Back to Journals » Clinical Ophthalmology » Volume 20
Femtosecond Laser-Assisted Cataract Surgery versus Conventional Phacoemulsification Combined with Vitrectomy for Cataract Complicated with Fundus Disease: Superior Efficacy in Patients with Vitreous Opacity and Cost-Effectiveness Analysis
Authors Yang J, Zhang Z, Fan H, Xie X, Ye B, Wu Y ![]() , Li W
, Li W
Received 25 November 2025
Accepted for publication 3 February 2026
Published 14 February 2026 Volume 2026:20 584215
DOI https://doi.org/10.2147/OPTH.S584215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Jiasong Yang,1– 3 Zhikun Zhang,4 Hua Fan,1,5,6 Xiaolin Xie,2,3 Bo Ye,7 Yajun Wu,1,7,8 Wensheng Li1– 3
1Aier Academy of Ophthalmology, Central South University, Changsha, Hunan, People’s Republic of China; 2Shanghai Aier Eye Hospital, Aier Eye Hospital Group, Shanghai, People’s Republic of China; 3Shanghai Aier Eye Institute, Aier Eye Hospital Group, Shanghai, People’s Republic of China; 4Integrated Traditional Chinese and Western Medicine, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China; 5Aier Eye Hospital, Jinan University, Guangzhou, Guangdong, People’s Republic of China; 6Shanxi Aier Eye Hospital, Aier Eye Hospital Group, Taiyuan, Shanxi, People’s Republic of China; 7Nanchang Aier Eye Hospital, Aier Eye Hospital Group, Nanchang, Jiangxi, People’s Republic of China; 8Hunan Aier Eye Research Institute, Aier Eye Hospital Group, Changsha, Hunan, People’s Republic of China
Correspondence: Yajun Wu, Nanchang Aier Eye Hospital, Aier Eye Hospital Group, No. 68, Jiefang West Road, Xihu District, Nanchang, Jiangxi, 330002, People’s Republic of China, Email [email protected] Wensheng Li, Aier Academy of Ophthalmology, Central South University, 435 Furong South Road, Tianxin District, Changsha, Hunan, 410015, People’s Republic of China, Email [email protected]
Aim: To compare the efficacy of femtosecond laser assisted cataract surgery (FLACS) combined with pars plana vitrectomy (PPV) and conventional phacoemulsification surgery (CPS) combined with PPV in the treatment of cataract patients with fundus diseases.
Methods: A retrospective analysis was conducted on 379 affected eyes from Shanghai Aier Eye Hospital from 01/02/2022 to 01/02/2025, divided into group A (n=182, 48%, FLACS+PPV) and group B (n=197, 52%, CPS+PPV), to compare surgical costs, best corrected visual acuity (BCVA), complications, and surgical time.
Results: Postoperative visual acuity improved significantly in both groups (all P < 0.0001). For vitreous opacity (VO) patients, the BCVA improvement in group A (0.34± 0.51) was significantly better than that in group B (0.15± 0.52, P=0.03), with a shorter surgical time (45.22± 8.15 vs 52.72± 7.17 min, P < 0.0001) and lower complication rate (7.14% vs 11.68%). Overall, group A had a shorter surgical time (47.75± 10.06 vs 59.22± 11.6 min, P < 0.0001) and better postoperative BCVA (0.36± 0.45 vs 0.49± 0.48, P=0.0001) than group B, but higher surgical costs (21,600± 9180 vs 15,399± 2996 yuan, P < 0.0001).
Conclusion: FLACS+PPV has excellent therapeutic effects but is expensive, while CPS+PPV has a high cost-effectiveness, and clinical selection should be based on the patient’s condition.
Keywords: femtosecond laser-assisted cataract surgery, conventional phacoemulsification surgery, pars plana vitrectomy, fundus diseases, cataract
Introduction
Cataracts and retinal diseases (eg, age-related macular degeneration [AMD], diabetic retinopathy) are leading causes of severe visual impairment. A meta-analysis reported 237 million people with moderate-to-severe visual impairment globally in 2020, including 57.1 million with cataracts, 8.8–32.1 million with AMD, and 3.2–12.9 million with diabetic retinopathy,1 all requiring surgical intervention for conditions such as non-absorbable vitreous opacity (VO), macular membrane, or retinal detachment (RD).
Conventional phacoemulsification surgery (CPS) combined with intraocular lens implantation (IOL) is a standard treatment for cataracts,2–4 while pars plana vitrectomy (PPV) is pivotal for the management of retinal diseases.5–7 Sequential surgeries for patients with concurrent cataracts and retinal diseases are problematic: prior PPV is hindered by cataract opacity and increases the subsequent risk of cataract development,8 whereas prior cataract surgery leaves visual impairment caused by vitreous opacity, necessitating repeated PPV. Therefore, combined cataract-PPV has become a standard approach, which avoids the need for additional ocular surgery in the short term, reduces the risks of corneal incisions, endophthalmitis, and intraocular pressure fluctuations, shortens postoperative recovery time, and saves medical costs—particularly benefiting elderly patients with systemic diseases (eg, diabetes, hypertension).9–11
Nowadays, CPS+PPV is the most common traditional combined procedure, while femtosecond laser-assisted cataract surgery (FLACS) represents a key advancement. Gómez-Resa M et al12 first validated FLACS+23g PPV safety and efficacy in 21 eyes with concurrent fundus diseases in 2014. Unlike CPS— which relies on manual corneal incisions, capsulorhexis, and ultrasonic lens emulsification—FLACS uses computer-guided laser for precise anterior capsulotomy, lens nucleus fragmentation, and corneal incisions. This reduces phacoemulsification energy use, minimizes surgical trauma, and enhances reproducibility.13,14 In contrast, CPS is dependent on surgeon experience, with higher variability in capsulorhexis quality and greater reliance on ultrasonic energy that may increase endothelial cell loss. Clinically, FLACS offers potential advantages of shorter surgical time and fewer complications, but its high equipment and consumable costs limit widespread adoption compared to the cost-effective CPS. Notably, despite its higher cost, FLACS remains a superior choice for patients with specific needs and high clinical expectations—such as those requiring maximally precise surgical manipulation, minimizing intraoperative trauma, or pursuing optimal visual and refractive outcomes.
Despite these technical and practical differences, large-sample comparative studies between FLACS+PPV and CPS+PPV remain scarce. This study aims to provide comprehensive clinical evidence by comparing the two approaches in terms of surgical cost, visual acuity improvement, complications, and duration—supporting individualized clinical decision-making for patients with cataract complicated by fundus diseases.
Method
Ethics
This study adheres to the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai Aier Eye Hospital (approval number: SHAIER2025YN011). A waiver of informed consent for retrospective data analysis was granted: the raw data contains only de-identified clinical records, with no personal identifiers. All patients provided informed consent for their surgical procedures, and data privacy was protected per institutional guidelines.
General Information and Methods
We conducted a systematic retrospective search in the hospital information system from 01/03/2025 to 01/04/2025[This search period was set to ensure complete collection of clinical data (including preoperative examinations, surgical records, and postoperative follow-up data) for all eligible patients]. At first, we conducted a retrospective review of the hospital information system and initially identified 403 patients who underwent combined cataract + PPV surgery at our hospital from 01/02/2022 to 01/02/2025 (187 for FLACS+PPV, 216 for CPS+PPV). To ensure data reliability, we prioritized patients with complete clinical data (preoperative examinations, surgical records, postoperative follow-up). A total of 24 patients (6.0% of initial 403) were excluded due to incomplete postoperative follow-up, resulting in a final sample of 379 patients (182 FLACS+PPV, 197 CPS+PPV). No data imputation was performed.
Inclusion Criteria
1. Patients diagnosed with both cataract (slit-lamp examination showing lens opacity affecting visual function) and vitreoretinal diseases requiring simple PPV. Specific diseases include:VO: Confirmed by fundus examination and optical coherence tomography (OCT), showing non-absorbable vitreous opacities that impair fundus observation;Macular epiretinal membrane (ERM): Diagnosed by OCT as membrane formation on the retinal surface with or without retinal thickening;Other fundus diseases: Rhegmatogenous retinal detachment (RRD), proliferative diabetic retinopathy (PDR), macular hole (MH), retinal vein occlusion (RVO), vitreomacular traction syndrome (VMTS), vitreous hemorrhage (VH), myopic foveoschisis (MF), lens dislocation (LD), uveitis, and Retinal Periphlebitis (Eales), all diagnosed by fundus examination and/or OCT. 2. Patients eligible for one-stage combined IOL (simultaneous IOL implantation during combined FLACS/CPS and PPV surgery, with no contraindications to IOL implantation). 3. Patients in good general condition who can tolerate the combined surgery. 4. Patients with no history of ocular trauma or previous ophthalmic surgeries (including cataract surgery, vitrectomy, glaucoma surgery, etc).
Exclusion Criteria
1. Patients with a history of ophthalmic surgeries that may affect the study outcomes, such as previous cataract surgery, vitrectomy, corneal transplantation, or glaucoma filtering surgery. 2. Patients with severe systemic diseases unable to tolerate surgery:Uncontrolled diabetes mellitus: Glycated hemoglobin (HbA1c) ≥8.0% for more than 3 months despite medical treatment;Uncontrolled hypertension: Persistent systolic blood pressure ≥160 mmHg or diastolic blood pressure ≥100 mmHg after medication;Other severe systemic diseases (eg, end-stage renal disease, advanced heart failure, malignant tumors) that may increase surgical risk or affect postoperative recovery. 3. Patients with severe fundus lesions requiring silicone oil tamponade: Including large-area RRD involving the macula, proliferative vitreoretinopathy (PVR) grade C or above, or other retinal diseases requiring silicone oil tamponade for retinal reattachment. 4. Patients unable to undergo one-stage IOL implantation due to anatomical abnormalities (eg, insufficient capsular support, severe ocular hypotony) or patient refusal.
Note: Age was not a predefined inclusion or exclusion criterion; all patients meeting the above criteria were included.
All patients undergo necessary general examinations and detailed eye examinations before and after the operation. Ocular examination includes best corrected visual acuity (BCVA), spherical equivalent (SE), IOP, slit lamp examination, axial length (AL), corneal topography, fundus examination and OCT.
Surgical Technique
FLACS Combined with PPV Group (Group A)
All patients underwent femtosecond laser assisted cataract surgery (LenSx laser, Alcon, TX, USA; catalysts, Abbott Medical Optics Inc., CA, USA). Femtosecond laser is used for anterior capsulotomy and lens nucleus fragmentation. The diameter of the anterior capsulotomy is 5.1mm, and the lens is pre split into 4 equal parts or 6 equal parts. The main incision of cataract surgery is handmade with a 2.2 mm corneal scalpel, and the side incision is made with a 15 degree side scalpel. All patients underwent transparent corneal incision. PPV was performed with 25 gauge vitrectomy machine (Alcon constellation vision system, Fort Worth, TX, USA) and Volk wide-angle lens or rest (Carl Zeiss meditec AG, Germany) wide-angle observation system.
Phacoemulsification Combined with PPV Group (Group B)
Patients in group B received phacovitrectomy surgery, including standard phacoemulsification cataract surgery, followed by three channel vitrectomy. The instruments and techniques used were the same as those of group A, but without femtosecond laser assistance.
Postoperative Results and Complications
Intraoperative and postoperative complications were recorded. The operation time, complications and results were recorded in detail. The main complications were endophthalmitis and RD. The best corrected visual acuity, intraocular pressure, refractive status and fundus of the patients were evaluated three months after surgery.
Cost Analysis
The materials and intraocular lens types used in the operation were recorded, and the operation costs were recorded. Analyze the cost-effectiveness of patients.
Statistical Analysis
Statistical analysis was performed using SPSS 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) and compared using independent samples t-test (for normally distributed data) or Wilcoxon test (for non-normally distributed data). Categorical variables were compared using the chi-square test. Normality was tested via the Shapiro–Wilk test, and homogeneity of variance was assessed with Levene’s test—Welch’s method was used for data violating variance homogeneity. Paired t-tests were applied for intragroup pre- and postoperative comparisons. A two-tailed P < 0.05 was considered statistically significant.
Result
To ensure the reliability of the results, 379 patients were divided into VO, ERM and other disease groups (including RRD, PDR, MH, etc). From the overall distribution, VO (188 cases, 49.6%) and ERM (105 cases, 27.7%) were the most common diagnostic types, while other diseases (86 cases, 22.7%) were relatively rare. There were 182 cases in group A, including 130 cases of VO (71.4%), 28 cases of ERM (15.4%), and 24 cases of other diseases (13.2%); There were 197 cases in group B, including 58 cases of VO (29.4%), 77 cases of ERM (39.1%), and 62 cases of other diseases (31.5%). See Table 1 for details. Group A and Group B showed no statistically significant differences in age across all patients (62.45±11.44 vs 64.14±9.37), VO patients (63.03±11.57 vs 64.95±8.14), MRE patients (59.86±12.32 vs 62.60±10.73), and patients with other diseases (62.33±9.49 vs 65.31±8.46). Additionally, gender distribution (all P>0.05) and affected eye proportion (all P>0.05 except for “Other” disease subtype with P=0.002) were generally comparable between the two groups. For details, see Table 2. There was no statistically significant difference in AL between group A and group B, with AL values of 27.46 ± 3.29 mm and 26.97 ± 3.64 mm, respectively. The AL values of VO patients in both groups were 27.70 ± 3.32 mm and 28.69 ± 3.30 mm, respectively, with no statistically significant difference; There was no statistically significant difference in AL between the two groups of MRE patients, with values of 26.70 ± 3.33 mm and 25.67 ± 3.16 mm, respectively. And here has also been no statistically significant difference in AL between the two groups of patients with other diseases, with values of 27.02 ± 2.97 mm and 26.77 ± 3.65 mm, respectively. Refer to Table 3 for details.
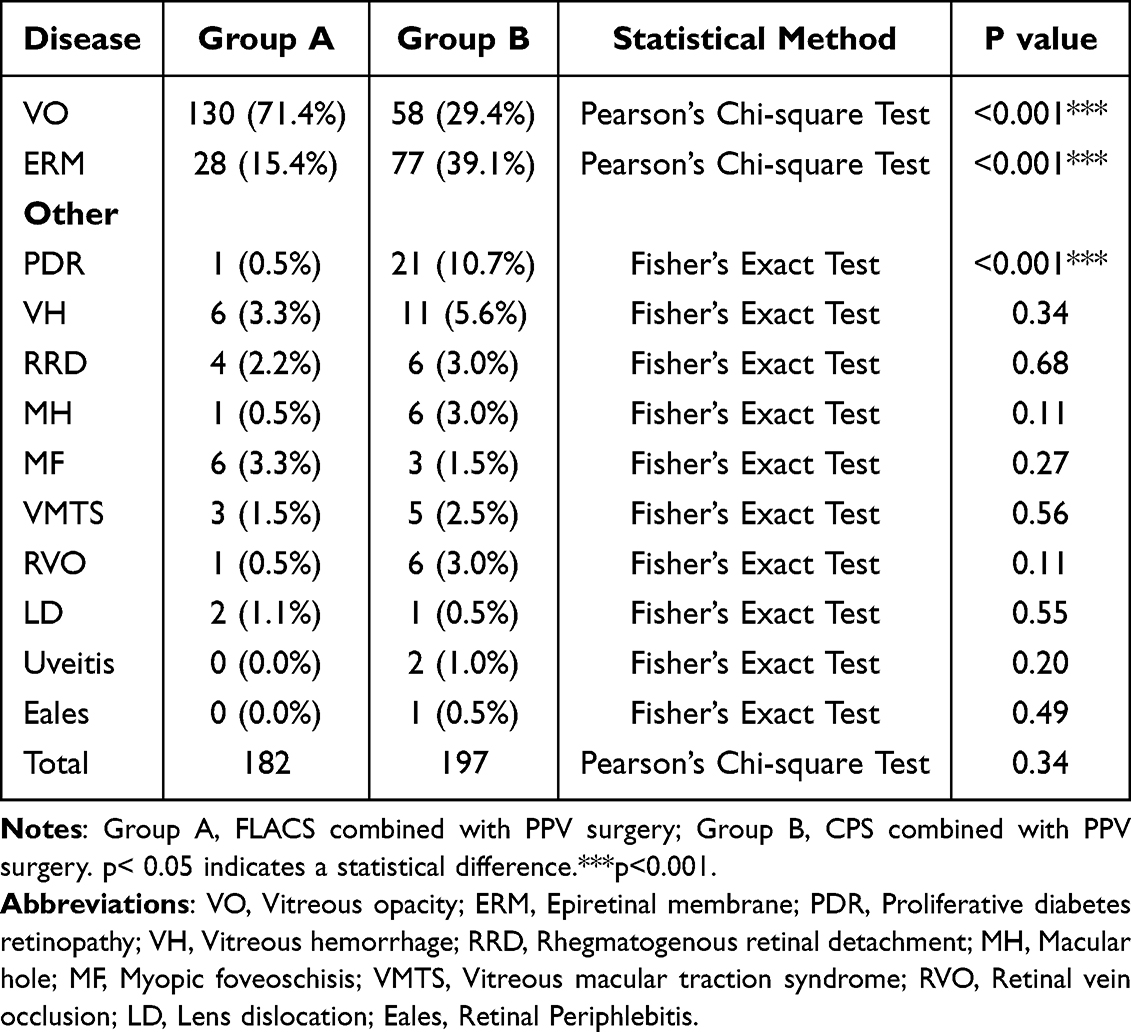 |
Table 1 Number of Patients for Each Disease in the Two Groups |
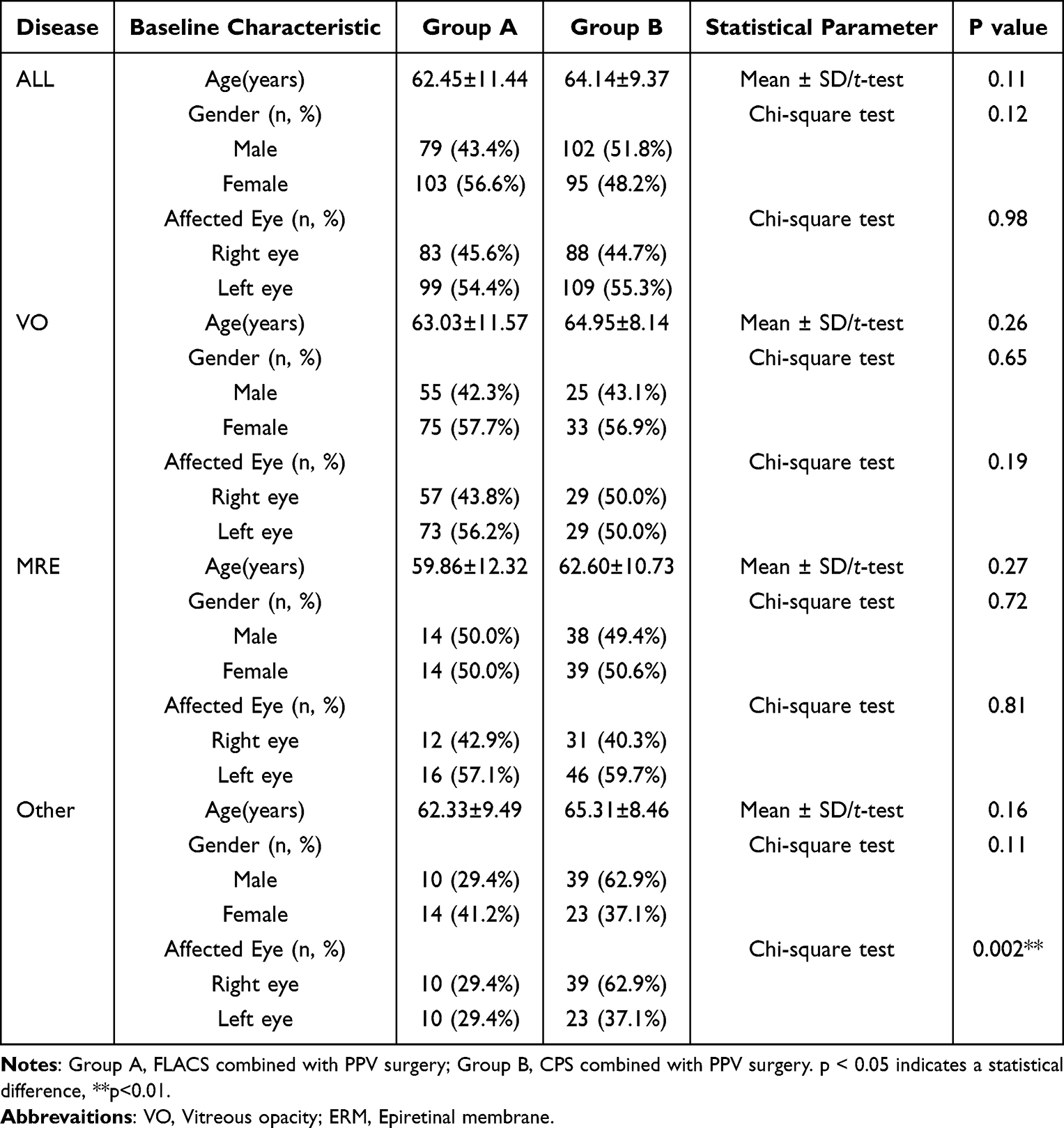 |
Table 2 The Age Comparison of the Two Groups of Patients Among Different Disease Types |
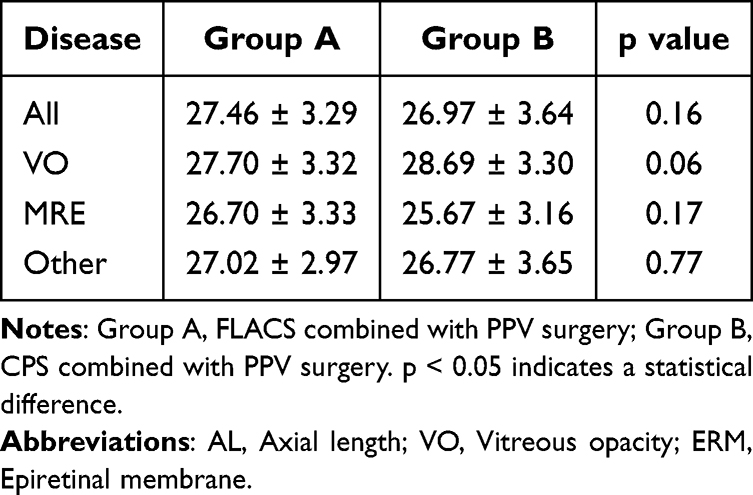 |
Table 3 The AL Comparison of the Two Groups of Patients Among Different Disease Types (mm) |
There was no statistically significant difference in preoperative and postoperative IOP between group A and group B patients, as well as in preoperative and postoperative IOP between different diseases. All IOP were within the normal range, as shown in Table 4 for details.
 |
Table 4 The IOP Comparison of the Two Groups of Patients Among Different Disease Types (mmHg) |
The SE of both group A and group B after surgery was significantly higher than that before surgery. There was no statistical difference in SE between group A and group B before surgery. However, after surgery, except for patients with VO, the SE of all patients, MRE, and patients with other diseases in group B was significantly lower than that in group A. Furthermore, there was no significant difference in the difference between postoperative SE and preoperative SE in all types of disease patients between the two groups. Details are shown in Table 5.
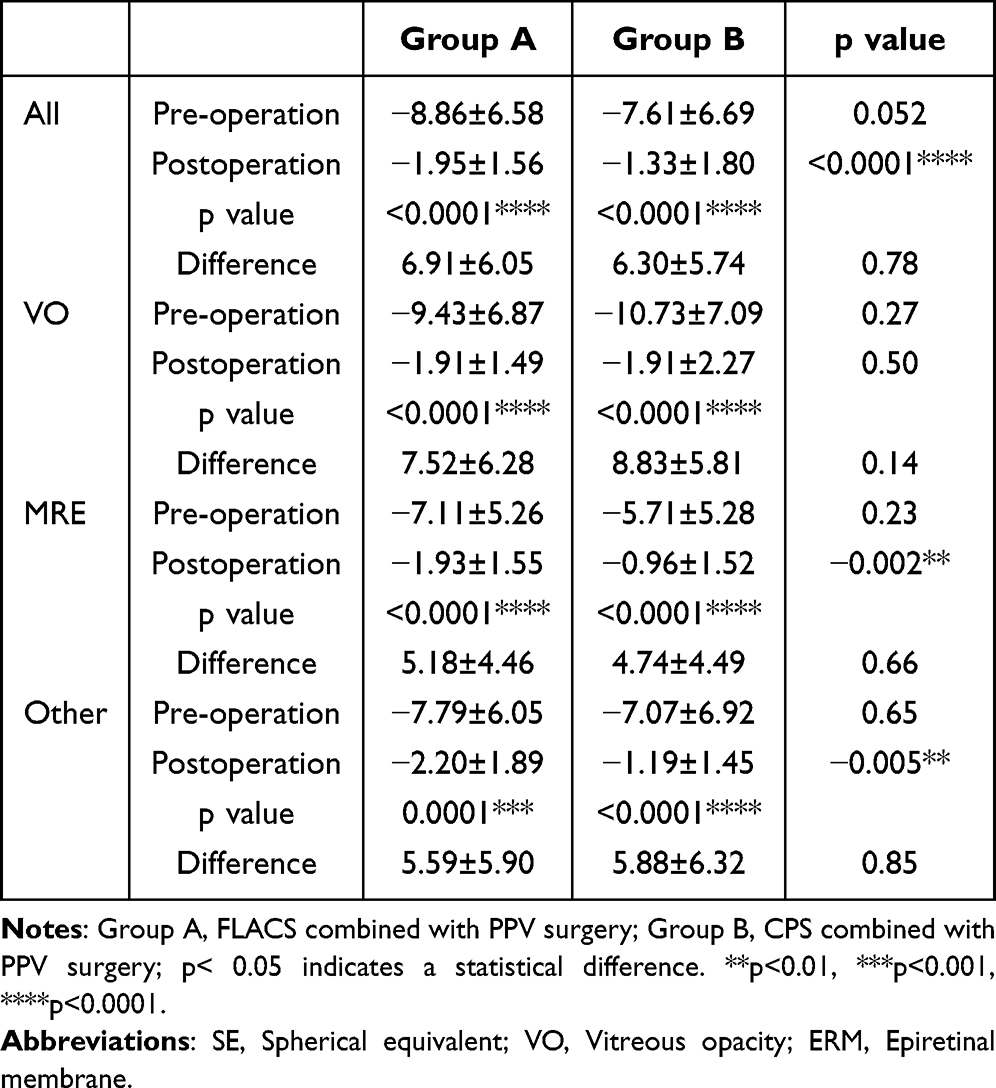 |
Table 5 The SE Comparison of the Two Groups of Patients Among Different Disease Types (D) |
The postoperative Logmar BCVA in both group A and group B was significantly lower than before surgery. There was no statistically significant difference in BCVA between group A and group B before surgery. However, after surgery, among all patient groups and VO patients, the BCVA of group A was significantly smaller than that of group B. The postoperative BCVA of group A and B patients were 0.36±0.45 and 0.49±0.48, respectively (p=0.0001), while that of VO patients was 0.29±0.37 and 0.45±0.50, respectively (p=0.01); In addition, the difference between postoperative SE and preoperative SE of VO patients in groups A and B, 0.34±0.51 in group A, was significantly greater than 0.15±0.52 in group B (p=0.03), while no differences in other diseases and all patients. For details, refer to Table 6 for details.
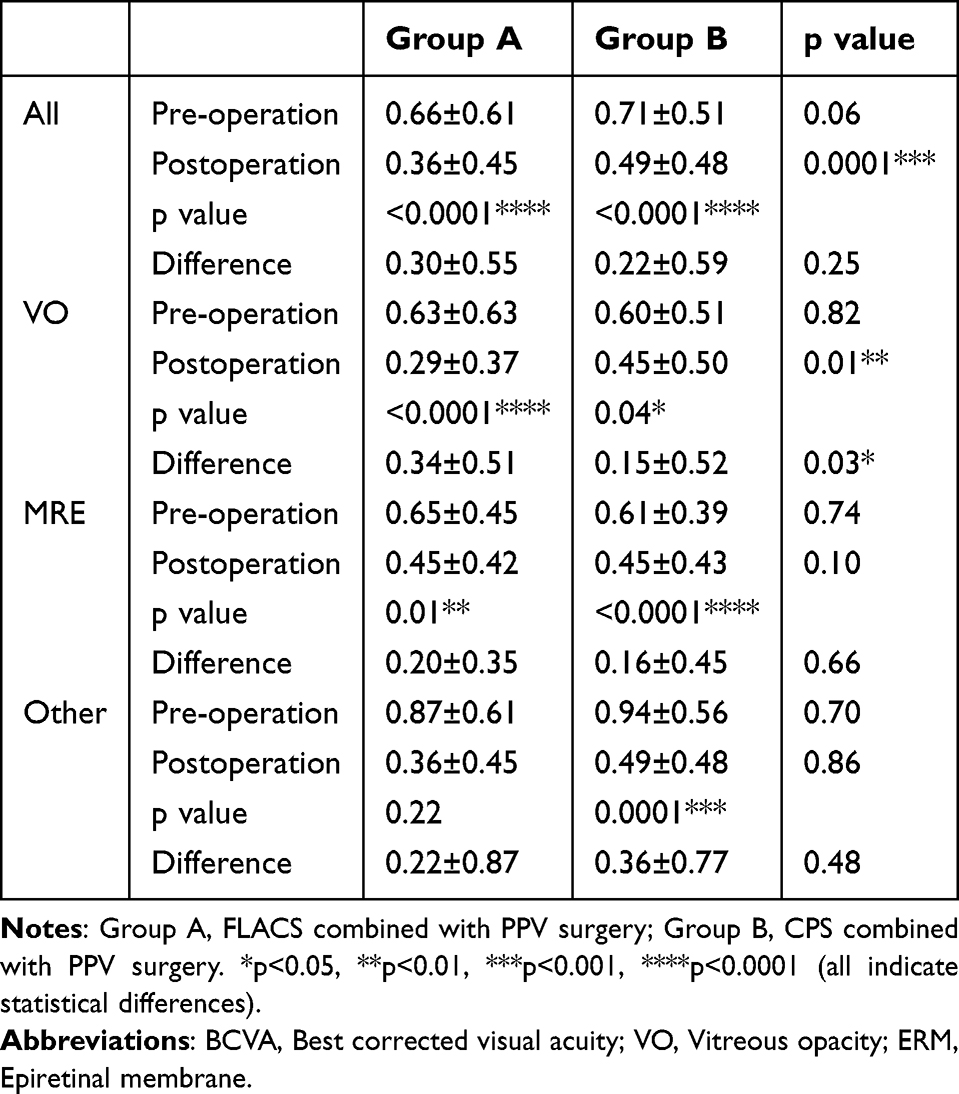 |
Table 6 The BCVA Comparison of the Two Groups of Patients Among Different Disease Types (Logmar) |
Among the 182 patients in Group A, 13 (7.14%) developed complications, while the complication rate in Group B (197 patients) was 11.68% (23 cases), with no statistically significant difference in the overall complication rate between the two groups (Pearson’s chi-square test, P=0.12). RRD was the most common complication, with 9 cases (4.95%) in Group A and 3 cases (1.52%) in Group B (almost all were HM patients, with more severe axial length in Group A but no statistical difference; Fisher’s exact test, P=0.04); Irvine-Gass syndrome occurred in 2 (1.10%) and 3 (1.52%) cases in Groups A and B, respectively (P=0.73), and posterior capsular rupture was reported in 1 case (≈0.5%) in each group (P=0.97). Notably, cefuroxime-induced toxic macular edema was exclusive to Group B (4 cases, 2.03%; P=0.02), and Group B also had 2 cases of recurrent vitreous hemorrhage and NVG, plus 1 case each of persistent corneal edema, ERM, ophthalmic artery occlusion, MHRD, BRVO, and endophthalmitis—none of these complications were observed in Group A (all P > 0.05 for these subtypes, Fisher’s exact test). For detailed data, see Table 7.
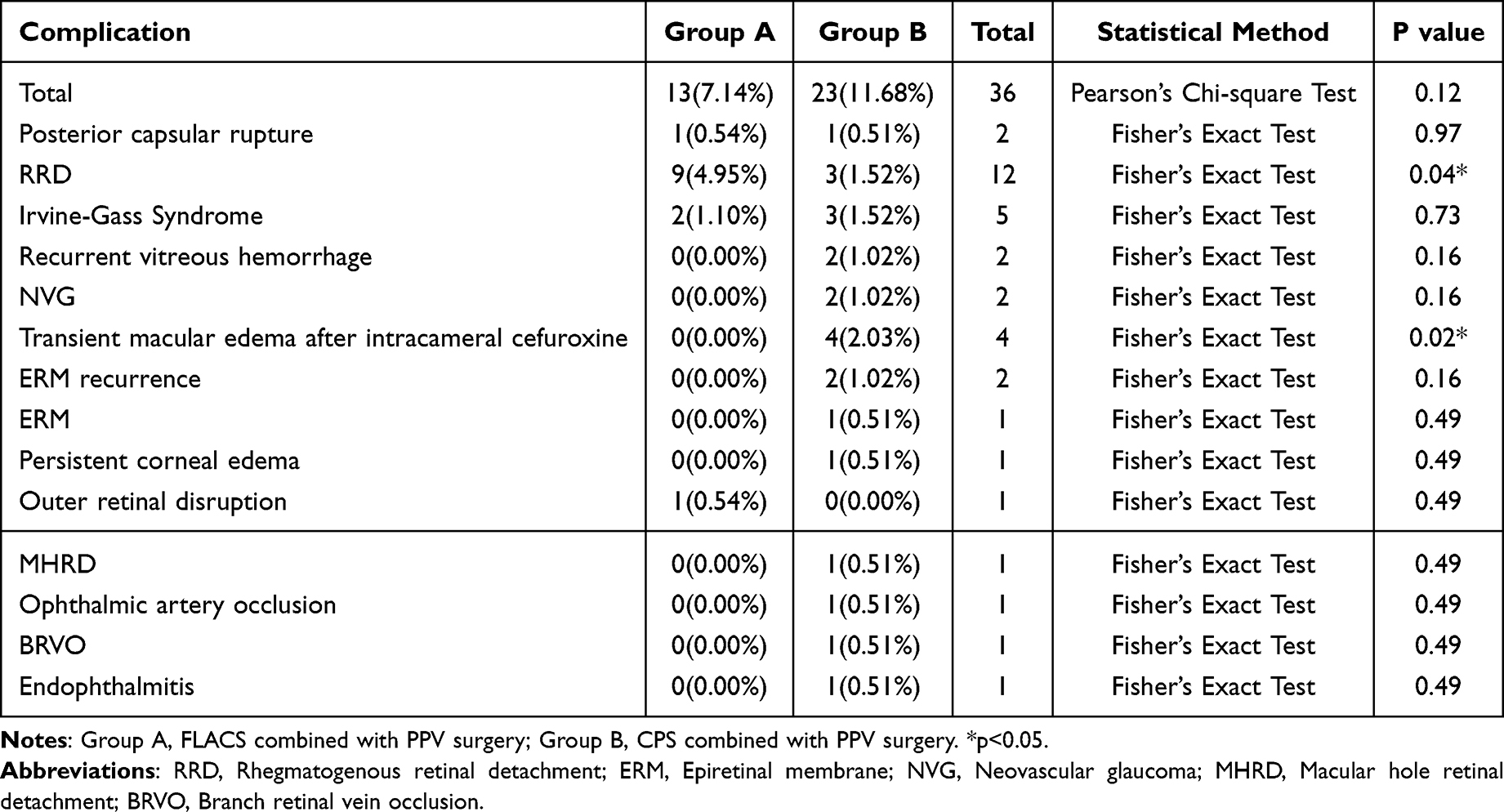 |
Table 7 The Complications of the Two Groups of Patients |
The comparison of operation time between the two groups of patients showed that the operation time of group A was 47.75±10.06min, which was 11.47min less than that of group B (59.22±11.6min) (p < 0.0001). The operation time of the two groups of VO patients was 45.22±8.15min and 57.72±7.17min respectively. The operation time of group A was 7.5min less than that of group B (p < 0.0001). And the operation time of MRE patients in the two groups was 52.50±5.25min in group A, which was approximately 6.14min shorter than 58.97±11.13 min in group B (p=0.004). Besides, the operation time of other diseases was 55.58±16.10 min in group A and 65.60±12.17min in group B, group A was 10.02min less than group B (p=0.0007). For detailed information, please refer to Table 8, It can be seen that the operation duration of group A is significantly shorter than that of Group B.
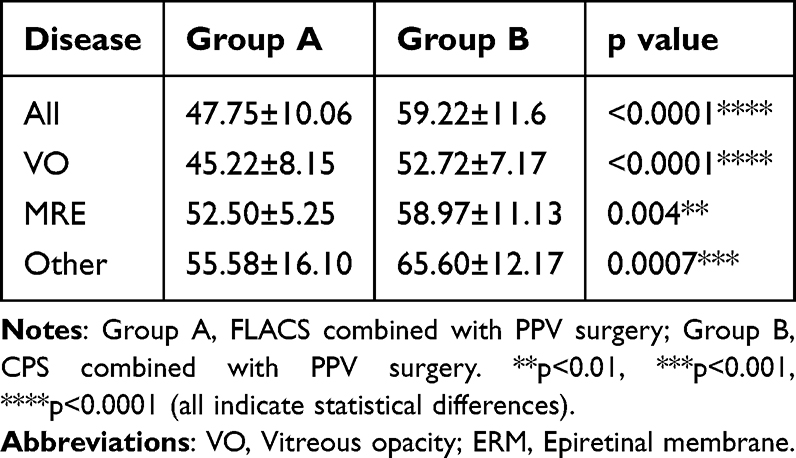 |
Table 8 The Duration of Surgery Comparison of the Two Groups of Patients Among Different Disease Types (min) |
In terms of treatment costs, among all patients, the cost in group A was 21,600 ± 9180 yuan, significantly higher than that in group B, which was 15,399 ± 2996 yuan (p<0.0001), approximately 6201 yuan higher. The values of the two groups of VO patients were 22,152 ± 9538 yuan and 17,113 ± 3716 yuan respectively. The average value of group A was 5039 yuan higher than that of group B (p=0.004). The cost for MRE patients in the two groups was 20,332 ± 7950 yuan in group A, which was 5739 yuan higher than 14,593 ± 2273 yuan in group B (p<0.0001); The costs of other diseases were 20,089 ± 8525 yuan and 14,797 ± 2349 yuan respectively, group A was 5292 yuan higher than group B (p=001). Details are shown in Table 9. It can be seen that FLACS combined with PPV surgery is relatively expensive.
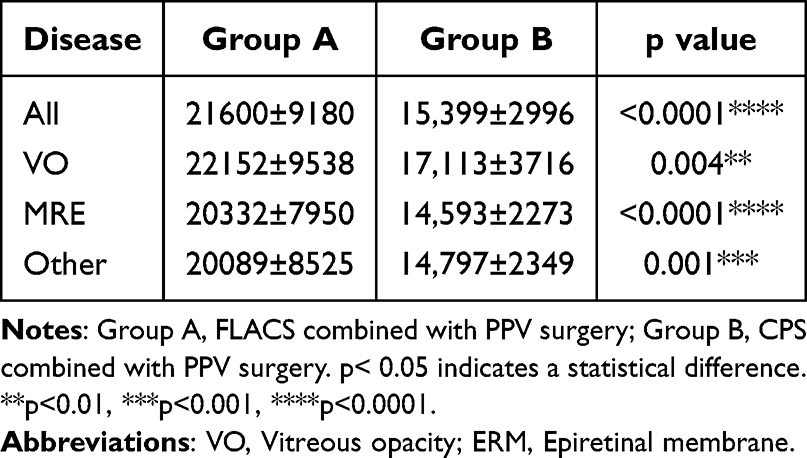 |
Table 9 The Cost Comparison of the Two Groups of Patients Among Different Disease Types (Yuan) |
Discussion
For patients with cataracts combined with fundus diseases, combined surgery is a safe and effective option.15 There have been many reports in the early stage confirming the efficacy of combined surgery. For example, in 2005, Hsu SY et al16 compared the efficacy of phacoemulsification and extracapsular excision combined with PPV and IOL surgery, they found that compared with extracapsular surgery, phacoemulsification combined with PPV could significantly improve the visual acuity of patients, reduce astigmatism, and have fewer postoperative complications. In addition, Axer-Siegel R et al17 also performed phacoemulsification combined with PPV surgery on 35 patients, confirming that this combined surgical method can better improve the vision of patients and is safe and effective. Nowadays, with the progress of technology, extracapsular cataract extraction has been gradually eliminated, phacoemulsification has become a conventional method of cataract surgery, and FLACS is a major progress in recent cataract surgery.18 Both CPS and FLACS can effectively treat cataract, while the latter has the advantages of short operation time and less endothelial cell loss.19 Unlike CPS, FLACS is a non-invasive surgical method. It uses a computer connected to an optical imaging system to guide the laser to perform corneal incision, cystectomy and lens fragmentation steps, etc., improving the tearing of the anterior capsule, reducing the time and effort of the surgery, and is a safer surgical method.20 Similarly, vitrectomy system has also made rapid development in the new century. With the continuous miniaturization of instruments, the vitrectomy system from 23g to 25g and then to 27g has become more and more minimally invasive.21–23 Compared with the traditional 20g PPV system, the minimally invasive vitrectomy system can achieve less injury and faster postoperative recovery. These technological advances not only improve the operation efficiency and reduce the surgical trauma, but also provide patients with better postoperative visual prognosis and quality of life. The application of these innovative technologies makes vitrectomy show greater potential and advantages in the treatment of complex fundus diseases. Although CPS remains the gold standard for cataract surgery at present, FLACS, as a new type of surgery, has become relatively mature. It has good visual and refractive effects, a low complication rate, a shorter operation time, and precise capsule incision, however, due to the high cost of lasers and surgical consumables, the overall expense is higher.24,25 Currently, FLACS has high potential and prospects, but its application in PPV combined surgery is still relatively limited, and there is a lack of large-sample clinical studies.
Statistical test (Table 1) showed that there was a significant difference in the distribution of major diseases between the two groups - the VO proportion of group A was significantly higher (p<0.001), while the ERM (p<0.001) and other diseases (p<0.001) of group B, especially the PDR subtype, accounted for a higher proportion (p<0.001); This distribution feature suggests that group B is more likely to deal with complex fundus diseases (such as PDR and MH), while group A is mainly for VO with relatively simple treatment. Notably, among the rare subtypes of other diseases, only PDR showed a statistically significant intergroup difference (Group A: 0.5% vs Group B: 10.7%, p<0.001), while VH, RRD, MH and other subtypes had no significant differences (all p>0.05). This indicates that although Group B undertakes more complex cases, the distribution of most rare diseases is balanced, which reduces the impact of disease severity on the comparative results of the two surgical methods. Moreover, baseline characteristic analysis (Table 2) confirmed that the two groups were balanced in age, gender, and most ocular parameters (eg, AL, IOP), except for the affected eye distribution in the “other diseases” subtype (p=0.002), which did not affect the core outcome comparison.
Besides, our study also compared FLACS combined PPV with CPS combined PPV in terms of cost, visual improvement, complications, and procedure time. The average surgical cost of group A was significantly higher than that of group B. This may limit widespread use of FLACS in resource-limited medical settings. The high cost mainly stems from the expensive technical equipment of FLACS, which increases the economic burden of patients. In terms of postoperative visual acuity improvement, group A showed a slight advantage, mainly in VO patients, the improvement of BCVA (logmar) in group A was 0.34±0.51, while that in group B was 0.15±0.52 (p=0.03), while there was no significant difference in BCVA improvement in all patients and other disease groups, although there was no significant difference between the two groups. Existing study also suggests that FLACS may have some advantages in visual improvement,26 but most studies indicate that the effect of FLACS on BCVA enhancement is comparable to CPS.27–29 Visual improvement is an important indicator of surgical success, although FLACS performs slightly better in this regard, and patients may need to weigh it based on financial circumstances. In addition, the average surgical time of group A was significantly shorter than that of group B. A shorter surgical time may have a positive impact on patient comfort and operating room utilization, not only improving surgical efficiency but also potentially reducing intraoperative discomfort for patients. However, FLACS surgery also has certain limitations. For example, due to small pupils and poor negative pressure suction, some patients are unable to complete the femtosecond laser procedure and switch to traditional phacoemulsification surgery. In this case, the surgical outcome may be affected, and detailed preoperative screening and intraoperative caution are required.
In addition, the results of this study showed that the incidence of complications in the FLACS+PPV group (Group A) was lower (7.14% vs 11.68% in Group B), although the overall difference was not statistically significant (Pearson’s chi-square test, p=0.12) (Table 7). However, subtype analysis revealed meaningful differences: RRD, the most common complication, was more frequent in Group A (4.95% vs 1.52%, p=0.04), which may be related to the more severe axial length in HM patients of Group A (though not statistically significant). In contrast, cefuroxime-induced toxic macular edema was exclusive to Group B (4 cases, 2.03%, p=0.02), and Group B also had multiple rare complications (eg, persistent corneal edema, ophthalmic artery occlusion, endophthalmitis) that were not observed in Group A. These results suggest that FLACS may reduce the risk of certain iatrogenic complications (eg, drug-induced macular edema) through precise surgical manipulation, while Group A’s higher RRD rate may be associated with baseline ocular characteristics rather than surgical technique. From the perspective of CPS clinical practice, certain specific issues may arise postoperatively: for instance, some patients may experience an increase in foveal macular thickness, but this can be effectively prevented by using cold irrigating solution during surgery.30 Additionally, although the incidence of retained lens fragments in the anterior chamber after CPS is low, such an occurrence can cause significant damage to corneal endothelial cells. Early Nd:YAG laser treatment serves as an optimal approach to promptly remove residual fragments, which not only reduces the persistent damage to endothelial cells caused by the fragments but also avoids the discomfort and additional costs associated with secondary surgery for patients. Simultaneously, it lowers the risk of delayed inflammatory complications potentially induced by retained lens fragments—these complications may occur several years after the initial surgery, leading to aggravated visual impairment due to endothelial cell damage from the fragments.31 These targeted management strategies provide effective safeguards for the safe application of CPS. Existing studies also suggest that FLACS possesses unique potential in reducing intraoperative and postoperative complications. Its characteristic of precise laser manipulation can minimize the risks arising from variations in manual operation. Meta-analyses have further confirmed that compared with CPS, FLACS is associated with a lower incidence of certain complications. Most of these complications can be prevented through adequate preoperative preparation and standardized surgical procedures; even if they occur, they typically resolve spontaneously within a short period without affecting the final visual outcomes.32 In summary, FLACS reduces the risk of complications at the source through its technical characteristics. Although CPS may be accompanied by certain specific issues, the risks can also be effectively controlled with mature intraoperative preventive measures and postoperative intervention protocols.
Our study has a relatively sufficient sample size. In previous reports, a larger sample size of FLACS combined with PPV was 34 eyes.33 At present, our study is the largest clinical report in terms of sample size. We found that FLACS combined with PPV surgery has certain advantages in improving vision and reducing complications, but its high cost is its main disadvantage. CPS combined with PPV has greater cost-effectiveness advantages, although its visual improvement effect and incidence of complications are slightly inferior to FLACS combined with PPV. Taking into account the higher cost of FLACS surgery, this surgical method does not have significant advantages over CPS combined with PPV. The choice of surgical approach should be balanced based on specific clinical conditions and patient needs. Future research should focus on technological improvements and cost reduction to evaluate the long-term clinical and economic benefits of FLACS combined with PPV surgery.
This study has made certain improvements in providing control group data and increasing the number of cases compared to existing reported studies. These improvements not only make our research results more convincing, but also provide a more solid foundation for future research and clinical practice. We hope that the results of this study can provide reference for the selection and optimization of ophthalmic surgery, promote the progress of clinical practice, and improve patient prognosis. Although this study provides important data support, there are still some limitations. Firstly, this study is a retrospective analysis and there may be selection bias, which is a retrospective analysis of secondary clinical data: 403 eyes undergoing combined cataract+PPV surgery were initially identified, with 24 (6.0%) excluded due to incomplete follow-up data, resulting in a final sample of 379 eyes with comprehensive records, inherent limitations include potential selection bias, unmeasured confounders, and marginal impacts on generalizability, mitigated by the large sample size and strict eligibility criteria;. Secondly, the follow-up time is relatively short, making it impossible to comprehensively evaluate the long-term effects of the surgery. Future research should focus on multicenter, large-scale prospective randomized controlled trials to validate the results of this study. In addition, further exploration should be conducted on the specific application and effects of FLACS combined with PPV surgery for patients with different types of fundus diseases, in order to provide more accurate treatment plans for clinical practice.
Conclusion
In conclusion, both FLACS+PPV and CPS+PPV effectively improve visual acuity in patients with cataract complicated by fundus diseases, with comparable overall safety. FLACS+PPV offers distinct advantages for vitreous opacity (VO) patients, including better visual improvement, shorter surgical time, and avoidance of certain complications (eg, cefuroxime-induced toxic macular edema), making it a preferred choice for this subgroup. CPS+PPV, however, demonstrates superior cost-effectiveness, suitable for resource-limited settings or non-VO cases. Clinical selection should be tailored to the patient’s disease type, economic status, and medical resources. Notably, this study is a retrospective analysis with potential selection bias. Clinical surgical selection should be based on the patient’s condition, economic status, and medical resources. Future prospective randomized controlled trials are needed to validate these findings.
Data Sharing Statement
All relevant data supporting the results of this study are available upon request from the correspondence authors.
Acknowledgments
Thanks to Hunan Aier Eye Research Institute for its funding support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
2023 Aier Eye Hospital Research Fund (AGF2301D25); The 2023 Research Fund of Aier Eye Research Institute (AEI202310LC01); The Technology Innovation Program of Hunan Province (2024JJ9022); The Science Research Foundation of Aier Eye Hospital Group (AGF2301D22).
Disclosure
The authors report no competing interests in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Global Health. 2017;5(12):e1221–13. doi:10.1016/S2214-109X(17)30393-5
2. Lee NS, Ong K. Changes in refraction after cataract phacoemulsification surgery. Int Ophthalmol. 2023;43(5):1545–1551. doi:10.1007/s10792-022-02550-9
3. Akmaz B, Kilic D, Duru N. The safety and efficacy of phacoemulsification surgery in uncomplicated cataracts with and without an ophthalmic-viscosurgical-device. Eur J Ophthalmol. 2023;33(1):269–277. doi:10.1177/11206721221116701
4. Zarei-Ghanavati S, Hadi Y, Habibi A, Ashraf Khorasani M, Yoo SH. Cataract and diabetes: review of the literature. J Cataract Refr Surg. 2024;50(12):1275–1283. doi:10.1097/j.jcrs.0000000000001547
5. Popovic MM, Muni RH, Nichani P, Kertes PJ. Pars plana vitrectomy, scleral buckle, and pneumatic retinopexy for the management of rhegmatogenous retinal detachment: a meta-analysis. Surv Ophthalmol. 2022;67(1):184–196. doi:10.1016/j.survophthal.2021.05.008
6. Mihalache A, Huang RS, Ahmed H, et al. pars plana vitrectomy with or without internal limiting membrane peel for epiretinal membrane: a systematic review and meta-analysis. Ophthalmologica. 2024;247(1):30–43. doi:10.1159/000534851
7. Ghoraba H, Rittiphairoj T, Akhavanrezayat A, et al. Pars plana vitrectomy with internal limiting membrane flap versus pars plana vitrectomy with conventional internal limiting membrane peeling for large macular hole. Cochrane Database of Syst Rev. 2023;8(8):CD015031. doi:10.1002/14651858.CD015031.pub2
8. Hernandez-Bogantes E, Abdala-Figuerola A, Olivo-Payne A, Quiros F, Wu L. Cataract following pars plana vitrectomy: a review. Semin Ophthalmol. 2021;36(8):824–831. doi:10.1080/08820538.2021.1924799
9. Awidi AA, Mathews PM, Shekhawat N, Woreta FA, Srikumaran D, Daoud YJ. Comparison of simultaneous vs sequential pars plana vitrectomy and cataract surgery. Bmc Ophthalmol. 2023;23(1):74. doi:10.1186/s12886-023-02801-y
10. Port AD, Nolan JG, Siegel NH, Chen X, Ness SD, Subramanian ML. Combined phaco-vitrectomy provides lower costs and greater area under the curve vision gains than sequential vitrectomy and phacoemulsification. Graefes Arch Clin Exp Ophthalmol. 2021;259(1):45–52. doi:10.1007/s00417-020-04877-4
11. Savastano A, Lenzetti C, Finocchio L, et al. Combining cataract surgery with 25-gauge high-speed pars plana vitrectomy: a prospective study. Eur J Ophthalmol. 2021;31(2):673–678. doi:10.1177/1120672120902030
12. Gómez-Resa M, Nieto I, Corcóstegui B. Combined 23-gauge vitrectomy and femtosecond laser-assisted cataract surgery. Ophthalmic Res. 2014;52(3):141–146. doi:10.1159/000367716
13. Lin H, Kao S, Chuang Y, Chen S, Lin P. Comparison of cumulative dispersed energy between conventional phacoemulsification and femtosecond laser-assisted cataract surgery with two different lens fragmentation patterns. Laser Med Sci. 2022;37(2):843–848. doi:10.1007/s10103-021-03321-1
14. Kolb CM, Shajari M, Mathys L, et al. Comparison of femtosecond laser-assisted cataract surgery and conventional cataract surgery: a meta-analysis and systematic review. J Cataract Refr Surg. 2020;46(8):1075–1085. doi:10.1097/j.jcrs.0000000000000228
15. Chaudhry NA, Cohen KA, Flynn HWJ, Murray TG. Combined pars plana vitrectomy and lens management in complex vitreoretinal disease. Semin Ophthalmol. 2003;18(3):132–141. doi:10.1076/soph.18.3.132.29806
16. Hsu S, Wu W. Comparison of phacoemulsification and planned extracapsular cataract extraction in combined pars plana vitrectomy and posterior chamber intraocular lens implantation. Ophthalmic Surg Lasers Imaging. 2005;36(2):108–113. doi:10.3928/1542-8877-20050301-05
17. Axer-Siegel R, Dotan G, Rosenblatt I, Benjamini Y, Weinberger D. Combined pars plana vitrectomy and cataract surgery: outcome of phacoemulsification versus manual extracapsular cataract extraction through a sclerocorneal tunnel. Ophthalmic Surg Lasers Imaging. 2006;37(2):94–98.
18. Narayan A, Evans JR, O’Brart D, Bunce C, Gore DM, Day AC. Laser-assisted cataract surgery versus standard ultrasound phacoemulsification cataract surgery. Cochrane Database Syst Rev. 2023;6(6):CD010735. doi:10.1002/14651858.CD010735.pub3
19. Yeh C, Fang H, Ou Y, Cheng C, Wu T. Comparison of low-energy FLACS and conventional cataract surgery: meta-analysis and systematic review. J Cataract Refr Surg. 2024;50(10):1074–1082. doi:10.1097/j.jcrs.0000000000001501
20. Sun H, Fritz A, Dröge G, Neuhann T, Bille JF. Femtosecond-Laser-Assisted Cataract Surgery (FLACS). In: Bille JF, editor. High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics. Cham (CH): Springer; 2019:301–317.
21. Otsuka K, Imai H, Fujii A, et al. Comparison of 25- and 27-gauge pars plana vitrectomy in repairing primary rhegmatogenous retinal detachment. J Ophthalmol. 2018;2018:7643174. doi:10.1155/2018/7643174
22. Sborgia G, Niro A, Sborgia L, et al. One-year outcomes of 27-gauge versus 25-gauge pars plana vitrectomy for uncomplicated rhegmatogenous retinal detachment repair. Int J Retina Vitr. 2019;5(1):13. doi:10.1186/s40942-019-0164-0
23. Li J, Zhao B, Liu S, Li F, Dong W, Zhong J. Retrospective comparison of 27-Gauge and 25-Gauge microincision vitrectomy surgery with silicone oil for the treatment of primary rhegmatogenous retinal detachment. J Ophthalmol. 2018;2018:7535043. doi:10.1155/2018/7535043
24. Dick HB, Gerste RD, Taneri S. Femtosecond laser-assisted cataract surgery. Asia Pac J Ophthalmol. 2025;14(4):100228. doi:10.1016/j.apjo.2025.100228
25. Kanclerz P, Alio JL. The benefits and drawbacks of femtosecond laser-assisted cataract surgery. Eur J Ophthalmol. 2021;31(3):1021–1030. doi:10.1177/1120672120922448
26. Ma L, Rong A, Jiang Y, Deng S. Effects of femtosecond laser-assisted cataract surgery on macular and choroidal thickness in diabetic patients. Ophthalmol Ther. 2021;10(1):137–150. doi:10.1007/s40123-020-00326-x
27. Gigliola S, Sborgia G, Niro A, et al. Comparison of perioperative parameters in one-handed rotational phacoemulsification versus conventional phacoemulsification and femtosecond laser-assisted cataract surgery. Int J Ophthalmol Chi. 2021;14(12):1868–1875. doi:10.18240/ijo.2021.12.09
28. Koo EH, Bolton EM, Vanner EA, Eghrari AO, Donaldson KE. Outcomes of femtosecond laser-assisted cataract surgery compared to conventional phacoemulsification in eyes with pseudoexfoliation syndrome. Semin Ophthalmol. 2022;37(5):631–636. doi:10.1080/08820538.2022.2051054
29. Chee SP, Yang Y, Wong MHY. Randomized controlled trial comparing femtosecond laser-assisted with conventional phacoemulsification on dense cataracts. Am J Ophthalmol. 2021;229:1–7. doi:10.1016/j.ajo.2020.12.024
30. Meduri A, Oliverio GW, Bergandi L, et al. Role of cold balanced salt solution (BSS) in the prophylaxis of cystoid macular edema after cataract surgery: a prospective randomized study. Clin Ophthalmol. 2021;15:2519–2526. doi:10.2147/OPTH.S304146
31. Meduri A, Oliverio GW, De Luca L, Borroni D, Frisina R, Aragona P. Anterior chamber retained lens fragments: a novel approach with Nd:Yag laser. Eur J Ophthalmol. 2025;35(3):917–921. doi:10.1177/11206721241280740
32. Xu J, Chen X, Wang H, Yao K. Safety of femtosecond laser-assisted cataract surgery versus conventional phacoemulsification for cataract: a meta-analysis and systematic review. Adv Ophthalmol Pract Res. 2022;2(1):100027. doi:10.1016/j.aopr.2022.100027
33. Kubota M, Watanabe A, Watanabe T, Kono H, Hayashi T, Nakano T. Complications of femtosecond laser-assisted cataract surgery combined with vitrectomy. Int Ophthalmol. 2020;40(4):943–949. doi:10.1007/s10792-019-01266-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.