Back to Journals » International Medical Case Reports Journal » Volume 12
Femoral mononeuropathy in Lyme disease: a case report
Received 7 March 2019
Accepted for publication 20 June 2019
Published 31 July 2019 Volume 2019:12 Pages 243—247
DOI https://doi.org/10.2147/IMCRJ.S207889
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ronald Prineas
Reynaldo P Lazaro,1 Khalid Butt2
1Neurology and Electroneuromyography Clinic, Oneonta, NY 13820, USA; 2Internal Medicine Clinic, Bainbridge, NY 13733, USA
Background: Peripheral neuropathy is a common complication of Lyme disease. Cranial mononeuropathy, particularly that affecting the facial nerve, can be a presenting symptom, and at times, it can be associated with polyradiculopathies or plexopathies. However, isolated femoral neuropathy has not yet been reported in Lyme disease; therefore, we felt the need to present this case.
Case presentation: Laboratory investigations were performed on a 67-year-old man living in a region at high risk for Lyme disease after he developed erythema migrans on his chest, accompanied by the swelling of his left knee joint. A Western blot immunoglobulin assay was performed, including a screening for connective tissue disorders. Positive serological test results led to the administration of oral doxycycline therapy at a dosage of 100 mg twice daily. Shortly afterwards, he developed gait difficulties and frequent falls. The clinical examination and electrodiagnostic studies were consistent with femoral neuropathy. To look for etiologies other than Lyme disease, radiographic studies of his lumbar spine, pelvic cavity, retroperitoneal compartment, and hips were conducted. In addition, he was screened for diabetes. However, no other etiologies were found to explain the femoral neuropathy. Eventually, he recovered, and he was able to return to work.
Conclusion: We firmly believe that the femoral neuropathy and Lyme disease seen in this patient were causally related.
Keywords: ataxic gait, femoral neuropathy, frequent falls, gait difficulty, Lyme disease, muscle weakness, plexopathy, peripheral neuropathy, radiculopathy
Introduction
Lyme borreliosis or Lyme disease (LD) is a tick-borne illness transmitted to mammals through the bite of an infected tick vector, Ixodes scapularis (deer tick), which releases the spirochete Borrelia burgdorferi into the bloodstream of the host. Deer ticks are most common in the eastern and central United States, and they are found in wooded or grassy areas. The risk of infection is the highest between the months of April and November. Within 1–2 weeks following a bite or the appearance of the characteristic “bull’s eye” rash, constitutional symptoms (fever, fatigue, muscle and joint pain) resembling the flu may occur. If left unrecognized or untreated, the dissemination of the infection results in various clinical manifestations referable to the joints, heart, central nervous system, and peripheral nervous system. The protean manifestations can mimic rheumatoid arthritis, cardiac disorders, and multiple sclerosis. Experimental models for LD, using tick-inoculated nonhuman primates, have shown lymphoplasmacytic inflammation in the perivascular spaces and collagenous tissues of the meninges, brainstem, peripheral nerves, synovium, perisynovial adipose tissue, urinary bladder, skeletal muscle, myocardium, and visceral pericardium.1
The peripheral neuromuscular segments affected in Lyme neuroborreliosis (LNB) include the nerve cell bodies and their axons, all of the cranial nerves except the olfactory nerve, the nerve roots, the brachial and lumbosacral plexuses, and the peripheral nerves, either in isolation or as part of a multiple or diffuse neuropathic process.2,3 Mononeuropathy multiplex has been demonstrated in nonhuman primates with chronic LD.4 In addition, rare cases of focal myositis have been reported in the literature,5–7 and the organism has been isolated from the myocardium of one patient with cardiomyopathy.8 The molecular confirmation of B. burgdorferi in the myocardium of patients with recent-onset dilated cardiomyopathy has been demonstrated in two large studies,9,10 and this strongly supports a causal relationship. Additionally, the microorganism has been shown to induce myositis in nonhuman primates.11 The most common cranial neuropathy affects the facial nerve, either unilaterally or bilaterally.
Here, we report the case of isolated femoral neuropathy (FN) in a 67-year-old man with LD that ameliorated gradually and significantly within 8 months following the appearance of a large circumscribed rash on his chest. To our knowledge, this is the first case report of isolated FN in LD in the English literature.
Case presentation
During the spring of 2017, a 67-year-old man presented with a large painless and nonpruritic rash of approximately 10 cm in size on the left side of his chest below the clavicle. The rash lasted for 3 weeks, and it was accompanied by the swelling of his left knee joint. A 4-week course of oral doxycycline therapy at a dosage of 100 mg twice daily was administered shortly after the serum tested positive for LD using the Western blot (WB) immunoglobulin (Ig)G criteria (Table 1). Shortly after the completion of the doxycycline therapy, this patient began complaining of gait difficulties and frequent falls, as well as intermittent painful cramps in his right thigh.
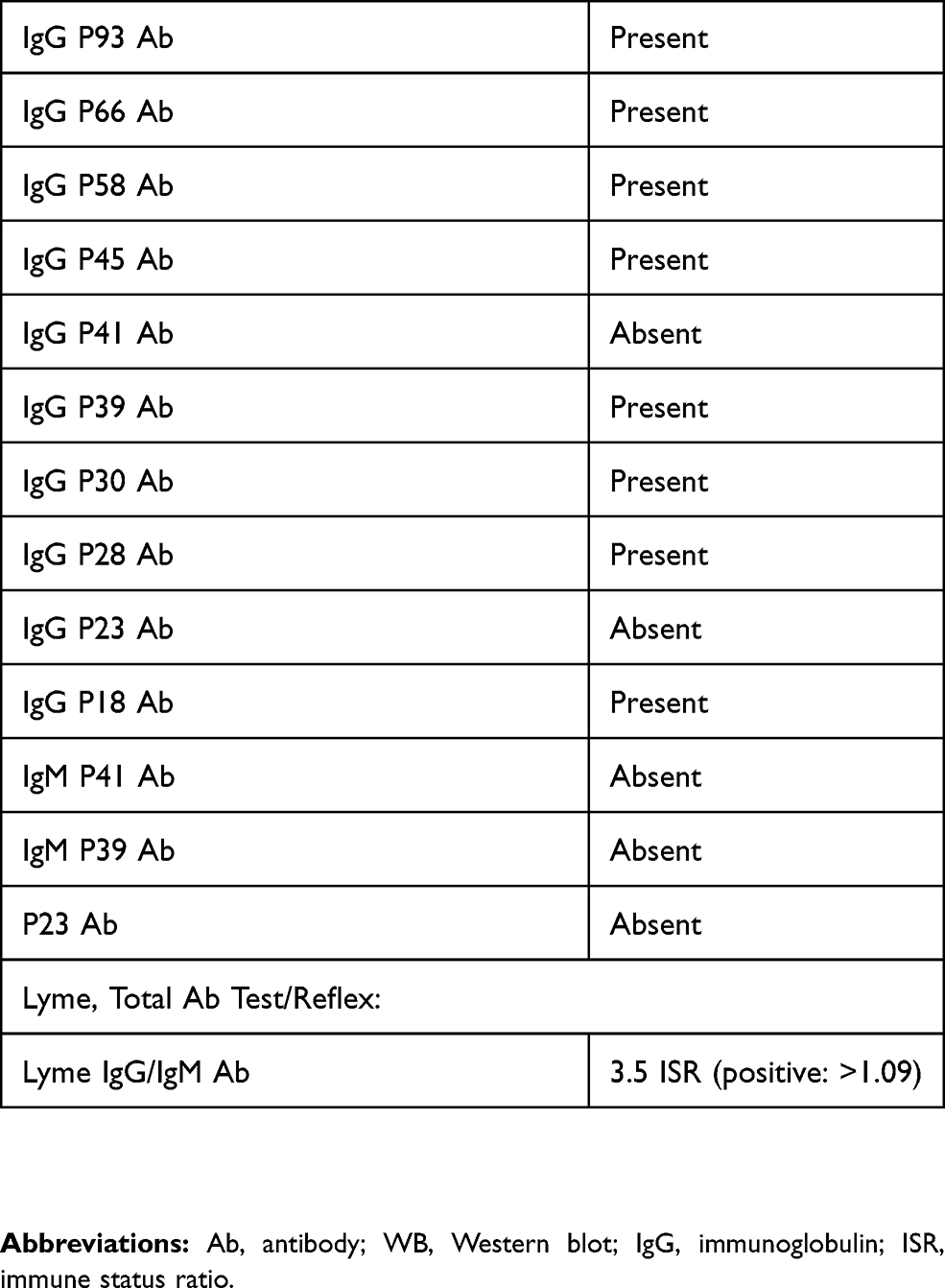 |
Table 1 WB serology* |
At the time of the neurological evaluation, this patient was taking tamsulosin (0.4 mg daily) for benign prostatic hypertrophy, atorvastatin (20 mg daily) for hyperlipidemia, and escitalopram (10 mg daily) for depression. He had taken furosemide (20 mg twice daily) to control the swelling in his left knee. Because the WB serology results were positive, the fluid from his left knee was not examined.
This patient had no history of diabetes, hypertension, coagulopathy, anticoagulant medication intake, traction injury to the hip or lumbar spine, femoral artery catheterization, or malignancy. His father, who suffered from chronic obstructive pulmonary disease, died of renal failure at 85 years old. His mother died of ovarian cancer at 92 years old. One of his brothers had a history of melanoma and one of his sisters had breast cancer.
The physical examination showed weakness in the right quadriceps and psoas muscles (3/5 using the Medical Research Council scale), conspicuous atrophy of the vastus medialis and lateralis muscles (Figure 1), an absent knee muscle stretch reflex, and hypoalgesia over the anterior aspect of the thigh and medial aspect of the leg. The strength of the adductors and abductors of the hips, flexors of the knees, and dorsal and plantar flexors of the ankles was preserved (5/5 on both sides). There were no neurological deficits in the left lower and upper extremities, nor in the cranial nerves. His higher cortical functions were normal, and there were no signs of meningeal irritation or radiculopathy. His clinical pulmonary and cardiovascular examinations were normal, and there were no palpable masses, lymph nodes, or audible bruits in the inguinal region. The hemogram and blood chemistry values were normal. The antinuclear antibody titer (direct) was negative, and the erythrocyte sedimentation rate (Westergren method) was 67 mm/hour (N=0–30).
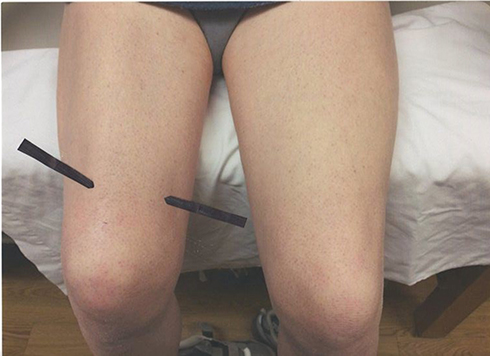 |
Figure 1 The quadriceps femoris muscle of the right thigh showing focal atrophies (arrows) of the vastus lateralis and medialis. |
The immunoscreening ordered by another physician for other tick-borne diseases (babesiosis and ehrlichiosis) and bartonellosis (an infectious disease caused by a bacterium belonging to the genus Bartonella) was essentially negative (test performed at IGeneX Inc., Palo Alto, CA, USA).
A peripheral electrodiagnostic study using a Sierra 11 Wedge EMG NCV System (Cadwell Industries, Inc., Kennewick, WA, USA), with the standard technique for transcutaneous nerve stimulation,12 showed a markedly reduced right femoral nerve action potential (0.19 mV) when compared to the 2.5 mV amplitude measured on the left side. However, there were no temporal dispersions of the muscle action potentials (recorded over the rectus femoris muscle). The peroneal and tibial motor nerve and sural sensory nerve conduction values were normal on both sides. Monopolar needle electromyography (EMG) sampling showed signs of active denervation (fibrillation potentials and sharp positive waves) in the femoral nerve innervated muscles on the right side. The obturator, sciatic, peroneal, and tibial motor nerve innervated muscles, including the paraspinal muscles, showed no signs of denervation or muscle membrane irritability. Four months later, a repeat electrodiagnostic study showed a persistently reduced femoral nerve action potential, but the needle EMG showed signs of reinnervation, with fewer signs of muscle membrane irritability, in the quadriceps femoris muscles.
In view of the absence of radicular or meningeal symptoms, together with the peripheral location of the neurological deficits (as demonstrated clinically and electrophysiologically), it was deemed unnecessary to perform a spinal fluid examination. We did not attempt to culture the synovial fluid in view of the clinical history and positive serology results.
The magnetic resonance imaging (MRI) of the pelvis showed no evidence of femoral neck fractures, hip dislocations, free fluid, or vascular necrosis. There were no retroperitoneal mass lesions or hemorrhages. The MRI of the lumbar spine showed mild disc desiccation and bulging discs, without disc herniation or nerve root compression.
A year after the onset of the disease, and following an extensive course of physical therapy, this patient was able to return to his full-time work as an attendant in a local store. As a practical matter, given his clinical history, laboratory findings, and favorable response to therapy, it was deemed unnecessary to repeat the serological studies.
Discussion
This patient’s clinical symptomatology, together with his history of a rounded expanding rash (erythema migrans) located on his chest and positive serology results (the presence of more than 5 bands in the IgG), argued strongly in favor of a causal relationship between his FN and LD. His place of residence in central New York, a high-risk region for LD, is a supportive and important consideration. In our patient, the other causes of FN, including diabetes, trauma, malignancy, and retroperitoneal hemorrhage, were ruled out clinically and via imaging studies.12,13 None of the medications that he had been taking, including doxycycline, have been reported to induce mononeuropathy, particularly FN.
The clinical course of peripheral neuropathy in LNB varies.2,3 The symptoms may persist long after completing the antibiotic therapy because of the slow nature of the histopathological recovery. It is possible that this patient’s FN had been in progress early on, and that the symptoms became overtly manifested following the doxycycline therapy. Because the natural history of untreated LNB is not well understood, the improvement in the symptoms, which is usually partial, is often coincidental with the antibiotic therapy. It is also plausible that the amelioration of the FN was spontaneous, and not necessarily directly related to the antibiotic therapy. The possibility that our patient’s FN could have been part of mononeuropathy multiplex is tenable, which, if not for a timely institution of antimicrobial therapy, might have evolved into a more overt or disseminated infectious or parainfectious process, affecting both the peripheral and central nervous systems.
The neurophysiological information concerning peripheral neuropathy in LNB revolves around the dysfunction of the myelin and/or axons, but it does not explain the actual mechanism of the neural injury. Isolated reports of demyelination have not been confirmed in other studies.14,15 In our patient, the presence of active denervation in the femoral nerve innervated muscles, as demonstrated by the EMG, did indicate an axonal pathology, raising the possibility of vasculopathy. However, despite the presence of perivascular inflammatory infiltrates in the epineurium reported in previous studies,16–18 unequivocal signs of vessel-wall necrosis have not been demonstrated in the peripheral nerves in LNB cases.19 The normal titer of antinuclear antibodies in our patient argues against collagen disease vasculopathy. One previous case report described the sural nerve from a patient with tertiary LD, and it showed axonal changes and the deposition of membrane attack complexes in the blood vessels of the perineurium and epineurium.20 The findings are intriguing, and they raise the possibility of an autoimmune response seen in various immune-mediated polyneuropathies. Since there is no demonstrable direct invasion of the peripheral nerves by the spirochete in LNB cases, an immune-mediated mechanism remains a viable underlying pathology in the pathogenesis of peripheral neuropathy in LD.
The diagnosis of LD is primarily clinical.21,22 The treatment depends on the clinical history and the identification of its essential dermatological marker, erythema migrans, a rash that grows larger over a period of days or weeks following a tick bite. As the rash expands, the central part fades, creating a ring-like appearance or a “bull’s eye.” In areas endemic to LD, such a clinical presentation makes serological testing either optional or unnecessary. Nevertheless, understanding the evolution of the immunology of LD is crucial for the interpretation of the results of the serology of this disease, setting aside the standard assays and testing algorithms used in a university or specialty laboratory. Within 2 weeks following the appearance of the rash, detectable IgM levels usually appear, and a great majority would yield positive enzyme-linked immunosorbent assay results.23,24 The absence of detectable IgM levels in our patient would indicate that the disease had been ongoing for more than 2 weeks prior to the serological testing, and for more than a month to explain the positive IgG WB results.25 However, in patients with an early localized disease, testing is not recommended because the immune response may not be fully developed. In recent years, a confirmatory serological diagnosis has been based on a 2-tiered testing algorithm recommended by the Centers for Disease Control and Prevention25 and by the Canadian Public Health Laboratory Network.26
Conclusion
This is the first case report in the English literature of isolated FN, documented both clinically and electrophysiologically, that occurred in association with LD. It is analogous to facial nerve palsy as a presenting symptom of LD without the overt involvement of other cranial or peripheral nerves.
Abbreviation list
EMG, electromyography; FN, femoral neuropathy; LD, Lyme disease; LNB, Lyme neuroborreliosis; MRI, magnetic resonance imaging.
Ethical statement
This study was reviewed by the Advarra Institutional Review Board (IRB) of Columbia, Maryland on June 21, 2018. It was determined that this study does not constitute research under 45 CFR 46.102 (d); therefore, it does not require IRB approval. Written informed consent was obtained from the patient to publish his case history and any accompanying images.
Acknowledgment
This manuscript was edited by Scribendi Editing Services, Ontario, Canada.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Crossland NA, Alvarez X, Embers ME. Late disseminated Lyme disease: associated pathology and spirochete persistence posttreatment in rhesus macaques. Am J Pathol. 2018;188(3):672–682. doi:10.1016/j.ajpath.2017.11.005
2. Halperin JJ. Lyme disease and the peripheral nervous system. Muscle Nerve. 2003;28:133–147. doi:10.1002/mus.10337
3. Logigian EL. Peripheral nervous system Lyme borreliosis. Semin Neurol. 1997;17:25–29. doi:10.1055/s-2008-1040909
4. England JD, Bohm RP, Roberts ED, Philipp MT. Mononeuropathy multiplex in rhesus monkeys with chronic Lyme disease. Ann Neurol. 1997;41(3):375–384. doi:10.1002/ana.410410313
5. Reimers CD, Pongratz DE, Neubert U, et al. Myositis caused by Borrelia burgdorferi: report of four cases. J Neurol Sci. 1989;91:215–226.
6. Reimers CD, de Koning J, Neubert U, et al. Borrelia burgdorferi myositis: report of eight patients. J Neurol. 1993;240:278–283.
7. Holmgren AR, Matteson EL. Lyme myositis. Arthritis Rheum. 2006;54:2697–2700. doi:10.1002/art.22007
8. Stanek G, Klein J, Bittner R, Glogar D. Isolation of Borrelia burgdorferi from the myocardium of a patient with long-standing cardiomyopathy. N Engl J Med. 1990;322:249–252. doi:10.1056/NEJM199001253220407
9. Kuchynka P, Palacek T, Havranek S, et al. Recent-onset dilated cardiomyopathy associated with Borrelia burgdorferi infection. Herz. 2015;40(6):892–897. doi:10.1007/s00059-015-4308-1
10. Kubanek M, Sramko M, Berenova D, et al. Detection of Borrelia burgdorferi sensu lato in endomycardial biopsy specimens in individuals with recent-onset dilated cardiomyopathy. Eur J Heart Fail. 2012;14(6):588–596. doi:10.1093/eurjhf/hfs027
11. Cadavid D, Bai Y, Dail D, et al. Infection and inflammation in skeletal muscle from nonhuman primates infected with different gene species of the Lyme disease spirochete Borrelia burgdorferi. Infect Immun. 2003;71:7087–7098. doi:10.1128/iai.71.12.7087-7098.2003
12. Stewart JD. Focal Peripheral Neuropathies. New York: Raven Press; 1993.
13. Lazaro RP, Brinker RA, Weiss JJ, et al. Femoral and obturator neuropathy secondary to retroperitoneal hemorrhage: the value of the CT scan. Comput Tomogr. 1981;5:226–229. doi:10.1016/0363-8235(81)90005-3
14. Halperin JJ, Kuft BJ, Volkman DJ, et al. Lyme neuroborreliosis: peripheral nervous system manifestations. Brain. 1990;113:1207–1221. doi:10.1093/brain/113.4.1207
15. Logigian EL, Steere AC. Clinical and electrophysiologic findings in chronic neuropathy in Lyme disease. Neurology. 1992;42:303–311. doi:10.1212/wnl.42.2.303
16. Camponova F, Meier C. Neuropathy of vasculitic origin in a case of Garin-Bujadoux-Bannwarth Syndrome with positive Borrelia antibody response. J Neurol. 1986;233:69–72.
17. Hopf HC. Peripheral neuropathy in acrodermatitis chronica atrophicans. J Neurol Neurosurg Psychiatry. 1975;38:452–458. doi:10.1136/jnnp.38.5.452
18. Meier C, Grahmann F, Engelhardt A, Dumas M. Peripheral nerve disorders in Lyme borreliosis: nerve biopsy studies from eight cases. Acta Neuropathol (Berl). 1989;79:271–272. doi:10.1007/BF00294661
19. Kindstrand F, Nilsson BY, Hovmark A, et al. Polyneuropathy in late Lyme borreliosis—a clinical, neurophysiological, and morphological description. Acta Neurol Scand. 2000;101:47–52.
20. Maimone D, Villanova M, Stanta G, et al. Detection of Borrelia burgdorferi DNA and complement membrane attack complex deposits in the sural nerve of a patient with chronic polyneuropathy and tertiary Lyme disease. Muscle Nerve. 1997;20:969–975.
21. Centers for Disease Control and Prevention. Case definitions for infectious conditions under public health surveillance. MMWR Recomm Rep. 1997;46(RR–10):1–55.
22. Golightly MG. Lyme borreliosis: laboratory considerations. Semin Neurol. 1997;17(1):11–15. doi:10.1055/s-2008-1040907
23. Aguero-Rosenfeld ME, Nowakowski J, Bittker S, et al. Evolution of serologic response to Borrelia burgdorferi in treated patients with culture-confirmed erythema migrans. J Clin Microbiol. 1996;34:1–9.
24. Engstrom SM, Shoop E, Johnson RC. Immunoblot interpretation criteria for serodiagnosis of early Lyme disease. J Clin Microbiol. 1995;33:419–427.
25. Centers for Disease Control. Recommendation for test performance and interpretation from second national conference on serological diagnosis of Lyme disease. Morb Mortal Wkly Rep. 1996;45(23):481–484.
26. Public Health Laboratory Network. The laboratory diagnosis of Lyme borreliosis: guidelines from the Canadian Public Health Laboratory Network. Can J Infect Dis Med Microbiol. 2007;18(2):145–148. doi:10.1155/2007/495108
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.