Back to Journals » Clinical Ophthalmology » Volume 8
Favorable anatomic and visual outcomes with 25-gauge vitrectomy for myopic foveoschisis
Authors Mii M, Matsuoka M, Matsuyama K, Otsu Y, Nishimura T
Received 12 May 2014
Accepted for publication 29 May 2014
Published 12 September 2014 Volume 2014:8 Pages 1837—1844
DOI https://doi.org/10.2147/OPTH.S67619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Mei Mii, Masato Matsuoka, Kayako Matsuyama, Yayoi Otsu, Tetsuya Nishimura
Department of Ophthalmology, Kansai Medical University, Takii Hospital, Osaka, Japan
Purpose: To report the surgical outcomes of 25-gauge vitrectomy in eyes with myopic foveoschisis (MF).
Methods: The medical records of 40 eyes of 36 patients that had undergone 25-gauge vitrectomy with internal limiting membrane peeling for MF were studied. The main outcome measures were the best-corrected visual acuity (BCVA) and the optical coherence tomography (OCT) findings. The eyes were divided into two groups: 1) those with a foveal detachment (FD; FD group); and 2) those without a FD (no-FD group).
Results: The postoperative OCT images showed a resolution of the MF with a significant reduction in the central foveal thickness from the preoperative values in both the FD group (479±150 µm to 196±56 µm; P=0.002, mean ± standard deviation) and in the no-FD group (369±116 µm to 245±50 µm; P=0.001). The final mean BCVA significantly improved from the preoperative values in the FD group (0.96±0.53 logarithm of the minimum angle of resolution [logMAR] units to 0.70±0.56 logMAR units; P=0.009) and in the no-FD group (0.46±0.38 logMAR units to 0.34±0.36 logMAR units; P=0.007). The final BCVA in the FD group improved in 63%, remained unchanged in 31%, and worsened in 6%. In the no-FD group, the final BCVA improved in 21%, remained unchanged in 71%, and worsened in 8% of the eyes. A better final BCVA was significantly correlated with a better preoperative BCVA in both groups (P<0.001).
Conclusion: Twenty five-gauge vitrectomy results in favorable visual and anatomic outcomes for MF. We recommend that 25-gauge vitrectomy be used to treat eyes with MF.
Keywords: myopic foveoschisis, 25-gauge vitrectomy, high myopia, internal limiting membrane, gas tamponade
Introduction
Myopic foveoschisis (MF) is one of the major causes of vision reduction in myopic patients, and its presence has been increasingly recognized with the advent of optical coherence tomography (OCT).1,2 The estimated incidence of MF ranges from 8%–34% in eyes with high myopia.3–7 Because MF is typically a slowly progressive condition, the majority of the patients retain relatively good vision.8 However, progression to more serious complications, such as foveal detachments (FD), epiretinal membrane (ERM), full-thickness macular hole (MH), and macular hole retinal detachment (MHRD), can occur during its natural course.9–11 Thus, surgical intervention is needed in these patients to prevent anatomic and functional worsening of the retina and vision.12,13
Minimally invasive vitreous surgery with 23- and 25-gauge instruments has been developed. The advantages of minimally invasive vitreous surgery are that no wound suture is required because of the smaller incision size, less inflammation, less patient discomfort, faster recovery of visual acuity, and occasional shorter operative time.14 Therefore, the indications for 25-gauge vitrectomy have been expanded.15–17
Many studies have already demonstrated the effectiveness of 20-gauge vitrectomy in treating MF.12,13,18–23 However, little has been reported about the surgical outcome with the 25-gauge vitrectomy. Thus, the purpose of this study was to report the surgical outcomes of 25-gauge vitrectomy in eyes of MF.
Materials and methods
Subjects
The procedures used in this study conformed to the tenets of the World Medical Association’s Declaration of Helsinki. This was a retrospective study of 40 eyes in 36 consecutive patients who underwent the 25-gauge vitrectomy for MF at the Kansai Medical University Takii Hospital (Osaka, Japan) between January 2007 and April 2013. All of the patients had a progressive reduction of their vision or metamorphopsia that was attributable to MF. The exclusion criteria included eyes with other retinal disease that could affect the central vision, eg, full-thickness MH, MHRD, choroidal neovascularization, macular atrophy, axial length <26.0 mm, or follow-up <6 months. The eyes were divided into two groups based on the foveal anatomy in the OCT images – those with a FD (FD group; Figure 1) and those without a FD (no-FD group; Figure 2).
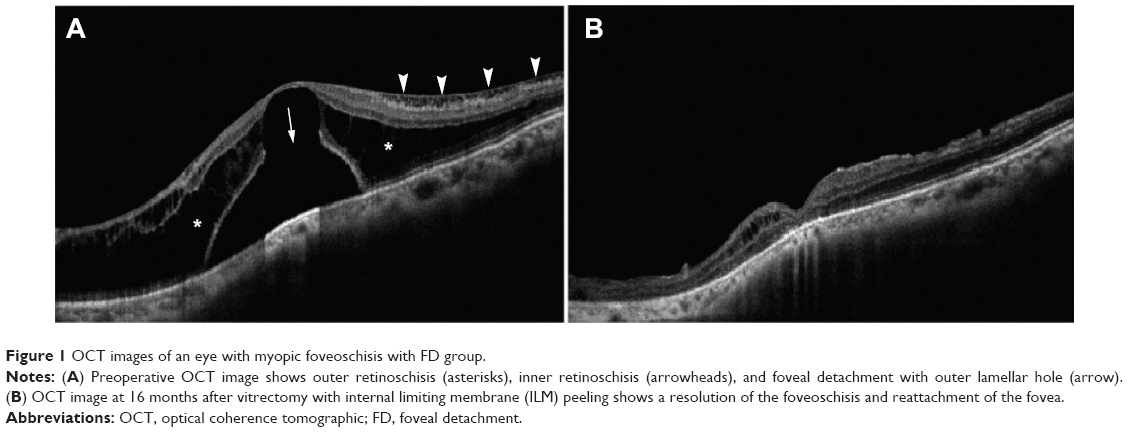 | Figure 1 OCT images of an eye with myopic foveoschisis with FD group. |
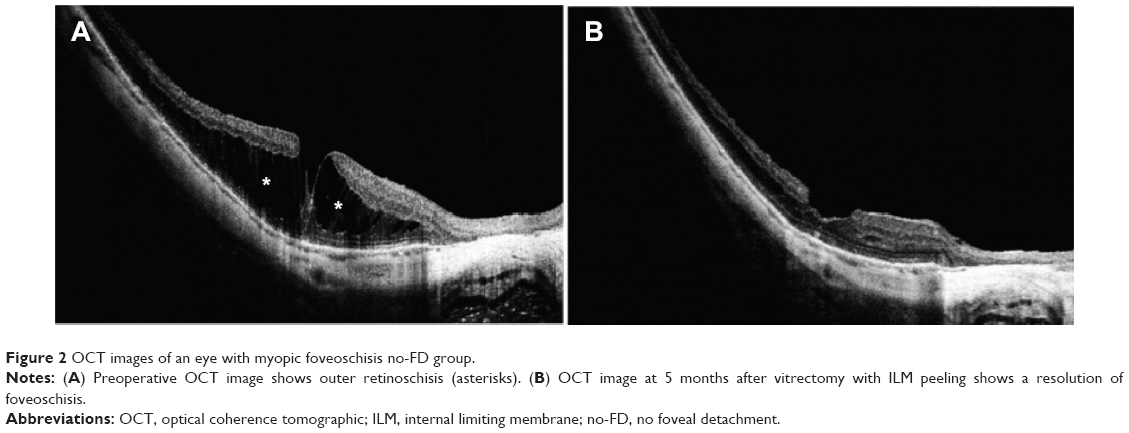 | Figure 2 OCT images of an eye with myopic foveoschisis no-FD group. |
Data collection
All patients had a complete ophthalmic examination, including measurement of the best-corrected visual acuity (BCVA), refraction, slit-lamp examination, fundus examination, color fundus photography, and OCT. The preoperative and postoperative BCVAs were determined as decimal visual acuity and then converted to logarithm of the minimum angle of resolution (logMAR) units for statistical analyses. An improvement or worsening of the postoperative BCVA was defined as a change >0.2 logMAR units. The preoperative and postoperative OCT recordings were performed with the OCT 3 (Carl Zeiss Meditec AG, Jena, Germany) or RTVue-100 (Optovue Inc., Fremont, CA, USA).
Surgical procedures
All surgeries were performed by one experienced surgeon (TN). The patients underwent the standard three-port 25-gauge pars plana vitrectomy with the insertion of a beveled cannula under retrobulbar anesthesia. Phacoemulsification with implantation of an intraocular lens was performed to avoid the effects of postoperative cataract development in 25 of the phakic eyes. The internal limiting membrane (ILM) was stained with 0.1% indocyanine green (ICG) or triamcinolone acetonide, and peeled over two to three disc diameters by intraocular forceps in all eyes. The decision to use gas tamponade was made based on the surgeon’s discretion, ie, the cases in which the macular hole or retinal breaks had occurred. A gas tamponade was made by injecting 20% sulfur hexafluoride in four eyes or air in five eyes after the fluid–air exchange. The patients with gas tamponade were encouraged to maintain a prone posture for at least a week postoperatively. When a leakage was detected at sclerotomy, the wound was sutured by 9-0 VICRYL® (Johnson & Johnson, New Brunswick, NJ, USA).
Statistical analyses
The results are expressed as the means ± standard deviations. The data were analyzed with Mann–Whitney U-tests, Wilcoxon paired signed-rank tests, Kruskal-Wallis test, and analysis of covariance. Associations between the final BCVA and the clinical parameters were examined by Pearson product moment correlation coefficients and multiple linear regression analyses. Differences were considered significant when the P-value was <0.05. All statistical analyses of the data were performed with IBM® SPSS® Statistics for Windows (version 22; IBM Corporation, Armonk, NY, USA).
Results
Preoperative characteristics
Forty eyes of 36 consecutive patients underwent 25-gauge vitrectomy; five were men and 31 were women. Their ages at the time of surgery ranged from 50–84 years with a mean of 70.0±7.7 years (Table 1). Of the 40 eyes, 25 were phakic, 14 were pseudophakic, and one was aphakic. The mean axial length was 28.9 mm, with a range from 26.2–32.8 mm. The mean postoperative follow-up period was 32.0±23.3 months with a range from 6–84 months.
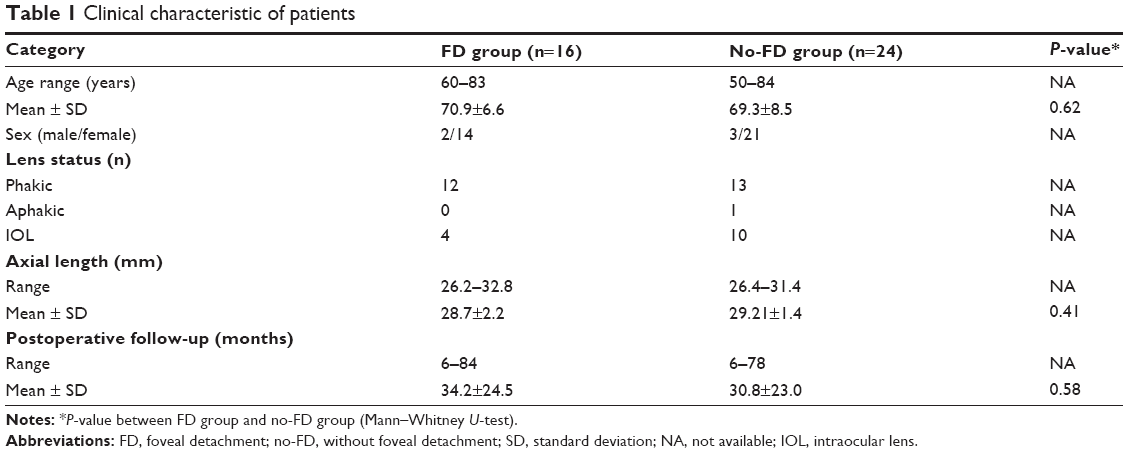 | Table 1 Clinical characteristic of patients |
Preoperatively, a foveoschisis was detected in all eyes by OCT. There were 16 eyes with FD (FD group) and 24 eyes without a FD (no-FD group). The preoperative differences in age, axial length, and postoperative follow-up periods were not significant between the two groups (Table 1). In contrast, the preoperative central foveal thickness and BCVA between two groups were significantly different (P=0.019 and P=0.003, respectively; Table 2).
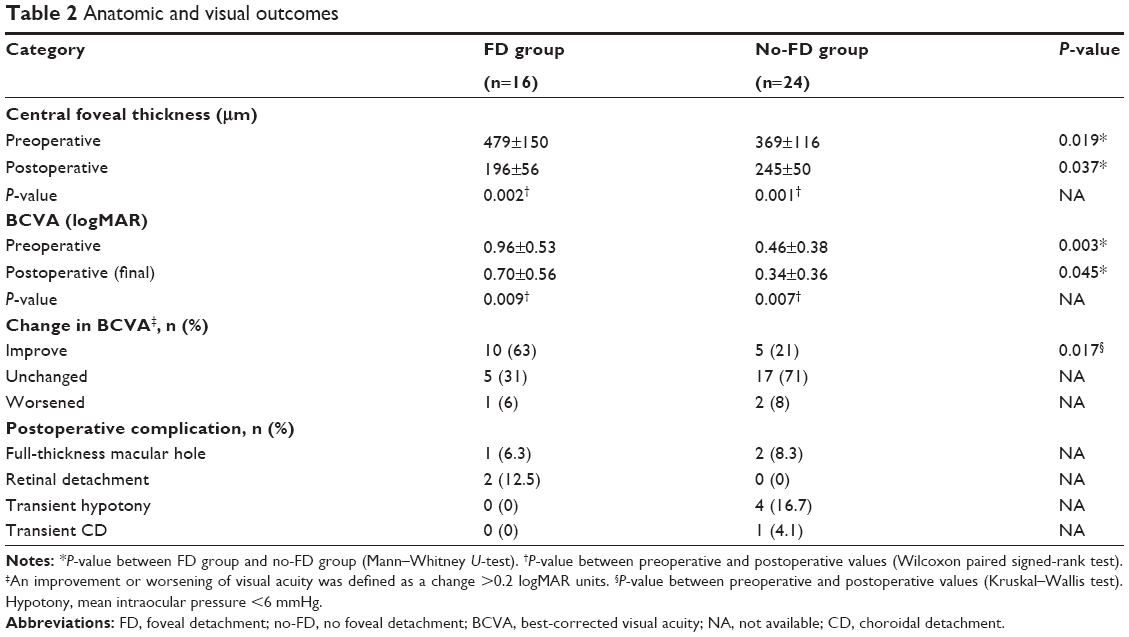 | Table 2 Anatomic and visual outcomes |
Surgical outcomes
Postoperative OCT showed a resolution of MF and a reattachment of the fovea in all eyes during the follow-up period (Figures 1 and 2). The postoperative central foveal thickness was significantly reduced from the preoperative values in FD group (479±150 μm to 196±56 μm; P=0.002; Table 2) and in the no-FD group (369±116 μm to 245±50 μm; P=0.001; Table 2).
The final BCVA significantly improved from the preoperative values in the FD group (0.96±0.53 logMAR to 0.70±0.56 logMAR; P=0.009; Table 2) and in the no-FD group (0.46±0.38 logMAR to 0.34±0.36 logMAR; P=0.007; Table 2). The percentage of eyes with a significant improvement of the final BCVA in FD group was greater than that in no-FD group (P=0.017; Table 2). The final BCVA in the FD group improved in 63%, remained unchanged in 31%, and worsened in 6%. In the no-FD group, the final BCVA improved in 21%, remained unchanged in 71%, and worsened in 8% of the eyes. The final BCVA was significantly correlated with the preoperative BCVA in the FD group (r2=0.74; P<0.001; Figure 3A) and in the no-FD group (r2=0.62; P<0.001; Figure 3B). The improvement of BCVA was not correlated with the presence of a FD, concomitant phacoemulsification, gas tamponade, and method of ILM visualization (P=0.71, 0.16, 0.63, and 0.88, respectively; Table 3).
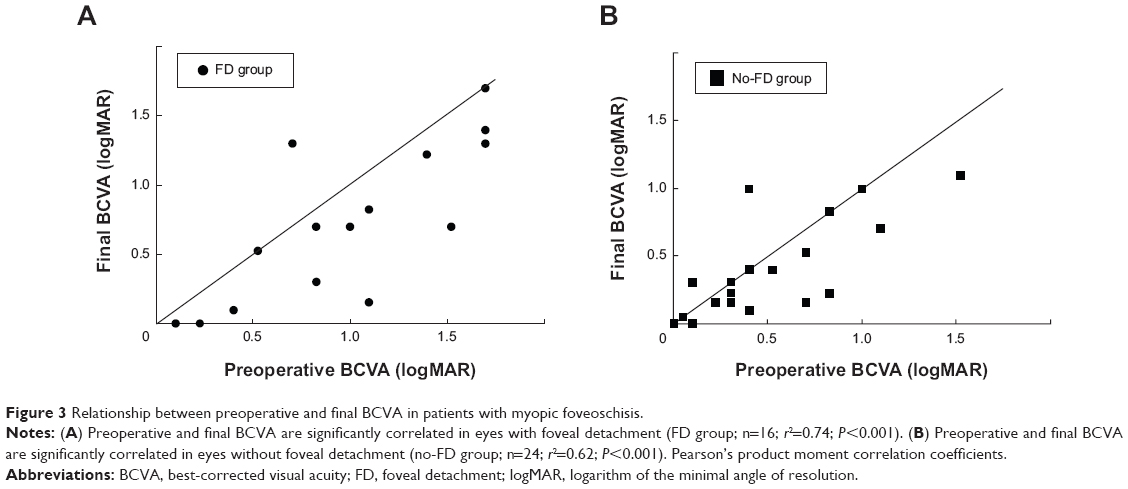 | Figure 3 Relationship between preoperative and final BCVA in patients with myopic foveoschisis. |
 | Table 3 Visual acuity improvement after 25-gauge vitrectomy |
Multiple linear regression analyses showed that the final BCVA was significantly correlated with preoperative BCVA (adjusted R2=0.66; P<0.001; Table 4), but not with age (P=0.49), axial length (P=0.08), preoperative central foveal thickness (P=0.61), FD (P=0.84), concomitant phacoemulsification (P=0.35), gas tamponade (P=0.48), or with use of ICG or triamcinolone acetonide (P=0.83).
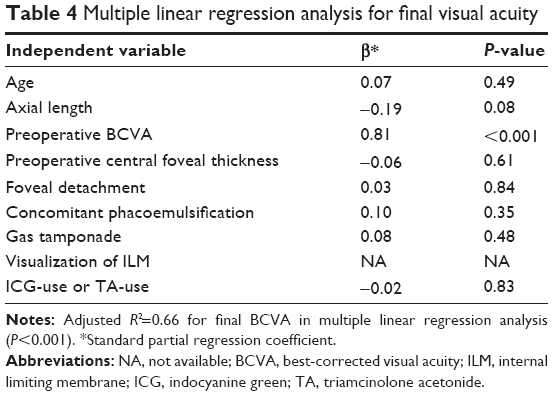 | Table 4 Multiple linear regression analysis for final visual acuity Independent variableβ*P-value |
Surgical complications
The postoperative complications in the FD group (16 eyes) included one with a MH (6.3%; Table 2) and two with a retinal detachment from a peripheral retinal break (12.5%). In the no-FD group (24 eyes), two eyes developed a MH (8.3%), four had hypotony (intraocular pressure <6 mmHg; 16.7%), and one had a choroidal detachment (4.1%). In the eyes with a postoperative MH, the preoperative inner segment/outer segment (IS/OS) junction line was disrupted or irregular at the fovea in the OCT images. These eyes underwent reoperation, and the MH was closed in one eye (FD group), but not in the other eye (no-FD group). The hypotony and choroidal detachment recovered without additional treatments within a week after the operation. The two eyes with a retinal detachment underwent reoperation, and the retinas were reattached.
Discussion
Our results confirmed the results of earlier studies that showed that 25-gauge vitrectomy with ILM peeling results in good anatomic and BCVA in eyes with MF. Evidence of these findings is based on the following: postoperative OCT showed a resolution of MF and a reattachment of the fovea in all eyes (Table 2; Figures 1 and 2), final mean BCVA significantly improved (Table 2), and better final BCVA was correlated with better preoperative BCVA (Table 4; Figure 3).
Vitrectomy or episcleral macular buckling has generally been used to treat MF.2 Although many studies had reported on the efficacy of episcleral macular buckling, this surgery has the potential complications, eg, difficult intraoperative access to posterior pole and risk of scleral perforation.2 Vitrectomy was believed to be a rational choice for the treatment of MF, because a MF was believed to be caused by premacular vitreous traction with a rigidity of the ILM and ERM, stiffness of the retinal vessels, and posterior staphyloma. Thus, vitrectomy with ILM peeling was expected to remove the tractional tension.7,18,20,24–26
Earlier studies reported on the favorable outcomes of 20-gauge vitrectomy for MF.12,13,18–23 More recently, Shimada et al reported on the surgical outcomes of 25-gauge vitrectomy for MF with FD, but they did not report on eyes without a FD.27 Shin et al reported on the outcomes of 25-gauge vitrectomy, but they did not compare the results in a FD group to a no-FD group.28 We now report on the surgical outcomes of 25-gauge vitrectomy for MF with and without FD.
Our results contain six major findings. First, 25-gauge vitrectomy resulted in favorable visual outcomes for MF; whereas, the visual improvement percentage in the no-FD group was lower than that in the FD group (21% versus 63%; Table 2). Earlier studies reported that the postoperative BCVA in patients in the FD group recovered, and the incidence was high, as did our results.12,13,22,27,29 This is quite reasonable because a reattachment of photoreceptors at the fovea should lead to recovery of the BCVA. Thus, eyes with FD are good candidates for vitrectomy.12 In contrast, several investigators reported that the final BCVA did not improve significantly in no-FD eyes.12,13 These other studies22,29 and our results showed a significant improvement of the final BCVA in the no-FD group, although the incidence of eyes with a visual improvement was low. This indicates that foveoschisis without a FD can result in decreased BCVA, which can be resolved by vitreous surgery.12 Additionally, FD, MH, or MHRD can develop in the no-FD group during its natural course.9–11 Thus, vitrectomy can prevent these changes and, thus, should be a useful treatment for the no-FD group to prevent further disease progression and retinal function damage.
Second, the final BCVA was significantly correlated with the preoperative BCVA in both the FD group and no-FD group (Table 4; Figure 3). These results agree with earlier reports on MF12,13,28 and also other macular disorders, such as ERM.30 This suggests that patients with MF should undergo surgery as soon as possible. However, to establish the surgical indications for MF is difficult because patients without a FD retain relatively good vision and do not visit eye doctors.8 Thus, patients who have progressive visual impairments, ie, vision reduction and metamorphopsia or FD attributable to MF should be good candidates for vitrectomy with ILM peeling.
Third, MF can be resolved by 25-gauge vitrectomy with ILM peeling in all eyes (Table 2; Figures 1 and 2). To date, the evidence that supports the need for ILM peeling is inconsistent. Many studies reported that vitrectomy with ILM peeling resulted in better anatomic and visual outcomes.12,13,18,19,27,31 On the other hand, other investigators reported on the effectiveness of vitrectomy without ILM peeling.20–22,32,33 Although ILM peeling can be a risk factor for iatrogenic MH in highly myopic eyes with very thin retina,20,27 it may ensure a complete removal of all premacular vitreous traction and decrease the retinal rigidity to conform better to the posterior staphyloma.24,26,34 In addition, Taniuchi et al reported that a recurrence of tractional macular detachment was observed more frequently in the eye without ILM peelings.29 Thus, we believe that ILM peeling is essential for resolving a MF.
Fourth, 25-gauge vitrectomy resulted in favorable anatomic and visual outcomes for MF with or without a gas tamponade (Table 2). The evidence to support the need for a gas tamponade also remains inconsistent. The rationale for a gas tamponade to treat a MF is because the gas is expected to push the retina back and close any paravascular breaks, which occasionally occur in highly myopic eyes.12,18–21,27,33 However, several studies have shown that vitrectomy without a gas tamponade also resulted in good anatomic and visual outcomes.13,22,23,31,32 In addition, Hirakata and Hida hypothesized that gas tamponade could be a cause of MH-formation because intraocular gas might push the subretinal fluid into the limited space under the FD toward the thin foveola.22 Thus, vitrectomy without gas tamponade might be a good treatment of MF – except for the cases in which intraoperative MH or retinal breaks had occurred. In support of this, we found that the final BCVA was not significantly correlated with whether a gas tamponade was used (Tables 3 and 4).
Fifth, a full-thickness MH can develop postoperatively as it did in three of 40 eyes (7.5%; Table 2). A postoperative MH is a serious complication in eyes with MF and the surgical results of this are not good.18,22 Gao et al reported that a defect in the IS/OS junction could be a risk factor for postoperative MH in the treatment of MF.35 Of the three eyes with a postoperative MH, two had an IS/OS junction defect (FD group and no-FD group), and one had an irregular IS/OS junction (no-FD group). Therefore, ILM peelings should be performed with care in eyes with MF and a defect in the IS/OS junction.35
Sixth, we found that the postoperative complications included transient hypotony (10.0%) and choroidal detachment (2.5%; Table 2). The 25-gauge sutureless vitrectomy technique is known to have higher incidence of postoperative wound leaks, hypotony, and endophthalmitis.36 Thus, using a beveled cannula has been recommended to prevent these complications.37,38 In highly myopic eyes, however, to create a self-sealing incision is occasionally difficult because the sclera is thin and of low rigidity, even if a beveled cannula is used.39 Although hypotony and choroidal detachment usually recover without additional treatment,15 a careful check of wound leakage is essential intraoperatively because wound leakage can be a cause of serious complications, such as endophthalmitis.
Our study has some limitations. This was a retrospective and nonrandomized study with a small number of cases and a short follow-up period. Therefore, further prospective and randomized clinical trials are needed with larger sample sizes.
In conclusion, our results show that 25-gauge vitrectomy with ILM peeling results in favolable anatomic and visual outcomes for eyes with myopic foveoschisis. In addition, our results show that the preoperative BCVA is a good predictor of the final BCVA. These results indicate that 25-gauge vitrectomy is a rational treatment for the patients who have progressive visual impairments due to myopic foveoschisis.
Disclosure
The authors report no conflicts of interest in this work.
References
Tano Y. Pathologic myopia: where are we now? Am J Ophthalmol. 2002;134(5):645–660. | ||
Todorich B, Scott IU, Flynn HW Jr, Chang S. Macular retinoschisis associated with pathologic myopia. Retina. 2013;33(4):678–683. | ||
Takano M, Kishi S. Foveal retinoschisis and retinal detachment in severely myopic eyes with posterior staphyloma. Am J Ophthalmol. 1999;128(4):472–476. | ||
Benhamou N, Massin P, Haouchine B, Erginay A, Gaudric A. Macular retinoschisis in highly myopic eyes. Am J Ophthalmol. 2002;133(6):794–800. | ||
Baba T, Ohno-Matsui K, Futagami S, et al. Prevalence and characteristics of foveal retinal detachment without macular hole in high myopia. Am J Ophthalmol. 2003;135(3):338–342. | ||
Panozzo G, Mercanti A. Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol. 2004;122(10):1455–1460. | ||
Wu PC, Chen YJ, Chen YH, et al. Factors associated with foveoschisis and foveal detachment without macular hole in high myopia. Eye (Lond). 2009;23(2):356–361. | ||
Ichibe M, Baba E, Funaki S, Yoshizawa T, Abe H. Retinoschisis in a highly myopic eye without vision impairment. Retina. 2004;24(2):331–333. | ||
Shimada N, Ohno-Matsui K, Baba T, Futagami S, Tokoro T, Mochizuki M. Natural course of macular retinoschisis in highly myopic eyes without macular hole or retinal detachment. Am J Ophthalmol. 2006;142(3):497–500. | ||
Gaucher D, Haouchine B, Tadayoni R, et al. Long-term follow-up of high myopic foveoschisis: natural course and surgical outcome. Am J Ophthalmol. 2007;143(3):455–462. | ||
Shimada N, Ohno-Matsui K, Yoshida T, Sugamoto Y, Tokoro T, Mochizuki M. Progression from macular retinoschisis to retinal detachment in highly myopic eyes is associated with outer lamellar hole formation. Br J Ophthalmol. 2008;92(6):762–764. | ||
Ikuno Y, Sayanagi K, Soga K, Oshima Y, Ohji M, Tano Y. Foveal anatomical status and surgical results in vitrectomy for myopic foveoschisis. Jpn J Ophthalmol. 2008;52(4):269–276. | ||
Kumagai K, Furukawa M, Ogino N, Larson E. Factors correlated with postoperative visual acuity after vitrectomy and internal limiting membrane peeling for myopic foveoschisis. Retina. 2010;30(6):874–880. | ||
Fujii GY, De Juan E Jr, Humayun MS, et al. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology. 2002;109(10):1807–1812; discussion 1813. | ||
Shimada H, Nakashizuka H, Mori R, Mizutani Y. Expanded indications for 25-gauge transconjunctival vitrectomy. Jpn J Ophthalmol. 2005;49(5):397–401. | ||
Recchia FM, Scott IU, Brown GC, Brown MM, Ho AC, Ip MS. Small-gauge pars plana vitrectomy: a report by the American Academy of Ophthalmology. Ophthalmology. 2010;117(9):1851–1857. | ||
Thompson JT. Advantages and limitations of small gauge vitrectomy. Surv Ophthalmol. 2011;56:162–172. | ||
Kobayashi H, Kishi S. Vitreous surgery for highly myopic eyes with foveal detachment and retinoschisis. Ophthalmology. 2003;110(9):1702–1707. | ||
Kanda S, Uemura A, Sakamoto Y, Kita H. Vitrectomy with internal limiting membrane peeling for macular retinoschisis and retinal detachment without macular hole in highly myopic eyes. Am J Ophthalmol. 2003;136(1):177–180. | ||
Spaide RF, Fisher Y. Removal of adherent cortical vitreous plaques without removing the internal limiting membrane in the repair of macular detachments in highly myopic eyes. Retina. 2005;25(3):290–295. | ||
Kwok AK, Lai TY, Yip WW. Vitrectomy and gas tamponade without internal limiting membrane peeling for myopic foveoschisis. Br J Ophthalmol. 2005;89(9):1180–1183. | ||
Hirakata A, Hida T. Vitrectomy for myopic posterior retinoschisis or foveal detachment. Jpn J Ophthalmol. 2006;50(1):53–61. | ||
Panozzo G, Mercanti A. Vitrectomy for myopic traction maculopathy. Arch Ophthalmol. 2007;125(6):767–772. | ||
Kuhn F. Internal limiting membrane removal for macular detachment in highly myopic eyes. Am J Ophthalmol. 2003;135(4):547–549. | ||
Ikuno Y, Gomi F, Tano Y. Potent retinal arteriolar traction as a possible cause of myopic foveoschisis. Am J Ophthalmol. 2005;139(3):462–467. | ||
Sayanagi K, Ikuno Y, Tano Y. Tractional internal limiting membrane detachment in highly myopic eyes. Am J Ophthalmol. 2006;142(5):850–852. | ||
Shimada N, Sugamoto Y, Ogawa M, Takase H, Ohno-Matsui K. Fovea-sparing internal limiting membrane peeling for myopic traction maculopathy. Am J Ophthalmol. 2012;154(4):693–701. | ||
Shin JY, Yu HG. Visual prognosis and spectral-domain optical coherence tomography findings of myopic foveoschisis surgery using 25-gauge transconjunctival sutureless vitrectomy. Retina. 2012;32(3):486–492. | ||
Taniuchi S, Hirakata A, Itoh Y, Hirota K, Inoue M. Vitrectomy with or without internal limiting membrane peeling for each stage of myopic traction maculopathy. Retina. 2013;33(10):2018–2025. | ||
Kumagai K, Ogino N. Results of epiretinal membrane removal combined with PEA and IOL. Semin Ophthalmol. 2001;16(3):151–157. | ||
Kim KS, Lee SB, Lee WK. Vitrectomy and internal limiting membrane peeling with and without gas tamponade for myopic foveoschisis. Am J Ophthalmol. 2012;153(2):320–326.e1. | ||
Ratiglia R, Osnaghi S, Bindella A, Pirondini C. Posterior traction retinal detachment in highly myopic eyes: clinical features and surgical outcome as evaluated by optical coherence tomography. Retina. 2005;25(4):473–478. | ||
Yeh SI, Chang WC, Chen LJ. Vitrectomy without internal limiting membrane peeling for macular retinoschisis and foveal detachment in highly myopic eyes. Acta Ophthalmol. 2008;86(2):219–224. | ||
Abdelkader E, Lois N. Internal limiting membrane peeling in vitreo-retinal surgery. Surv Ophthalmol. 2008;53(4):368–396. | ||
Gao X, Ikuno Y, Fujimoto S, Nishida K. Risk factors for development of full-thickness macular holes after pars plana vitrectomy for myopic foveoschisis. Am J Ophthalmol. 2013;155(6):1021–1027.e1. | ||
Govetto A, Virgili G, Menchini F, Lanzetta P, Menchini U. A systematic review of endophthalmitis after microincisional versus 20-gauge vitrectomy. Ophthalmology. 2013;120(11):2286–2291. | ||
Inoue M, Shinoda K, Shinoda H, Kawamura R, Suzuki K, Ishida S. Two-step oblique incision during 25-gauge vitrectomy reduces incidence of postoperative hypotony. Clin Experiment Ophthalmol. 2007;35(8):693–696. | ||
Kunimoto DY, Kaiser RS; Wills Eye Retina Service. Incidence of endophthalmitis after 20- and 25-gauge vitrectomy. Ophthalmology. 2007;114(12):2133–2137. | ||
Ikuno Y, Asai T, Yano S, Nishida K. [Small gauge vitrectomy in macular surgery for myopic complications]. Nihon Ganka Gakkai Zasshi. 2012;116(12):1130–1136. Japanese. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.