Back to Journals » Drug Design, Development and Therapy » Volume 20
Feedback-Regulated versus Constant-Rate Sufentanil Patient-Controlled Analgesia for Postoperative Nausea and Vomiting After Laparoscopic Myomectomy: A Randomized Controlled Trial
Authors Ma Q, Wang M, Zhang W, Chen L, Guo X ![]() , Mei Z
, Mei Z ![]() , Ma T
, Ma T
Received 20 January 2026
Accepted for publication 10 April 2026
Published 23 April 2026 Volume 2026:20 597391
DOI https://doi.org/10.2147/DDDT.S597391
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Qian Ma, Mingming Wang, Weiqiao Zhang, Linfang Chen, Xiaowen Guo, Zhong Mei, Ting Ma
Department of Anesthesiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, 310003, People’s Republic of China
Correspondence: Zhong Mei, Department of Anesthesiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected] Ting Ma, Department of Anesthesiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected]
Background: Postoperative nausea and vomiting (PONV) remains a common and distressing side effect of opioid-based patient-controlled analgesia (PCA). Although continuous background infusion stabilizes analgesia, it often induces excessive opioid exposure and related adverse events. This study evaluates a novel smart PCA system featuring feedback-regulated background infusion (FRBI) designed to dynamically adjust opioid delivery based on real-time pain feedback, aiming to reduce PONV without compromising analgesia.
Methods: In this prospective, randomized, controlled, single-center trial, 132 patients undergoing laparoscopic myomectomy were assigned in a 1:1 parallel-group design to either constant-rate background infusion (CRBI) at 2 mL/h (Group A) or FRBI with adjustable rates of 1– 4 mL/h (Group B). Both groups received a standardized sufentanil–flurbiprofen solution via PCA. The FRBI algorithm dynamically adjusted the infusion rate: a 20% increase was triggered by ≥ 2 bolus demands within 30 minutes, and a 20% decrease followed 4 consecutive demand-free hours. The primary outcome was the incidence of PONV (defined as nausea and/or vomiting) within 48 hours postoperatively. Secondary outcomes included pain scores (NRS), total opioid consumption, occurrence of other adverse events, and patient satisfaction.
Results: The FRBI group demonstrated a significantly lower incidence of PONV (nausea and/or vomiting) compared to the CRBI group (41.7% vs 62.7%, risk difference: − 21.0% [95% CI: − 38.1% to − 3.9%]; risk ratio: 0.66 [95% CI: 0.46 to 0.96], P = 0.022). Total sufentanil consumption was reduced by approximately 30% in the FRBI group (P < 0.01). Pain scores were comparable between groups at all time points. Patient satisfaction was significantly higher in the FRBI group (P < 0.01). No cases of respiratory depression were observed in either group.
Conclusion: The feedback-regulated background infusion mode significantly reduces the incidence of PONV and total opioid consumption while maintaining effective analgesia in patients undergoing laparoscopic myomectomy. This strategy suggests a favorable safety profile in this specific surgical population and may represent a promising strategy for opioid-sparing analgesia. Further studies are needed to validate these findings in broader patient populations and to assess economic feasibility.
Keywords: patient-controlled analgesia, feedback-regulated infusion, postoperative nausea and vomiting, opioid reduction, smart pump, laparoscopic myomectomy
Background
Uterine myoma is one of the most prevalent benign tumors in women of reproductive age, with laparoscopic myomectomy (LM) being a standard minimally invasive surgical treatment.1 Effective postoperative pain management is crucial for recovery,2 and intravenous patient-controlled analgesia (IV-PCA) with opioids—particularly sufentanil—remains a cornerstone for moderate to severe pain.3 However, opioid-based analgesia is frequently associated with dose-dependent adverse effects,4 among which postoperative nausea and vomiting (PONV) represents a major clinical challenge, occurring in 30–80% of high-risk patients and leading to prolonged hospitalization, increased costs, and reduced patient satisfaction.5–7 The 2020 PONV consensus guidelines emphasize the importance of multimodal prophylaxis and risk stratification using the Apfel score.8
Conventional IV-PCA often employs a constant-rate background infusion (CRBI) to maintain baseline analgesia. While effective in pain control, this fixed-rate paradigm lacks responsiveness to dynamic pain states and often results in unnecessary opioid accumulation, thereby exacerbating side effects such as PONV, dizziness, and respiratory depression.9 Current guidelines, including those from the American Pain Society, advise against routine continuous background infusion due to its association with increased opioid-related complications.10
Several studies have explored variable-rate or closed-loop PCA systems to optimize opioid delivery. Early investigations demonstrated that demand-driven algorithms could reduce total opioid consumption compared to fixed-rate infusions,11,12 but these systems often required complex external monitoring or were not widely adopted. More recently, smart infusion pumps with embedded feedback algorithms have emerged, allowing automatic adjustment of background infusion rates based on real-time patient demand patterns. However, clinical evidence validating their efficacy in reducing opioid-related adverse events, particularly PONV, remains limited.13
Enhanced Recovery After Surgery (ERAS) guidelines strongly advocate for opioid-sparing analgesic strategies to minimize opioid-related adverse effects and promote early recovery.14 Within this framework, optimizing PCA delivery through dynamic feedback systems represents a promising approach to align drug administration with individual patient needs.
To date, few clinical studies have evaluated whether such a demand-responsive PCA system can meaningfully reduce opioid-induced side effects without compromising analgesia. This study therefore investigates the impact of a smart PCA pump with FRBI capability, compared to conventional CRBI, on the incidence of PONV and other opioid-related adverse events in patients undergoing laparoscopic myomectomy. We hypothesize that FRBI mode not only provides equivalent analgesia but also significantly decreases sufentanil consumption and PONV incidence, supporting a drug-delivery optimization strategy consistent with ERAS principles.
Materials and Methods
Study Design and Ethical Approval
This prospective, randomized, controlled, single-center trial was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of The First Affiliated Hospital of Zhejiang Chinese Medical University (Approval No: 2024-KLS-661-02). The study was prospectively registered at the Chinese Clinical Trial Registry (Registration number: ChiCTR2500100820). Written informed consent was obtained from all participants prior to enrollment.
Participants
Female patients aged 18–70 years, classified as American Society of Anesthesiologists (ASA) physical status I or II, and scheduled for elective laparoscopic myomectomy were eligible for inclusion. Exclusion criteria were: a history of chronic obstructive pulmonary disease or significant brain injury; known allergy or contraindication to sufentanil or flurbiprofen; chronic opioid or sedative abuse; renal or hepatic insufficiency; and an inability to understand or operate the PCA device. Participants could be withdrawn for analgesic pump failure, a Ramsay sedation score >4, or the occurrence of respiratory depression.
Randomization and Blinding
Eligible patients were randomly assigned in a 1:1 ratio to one of two IV-PCA groups using a computer-generated randomization sequence. The allocation was concealed in sequentially numbered, opaque, sealed envelopes. An anesthesia nurse, not involved in patient assessment or data collection, opened the envelopes and programmed the PCA pump according to the assigned group. The pumps were identical in appearance. Patients, surgeons, postoperative assessors, and data analysts were blinded to group allocation.
Study Interventions and Anesthesia Protocol
All patients received standardized general anesthesia. Induction was achieved with intravenous propofol (1.5 mg/kg) (Fresenius Kabi Austria GmbH), cis-atracurium (0.2 mg/kg), and sufentanil (0.3 μg/kg) (Yichang Humanwell Pharmaceutical Co., Ltd.) Anesthesia was maintained with sevoflurane titrated to maintain a Bispectral Index (BIS) between 40 and 60, with supplemental doses of sufentanil and cis-atracurium as needed. At the conclusion of surgery, all patients received tropisetron 5 mg intravenously for PONV prophylaxis. Upon extubation in the post-anesthesia care unit (PACU), the PCA pump was connected and initiated.
The PCA solution for both groups consisted of sufentanil (2 μg/kg) and flurbiprofen (3 mg/kg) diluted in 150 mL of normal saline, administered via a smart infusion pump (Henan Tuoren Medical Device Co., Ltd.).
Group A (Constant-Rate Background Infusion, CRBI): A fixed background infusion of 2 mL/h was set, with a patient-controlled bolus of 1.5 mL and a lockout interval of 10 minutes.
Group B (Feedback-Regulated Background Infusion, FRBI): The initial background infusion was set at 2 mL/h, with the same bolus parameters as Group A. The FRBI algorithm dynamically adjusted the background rate (range: 1–4 mL/h) based on patient demand: it increased by 20% following two or more effective bolus demands within 30 minutes, and decreased by 20% after four consecutive hours without any demand. The 20% adjustment threshold was chosen based on preliminary simulation studies, which indicated that this magnitude provided a clinically meaningful change in opioid delivery while avoiding excessive rate oscillations.
Rescue analgesia (intramuscular ketorolac 30 mg) was available for breakthrough pain (NRS > 4). Rescue antiemetics (intravenous tropisetron 5 mg) were administered when patients reported intolerable nausea/vomiting or when nausea/vomiting was documented during standardized assessments (at 2, 6, 12, 24, and 48 hours postoperatively).
Outcome Measures
The primary outcome was the incidence of PONV within 48 hours postoperatively. PONV was defined as the occurrence of nausea and/or vomiting. PONV was assessed by trained, blinded post-anesthesia care unit (PACU) nurses and ward nurses using a standardized questionnaire at 2, 6, 12, 24, and 48 hours postoperatively.
Secondary Outcomes Included
Pain Intensity
Assessed using the 11-point Numerical Rating Scale (NRS, 0=no pain, 10=worst imaginable pain) at rest at 2, 6, 12, 24, and 48 hours after surgery.
Opioid Consumption
Total consumption of sufentanil (μg) over 48 hours.
Other Adverse Events
Incidence of dizziness, headache, and respiratory depression (defined as respiratory rate <8 breaths/min or SpO2 <90% on room air).
Rescue Interventions
Number of patients requiring rescue analgesia or antiemetics.
Patient Satisfaction
Evaluated at 48 hours using a 5-point Likert scale (1=very dissatisfied to 5=very satisfied).
Sedation Level
Assessed using the Ramsay sedation scale at the same time points as NRS.
Statistical Analysis
Based on preliminary data from our institution estimating PONV incidences of 58% (CRBI) and 33% (FRBI), a sample size of 66 patients per group was calculated to achieve 80% power with a two-sided alpha of 0.05, allowing for a 10% dropout rate.
Statistical analyses were performed using SPSS version 17.0. Normality of data distribution was assessed with the Kolmogorov–Smirnov test. Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range) and were compared using independent t-tests or Mann–Whitney U-tests, as appropriate. Categorical variables are presented as counts (percentages) and were compared using the Chi-square or Fisher’s exact test. A repeated-measures analysis of variance (RM-ANOVA) was used to analyze changes in NRS scores over time. Binary logistic regression was performed to identify factors associated with PONV, adjusting for Apfel score and intraoperative opioid use. As multiple secondary endpoints were tested, these results should be interpreted as exploratory. A two-tailed P-value of less than 0.05 was considered statistically significant. For the primary outcome, we also calculated the risk difference and risk ratio with 95% confidence intervals. A modified intention-to-treat (ITT) analysis, which included all randomized patients, was performed for the primary outcome to reduce potential bias. Results were consistent with the per-protocol analysis.
Results
Of the 151 patients initially assessed for eligibility, 13 declined participation and six did not meet inclusion criteria. The remaining 132 patients were randomized into either Group A (CRBI, n=66) or Group B (FRBI, n=66). Prior to induction, four patients in Group A and three in Group B withdrew consent. Intraoperative conversion to open surgery led to the exclusion of three patients in each group. Consequently, the final analysis included 119 patients (Group A: n=59; Group B: n=60) (Figure 1).
 |
Figure 1 CONSORT flow diagram of patient enrollment, randomization, and follow-up. |
Demographic and intraoperative characteristics were comparable between the two groups (Table 1). There were no statistically significant differences in age, weight, ASA physical status, Apfel score, or intraoperative sufentanil consumption (all P > 0.05). Hospital length of stay was comparable between groups (3.2 ± 0.8 days vs 3.3 ± 0.9 days, P = 0.52).
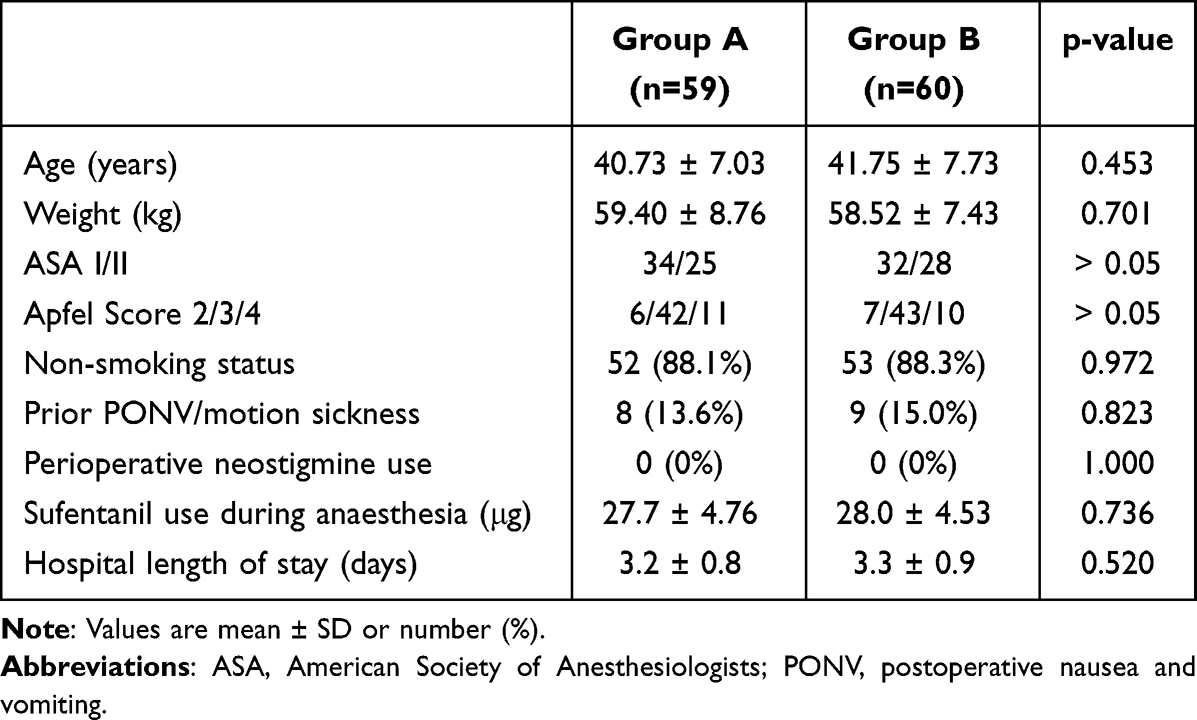 |
Table 1 Demographic and Intraoperative Variables |
Pain control, as assessed by NRS scores at rest at 2, 6, 12, 24, and 48 hours postoperatively, was equivalent between groups (all P > 0.05, Table 2). The number of effective PCA demands and the requirement for rescue analgesia (ketorolac) were also similar. However, total postoperative sufentanil consumption over 48 hours was significantly lower in the FRBI group (88.53 ± 20.05 μg) compared to the CRBI group (122.56 ± 18.91 μg), representing an approximate reduction of 28% (P < 0.001).
 |
Table 2 Postoperative Pain-Related Profile Up to 48 h After Surgery |
The FRBI group demonstrated a significantly lower overall incidence of PONV (nausea and/or vomiting) compared to the CRBI group (41.7% vs 62.7%, risk difference: −21.0% [95% CI: −38.1% to −3.9%]; risk ratio: 0.66 [95% CI: 0.46 to 0.96], P = 0.022). Subgroup analysis revealed that the incidence of nausea (41.7% vs 62.7%, P = 0.022) and the combined outcome of nausea and vomiting (33.3% vs 52.5%, P = 0.034) were both markedly reduced in the FRBI group (Table 3). The incidence of dizziness and headache was significantly lower in the FRBI group (5.0% vs 20.3%, P = 0.012). No episodes of respiratory depression (defined as respiratory rate <8/min or SpO2 <90%) were observed in either group. The use of rescue antiemetics (tropisetron) showed a downward trend in the FRBI group but did not reach statistical significance (16.7% vs 27.1%, P = 0.167). Patient satisfaction with postoperative analgesia was significantly higher in the FRBI group, with a median satisfaction score of 4 (IQR 4–5) versus 4 (IQR 3–4) in the CRBI group (P = 0.002).
 |
Table 3 Efficacy Outcomes |
In the modified intention-to-treat (ITT) analysis (n=132), the incidence of PONV remained significantly lower in the FRBI group (41.7% vs 62.7%, P = 0.022).
Multivariable binary logistic regression analysis (Table 4) showed that after adjusting for Apfel score and intraoperative opioid use, group allocation (FRBI vs CRBI) was an independent predictor of PONV (adjusted odds ratio: 0.45 [95% CI: 0.22–0.92], P = 0.009).
 |
Table 4 Binary Logistic Regression Analysis for Factors Associated with PONV |
Table 5 summarizes the FRBI algorithm performance. The mean rate adjustments per patient were 4.2 ± 1.8, with balanced up‑ and down‑titrations. Altogether 28 patients (46.7%) had up‑titrations. The maximum protocol rate was 4 mL/h, and the highest observed rate was 3.5 mL/h. Most time (60%) was spent at intermediate rates. The FRBI group achieved a 28% mean opioid reduction. No safety events, alarms, manual overrides, or respiratory depression occurred, confirming the safety of the system.
 |
Table 5 FRBI Algorithm Behavioral Characteristics |
Discussion
This randomized controlled trial demonstrates that a smart PCA system utilizing a patient-demand-responsive, feedback-regulated background infusion (FRBI) algorithm significantly reduces the incidence of postoperative nausea and vomiting (PONV) and total opioid consumption in patients undergoing laparoscopic myomectomy, while maintaining analgesia comparable to a conventional constant-rate infusion (CRBI).
The clinical significance of the observed 32% relative reduction in PONV incidence is underscored by the high baseline risk in this population, which aggregates female gender, opioid use, and laparoscopic gynecological surgery.8,15,16 Our results align with the pharmacodynamic principle that total opioid exposure is a modifiable driver of PONV. Current guidelines, including those from the American Pain Society, prudently advise against routine fixed-rate background infusion due to its propensity to increase opioid-related side effects without consistent analgesic benefit.10,17 Our study advances this discourse by demonstrating that a dynamic, feedback-informed infusion paradigm can circumvent the inherent limitations of static dosing. The FRBI system’s ability to automatically down-titrate the infusion rate during periods of low analgesic demand (eg., after four consecutive demand-free hours) appears to be a pivotal mechanism. This prevents the passive accumulation of opioid that typically occurs with CRBI, thereby directly attenuating opioid-mediated activation of the chemoreceptor trigger zone and vestibular system.18,19
Crucially, this opioid-sparing effect, amounting to an approximate 28% reduction in sufentanil consumption over 48 hours, was achieved without any compromise in analgesic efficacy. Pain scores remained equivalently low between groups at all time points, and the need for rescue analgesia was similar. This indicates that the FRBI algorithm successfully implements a form of “closed-loop” control, responding to increased nociceptive signals (via patient bolus demands) to up-titrate delivery, while proactively reducing background infusion during periods of adequate analgesia. The significantly higher patient satisfaction in the FRBI group underscores the tangible clinical benefit of this approach.
From the perspective of drug delivery systems, our study highlights that therapeutic outcomes can be improved by innovating how existing potent drugs are delivered. The FRBI mode represents a step toward intelligent, adaptive drug delivery systems for perioperative medicine. It exemplifies a “device-enabled pharmacology” strategy, where embedded algorithms modulate drug administration based on physiologic feedback.
Our findings must be interpreted considering certain limitations. First, this was a single-center study in a specific surgical cohort (laparoscopic myomectomy). Our results may not be generalizable to other surgeries with different pain trajectories (eg., major orthopedic or thoracic procedures) or to male patients. Second, we reported the incidence but not the severity or time profile of PONV, and we did not have a standardized rescue antiemetic protocol beyond patient-reported “intolerable nausea/vomiting”; future studies would benefit from using multi-dimensional assessment tools and standardized rescue protocols. Third, the algorithm parameters (eg., two demands in 30 minutes to trigger an increase, four demand-free hours to trigger a decrease) were empirically chosen and warrant further investigation to determine their optimality across different contexts and patient phenotypes. Fourth, ERAS principles were applied but not standardized, which may have introduced variability. Fifth, no formal cost-effectiveness analysis was performed, which would be valuable to assess the economic feasibility of adopting this smart pump system.
In conclusion, under the conditions of this study, the implementation of a feedback-regulated background infusion mode in IV-PCA reduced opioid consumption and PONV while maintaining analgesia after laparoscopic myomectomy. This strategy suggests a favorable safety profile in this specific surgical population.
Data Sharing Statement
The datasets and materials used during the current study, including the study protocol and statistical analysis plan, are available from the corresponding author upon reasonable request, starting from publication and for 5 years.
Ethics Approval and Consent to Participate
The clinical trial was reviewed and approved by the Ethics Committee of The First Affiliated Hospital of Zhejiang Chinese Medical University (No: 2024-KLS-661-02) and registered at the International Clinical Trials Registry Platform (Registration number: ChiCTR2500100820). Participants were recruited following the acquisition of written informed consent. We confirm our study complies with the Declaration of Helsinki.
Funding
Supported by departmental and institutional funds only.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Krimou Y, Erraghay S, Guennoun A, Mamouni N, Bouchikhi C, Banani A. Myoma praevia and pregnancy. Pan Afr Med J. 2019;33:216. doi:10.11604/pamj.2019.33.216.14898
2. Kanellos P, Nirgianakis K, Siegenthaler F, Vetter C, Mueller MD, Imboden S. Postoperative pain is driven by preoperative pain, not by endometriosis. J Clin Med. 2021;10(20):4727. doi:10.3390/jcm10204727
3. Qin Y, Yang Y, Qin S, Xiong Z. Regional nerve block in postoperative analgesia after cesarean section: a narrative review. Medicine. 2024;103(52):e41159. doi:10.1097/MD.0000000000041159
4. Tang JC, Ma JW, Jian JJ, Shen J, Cao LL. Effect of different anesthetic modalities with multimodal analgesia on postoperative pain level in colorectal tumor patients. World J Gastrointest Oncol. 2024;16(2):364–9. doi:10.4251/wjgo.v16.i2.364
5. Hailu S, Mekonen S, Shiferaw A. Prevention and management of postoperative nausea and vomiting after cesarean section: a systematic literature review. Ann Med Surg. 2022;75:103433. doi:10.1016/j.amsu.2022.103433
6. Lu H, Zheng C, Liang B, Xiong B. Mechanism and risk factors of nausea and vomiting after TACE: a retrospective analysis. BMC Cancer. 2021;21(1):513. doi:10.1186/s12885-021-08253-1
7. Ishikawa E, Hojo T, Shibuya M, et al. Risk factors for postoperative nausea and vomiting in patients of orthognathic surgery according to the initial onset time: a cross-sectional study. J Dent Anesth Pain Med. 2023;23(1):29–37. doi:10.17245/jdapm.2023.23.1.29
8. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2020;131(2):411–448. doi:10.1213/ANE.0000000000004833
9. Chalabianloo F, Fadnes LT, Høiseth G, et al. Subjective symptoms and serum methadone concentrations: what should guide dose adjustments in methadone maintenance treatment? A naturalistic cohort study from Norway. Subst Abuse Treat Prev Policy. 2021;16(1):39. doi:10.1186/s13011-021-00367-w
10. Gordon DB, de Leon-Casasola OA, Wu CL, Sluka KA, Brennan TJ, Chou R. Research gaps in practice guidelines for acute postoperative pain management in adults: findings from a review of the evidence for an American Pain Society Clinical Practice Guideline. J Pain. 2016;17(2):158–166. doi:10.1016/j.jpain.2015.10.023
11. Sng BL, Tan DJ, Tan CW, Han NR, Sultana R, Sia ATH. A preliminary assessment of vital-signs-integrated patient-assisted intravenous opioid analgesia (VPIA) for postsurgical pain. BMC Anesthesiol. 2020;20(1):145. doi:10.1186/s12871-020-01060-4
12. Lucci M, Dixon A, Walker K. Feedback control systems could revolutionize the administration of prescription opioids. J Opioid Manag. 2025;21(5):369–371. doi:10.5055/jom.0946
13. Song Y, He Q, Huang W, et al. New insight into the analgesic recipe: a cohort study based on smart patient-controlled analgesia pumps records. Front Pharmacol. 2022;13:988070. doi:10.3389/fphar.2022.988070
14. Ishaku Z, Koshy DI, Adamu Bala M. Enhanced Recovery After Surgery (ERAS) pathways in elective total joint arthroplasty. Cureus. 2025;17(9):e91481. doi:10.7759/cureus.91481
15. Echeverria-Villalobos M, Fiorda-Diaz J, Uribe A, Bergese SD. Postoperative nausea and vomiting in female patients undergoing breast and gynecological surgery: a narrative review of risk factors and prophylaxis. Front Med. 2022;9:909982. doi:10.3389/fmed.2022.909982
16. Zhu T, Lu W, Wang W, Zhou L, Yan W. Effect of Patient-Controlled Epidural Analgesia (PCEA) based on ERAS on postoperative recovery of patients undergoing gynecological laparoscopic surgery. Evid Based Complement Alternat Med. 2022;2022:6458525. doi:10.1155/2022/6458525
17. Jun MR, Lee MO, Shim HS, et al. Intravenous patient-controlled analgesia regimen in postoperative pain management following elective cesarean section: a single-center retrospective evaluation. Medicine. 2023;102(15):e33474. doi:10.1097/MD.0000000000033474
18. Zhang T, Yue Z, Yu L, et al. S-ketamine promotes postoperative recovery of gastrointestinal function and reduces postoperative pain in gynecological abdominal surgery patients: a randomized controlled trial. BMC Surg. 2023;23(1):74. doi:10.1186/s12893-023-01973-0
19. Xu S, Hu S, Ju X, Li Y, Li Q, Wang S. Effects of intravenous lidocaine, dexmedetomidine, and their combination on IL-1, IL-6 and TNF-α in patients undergoing laparoscopic hysterectomy: a prospective, randomized controlled trial. BMC Anesthesiol. 2021;21(1):3. doi:10.1186/s12871-020-01219-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.