Back to Journals » International Journal of Women's Health » Volume 18
Female Sexual Dysfunction and Irritable Bowel Syndrome: A Cross-Sectional Study in Jordanian Women
Authors Dwairi R ![]() , Al-Refu K, Al Tah B, Al Saraireh T, Al Dwairy M, Al-Qarawneh A, Abdelmoaty AA, Alsadik ME
, Al-Refu K, Al Tah B, Al Saraireh T, Al Dwairy M, Al-Qarawneh A, Abdelmoaty AA, Alsadik ME ![]() , Aborajooh E, Sawaqed F
, Aborajooh E, Sawaqed F ![]() , Al-Saraireh YM
, Al-Saraireh YM ![]()
Received 28 August 2025
Accepted for publication 29 January 2026
Published 6 February 2026 Volume 2026:18 563741
DOI https://doi.org/10.2147/IJWH.S563741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Rami Dwairi,1 Khitam Al-Refu,1 Basil Al Tah,2 Taif Al Saraireh,3 Majed Al Dwairy,4 Alaa Al-Qarawneh,5 Ahmed A Abdelmoaty,1,6 Maha E Alsadik,1,7 Emad Aborajooh,8 Fadi Sawaqed,9 Yousef M Al-Saraireh10
1Department of Internal and Forensic Medicine, Faculty of Medicine, Mutah University, Al-Karak, Jordan; 2Neurosurgery Department, Ibn Al-Haitham Hospital, Amman, Jordan; 3Department of General Surgery, Ministry of Health, Amman, Jordan; 4Department of Anesthesiology, Royal Medical Services, Amman, Jordan; 5Department of Obstetrics and Gynecology, Faculty of Medicine, Mutah University, Al-Karak, Jordan; 6Gastroenterology and Hepatology Department, Zagazig University, Zagazig, Egypt; 7Pulmonology Department, Zagazig University, Zagazig, Egypt; 8Department of General Surgery and Anesthesia, Faculty of Medicine, Mutah University, Al-Karak, Jordan; 9Department of Special Surgery, Faculty of Medicine, Mutah University, Al-Karak, Jordan; 10Department of Pharmacology, Faculty of Medicine, Mutah University, Al-Karak, Jordan
Correspondence: Rami Dwairi, Department of Internal and forensic medicine, Faculty of Medicine, Mutah University, P.O. Box 7, Al-Karak, 61710, Jordan, Tel +962799248184, Email [email protected]
Purpose: Female sexual function can be influenced by many somatic and psychosocial factors. Many chronic diseases, such as irritable bowel syndrome (IBS), can induce long-term suffering leading to a negative effect on sexual function. The impact of IBS on women’s sexual health is an underexplored area, particularly in Middle Eastern populations. The aim of this study is to compare the prevalence and domains of sexual dysfunction in Jordanian women with and without IBS.
Patients and Methods: This is a cross-sectional study, conducted at two hospitals in Jordan, from February to August 2024. 504 women, aged 18 or more, agreed to participate in this study, including 279 diagnosed with IBS. Our questionnaire incorporated clinical and sociodemographic data, relevant items of the Rome IV criteria, and the validated Arabic version of the Female Sexual Function Index (FSFI).
Results: Among 504 female participants (mean age 34.1 ± 10.7 years), 88.2% were found to have sexual dysfunction, defined as an FSFI score < 26.55, in the IBS group, and 76% in the non-IBS group, with an odds ratio of 2.354 (p < 0.001). IBS patients demonstrated significantly lower mean scores in most FSFI domains (desire, arousal, lubrication, orgasm, and satisfaction) and a lower total FSFI score (19.2 ± 9.9 vs 16.6 ± 10.2; p < 0.05 for all comparisons), while the pain domain did not differ significantly between the two groups. Logistic regression identified IBS as a statistically significant predictor of sexual dysfunction (p = 0.007).
Conclusion: IBS is associated with a higher prevalence of female sexual dysfunction in Jordan, which was demonstrated by lower scores in most sexual function domains. Our findings emphasize the need to integrate sexual health assessment as a part of IBS care. Future studies should explore the causality and the mechanism of this relationship.
Keywords: irritable bowel syndrome, female sexual health, sexual dysfunction, extraintestinal manifestations, female sexual function index
Introduction
Irritable bowel syndrome (IBS) is a functional gastrointestinal disorder with a prevalence range from 9 to 23% worldwide.1 The main feature of IBS is recurrent abdominal pain, along with a change in bowel habits, including diarrhea, constipation, or a combination of both, without structural abnormalities in the gastrointestinal tract. About half of IBS patients experience extraintestinal manifestations, which were reported more in female patients.2 The extraintestinal symptoms may include somatic pain, fatigue, sleep disturbances, psychiatric comorbidities, and sexual dysfunction.3–5 The presence of these manifestations is associated with increased severity of the gastrointestinal symptoms and lower quality of life.3 Despite their significance, limited research is currently available on extraintestinal manifestations of IBS.
One of the least investigated extraintestinal manifestations of IBS is sexual dysfunction. Sexual dysfunction is defined by the Fourth International Consultation on Sexual Medicine (ICSM) as the persistent problems encountered during any stage of the sexual cycle that restrict an individual’s ability to attain satisfaction from sexual activity.6 This includes sexual pain disorders such as dyspareunia, reduced sexual desire, problems achieving orgasm, and difficulties with arousal.
Globally, sexual dysfunction is a prominent concern impacting around 41% of women,7 with even higher prevalence in the Middle East; in Jordan, it has been reported in 64.7% of women aged 18–69 years.8
Several related mechanisms are thought to play a role in the development of sexual dysfunction noted in women with IBS, including pelvic floor dysfunction and visceral hypersensitivity.9,10 Visceral hypersensitivity is a complex phenomenon that can manifest within the peripheral or central nervous systems, thought to have a key role in the pathogenesis of IBS symptoms. A broad spectrum of molecules involved in the perception of visceral pain are considered appealing targets for novel treatments, aiming to improve IBS symptom profiles.10 Additionally, psychological stressors such as depression and anxiety can further worsen sexual difficulties.11,12
Studies have shown significant heterogeneity among the rates of sexual dysfunction in different groups, reflecting the diversity of available criteria for diagnosis and tools of assessment.7 Characteristics of study samples and their cultural context can substantially affect study outcomes, particularly in the presence of other somatic illnesses and psychologic conditions.13,14 Moreover, this wide variability might be attributed to the use of non-standardized sexual function assessment instruments or the utility of different diagnostic criteria for IBS, such as the Rome III and Rome IV criteria, for example. Multiple previous reports have focused on evaluating the overall prevalence of sexual dysfunction without systemic analysis of the specific domains of this issue.9,15
A systematic review by Sørensen et al revealed that while evidence indicates that IBS patients encounter more sexual issues than controls, our knowledge about sexual dysfunction in this population is limited and comes mainly from quality of life questionnaires.15 Evidence from previous reports suggests an increased rate of sexual dysfunction in people suffering from IBS when compared to the general population, but the extent and nature of these issues are still not clearly described, leaving an important knowledge gap to be investigated.
Persistent medical conditions, such as IBS, may have a disproportionate effect on sexual function in this setting by increased patient anxiety toward symptoms and impaired body image issues.16,17 Recurring psychosocial conditions frequently observed in patients with IBS, including stress, anxiety, and depression, often engage with cultural standards regarding marital roles and sexual attitudes and performance, which may result in further deterioration of sexual function.
Data on female sexual dysfunction in the Middle East region is particularly limited, being greatly influenced by societal norms. In many Middle Eastern societies, religious and cultural conventions greatly affect women’s ability to report sexual health-related problems and negatively impact health-seeking patterns, resulting in underestimation of this burden.18 The absence of structured services that provide women with sexual health consultation and support, combined with social constraints on open discussion of sexual concerns, further worsens the magnitude of the problem.19 Findings from western populations might not be readily generalizable in such populations, highlighting the importance of region-specific studies to better characterize the prevalence and severity of these issues.
Our study employed a cross-sectional design to examine the correlation between IBS and sexual dysfunction in Jordanian women, comparing overall and domain-specific female sexual function between women with and without IBS using the Rome IV criteria, which are an array of guidelines based on symptoms utilized by physicians and researchers to identify functional gastrointestinal disorders (FGIDs), also referred to as disorders of gut-brain interaction.20 Assessment of sexual dysfunction was achieved by using the validated Arabic version of the Female Sexual Function Index (FSFI), a self-assessment tool evaluating various domains of sexual function, including desire, arousal, lubrication, orgasm, satisfaction, and pain, which has been validated in Arabic-speaking populations.21,22
Materials and Methods
This is a cross-sectional study that was conducted from February to August 2024 at the gastroenterology unit of Al-Karak Teaching Hospital and Al-Basheer Hospital, both of which are teaching hospitals affiliated with the faculty of medicine at Mutah University in Jordan. These hospitals represent two distinct regions, the capital and a smaller city. We evaluated the relationship between IBS and FSD using the validated Arabic version of the FSFI.22 The Institutional Review Boards of Mutah University granted ethical approval (Approval No. 1352023).
The study population involved women aged 18 years and above with a diagnosis of IBS confirmed clinically by a gastroenterologist, with the exclusion criteria including current pregnancy, breastfeeding, confirmed diagnosis of other gastrointestinal or sexual disorders including inflammatory bowel disease, celiac disease, pelvic inflammatory disease, endometriosis, or sexually transmitted infections, being on a regular medication that could affect sexual function, such as antidepressants and antipsychotics, over the past 3 months, or the presence of known gynecological or urological conditions that could affect sexual function. The comparison group included community volunteers who satisfied the inclusion criteria and were identified as individuals who came for a routine clinic visit either as companions or visitors or those who came in for other unrelated issues.
Initially, we intended to employ random sampling to ensure that every participant within the target population had an equal likelihood of being selected. However, due to the sensitive nature of the topic and the clinical setting, convenience sampling was employed.
We used Epi Info™ software created by the Centers for Disease Control and Prevention (CDC) to calculate the necessary sample size for this study, assuming a 95% confidence level, 80% power, and an estimated prevalence of 50% of sexual dysfunction. The estimated minimum sample size needed was 384 participants; 504 women consented to participate.
Evaluation of FSD was achieved utilizing the validated Arabic version of the FSFI. Domain scores of the FSFI were calculated separately, along with the overall FSFI score, which ranges from 2 to 36, with scores of 26.55 or lower indicating sexual dysfunction.23 Noteworthy, even though this cut-off is widely accepted as a reliable benchmark, it was not specifically validated for Arabic-speaking populations and the possible cultural difference in the perception of sexual health was not considered.
Participants were approached during routine outpatient visits and informed about the study and its goals. It was explained to the participants that no personal information will be collected. Those who agreed were provided with a printed informed consent form, which they completed prior to answering the questionnaire. All questionnaires were completed in a private setting to ensure participant comfort and confidentiality. The questionnaire was administered in the form of a structured interview by female resident doctors currently specializing in internal medicine or gynecology, who underwent a special training for one week on sexual health history taking and administration of the study questionnaire to ensure that participants understood each question properly prior to answering it to reduce misunderstanding and reporting bias.
Descriptive statistics (SPSS V 30.0.0) were employed to describe demographic and clinical characteristics. The prevalence of FSD was determined based on FSFI scores. Continuous variable normality was tested using the Shapiro–Wilk test, which indicated that data was not normally distributed (p<0.001). Therefore, chi-square test and non-parametric Mann–Whitney tests were applied to examine associations between FSD and IBS, and r was used to estimate effect sizes, as well as socio-demographic variables. Binary logistic regression with sexual dysfunction being a dependent variable was performed to account for confounding factors including age, marital status, and comorbidities. A p-value of less than 0.05 was considered statistically significant.
Results
Sociodemographic Characteristic
A total of 504 women were included in the study, with participants stratified based on the presence or absence of IBS (Table 1). The age range of participants was between 18 and 72 years, with the mean age being 34.1 ± 10.7 years. Most participant at least completed high school, and the majority of the study participants hold a bachelor’s degree (45.4%, 229 cases), while others comprise individuals whohad variable degrees of education with post graduate degree holders comprising the lowest proportion (4.8%, 24). Moreover, most of the study participants were menstruating (88.9%, 448), while the rest were postmenopausal (11.1%, 56). Additionally, almost half of the participants were employed (50.8%, 256). There was no significant difference in the mean age, education level, menstrual status, and employment status between the IBS and non-IBS groups (p value > 0.05). Interestingly, there was a trend that individuals who are employed had IBS more than the unemployed participants, with an almost significant difference (p value = 0.096).
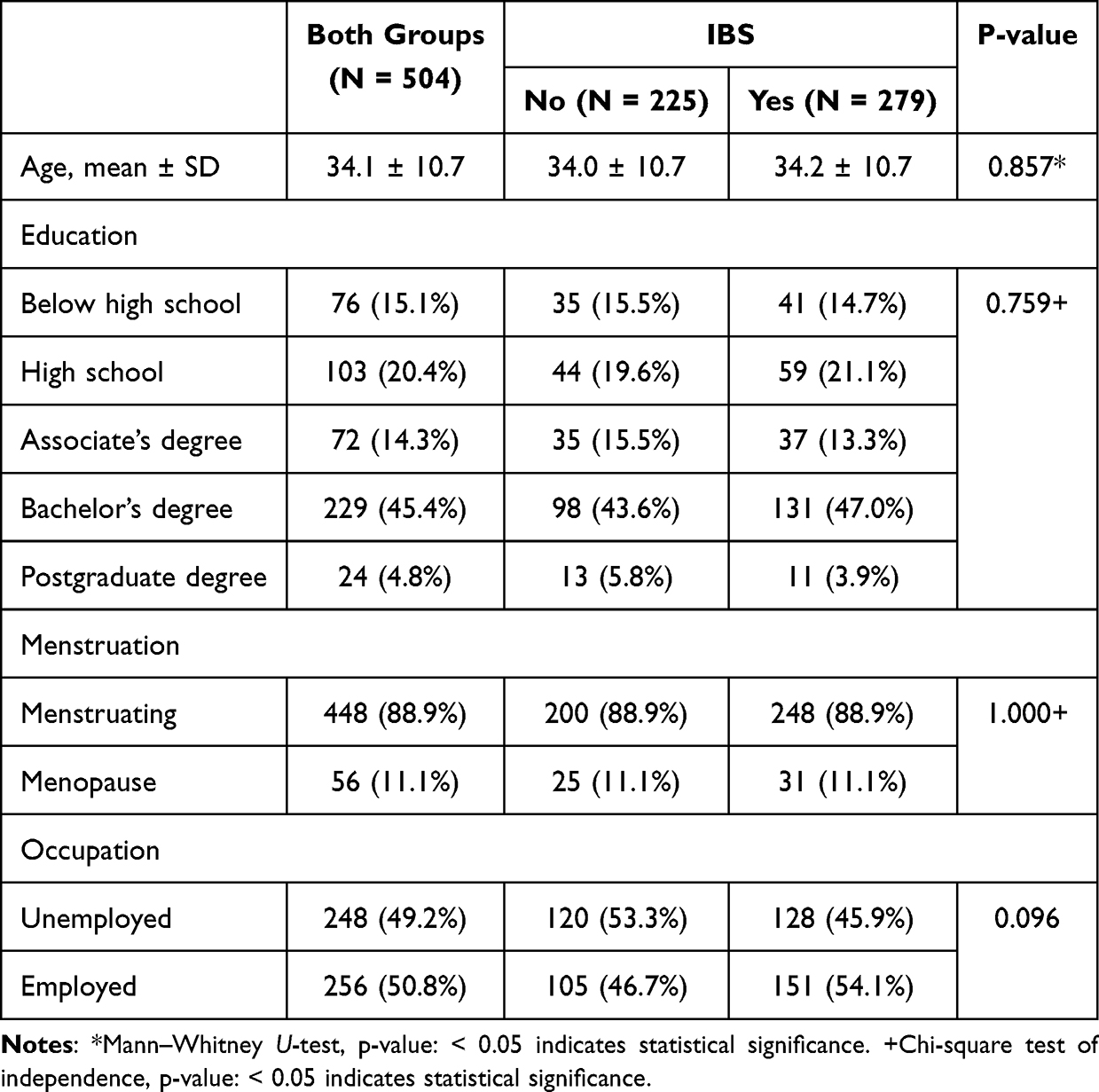 |
Table 1 Sociodemographic Table Showing Differences Between IBS and Non-IBS Population |
We wanted to test for potential confounders, so a binary logistic regression was applied to examine the association between different sociodemographic variables (age, marital status, comorbidities including hypertension and diabetes, and occupation) along with IBS and presence of sexual dysfunction. Interestingly, all factors did not demonstrate significant associations (all p-values >0.05), except for IBS which served as a statistically significant predictor of sexual dysfunction (p=0.007).
Influence of IBS on Sexual Function
Women with IBS exhibited lower scores in the majority of FSFI domains when compared with those without IBS, however effect sizes were generally small (Table 2). The desire score was rather decreased in the IBS group (2.6 ± 1.2) compared to the non-IBS group (2.8 ± 1.2; p = 0.012; r = −0.112). The arousal domain showed a difference between groups as the IBS group scored 2.4 ± 1.8, and the non-IBS group scored 2.9 ± 1.8 (p < 0.001; r = −0.164). The lubrication scores for the IBS group (2.8 ± 1.9) also exhibited lower scores compared to the non-IBS cohort (3.2 ± 1.9; p = 0.012; r = −0.112). The orgasm scores for IBS patients were also less (2.8 ± 2.0) than those for women who did not have IBS (3.3 ± 2.0; p = 0.004; r = −0.127). The satisfaction domain showed one of the largest differences, with the IBS group scoring 3.0 ± 2.2 versus 3.7 ± 2.1 in the non-IBS group (p < 0.001; r = −0.166). Conversely, the pain domain revealed no statistically significant difference across the two sets (P value 0.177; r = −0.060).
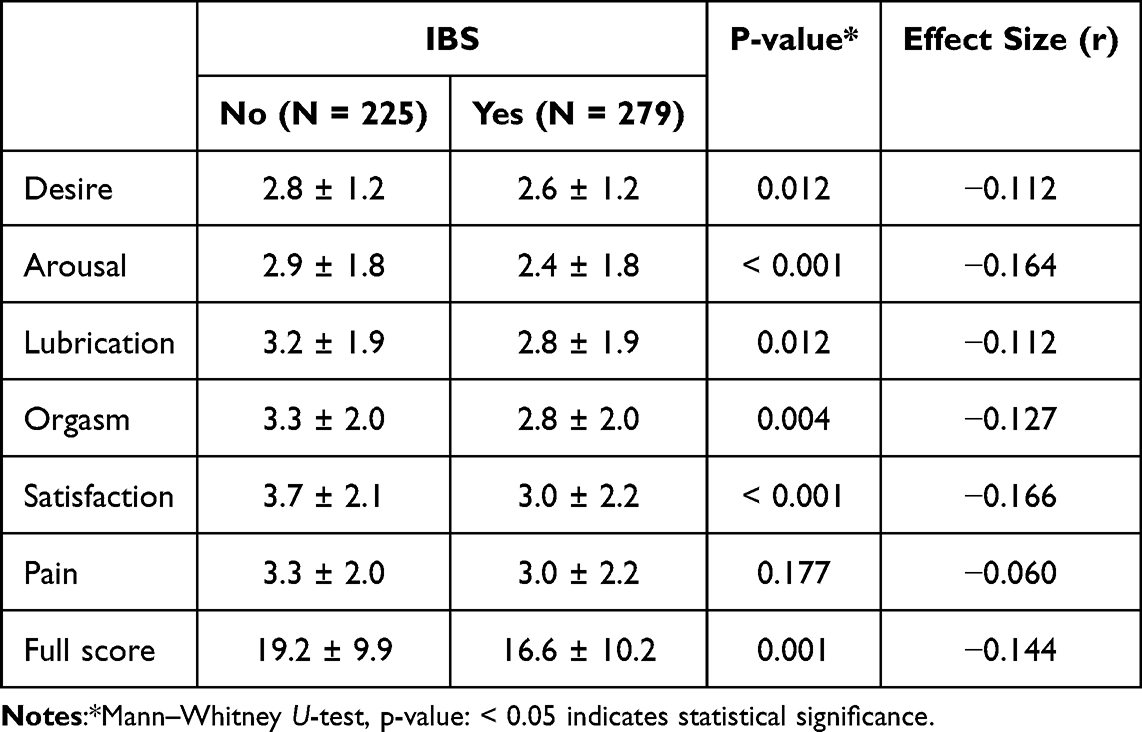 |
Table 2 Comparison Between IBS and Non-IBS Populations Regarding Different FSFI Domains |
The total FSFI score was also significantly lower among IBS participants (16.6 ± 10.2) compared with non-IBS participants (19.2 ± 9.9; p = 0.001; r = −0.144). Based on the FSFI cut-off (<26.55), sexual dysfunction was reported in 88.2% of IBS women versus 76.0% of non-IBS women (Table 3), corresponding to an odds ratio of 2.354 (95% CI: 1.464–3.785, p < 0.001). These differences are visually represented in Figure 1, which shows the domain-specific score reductions and the higher proportion of sexual dysfunction in the IBS group.
 |
Table 3 Comparison Between IBS and Non-IBS Populations Regarding FSFI Total Score |
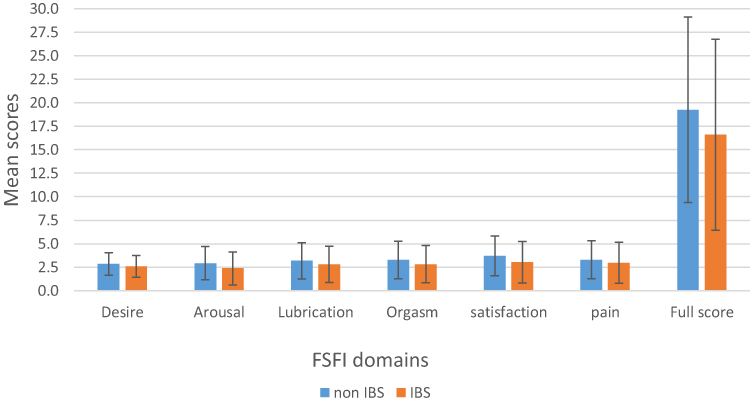 |
Figure 1 Mean FSFI domain scores for women with and without IBS. Error bars represent standard deviation (SD). Statistical comparisons were performed using the Mann–Whitney U-test. |
Sexual Function by Employment Status
On the basis of the trend shown on the increasing prevalence of IBS among the employed participants, we conducted an exploratory subgroup analysis for the employed participants comparing the IBS and non-IBS individuals and for the unemployed individuals to compare the same aspects (Table 4). Although the increase in IBS prevalence showed a non-significant trend, we conducted this analysis due to the clinical relevance of employment potentially altering the relationship between IBS and sexual dysfunction.
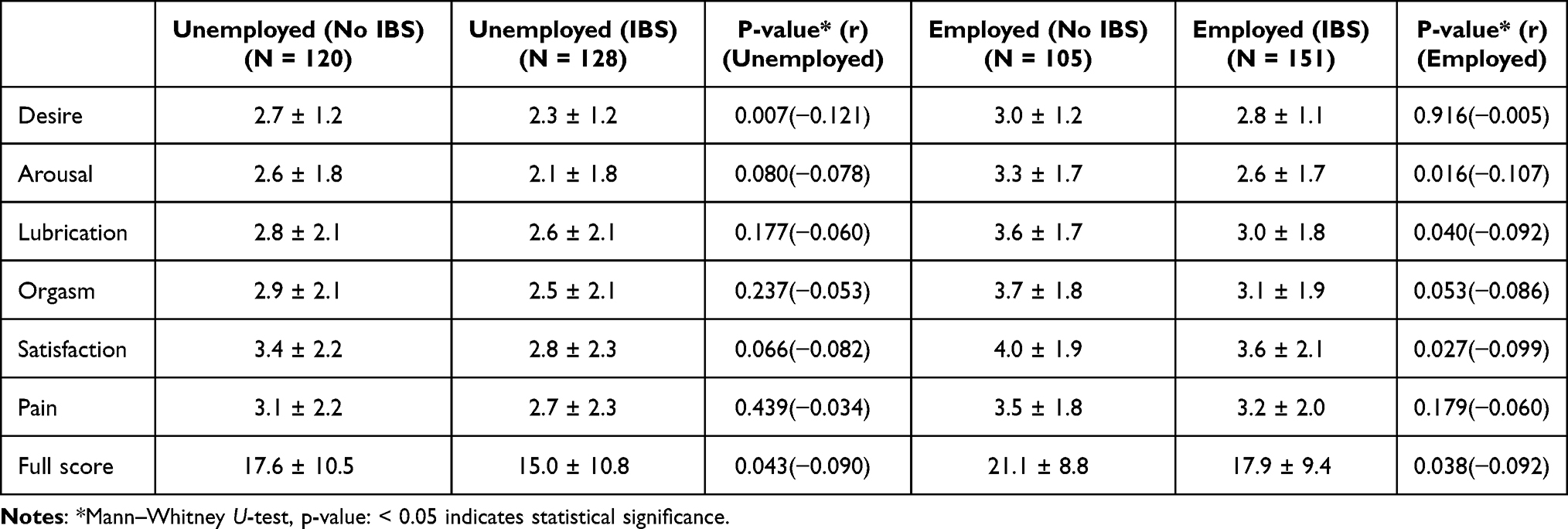 |
Table 4 Subgroup Analysis of FSFI Scores by Employment Status Comparing the IBS and Non-IBS Individuals |
Among unemployed participants, women with IBS showed lower mean scores in the desire domain (2.3 ± 1.2 vs 2.7 ± 1.2; p = 0.007) of FSFI as well as the full score (15.0 ± 10.8 vs 17.6 ± 10.5; p = 0.043) compared to their non-IBS counterparts. On the other hand, the sexual function scores among the employed participants with and without IBS were examined. Likewise, employed participants with IBS had particularly lower scores in several FSFI domains compared to their non-IBS counterparts, with some difference in domains. Notably, the IBS group had significantly lower scores in arousal (2.6 ± 1.7 vs 3.3 ± 1.7; p = 0.016), lubrication (3.0 ± 1.8 vs 3.6 ± 1.7; p = 0.040), orgasm (3.1 ± 1.9 vs 3.7 ± 1.8; p = 0.053), and satisfaction (3.6 ± 2.1 vs 4.0 ± 1.9; p = 0.027). There was no substantial variation observed in the desire and pain domains. The IBS group had a total FSFI score that was much lower (17.9 ± 9.4) than the non-IBS group (21.1 ± 8.8; p = 0.038). Taking effect sizes into account, IBS appears to negatively impact sexual function albeit a small effect, regardless of occupation status.
Correlation Between Age and Sexual Function
The Spearman correlation analysis between participants’ age and the different domains of the FSFI, including the total score (Table 5). Interestingly, a noteworthy positive link was identified between pain during sexual activity and the participants’ age (r = 0.240, p < 0.001), although this correlation could be clinically negligible. There were no significant correlations between age and the other FSFI domains.
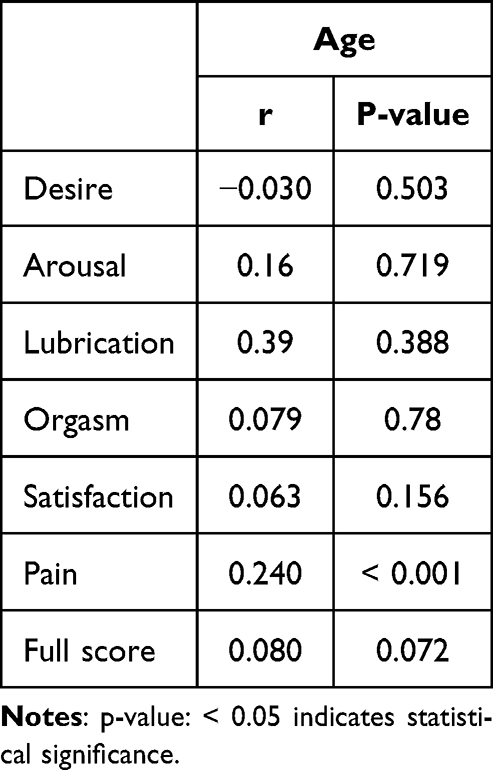 |
Table 5 Spearman Correlation for FSFI Domains and Total Score with Participants’ Age |
Discussion
Many studies have investigated the effects of IBS on human body systems;2 however, reports discussing sexual function in women from Middle Eastern populations are still limited. To our knowledge, this is the first study examining sexual function in Jordanian women with IBS despite it being one of the major cultural barriers. Our results revealed that IBS was associated with lower scores across multiple FSFI domains when compared to women without IBS, corroborating prior research that highlighted the relationship between IBS and impairment of sexual health.
In our study we found that the prevalence of sexual dysfunction, defined as an FSFI score <26.55, was high in both groups, with higher rates observed in women with IBS. These findings align with previous literature that demonstrates comparable impairment in sexual function among IBS patients.15 Even with the significant impact on quality of life, sexual health issues are often inadequately handled in clinical practice; this is a direct reason calling for further investigation on this topic.
Women with IBS frequently report psychological and physical symptoms related to this condition, which can be associated with a reduction in sexual desire and satisfaction.15,24 The significantly lower FSFI scores in areas such as arousal and satisfaction in our IBS cohort further reflect the chronic and distressing nature of IBS with decreased sexual function, rather than establish a causal relationship.
Subgroup analysis on our cohort showed that employed women with IBS reported lower FSFI scores compared to employed women without IBS, mainly in the satisfaction, arousal, orgasm, and lubrication domains. One possible explanation of this observation is the added stress of work that might worsen IBS symptoms, further worsening the sexual function.25 Workplace stress, limited time for intimacy, societal expectations, and role strain may excessively affect employed women in conservative societies, which may exacerbate the adverse effects of IBS on the mood and mental wellness, also worsening the sexual desire and function.26,27 Notably, chronic stress is known to worsen all the manifestations of IBS, disregarding the source of stress.28
Being employed seems to introduce additional stressors on psychosocial levels, such as conflicts between family and work, time pressure, and overload of responsibility, which might exert further pressure on different quality of life aspects, including sexual life. Previous reports highlighted the contribution of employment and job-related stresses to sexual health challenges, manifesting as difficulties in dealing with job demands along with family responsibilities and intimate needs and impacting elements of sexual life.29 Documented literature frequently describes stress as an important risk factor for sexual dysfunction in females in addition to other psychosocial factors such as anxiety or depression.30
The results of our study are broadly consistent with the results of Slawik et al, which illustrated that the prevalence of sexual dysfunctions was higher in women with IBS (48%) in comparison to healthy controls (23%) with a significant reduction in both the overall FSFI score and all of its specific domains.31 Furthermore, these outcomes agreed with the findings of Mahran et al, which demonstrated that women with IBS had significantly lower scores in both the total FSFI score and its specific domains, with the exception of the lubrication domain.32 The similarities observed in these geographically distinct populations are suggestive of a reproducible link between IBS and certain aspects of normal sexual function, though the degree of impairment may vary across different settings.
In comparing our findings to international literature, the prevalence of FSD in both IBS and non-IBS groups in the Jordanian sample was notably high, which is equal to or somewhat higher than rates observed in prior reports, where prevalence estimates range from 70% to 90%.32–34 Such results may suggest cultural implications on the reporting of sexual symptoms, including potential reporting barriers, differences in healthcare-seeking behavior, and limited openness on sexual health issues, which may have an influence on women’s interpretation and response to different sexual function assessment tools. Additionally, cut-off values for the FSFI were developed in western populations. The application of these values in Middle Eastern populations is not yet well established, which may contribute to elevated prevalence estimates.
A number of processes have been proposed to explain these observations, as IBS and sexual health are linked through physical, psychological, hormonal, and social factors.9
Psychological aspects like depression, anxiety, and negative body image, which are also common in IBS, are frequently associated with impaired sexual function.11,35 Literature also mentions that sex hormones, and more particularly ovarian hormones, modulate IBS symptoms and may influence pain perception, stress response, and gut function.24
The gut-brain axis, which is influenced by sex steroids, plays a role in regulating visceral sensitivity and psychological conditions that link IBS to sexual health.36 Moreover, alterations in gut hormonal regulation, including serotonin, motilin, and peptide YY, which are involved in regulating sexual function, are established to be prevalent in patients with IBS.37
The Rome IV criteria classifies IBS patients according to their predominant bowel habit pattern into three subtypes: diarrhea predominant (IBS-D), constipation predominant (IBS-C), and mixed (IBS-M) subtypes.20 Previous studies illustrated that these subtypes are distinguishable for their impact on different aspects of quality of life, in addition to their different gastrointestinal symptom profiles.35,38 Prior reports have shown that individuals with IBS-D and IBS-M subtypes were found to have lower quality of life measures in comparison to patients categorized as having the IBS-C subtype in terms of the effect on social functioning and normal daily activities; suffering that may potentially influence sexual function indirectly.39 This possible association between various aspects of quality of life, including sexual health, and different subtypes of IBS needs further research for a better understanding and clarification.
Prior studies from other Middle Eastern countries, where social standards and inadequate sexual health education may lead to failure to report such complaints, demonstrated comparable outcomes.18,40 High rates of sexual health issues observed in women suffering from IBS warrants routine sexual function assessment along with the medical care of IBS patients, aiming to implement a multidisciplinary approach that involves gastroenterologists, mental health professionals, and gynecologists.6,9
Training of healthcare providers to address sexual complaints is essential to enable them to evaluate such issues in a culturally respectful and sensitive way, especially in communities where open discussion of these topics is considered taboo. Additionally, psychological support and stress management programs should be incorporated into the management plans of IBS patients to help lessen the emotional toll and improve quality of life.28
The pain domain in our sample did not exhibit a significant difference between IBS and non-IBS groups, despite the fact that women with IBS showed significantly lower scores across several domains of sexual function. Assessment of sexual pain by the FSFI primarily reflects discomfort during or after vaginal penetration, which might not be consistent with visceral pain that is usually encountered in patients with IBS. Another factor that may have a role in explaining this observation is the influence of gynecological conditions and female hormonal status on pain during sexual activity, which were not specifically assessed despite their effect on both study groups.41,42 On the other hand, a positive correlation between age and pain during sexual activity was identified. This might suggest that sexual pain is more strongly influenced by age-related changes rather than IBS effects.43,44 Factors such as pelvic floor disorders and vaginal atrophy, which both increase with age, can be major contributors to increased dyspareunia in older women.45 The observed negative correlation between patient’s age and sexual desire is consistent with age-related changes that are well established in the literature.46,47
Sexual dysfunction in women of all ages remains a significant, yet under-evaluated, health aspect that greatly impacts quality of life. Evaluating sexual dysfunction as part of the scope of IBS treatment may enhance patient-related outcomes and help understand the complex factors involved in the pathology and manifestations of IBS through further structured research.
Several confounding factors were not considered in our work, including psychological and social factors such as anxiety, depression, and relationship satisfaction. The cross-sectional design employed limits the ability to infer a causal relationship between IBS and sexual dysfunction and allows only for the establishment of associations. While participant recruitment happened to be from two hospitals in two different regions aiming at increasing regional diversity and enhancing the representativeness of our sample, it is important to acknowledge that this can also limit the generalizability of the study findings to the Jordanian population as a whole.
Cultural barriers in this society may also have led to underreporting of sexual symptoms. IBS severity and specific subtypes of IBS and their association with variable patterns of sexual dysfunction were not evaluated. Use of FSFI cut-offs established in culturally different populations is broadly unclear and might limit their applicability to Middle Eastern populations and could influence interpretation of results.
Conclusion
Sexual dysfunction appears to affect a high percentage of Jordanian women and even a higher proportion of women suffering from IBS, who had more than twice the odds of experiencing sexual dysfunction compared to women without IBS (odds ratio = 2.354), highlighting the importance of routine evaluation of sexual health in patients with IBS. Healthcare professionals should be trained to use assessment tools, like the FSFI, adopting a team-based approach including gastroenterologists, gynecologists, primary care physicians, and psychosocial workers aiming to promote communication and enhance patient outcomes.
Clarification and explanation of the causal relationships between IBS and FSD through future research, including longitudinal studies, is essential to create a better understanding of these relations, as the findings of this study present associations between IBS and sexual dysfunction rather than a causal relationship.
Abbreviations
IBS, Irritable Bowel Syndrome; FSD, Female Sexual Dysfunction; FSFI, Female Sexual Function Index; IBS-D, Diarrhea Predominant Irritable Bowel Syndrome; IBS-C, Constipation Predominant Irritable Bowel Syndrome; IBS-M, Mixed Irritable Bowel Syndrome.
Data Sharing Statement
Data will be available from the corresponding author upon reasonable request.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Mutah University Institutional Review Boards (Approval No. 1352023). Informed consent was acquired from all participants, and data was anonymized before analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saha L. Irritable bowel syndrome: pathogenesis, diagnosis, treatment, and evidence-based medicine. World J Gastroenterol. 2014;20(22):6759–11. doi:10.3748/wjg.v20.i22.6759
2. Ohlsson B. Extraintestinal manifestations in irritable bowel syndrome: a systematic review. Therap Adv Gastroenterol. 2022;15:17562848221114558. doi:10.1177/17562848221114558
3. Whorwell PJ. Diagnosis and management of irritable bowel syndrome: discussion paper. J R Soc Med. 1989;82(10):613–614. doi:10.1177/014107688908201017
4. Mayer EA, Ryu HJ, Bhatt RR. The neurobiology of irritable bowel syndrome. Mol Psychiatry. 2023;28(4):1451–1465. doi:10.1038/s41380-023-01972-w
5. Abdoly M, Esmaeeli B. (027) The prevalence of female sexual dysfunction in patients with irritable bowel syndrome (IBS). J Sexual Med. 2024;21(Supplement_2). doi:10.1093/jsxmed/qdae002.027
6. McCabe MP, Sharlip ID, Atalla E, et al. Definitions of sexual dysfunctions in women and men: a consensus statement from the fourth international consultation on sexual medicine 2015. J Sex Med. 2016;13(2):135–143. doi:10.1016/j.jsxm.2015.12.019
7. Ramírez-Santos J, Cristóbal-Cañadas D, Parron-Carreño T, Lozano-Paniagua D, Nievas-Soriano BJ. The problem of calculating the prevalence of sexual dysfunction: a meta-analysis attending gender. Sex Med Rev. 2024;12(2):116–126. doi:10.1093/sxmrev/qead058
8. Maaita ME, Khreisat BM, Tasso OA, Otom NN, Aljaafreh BM, Abuassaf GM. Prevalence and associated risk factors of female sexual dysfunction among Jordanian women. J Family Med Prim Care. 2018;7(6):1488–1492. doi:10.4103/jfmpc.jfmpc_200_18
9. Hacker KS, Bedell A, Hachem C, Velez C, Patel D. Reproductive and sexual health concerns in gastrointestinal illness: a narrative review. Translat Gastroenterol Hepatol. 2024;9:10. doi:10.21037/tgh-23-59
10. Farzaei MH, Bahramsoltani R, Abdollahi M, Rahimi R. The role of visceral hypersensitivity in irritable bowel syndrome: pharmacological targets and novel treatments. J Neurogastroenterol Motil. 2016;22(4):558–574. doi:10.5056/jnm16001
11. Keshavarzi A, Talebi SS, Ahmadpanah M, Soltanian A, Torkashvand S. Sexual function, depression, and quality of life in patients with irritable bowel syndrome. BMC Gastroenterol. 2025;25(1):504. doi:10.1186/s12876-025-04102-8
12. Kırat S. Sexual dysfunction in the life cycle of women: implications for psychological health. Healthcare. 2025;13(11):1268. doi:10.3390/healthcare13111268
13. Santos-Iglesias P, Mohamed B, Walker LM. A systematic review of sexual distress measures. J Sex Med. 2018;15(5):625–644. doi:10.1016/j.jsxm.2018.02.020
14. Mitchell KR, Jones KG, Wellings K, et al. Estimating the prevalence of sexual function problems: the impact of morbidity criteria. J Sex Res. 2016;53(8):955–967. doi:10.1080/00224499.2015.1089214
15. Sørensen J, Schantz Laursen B, Drewes AM, Krarup AL. The incidence of sexual dysfunction in patients with irritable bowel syndrome. Sex Med. 2019;7(4):371–383. doi:10.1016/j.esxm.2019.08.010
16. Geller S, Levy S, Avitsur R. Psychological distress in individuals with irritable bowel syndrome: the roles of body image and self-criticism. Health Psychol Behav Med. 2024;12(1):2334466. doi:10.1080/21642850.2024.2334466
17. Sobel T, David P. Impact of chronic medical disease on sexual function and other conditions. Obstet Gynecol Clin North Am. 2024;51(2):323–340. doi:10.1016/j.ogc.2024.02.006
18. Zakhour S, Gonçalves W, Sardinha A, Levitan M, Nardi AE. A systematic review on the prevalence of a silent female disorder in Arabic-speaking countries and the Middle East: sexual dysfunctions and the role of culture. Sex Med Rev. 2025;13(1):62–78. doi:10.1093/sxmrev/qeae070
19. Elsayed R, Zembe-Mkabile W. Women’s access to sexual and reproductive health services and information in Ismailia, Egypt. BMC Womens Health. 2024;24(1):163. doi:10.1186/s12905-024-02986-4
20. Drossman DA, Hasler WL. Rome IV-Functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257–1261. doi:10.1053/j.gastro.2016.03.035
21. Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–208. doi:10.1080/009262300278597
22. Anis TH, Gheit SA, Saied HS, Al Kherbash SA. Arabic translation of female sexual function index and validation in an Egyptian population. J Sex Med. 2011;8(12):3370–3378. doi:10.1111/j.1743-6109.2011.02471.x
23. Wiegel M, Meston C, Rosen R. The female sexual function index (FSFI): cross-validation and development of clinical cutoff scores. J Sex Marital Ther. 2005;31(1):1–20. doi:10.1080/00926230590475206
24. Cigna S. Irritable bowel syndrome and female sexual dysfunction. In: Female Sexual Pain Disorders. 2020:359–366.
25. Mües HM, Markert C, Feneberg AC, Nater UM. Too stressed for sex? Associations between stress and sex in daily life. Psychoneuroendocrinology. 2025;181:107583. doi:10.1016/j.psyneuen.2025.107583
26. Hosseini Z, Rahimi SF, Salmani F, Miri MR, Aghamolaei T, Dastjerdi R. Etiology, consequences, and solutions of working women’s work-life conflict: a qualitative study. BMC Womens Health. 2024;24(1):62. doi:10.1186/s12905-023-02873-4
27. Zhou S, Da S, Guo H, Zhang X. Work-Family conflict and mental health among female employees: a sequential mediation model via negative affect and perceived stress. Front Psychol. 2018;9:544. doi:10.3389/fpsyg.2018.00544
28. Chang L. The role of stress on physiologic responses and clinical symptoms in irritable bowel syndrome. Gastroenterology. 2011;140(3):761–765. doi:10.1053/j.gastro.2011.01.032
29. Abadian K, Keshavarz Z, Milani HS, Hamdieh M, Nasiri M. Exploring Iranian married working women’s experiences regarding sexual health challenges. J Educ Health Promot. 2021;10:121. doi:10.4103/jehp.jehp_922_20
30. McCool-Myers M, Theurich M, Zuelke A, Knuettel H, Apfelbacher C. Predictors of female sexual dysfunction: a systematic review and qualitative analysis through gender inequality paradigms. BMC Womens Health. 2018;18(1):108. doi:10.1186/s12905-018-0602-4
31. Sławik P, Szul M, Fuchs A, Waluga M, Krzystanek M. Could problems in the bedroom come from our intestines? A preliminary study of IBS and its impact on female sexuality. Psychiatry Danub. 2019;31(Suppl 3):561–567.
32. Mahran AM, Sabry AMM, Ghadour AA, Ibrahiem IA, Hosny A. Evaluation of sexual function in Egyptians with irritable bowel syndrome: a case-control study. Int J Med Arts. 2024;6(7):4620–4626. doi:10.21608/ijma.2024.290326.1973
33. Heshmatnia F, Azizi M, Milani H, et al. Prevalence and correlates of female sexual dysfunction and sexual distress in reproductive-aged women: a systematic review and meta-analysis. BMC Womens Health. 2025;25(1):451. doi:10.1186/s12905-025-03960-4
34. Rivière P, Zallot C, Desobry P, et al. Frequency of and factors associated with sexual dysfunction in patients with inflammatory bowel Disease. J Crohns Colitis. 2017;11(11):1347–1352. doi:10.1093/ecco-jcc/jjx100
35. Roohafza H, Bidaki EZ, Hasanzadeh-Keshteli A, Daghaghzade H, Afshar H, Adibi P. Anxiety, depression and distress among irritable bowel syndrome and their subtypes: an epidemiological population based study. Adv Biomed Res. 2016;5(1):183. doi:10.4103/2277-9175.190938
36. So SY, Savidge TC. Sex-Bias in irritable bowel syndrome: linking steroids to the gut-brain axis. Front Endocrinol. 2021;12:684096. doi:10.3389/fendo.2021.684096
37. El-Salhy M, Hatlebakk JG, Hausken T. Possible role of peptide YY (PYY) in the pathophysiology of irritable bowel syndrome (IBS). Neuropeptides. 2020;79:101973. doi:10.1016/j.npep.2019.101973
38. Pereyra F, Bustos Fernández LM, Schlottmann F, et al. Prevalence of extra-intestinal symptoms according to irritable bowel syndrome subtype. Neurogastroenterol Motil. 2024;36(7):e14796. doi:10.1111/nmo.14796
39. Singh P, Staller K, Barshop K, et al. Patients with irritable bowel syndrome-diarrhea have lower disease-specific quality of life than irritable bowel syndrome-constipation. World J Gastroenterol. 2015;21(26):8103–8109. doi:10.3748/wjg.v21.i26.8103
40. AlShamlan NA. Breaking the silence on female sexual dysfunction in Saudi Arabia: a narrative review of barriers to women’s health services in primary care. Middle East Fertil Soc J. 2025;30(1):24. doi:10.1186/s43043-025-00239-4
41. Beckman A, Moss C, Goldstein AT. Evaluation and treatment of sexual pain disorders. Clin Obstet Gynecol. 2025;68(1):21–31. doi:10.1097/GRF.0000000000000909
42. Zhu X, Wu Y, Jia J, Zhao X, Zhao X. Impact of endometriosis on female sexual function: an updated systematic review and meta-analysis. Sex Med. 2023;11(2):qfad026. doi:10.1093/sexmed/qfad026
43. Pérez-Herrezuelo I, Aibar-Almazán A, Martínez-Amat A, et al. Female sexual function and its association with the severity of menopause-related symptoms. Int J Environ Res Public Health. 2020;17(19):7235. doi:10.3390/ijerph17197235
44. Liang B, Xu C, Wang B, et al. Sexual response problems and their correlates among older adults from the Sexual Well-Being (SWELL) study in china: multicenter cross-sectional study. JMIR Aging. 2025;8:e66772.
45. Kingsberg SA, Wysocki S, Magnus L, Krychman ML. Vulvar and vaginal atrophy in postmenopausal women: findings from the REVIVE (REal women’s views of treatment options for menopausal vaginal changEs) survey. J Sex Med. 2013;10(7):1790–1799. doi:10.1111/jsm.12190
46. Athey RA, Kershaw V, Radley S. Systematic review of sexual function in older women. Eur J Obstet Gynecol Reprod Biol. 2021;267:198–204. doi:10.1016/j.ejogrb.2021.11.011
47. Hayes R, Dennerstein L. The impact of aging on sexual function and sexual dysfunction in women: a review of population‐based studies. J Sexual Med. 2005;2(3):317–330. doi:10.1111/j.1743-6109.2005.20356.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.