titration in this case supports a pharmacologically mediated mechanism.9,10
In ventilated ICU patients, elevated peak airway pressures and dyssynchrony require immediate evaluation for life-threatening causes. Differential diagnoses include pneumothorax, mucus plugging, bronchospasm, endotracheal tube obstruction, ventilator circuit malfunction, and progression of underlying acute respiratory distress syndrome. In this case, mechanical and pulmonary causes were excluded through appropriate imaging, airway suctioning, and ventilator assessment.11 The temporal association between fentanyl dose escalation and onset of dyssynchrony, coupled with resolution following fentanyl reduction, supports a causal relationship. The absence of new radiographic abnormalities and the rapid improvement in ventilator synchrony after dose adjustment further strengthen this inference.
Unlike typical anesthesia-related presentations characterized by visible generalized rigidity, intubated ICU patients may not exhibit overt extremity stiffness or jaw clenching. Instead, the primary manifestation includes unexplained ventilator dyssynchrony with preserved airway patency. Recognition in this setting therefore requires heightened clinical suspicion, particularly when conventional causes of elevated airway pressures are excluded.
Management strategies for opioid-induced chest wall rigidity include administration of naloxone, neuromuscular blockade, and discontinuation or reduction of the offending agent. Naloxone produces rapid reversal through competitive antagonism at opioid receptors but may precipitate acute withdrawal and sympathetic activation in opioid-dependent or critically ill patients. Neuromuscular blocking agents effectively reduce skeletal muscle tone and facilitate ventilation but necessitate continued mechanical ventilation and deep sedation.12 In this case, gradual titration of fentanyl with transition to alternative sedative agents resulted in sustained resolution of dyssynchrony without need for prolonged paralysis. Selection of alternative analgesic and sedative regimens should consider hemodynamic stability, organ function, and ongoing ventilatory requirements.
In a Somalia, where access to advanced monitoring, continuous neuromuscular blockade, or sophisticated ventilator analytics are limited, this case has several practical implications. First, clinicians should regard unexplained rises in Ppeak with stable Pplat, new rigidity on examination, and temporal association with fentanyl (or similar synthetic opioids) as sufficient to presume WCS once structural causes have been reasonably excluded, even without bronchoscopy or advanced imaging. Second, early, protocolized steps—stop the opioid, administer naloxone if available, switch to pressure-controlled ventilation. Third, in settings where naloxone supply is constrained, understanding fentanyl’s context-sensitive half-life can guide decisions about whether to prioritize opioid cessation and supportive ventilation alone versus using scarce naloxone for rapid reversal, particularly in patients with limited physiological reserve. Fourth, preventive strategies including avoiding large initial boluses; using the lowest effective infusion rate; and incorporating multimodal analgesia (paracetamol, regional techniques, low-dose ketamine).
Fentanyl-induced chest wall rigidity should be considered in mechanically ventilated ICU patients who develop unexplained ventilator dyssynchrony and elevated airway pressures following opioid administration. Prompt recognition and targeted management, including dose reduction or alternative sedation strategies, lead to clinical improvement and prevent avoidable complications. Increased awareness among critical care clinicians is essential to reduce morbidity associated with this rare but reversible adverse effect.
This report has limitations. Objective measurements of chest wall compliance were not obtained, and electromyographic confirmation of skeletal muscle rigidity was not performed. Serum fentanyl concentrations were not measured. As a single case report, findings are hypothesis-generating rather than definitive. Nonetheless, the consistent temporal relationship between fentanyl exposure and ventilator dyssynchrony, along with reproducible clinical improvement after dose reduction, provides supportive evidence for causality.
Conclusions
Fentanyl-induced chest wall rigidity is an uncommon but clinically significant cause of ventilator dyssynchrony in mechanically ventilated ICU patients. Recognition requires high clinical suspicion, particularly when conventional causes of elevated airway pressures are excluded. Early identification and targeted management such as opioid-dose adjustment, use of alternative sedatives, or selective neuromuscular blockade restores ventilator synchrony and prevent complications. Awareness of this phenomenon is essential for critical care clinicians to ensure safe and effective sedation in the ICU.
Abbreviations
ICU, Intensive care unit; WCS, wooden chest syndrome; NIV, Noninvasive ventilation; PH, potential of hydrogen; PCO2, partial pressure of carbon dioxide; PEEP, Positive End-Expiratory Pressure; FiO2, Fraction of Inspired Oxygen; PaO2, Partial Pressure of Oxygen in Arterial Blood; SpO2, Peripheral Capillary Oxygen Saturation; cm H2O, Centimeters of Water (unit of pressure).
Data Sharing Statement
The data supporting the findings of this case report are available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
In our institution, ethical approval is not required for case reports.
Consent for Publication
A written consent form was obtained from the patient for publication of this case report.
Acknowledgments
We express our sincere gratitude and deep appreciation to the Center of Research and Development, SIMAD University, for their guidance and recommendations.
Funding
The authors received institutional support from SIMAD University, Mogadishu, Somalia.
Disclosure
The authors declare no conflicts of interest in this case report.
References
1. Trujillo C, Rudd D, Ogutcu H, et al. Objective characterization of opiate-induced chest wall rigidity. Cureus. 2020;12(6). doi:10.7759/cureus.8459
2. Devarashetty S, Arty F, Vangala A, Shanab AA, Du D. The silent threat of wooden chest syndrome: prompt management of fentanyl-induced muscle rigidity in the intensive care unit. Eur J Case Rep Intern Med. 2025;12(8). doi:10.12890/2025_005363
3. Ham SY, Lee BR, Ha T, Kim J, Na S. Recurrent desaturation events due to opioid-induced chest wall rigidity after low dose fentanyl administration. Korean J Crit Care Med. 2016;31(2):118–6. doi:10.4266/kjccm.2016.31.2.118
4. Fukasawa R, Oishi A, Nemoto C, Inoue S. A case of opioid-induced rigidity requiring naloxone administration at the time of anesthesia emergence. JA Clin Rep. 2024;10(1):47. doi:10.1186/s40981-024-00732-1
5. Hamilton WK, Cullen SC. Effect of levalloephan taetrate upon opiate induced respiratory depression. Anesthesiology. 1953;14(6):550–554. doi:10.1097/00000542-195311000-00002
6. Comstock M, Carter JG, Moyers JR, Stevens W. Rigidity and hypercarbia associated with high dose fentanyl induction of anesthesia. Anesthesia Analg. 1981;60(5):362–363. doi:10.1213/00000539-198105000-00018
7. Abrams JT, Horrow JC, Bennett JA, Van Riper DF, Storella RJ. Upper airway closure: a primary source of difficult ventilation with sufentanil induction of anesthesia. Surv Anesthesiol. 1997;41(3):146. doi:10.1097/00132586-199706000-00015
8. Bennett JA, Abrams JT, Van Riper DF, Horrow JC. Difficult or impossible ventilation after sufentanil-induced anesthesia is caused primarily by vocal cord closure. Anesthesiology. 1997;87(5):1070–1074. doi:10.1097/00000542-199711000-00010
9. Ming PW, Singh DL. Fentanyl-induced chest wall rigidity as a cause of acute respiratory failure in the intensive care unit. J Med Cases. 2019;10(8):249. doi:10.14740/jmc3351
10. Vankova ME, Weinger MB, Chen D-Y, Bronson JB, Motis V, Koob GF. Role central mu, delta-1, and kappa-1 opioid receptors in opioid-induced muscle rigidity in the rat. Anesthesiology. 1996;85(3):574–583. doi:10.1097/00000542-199609000-00017
11. Çoruh B, Tonelli MR, Park DR. Fentanyl-induced chest wall rigidity. Chest. 2013;143(4):1145–1146. doi:10.1378/chest.12-2131
12. Pasternak GW. Opiate pharmacology and relief of pain. J clin oncol. 2014;32(16):1655–1661. doi:10.1200/JCO.2013.53.1079
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.