Back to Journals » International Medical Case Reports Journal » Volume 18
Fecal Fistula Following Appendectomy as an Unusual Late Complication: A Rare Case Report
Authors Nazari FA, Baset G ![]() , Zarif SK, Rahimdeen MA, Amiri A
, Zarif SK, Rahimdeen MA, Amiri A ![]() , Seyar F
, Seyar F
Received 5 February 2025
Accepted for publication 15 March 2025
Published 20 March 2025 Volume 2025:18 Pages 381—386
DOI https://doi.org/10.2147/IMCRJ.S518439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Fareed Ahmad Nazari,1 GhulamYahia Baset,1 Saied Karim Zarif,1 Muhammad Anwar Rahimdeen,1 Ahmad Amiri,2 Farukh Seyar2
1Department of Emergency Surgery and Trauma, Kabul University of Medical Science, Ali Abad University Hospital, Kabul, Afghanistan; 2Department of Abdominal Surgery, Kabul University of Medical Science, Ali Abad University Hospital, Kabul, Afghanistan
Correspondence: GhulamYahia Baset, Email [email protected]
Abstract: Post-appendectomy fecal fistula is a rare complication, but it is associated with significant morbidity. Etiological factors of post-appendectomy fecal fistula formation include severe peri-appendicitis involving the base of the appendix as well as adjoining caecal wall; neoplasia of the appendix and caecum; infective bowel conditions especially intestinal tuberculosis, actinomycosis and Crohn’s disease; distal obstruction and gossypiboma. Diagnosis of post-appendectomy fecal fistula is usually made on CT-scan but Fistulography is also useful in the late stages of the disease. Treatment of post-appendectomy fecal fistula includes non-surgical and surgical management options. We present a 20-year-old male patient who presented to the hospital with a longstanding surgical site infection in the scar of a previous appendectomy incision.
Keywords: fecal fistula, post-appendectomy, gossypiboma, appendicitis
Introduction
Acute appendicitis is the most commonly encountered cause of acute abdomen in general surgery and appendectomy is one of the most frequently performed procedures in clinical practice.1 Complications of appendectomy include surgical-site infection, postoperative ileus, stump appendicitis, intra-abdominal abscess formation, leaks from the remnant stump, fistula formation, small bowel obstruction, and localized or diffused peritonitis.2 In the case of appendix perforation or gangrene with peri-appendicitis, the frequency of septic complications is as high as 30%.3
Post-appendectomy fecal fistula is a rare complication, but it is associated with significant morbidity.4 Fecal fistula is distressing for both the surgeon and the patient. In some references, it has been given the first position among the unfortunate sequelae of appendectomies.5
Various types of fistulous communication can occur, including appendicovesical, appendicointestinal, appendicouterine, and appendicocutaneous.6 In our case, it was an appendicocutaneous fistula caused by a remnant foreign body after appendectomy.
Case Presentation
A 20-year-old male presented to the general surgery department of our hospital with a longstanding surgical site infection in the scar of a previous appendectomy incision. Appendectomy has been performed one year earlier at a provincial hospital. The procedure was said to be performed without any difficulty, and the appendix has not been perforated or gangrenous. The patient had been discharged home 2 days later. The patient had developed a surgical site infection in the second week of surgery which has been managed with removal of a skin suture and regular dressings. The disease had been controlled temporarily but reoccurred frequently.
On physical examination, a scar of Gridiron incision with purulent discharge from a corner of it was seen in the right iliac fossa (Figure 1). After dressing, it was seen that fecal materials were present in the discharge of surgical site infection. Bowel sounds were normally audible, and the abdomen was soft with no tenderness or rigidity.
 |
Figure 1 Scar of previous gridiron incision with fecal fistula presenting as wound infection. |
The patient was stable hemodynamically with a blood pressure of 110/70 mmHg. Complete blood count revealed white blood cells of 7500/dL, Hb of 13 mg/dL, and platelet of 245000/dL. Urea, creatinine, and glycemia were within normal limits. Ultrasonography of the abdomen reported a small collection in the right iliac fossa with possible communication with bowel loops. A fistulography with contrast injection from the fistula site revealed communication between skin and caecum (Figure 2). Contrast-enhanced CT scan of the abdomen revealed a colocotaneous fistula and underlying gossypiboma/foreign body (Figure 3).
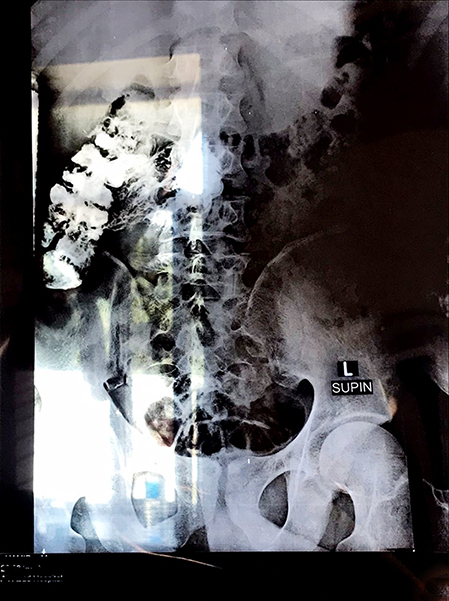 |
Figure 2 Fistulography showing contrast material inside the colon. |
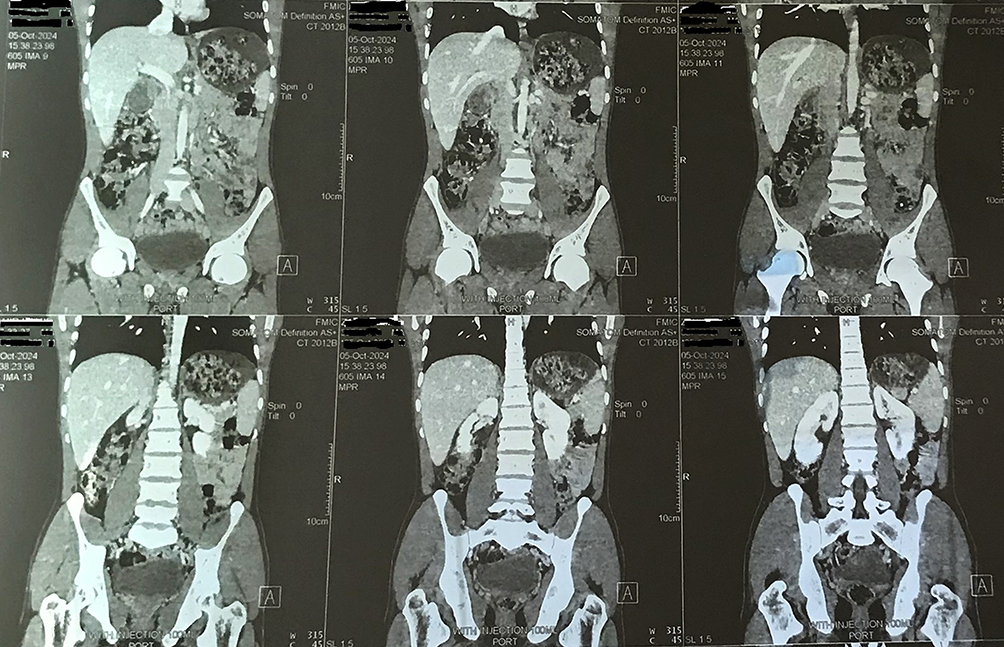 |
Figure 3 Contrast-enhanced CT scan of the abdomen showing underlying gossypiboma. |
The patient was planned for a laparotomy. A lower midline laparotomy was performed to prepare for a possible right hemicolectomy. During the operation, it was found that there is a foreign body in the right iliac fossa (Figure 4), a hole in the wall of the caecum, and a small amount of pus collection and adhesions between the caecum and abdominal wall (Figure 5). The collection was suctioned, the foreign body removed, and the fistula was repaired primarily as the patient was young and well-nourished. The abdomen was closed layer by layer after hemostasis and the insertion of a tube drain.
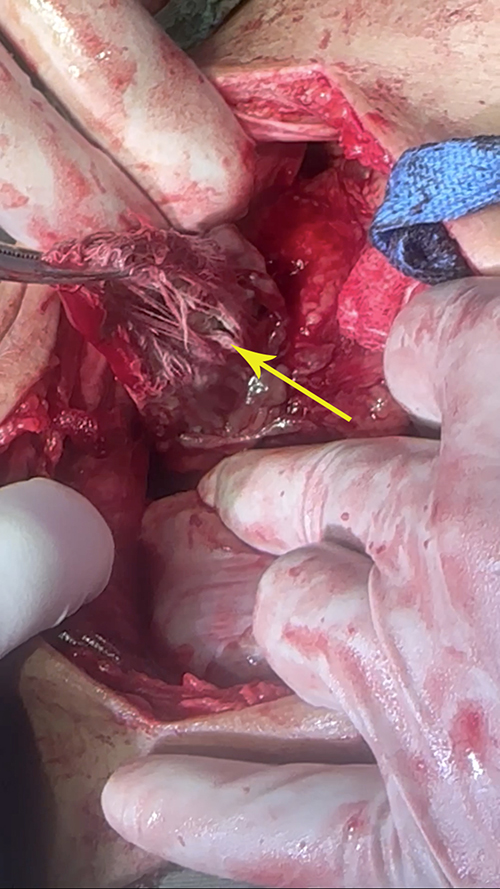 |
Figure 4 A foriegn body in the right iliac fossa during operation. The yellow arrow shows the surgical gauze. |
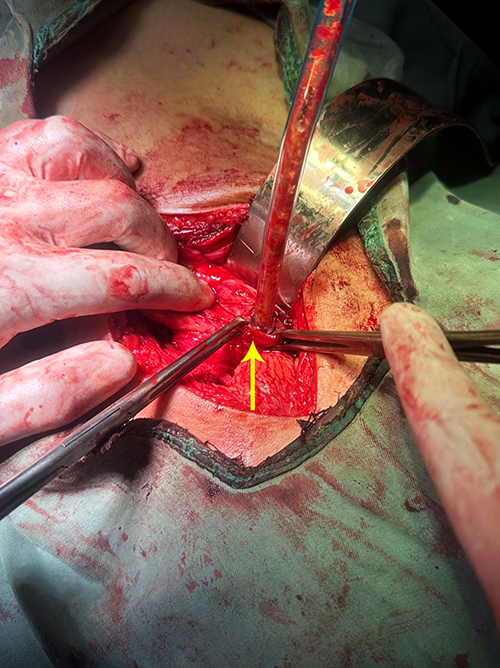 |
Figure 5 Fecal fistula intra-operatively. The yellow arrow shows the fistula tract. |
The patient was nil by mouth (NPO) for four days. Bowel sounds were audible on the fourth postoperative day, so a liquid diet was started, and the tube drain was removed. The patient was discharged from the hospital on the eighth postoperative day and followed up for two months with no complications.
Discussion
Fecal fistula following appendectomy is a rare complication.2 This complication presents as a late but serious and challenging complication.2 Etiological factors of post-appendectomy fecal fistula formation include severe peri-appendicitis involving the base of the appendix as well as adjoining caecal wall; neoplasia of appendix and caecum; infective bowel conditions especially intestinal tuberculosis, actinomycosis and Crohn’s disease; distal obstruction and foreign body.2 Nutritional debilitation of the patient will also play a role in forming such a fistula.4 Iatrogenic injuries to the caecum during appendectomy are also an etiological factor.4 Some authors believe that the use of purse-string sutures during appendectomy is the main contributory factor in the development of fecal fistula.7 In our case, the foreign body was the etiological factor of the disease.
About 90% of post-appendectomy fecal fistulas will not persist for a long time and close spontaneously within a month and about 10% within the next two months.8 After three months, none have been reported to close spontaneously.8 The longest duration of fecal drainage, before operative relief, so far reported was in a patient who had intermittent discharge for seven years; while the shortest duration of the fistula was a case which closed spontaneously in twelve hours.9
Fecal fistula may be confused with surgical site infection at its early stages.4 It usually presents with persistent fecal discharge from the wound, which continues despite frequent drainage and dressing.4 Associated symptoms include fever, nausea, and vomiting, and symptoms and signs of paralytic ileus.1
Diagnosis of the post-appendectomy fecal fistula is usually made on a CT scan which shows extravasation of the oral contrast medium or air at the caecum. A CT scan will also show the foreign body if present.1 Fistulography is useful in the late stages of the disease when the fistula tract is well-matured.1
Treatment of post-appendectomy fecal fistula includes non-surgical and surgical management options.2 Non-surgical or conservative management is appropriate for most fistulas in the absence of underlying pathology and distal obstruction.2
Non-surgical management options for post-appendectomy fecal fistula include vacuum-assisted closure (VAC),10 fistulotoscopy with fibrin glue injection,11 Infliximab in case of underlying Crohn’s disease, and Somatostatin analogs which reduce fistula output and thereby easing management of fluid and electrolyte losses.12 As the etiological factor of fistula formation in our case was the presence of the foreign body, none of these conservative managements will be appropriate.
Surgical treatment of post-appendectomy fecal fistula should be considered after 4–6 weeks of sepsis-free adequate nutritional support.9 Fistula tract excision, removal of the foreign body if present, and segmental resection of the involved bowel, with end-to-end anastomosis, is recommended.9 Surgical management will be the most appropriate option in our case to remove the foreign body, excise the long-standing fistula tract which has been there for one year, and repair the fistula primarily.
Conclusion
Fecal fistula following appendectomy is a rare but important complication. The presence of a remnant foreign body should be kept in mind in any case of persistent wound infection and fecal fistula after a surgical operation. CT scan of the abdomen with contrast is the diagnostic modality of choice for post-appendectomy fecal fistula. Most of the patients can be managed with conservative treatment, but surgical management with fistula tract excision, removal of foreign body, and segmental resection of involved bowel when appropriate is necessary in case of underlying pathologies such as the presence of distal obstruction, foreign body, and neoplasm.
Ethical Approval
This case report is exempt from ethical approval as determined by the ethical review board at our institution, given the nature of the article.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Acknowledgment
The authors would like to express their sincere gratitude to the patient and the patient’s guardian for providing consent to include the case details and photographs in this publication.
Funding
No funding was received for this case report.
Disclosure
The authors declare that they have no competing in this work.
References
1. Anamika S, Rinki, Anoop Y, Satish K. Post appendectomy faecal fistula: a rare complication. Global J Res Anal. 2023;12(01):173–174.
2. Muhammad S, Syed HA, Syed IA. Persistent appendiceal faecal fistula following a complicated open appendicectomy. J Pak Med Assoc. 2009;59(3):181–183.
3. Helmer KS, Robinson EK, Lally KP, et al. Standardized patient care guidelines reduce infectious morbidity in appendectomy patients. Am J Surg. 2002;183:608–613. doi:10.1016/S0002-9610(02)00860-7
4. Shirbur SN, Telkar SR, Goudar BV, Muzamil PMD, Chethan VN. Faecal fistula following appendicectomy: a case report. J Clin Diagn Res. 2012;6(7):1322–1323.
5. Mohamed A. Faecal fistula, the most unfortunate sequelae of appendectomy. case report. Internet J Surg. 2010;27(2):1–4.
6. Muthukumarassamy R, Shankar Raman R, Sarath Chandra S, Jagdish S. Appendico-cutaneous fistula. Indian J Surg. 2005;67(6):323–324.
7. Baldwin JF. The prevention of faecal fistulas after appendectomy simple ligation vs precarious purse-string. Ann Surg. 1932;95(5):704–714. doi:10.1097/00000658-193205000-00008
8. Teubner A, Morrison K, Ravishankar HR, Anderson ID, Scott NA, Carlson GL. Fistulocyclysis on successfully replace parenteral feeding in the nutritional support of patients with enterocutaneous fistula. Br J Surg. 2004;91:625–631. doi:10.1002/bjs.4520
9. Deaver JB. Appendiceal fecal fistula. Ann Surg. 1924;80:56–57. doi:10.1097/00000658-192407000-00007
10. Cro C, George KJ, Donnelly J, Irwin ST, Gardiner KR. Vacuum assisted closure system in the management of enterocutaneous fistulae. Postgrad Med J. 2002;78:364–365. doi:10.1136/pmj.78.920.364
11. Eleftheriadis E, Kotzampassi K. Therapeutic fistuloscopy: an alternative approach in the management of postoperative fistulas. Dig Surg. 2002;19:230–236. doi:10.1159/000064218
12. Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N Engl J Med. 1999;340:1398–1405. doi:10.1056/NEJM199905063401804
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.