Back to Journals » International Journal of Women's Health » Volume 17
Fatal Umbilical Cord Hemorrhage Triggering Neonatal Demise: Clinicopathological Insights from the Case Analysis
Received 24 May 2025
Accepted for publication 23 August 2025
Published 29 August 2025 Volume 2025:17 Pages 2741—2745
DOI https://doi.org/10.2147/IJWH.S542329
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Tianshui Yu,1 Baoqing Pei,2 Dong Zhao1
1Key Laboratory of Evidence Science (China University of Political Science and Law), Ministry of Education, Beijing, 100088, People’s Republic of China; 2Beijing Key Laboratory for Design and Evaluation Technology of Advanced Implantable and Interventional Medical Devices, Beijing Advanced Innovation Center for Biomedical Engineering, School of Biological Science and Medical Engineering, Beihang University, Beijing, 100083, People’s Republic of China
Correspondence: Tianshui Yu, Key Laboratory of Evidence Science (China University of Political Science and Law), Ministry of Education, No. 25, Xitucheng Road, Haidian District, Beijing, 100088, People’s Republic of China, Tel +86 10 62921002 (Ext.), Fax +86 10 68633318, Email [email protected]
Background: Umbilical cord hemorrhage (UCH) is a rare but catastrophic obstetric emergency associated with nearly 50% fetal mortality, and its precise pathogenic mechanisms remain elusive in clinical practice. The pathophysiological cascade involves hemorrhagic expansion from ruptured umbilical vessels predominantly the umbilical vein which generates compressive forces on adjacent umbilical arteries within the constrained Wharton’s jelly. This acute vascular compromise precipitates the sudden cessation of fetoplacental circulation, culminating in irreversible hypoxic-ischemic injury. Although the pathogenesis of UCH is multifactorial, the structural vulnerabilities of the umbilical vessels particularly elastic fiber deficiencies in the umbilical vein remain understudied. This case report describes a clinical outcome characterized by multifocal hemorrhagic lesions along the umbilical cord resulting from congenital elastic fiber deficiency in the umbilical vein during the late gestational stages, culminating in neonatal death despite emergent intervention.
Case Report: A 31-year-old primigravida at 40+4 weeks gestation presented with abdominal pain and vaginal bleeding. Ultrasonography revealed cephalic presentation with the umbilical cord encircling the neck and torso once each. Following abrupt fetal bradycardia (80 bpm), fetal membrane was artificially ruptured, resulting in the release of 10 mL of yellowish-green amniotic fluid, which was classified as thick and contaminated to degree III. An emergency cesarean section was performed, delivering a male neonate (3,670 g). The Apgar scores were 10/2/0 at 1/5/10 min. Despite T-piece ventilation and chest compressions, resuscitation failed, resulting in neonatal death. Histopathological and macroscopic autopsy analyses revealed umbilical cord hemorrhage accompanied by umbilical vascular anomalies, specifically demonstrating a significant deficiency or complete absence of elastic fibers within the umbilical vein wall.
Conclusion: Umbilical vein dysplasia, characterized by elastic fiber deficiency, is an underrecognized yet critical contributor to perinatal hemorrhage-related mortality, particularly in cases of mechanical cord compression. We propose systematic elastin-specific histochemical evaluation as an essential component of postmortem protocols for unexplained intrauterine fetal demise. This evidence underscores the need to develop antenatal surveillance strategies targeting high-risk cord structural cord anomalies, specifically incorporating elastin-specific screening.
Keywords: umbilical cord bleeding, umbilical cord entanglement, umbilical vein dysplasia, elastic fiber
Introduction
The umbilical cord serves as the sole vital conduit for gas exchange, nutrient transfer, and waste elimination between the fetus and the placenta. In a full-term pregnancy, the umbilical cord measures 30–100 cm in length and 0.8–2.0 cm in diameter, comprising two umbilical arteries and one umbilical vein. Umbilical vessels are encased in a distinctive gelatinous tissue known as Wharton’s jelly. This tissue is colorless and translucent due to its high moisture content, which protects the umbilical vessels. Umbilical cord hematoma (UCH) is a rare cause of morbidity and mortality in neonates. This pathology may occur during pregnancy or, more frequently, during labor and is characterized by a hemorrhagic mass within the Wharton’s jelly of the umbilical cord, primarily localized near the fetal insertion of the umbilical cord. The hematoma may compress the vessels, specifically the two umbilical arteries and one umbilical vein, compromising maternal-fetal circulation and leading to an acute deficit in fetal blood supply. The umbilical vein exhibits a thinner wall, rendering it more vulnerable to compression and dilation.1 Consequently, neonatal hypoxia occurs, a condition that can be lethal without prompt extraction of the fetus.
This report presents a case of multiple umbilical cord hemorrhage occurring at the end of term pregnancy, that resulted in neonatal fatalities. This case emphasizes the importance of assessment of underlying causes of umbilical cord hemorrhage and its relationship to causes of death in clinical diagnosis and death cause analysis.
Case Presentation
A 31-year-old primigravida presented with negative general and obstetric histories. The patient was admitted at 40 weeks and 4 days of gestation because of persistent lower abdominal pain lasting 3 h, accompanied by minimal vaginal bleeding. Color ultrasonography indicated that the fetus was in the cephalic position, with the umbilical cord wrapped around the neck and body in a single loop. An electronic fetal heart rate monitor indicated a reactive non-stress test with a fetal heart rate of 148 bpm. Forty minutes post-admission, the obstetrician auscultated the fetal heart rate at 80 bpm and promptly performed manual rupture of the amniotic membranes, leading to the release of 10 mL of yellowish-green amniotic fluid, which was classified as thick and contaminated to degree III. After 10 min, a caesarean section of the lower uterine segment was performed, resulting in the delivery of a live male infant in the right occiput posterior position, with a birth weight of 3670 g. The Apgar scores were 10 and 2 (one point each was awarded for heart rate and respiration) at 1 and 5 min post-birth, respectively. Positive pressure ventilation used a T-piece face mask for connection to an endotracheal tube, prompting the initiation of chest compressions. The Apgar score was 0 at 10 min post-birth. Resuscitative maneuvers proved unsuccessful, and clinical death was declared 1 h and 40 min after birth.
An autopsy was conducted on the third day after the neonate’s death. The neonate was male, weighing 3,600 g and 50 cm in length. The autopsy revealed pathological findings consistent with acute death characterized by cerebral edema and multiple organ congestion. The placenta weighed of 665 g and measured 17.5×15.5 ×2.2 cm. The umbilical cord was attached to the placenta at an eccentric location, with 32 cm of length remaining on the placenta, displaying slight spiral curling and subamniotic hemorrhage (Figure 1A). The umbilical cord at the base of the umbilicus in the fetus has been severed and tightly sutured on both sides, exhibiting a fusiform brownish alteration, measuring 6.4 cm in length and 3.3 cm in width at its widest point (Figure 1A). Continuous transverse sections demonstrated significant Wharton’s jelly hemorrhage, resulting in hematoma formation around the umbilical vein and two umbilical arteries, extending to the amniotic membrane (Figure 1B). The umbilical arteries exhibited notable thinning, which was difficult to observe visually due to hematoma compression. Microscopic analysis revealed that the umbilical vein lacked a muscular layer, which led to thinning and structural discontinuity (Figure 2A). Staining of the elastic fibers revealed a notable reduction or total absence of the purple internal elastic membrane in the umbilical vein as well as purple elastic fibers in the tunica media of the umbilical vein (Figure 2B). Considerable hemorrhage of the Wharton’s jelly surrounding the umbilical vein and arteries extending to the amniotic membrane resulted in significant compression of both umbilical arteries, as observed by microscopic analysis (Figure 3A and B).
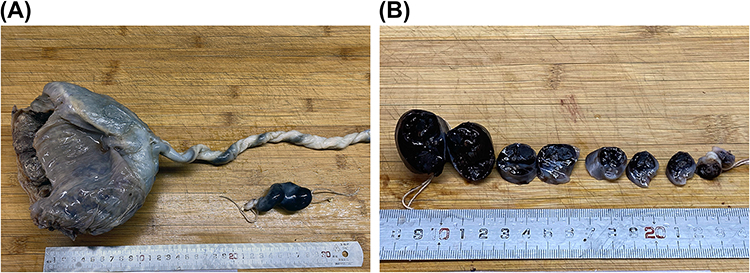 |
Figure 1 Gross findings of the placenta and umbilical cord. (A) The umbilical cord attached to the placenta exhibited a slight spiral curling and subamniotic hemorrhage. The umbilical cord at the base of the umbilicus in the fetus has been severed and tightly sutured on both sides, exhibiting a fusiform brownish alteration. (B) The continuous transverse sections of the umbilical cord at the base of the umbilicus in the fetus demonstrated extensive hemorrhage of Wharton’s jelly, resulting in hematoma formation around the umbilical vein and the two umbilical arteries, which extended to the amniotic membrane. |
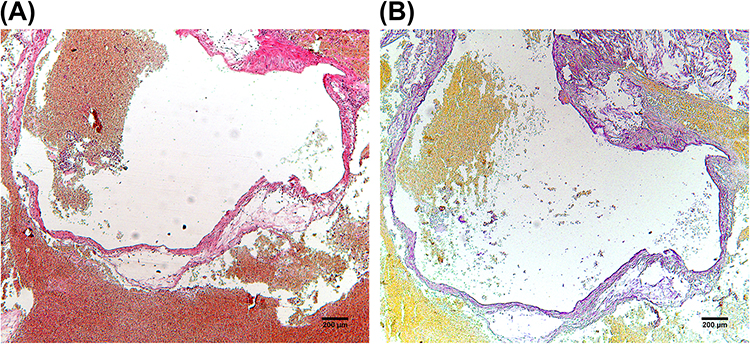 |
Figure 2 Microscopic observations of the umbilical vein. (A) The umbilical vein lacked a muscular layer, leading to thinning and structural discontinuity as observed through HE staining. (B) A notable reduction or total absence of the purple internal elastic membrane in the umbilical vein, along with the purple elastic fibers in the tunica media of the umbilical vein by staining of elastic fibers. The scale bar, 200 µm. |
 |
Figure 3 Microscopic observations of the umbilical arteries. (A and B) HE staining demonstrates Wharton’s jelly hemorrhage compressing both umbilical arteries. The scale bar, 200 µm. |
Discussion
From a clinical perspective, this case illustrates acute intrapartum fetal distress characterized by sudden fetal heart rate deceleration and meconium-stained amniotic fluid that progressed rapidly from initial clinical stability to acute fetal decompensation. Despite an initial Apgar score of 10 at 1 min, the neonate developed critically low scores (5 min: 2; 10 min: 0) and succumbed within 100 min post-delivery. Notably, this outcome underscores the limited sensitivity of Apgar scoring in assessing oxygenation and metabolism, as neonates may experience severe hypoxia and metabolic acidosis despite normal/near-normal Apgar assessments.2 However, sustained arterial compression leads to rapid deoxygenation, evidenced by significant cord arterial pH decline with the bradycardia-to-delivery interval, at a rate of 0.009 per minute.3 Therefore, mandatory umbilical cord blood analysis (pH, blood gases, lactate) is essential for accurate evaluation of perinatal hypoxia-acidosis.4
The umbilical cord, comprising three vital blood vessels (typically two arteries and one vein), serves as a critical lifeline between the mother and fetus. Prenatal care includes detailed ultrasound examination of the umbilical cord, complemented by postnatal inspection of the placenta and umbilical cord, to identify and mitigate potential complications.5 Color ultrasonography serves as the gold standard for the prenatal diagnosis of umbilical cord entanglement. The sensitivity and specificity of prenatal ultrasound diagnosis of umbilical cord conditions are 80–96.8% and 87–96%, respectively.6 Color ultrasonography revealed umbilical cord entanglement in the fetus in this case. The prevalence of umbilical cord entanglement increases progressively with maternal gestational age, and it frequently leads to umbilical cord compression during delivery.2 Umbilical cord entanglement refers to wrapping of the umbilical cord around the neck, limbs, or trunk of the fetus. Incidence rate of pregnancies involving entanglement around the neck is 14.7–33.9%.7 The effects on perinatal outcomes are comparable for umbilical cord entanglement around the neck and trunk but lower for entanglement around the limb.8,9 Umbilical cord wrapping around the neck typically involves a single loop around the neck, which exerts minimal influence on safe length, and secondary hemorrhage of umbilical vessels is rare. In this case, at 40 weeks and 4 days of gestation, the umbilical cord exhibited complex entanglement around the fetal neck and torso, accompanied by significant cord hemorrhage. This presentation suggests associations with multiple entanglement sites and prolonged compression duration.
The postmortem identification of Wharton’s jelly hematoma, as described in this case, may lead to significant adverse outcomes, such as fetal distress, intrauterine death, and neonatal asphyxia, which can occur during or following delivery.9 Therefore, umbilical cord hemorrhage represents a critical obstetric emergency, necessitating meticulous evaluation of umbilical cord integrity to elucidate underlying etiologies. The rupture of the umbilical vein—a vessel anatomically predisposed to failure owing to its thin walls and high capacitance (transporting 50–60% of umbilical blood flow)—represents the primary pathomechanism initiating hemorrhagic cascades in the Wharton’s jelly.10 The extravasation of blood into the Wharton’s jelly, a proteoglycan-rich matrix normally resistant to compression, generates space-occupying hematomas that exert radial pressure on adjacent umbilical arteries.11 Computational modeling indicates that a hematoma volume >5 cm³ creates intracordal pressures >30 mmHg, sufficient to collapse the low-pressure umbilical arterial system in late gestation.12
Wharton’s jelly hematomas are particularly insidious because of their dual roles as both mechanical disruptors and biochemical stressors. Hemoglobin degradation products, including free iron and heme, induce oxidative damage to adjacent cord structures, weakening vascular integrity.13 Additionally, thrombin released during clot formation activates protease-activated receptors on umbilical smooth muscle cells, triggering vasospasm and exacerbating circulatory stasis.14 These mechanisms together create a “no-reflow” phenomenon, where even hematoma resolution fails to restore adequate perfusion. Clinically, this manifests as sudden fetal heart rate decelerations (prolonged late decelerations with loss of variability) or atypical sinusoidal patterns, often misinterpreted as placental insufficiency rather than cord-specific pathology. Additionally, postmortem findings of fusiform brownish swelling in the umbilical arteries correlate with intimal necrosis and thrombosis, which are hallmarks of prolonged ischemia-reperfusion injury. Notably, the localization of hematomas near the fetal umbilicus, a region with reduced Wharton’s jelly thickness, amplifies vascular compression risks, as the cord’s diameter-to-jelly ratio here is lower than that in mid-cord segments.15
Owing to the absence of routine prenatal vascular elastography in this case, early detection of vascular wall abnormalities was not feasible, delaying diagnostic intervention. Additionally, as this is a case report, our findings cannot establish causal relationships or prevalence rates. Future multicenter studies with longitudinal prenatal monitoring are required to validate the association between elastic fiber loss and UCH.
Conclusion
The etiology of Wharton’s jelly hemorrhage remains multifactorial, with the following potential risk factors identified in this case: (1) umbilical cord anomalies, such as wrapping; and (2) umbilical vessel wall abnormalities, including congenital dysplasia of the muscle layer or elastic fibers. Therefore, acquiring clinical data regarding umbilical cord entanglement and utilizing elastic fiber staining to detect umbilical vessel wall abnormalities are essential for clinical diagnosis and death cause analysis.
Ethics Approval and Consent to Participate
Ethical approval was required for case reports according to th guidelines of our institution. This work was approved by Ethics Committee, Institute of Evidence Law and Forensic Science, China University of Political Science and Law, and was performed in accordance with the 1964 Declaration of Helsinki.
Consent Statement
Written informed consent was obtained from the patient for publication of this case report and the accompanying images.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gualandri G, Rivasi F, Santunione AL, et al. Spontaneous umbilical cord hematoma: an unusual cause of fetal mortality: a report of 3 cases and review of the literature. Am J Forensic Med Pathol. 2008;29(2):185–190. doi:10.1097/PAF.0b013e318174e7e1
2. Peesay M. Nuchal cord and its implications. Matern Health Neonatol Perinatol. 2017;3:28. doi:10.1186/s40748-017-0068-7
3. Wong L, Kwan AHW, Lau SL, et al. Umbilical cord prolapse: revisiting its definition and management. Am J Obstet Gynecol. 2021;225(4):357–366. doi:10.1016/j.ajog.2021.06.077
4. Olofsson P. Umbilical cord pH, blood gases, and lactate at birth: normal values, interpretation, and clinical utility. Am J Obstet Gynecol. 2023;228(5S):S1222–S1240. doi:10.1016/j.ajog.2022.07.001
5. Remorgida V, Nicosia A, Leo L, et al. Aberrant number of vessels in the umbilical cord: what do we know? Sci. 2024;6:65. doi:10.3390/sci6040065
6. Sherer DM, Roach C, Soyemi S, et al. Current perspectives of prenatal sonographic diagnosis and clinical management challenges of complex umbilical cord entanglement. Int J Womens Health. 2021;13:247–256. doi:10.2147/IJWH.S285860
7. Mariya T, Fujibe Y, Shinkai S, et al. Multiple part umbilical cord entanglement and neonatal outcomes. Taiwan J Obstet Gynecol. 2018;57(5):672–676. doi:10.1016/j.tjog.2018.09.001
8. Beer N, Danieli-Gruber S, Bardin R, et al. Adverse outcomes of nonnuchal umbilical cord entanglement. Int J Gynaecol Obstet. 2024;164(1):66–172. doi:10.1002/ijgo.14992
9. Hayes DJL, Warland J, Parast MM, et al. Umbilical cord characteristics and their association with adverse pregnancy outcomes: a systematic review and meta-analysis. PLoS One. 2020;15(9):e0239630. doi:10.1371/journal.pone.0239630
10. Isotani N, Kanahashi T, Imai H, et al. Regional differences in the umbilical vein and ductus venosus at different stages of normal human development. Anat Rec. 2024;307(10):3306–3326. doi:10.1002/ar.25421
11. Xiao T, Guo W, Chen M, et al. Fabrication and in vitro study of tissue-engineered cartilage scaffold derived from jelly extracellular matrix. Biomed Res Int. 2017;2017:5839071. doi:10.1155/2017/5839071
12. Baschat AA. Fetal responses to placental insufficiency: an update. BJOG. 2004;111(10):1031–1041. doi:10.1111/j.1471-0528.2004.00273.x
13. Tang Y, Yang S, Yao M, et al. Hemoglobin induces inflammation through NF-kB signaling pathway and causes cell oxidative damage in grass carp (Ctenopharyngodon idella). Front Immunol. 2022;13:1044299. doi:10.3389/fimmu.2022.1044299
14. El-Daly M, Saifeddine M, Mihara K, et al. Proteinase-activated receptors 1 and 2 and the regulation of porcine coronary artery contractility: a role for distinct tyrosine kinase pathways. Br J Pharmacol. 2014;171(9):2413–2425. doi:10.1111/bph.12593
15. Brunelli R, De Spirito M, Giancotti A, et al. The biomechanics of the umbilical cord Wharton’s jelly: roles in hemodynamic proficiency and resistance to compression. J Mech Behav Biomed Mater. 2019;100:103377. doi:10.1016/j.jmbbm.2019.103377
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.