Back to Journals » International Journal of Women's Health » Volume 18
Fatal Retroperitoneal Desmoid-Type Fibromatosis Masquerading as Uterine Fibroid with Colonic Invasion and Fecal Peritonitis: A Case Report
Authors Owais M ![]() , Manzoor MU
, Manzoor MU ![]() , Haider MS, Mukhtar H, Ali H, Afzal A, Noreen F, Shidane AA
, Haider MS, Mukhtar H, Ali H, Afzal A, Noreen F, Shidane AA ![]() , Mohamed ZI
, Mohamed ZI ![]()
Received 5 May 2026
Accepted for publication 16 June 2026
Published 19 June 2026 Volume 2026:18 622078
DOI https://doi.org/10.2147/IJWH.S622078
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Muhammad Owais,1 Muhammad Umair Manzoor,1 Muhammad Salal Haider,1 Hammad Mukhtar,2 Huda Ali,2 Ayesha Afzal,3 Fozia Noreen,4 Abdinasir Adam Shidane,5 Zakariye Isak Mohamed5
1Department of Medicine, Wah Medical College, National University of Medical Sciences, Rawalpindi, Pakistan; 2Department of Surgery, Pof Hospital, Wah Cantt, Pakistan; 3Pharmacology Department, Wah Medical College (NUMS), Wah Cantt, Pakistan; 4Department of Pathology, Pof Hospital, Wah Cantt, Pakistan; 5Faculty of Medicine and Surgery, Somali National University, Mogadishu, Somalia
Correspondence: Abdinasir Adam Shidane, Faculty of Medicine and Surgery, Somali National University, Mogadishu, Somalia, Email [email protected]
Abstract: Desmoid-type fibromatosis is a rare, locally aggressive mesenchymal neoplasm that accounts for fewer than 0.03% of all tumors. Its retroperitoneal variant in young women closely mimics uterine leiomyoma on pelvic ultrasonography. When the diagnosis of desmoid-type fibromatosis is delayed, the tumor can silently invade adjacent viscera with fatal consequences. A 21-year-old woman presented with lower abdominal pain and a large pelvic mass on ultrasonography. The mass was labelled a uterine fibroid, and she was discharged. Two days later, she returned with an acute abdomen; CT revealed a 29 cm retroperitoneal mass with pneumoperitoneum. Emergency laparotomy confirmed colonic invasion and perforation with gross fecal peritonitis. Debulking colectomy with colostomy was performed; complete resection was not achievable. Histopathology was morphologically consistent with desmoid-type fibromatosis; confirmatory immunohistochemistry was not performed. Postoperatively, the patient developed refractory septic shock driven by an MDR Escherichia coli wound infection. Serum lactate never normalized across thirteen serial measurements over nine days from admission to death. She died nine days after presentation with a terminal lactate of 4.8 mmol/L and combined metabolic and respiratory failure. This case shows how retroperitoneal desmoid-type fibromatosis (DTF) can precisely replicate a uterine fibroid on ultrasound when it compresses but does not invade the uterus. Sporadic desmoid disease can reach catastrophic size silently and cause hollow-viscus perforation. Any large pelvic mass with bilateral ureteric obstruction in a young woman should prompt cross-sectional imaing before discharge.
Keywords: desmoid-type fibromatosis, retroperitoneal tumor, uterine fibroid mimic, bowel perforation, fecal peritonitis, septic shock, diagnostic errors, fibromatosis, aggressive
Introduction
Desmoid-type fibromatosis (DTF), also known as aggressive fibromatosis or desmoid tumor, is a rare clonal proliferation of myofibroblasts arising from musculoaponeurotic structures of the deep soft tissues.1,2 Although it lacks metastatic potential, its relentless local invasiveness renders it functionally malignant in anatomically critical locations. The annual incidence is approximately 2 to 6 cases per million population worldwide, accounting for roughly 0.03% of all neoplasms and fewer than 3% of all soft-tissue tumours.1,2
DTF carries a well-recognized predilection for young women of reproductive age, among whom the anterior abdominal wall is the dominant site.2 Intra-abdominal desmoids, comprising mesenteric and retroperitoneal variants, account for roughly 8% of all DTF and most commonly arise in the setting of familial adenomatous polyposis (FAP). Sporadic retroperitoneal DTF without FAP or Gardner syndrome is distinctly uncommon, accounting for fewer than 3% of all desmoid tumors in published case series.3,4 In the pelvis, a large retroperitoneal desmoid can compress the uterus, adnexa, and bladder so intimately that it is indistinguishable from a uterine leiomyoma on standard ultrasonography, a diagnostic trap that has been described in isolated case reports.4,5 The role of ultrasound and MRI in characterizing pelvic masses has been well described; while ultrasound remains the first-line modality, MRI provides superior soft-tissue contrast and is essential for defining tumor origin, extent, and relationship to adjacent structures in ambiguous cases.6 Furthermore, intra-abdominal DTF involving the ureter following gynecologic surgery has also been documented, underscoring the tumor’s capacity to encroach upon critical pelvic structures beyond the uterus itself.7
Although most intra-abdominal desmoids follow an indolent course of silent enlargement, a subset progresses to hollow-viscus obstruction, fistulation, or perforation.8–10 Such presentations carry high surgical morbidity and, in resource-limited environments where cross-sectional imaging is not reflexively obtained for pelvic masses in young women, they may culminate in death. We report a 21-year-old woman whose retroperitoneal desmoid fibromatosis was labelled a uterine fibroid on ultrasonography and who subsequently died of fecal peritonitis and MDR septic shock. This case was written and reported in conformance with the 2020 SCARE (Surgical Case Report) guidelines.11
Case Presentation
Initial Presentation
A 21-year-old unmarried woman presented to the emergency department of a tertiary-level hospital in northern Pakistan on 29 November 2025 with a two-day history of progressive hypogastric pain. She left with iliac fossa pain accompanied by six to seven episodes of vomiting and loose stool. She had no prior surgical history, no known family history of colorectal polyposis or soft-tissue tumors, and was not pregnant (serum beta-hCG <0.1 mIU/mL). She had been told previously, on an outpatient ultrasound, that she had a uterine fibroid.
On examination, she was hemodynamically stable with a blood pressure of 118/76 mmHg and a heart rate of 94 beats per minute. Abdominal examination revealed a large, firm, non-tender pelvic mass extending to the umbilicus. There was no peritonism. She was admitted under the gynecology service.
Pelvic ultrasonography demonstrated a large heterogeneous mass arising from the pelvis, with the largest lesion measuring 14.5 × 11 cm. The mass was reported as consistent with multiple uterine fibroids, with the largest component in the fundal region. Bilateral hydronephroureter was noted, attributed to ureteric compression by the mass. Laboratory investigations revealed hemoglobin 10.1 g/dL, creatinine 1.33 mg/dL (above the female upper limit of 1.1), D-dimer 4,507 ng/mL (reference <500 ng/mL), LDH 264 U/L, and a lactate of 2.0 mmol/L on arterial blood gas. Serum CA-125 was mildly elevated at 38.9 U/mL, attributable to peritoneal irritation. She was managed with analgesics and antiemetics and discharged.
Acute Deterioration and Emergency Laparotomy
She returned to the emergency department two days later, on 1 December 2025, with sudden-onset severe, diffuse abdominal pain and clinical signs of generalized peritonitis. She was tachycardic (heart rate 110 bpm), tachypneic (respiratory rate 24/minute), and in evident distress. Repeat arterial blood gas demonstrated a lactate of 3.7 mmol/L with compensated metabolic acidosis (pH 7.46, HCO3 16.4 mEq/L, PCO2 22.7 mmHg), signifying established tissue hypoperfusion despite preserved hemodynamic parameters, a presentation consistent with cryptic septic shock.
Emergency contrast-enhanced CT of the abdomen and pelvis revealed a 13 × 12.7 × 29 cm heterogeneous pelvic mass, the smaller dimensions reported on initial ultrasonography (14.5 × 11 cm) reflected only the dominant cross-sectional plane visible on pelvic ultrasound; the craniocaudal long axis of 29 cm was not captured, consistent with the known limitation of ultrasound in defining the full extent of retroperitoneal masses, with moderate free pneumoperitoneum, bilateral hydronephrosis, bilateral pleural effusions with passive basal collapse on chest cuts, and minimal ascites. The mass was fixed in the pelvis and appeared to arise from the retroperitoneum rather than from the uterus. Emergency laparotomy was performed within 6 hours of re-admission.
Operative Findings and Procedure
At laparotomy, the following findings were documented: pneumoperitoneum; gross fecal peritonitis with frank pus; direct invasion and perforation of the descending colon by the tumor; a large retroperitoneal mass occupying almost half of the abdominal cavity, fixed in the pelvis, and arising from the retroperitoneum (Figure 1); uterine compression by the tumor without uterine invasion; and macroscopic omental lesions. The intraoperative diagnosis was unclear; the lesion had the appearance of a sarcoma or aggressive mesenchymal neoplasm.
 |
Figure 1 Intraoperative view demonstrating a massive, solid retroperitoneal tumor (approximately 29 cm) directly invading the descending colon. Note the presence of gross fecal contamination and macroscopic omental lesions, confirming visceral perforation and macroscopic omental involvement, most likely reflecting peritoneal contamination at the time of colonic perforation rather than true metastatic spread. |
Distal transverse and descending colectomy with transverse end colostomy was performed. Tumor debulking was performed; complete excision was not achieved, and margins were macroscopically involved at the conclusion of the procedure. Ureteric stenting was attempted bilaterally for the obstructive uropathy, but could not be accomplished due to tumor fixation. The patient received six units of packed red blood cells intraoperatively owing to operative hemorrhage. The resected colonic segment and tumor tissue were sent for histopathological examination.
Histopathological Findings
Histopathology (Sampled 2 December 2025) demonstrated a spindle cell neoplasm involving the serosal surface of the colon, composed of bland fibroblast-like spindle cells arranged in long sweeping fascicles within a collagenous stroma (Figure 2), with associated thin-walled parallel vessels. Nuclear pleomorphism and mitotic activity were minimal. No necrosis was identified. The morphology was reported as consistent with deep fibromatosis (desmoid tumor). Resection margins were involved (R2 resection). Immunohistochemistry was recommended for confirmation, but results were unavailable at the time of this report.
 |
Figure 2 Photomicrograph of the resected specimen showing classic features of desmoid-type fibromatosis. (A) Spindle-shaped myofibroblasts are arranged in long, sweeping fascicles. (B) Abundant collagenous stroma with thin-walled, elongated blood vessels and an absence of significant nuclear atypia or necrosis (H&E stain, 200x magnification). |
Postoperative Course and Laboratory Trajectory
The postoperative course was dominated by refractory sepsis with progressive multiorgan dysfunction. Empirical broad-spectrum antibiotic therapy was initiated postoperatively. Wound culture subsequently yielded MDR Escherichia coli resistant to all cephalosporins and fluoroquinolones; antibiotic therapy was escalated accordingly, though the specific agents and timeline of escalation are not fully retrievable from institutional records. Blood cultures were obtained; results were not documented in the available case records. Vasopressor support was required to maintain haemodynamic stability, and the patient received ICU-level monitoring throughout her postoperative course. Mechanical ventilation was not instituted, consistent with the terminal trajectory and resource constraints described. Renal replacement therapy was not performed despite evidence of acute kidney injury on laboratory parameters. While 2.0 mmol/L lies at the upper boundary of normal in most laboratories, the local institutional reference range defines normal lactate as <2.0 mmol/L; this value therefore represented the threshold of abnormality at admission, and all subsequent measurements exceeded this level without exception. Serum lactate never normalized across thirteen serial arterial blood gas measurements, an unbroken physiological signature of refractory tissue oxygen debt from admission to death. The patient died on 7 December 2025, nine days after initial presentation, with a terminal pH of 7.30, PO2 of 23.3 mmHg, and lactate of 4.8 mmol/L, representing combined metabolic and respiratory failure. The complete laboratory and arterial blood gas trajectory is detailed in Tables 1 and 2, and Full arterial blood gas interpretation and clinical correlation are provided in the Supplementary File 1.
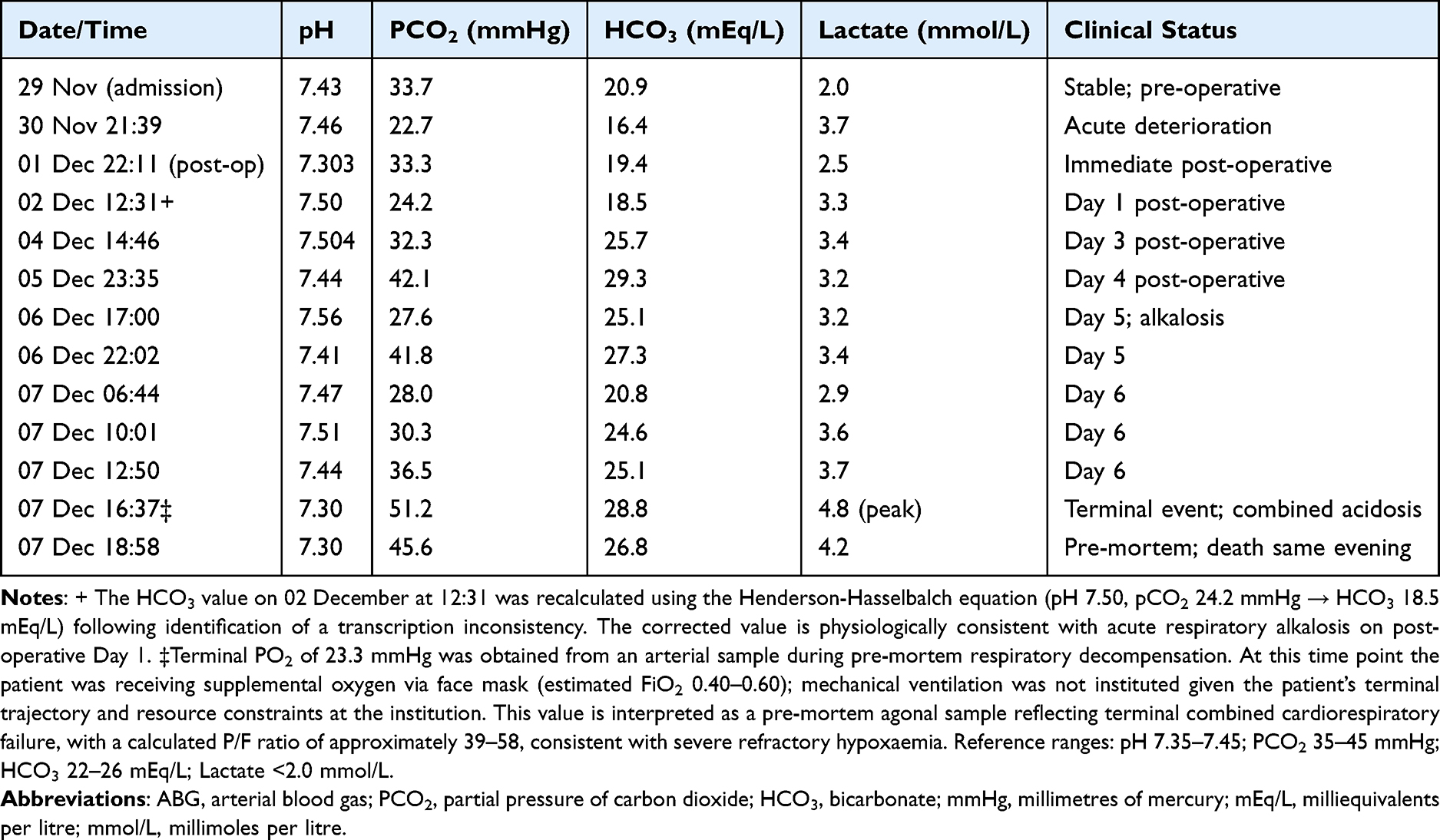 |
Table 1 Serial Arterial Blood Gas and Lactate Values During Admission |
 |
Table 2 Key Laboratory Parameters at Selected Time Points |
Discussion
Diagnostic Mimicry of Retroperitoneal DTF as a Uterine Fibroid
Retroperitoneal DTF does not announce itself. In a 21-year-old woman with a large fixed pelvic mass, leiomyoma is the intuitive diagnosis, and ultrasound confirms what the clinician already suspects. The problem is not that the diagnosis is unreasonable. The problem is that it stops further inquiry.
The operative finding explained the imaging error. The tumor had compressed the uterus from outside without invading it. This external compression replicated the contour and spatial position of a subserosa fibroid on pelvic ultrasound. Hung et al described the same phenomenon in a DTF that mimicked a uterine fibroid while invading the bladder.12 Njoku et al6 reported a giant desmoid presenting as a recurrent uterine myoma in a nulliparous Nigerian woman In each of these cases, the imaging was not wrong. It answered the question it was asked. The question itself was the problem. Furthermore, there is a study demonstrating that Ultrasound cannot determine retroperitoneal tumor origin, tissue composition, or the absence of a uterine plane.13 For instance, A 14.5 cm heterogeneous mass in a 21-year-old with bilateral hydronephroureter and an admission lactate of 2.0 mmol/L was already enough to warrant cross-sectional imaging before discharge. CT would have shown what ultrasound could not. This case was diagnosed on the CT obtained two days later, after the colon had perforated.
Biology of Sporadic Retroperitoneal Desmoid
Sporadic DTF arises from activating mutations in CTNNB1, driving uncontrolled myofibroblast proliferation through the signaling pathway.3,4,14 Oestrogen acts as a co-driver, which explains the well-established female predominance from puberty to age 40. Nevertheless, sporadic DTF is not exclusive to women; cases in male patients have been documented, confirming that biological sex alone should not exclude DTF from the differential diagnosis of retroperitoneal masses.4 Howard et al noted that retroperitoneal desmoids differ from mesenteric variants by growing silently to very large sizes before becoming symptomatic, because the retroperitoneum imposes no anatomical limit on expansion.4 This is what happened here. A 29 cm tumor had reached the point of visceral destruction before it was found.
The omental deposits at laparotomy are worth noting. DTF does not metastasize. The omental involvement in this case most likely reflects peritoneal seeding at the moment of colonic perforation, or multifocal disease, rather than true spread. Howard et al reported that omental involvement in aggressive intra-abdominal DTF is associated with poor surgical outcomes.4,9 Whether this patient had an unusually aggressive sporadic variant or an undetected FAP-associated desmoid cannot be determined. The IHC for nuclear beta-catenin was recommended but never performed before she died.
Bowel Perforation as the Presenting Catastrophe
Colonic perforation from direct DTF invasion is uncommon but documented. Hajri et al reported mesenteric DTF causing jejunal perforation and diffuse peritonitis in a 26-year-old woman, one of fewer than a dozen such cases in the literature.8,15 Ibrahim et al described a 46-year-old man with a 31 cm mesenteric fibromatosis who developed bowel perforation and required urgent laparotomy with temporary stoma formation. What those cases shared with ours was the combination of a large tumour and delayed diagnosis.16
What set this case apart was the retroperitoneal fixation. Hajri et al noted an uneventful postoperative course after complete resection. That was not possible here. The tumor was fixed to the pelvic sidewall, bilateral ureteric stenting failed, and obstructive uropathy remained unrelieved throughout. R2 margins left viable tumor in situ. In a patient already in septic shock, that meant source control was never achieved from the moment the abdomen was closed.
The Never-Clearing Lactate as the Clinical Signature
Serum lactate was 2.0 mmol/L on admission, before peritonitis was clinically evident. Obstructive uropathy, visceral compression, and subclinical peritoneal contamination had already established occult tissue hypoperfusion. Singer et al described this state in the Sepsis-3 consensus as occult tissue hypoperfusion with admission lactate of 2.0 mmol/L, consistent with early septic physiology per Sepsis-3 criteria, where oxygen debt persists without frank hypotension17 and carries the same mortality risk as overt shock.
Lactate never normalized. Across thirteen serial measurements over nine days, it ranged from 2.5 to 4.8 mmol/L, never approaching the normal range. Failure to clear lactate at 6 and 12 hours is a validated mortality predictor and a Sepsis-3 escalation trigger.17 The terminal arterial blood gas told the story plainly. pH fell to 7.30, PCO2 rose to 51.2 mmHg, and PO2 fell to 23.3 mmHg. That was combined metabolic and respiratory failure. The wound grew MDR Escherichia coli resistant to all cephalosporins and fluoroquinolones. These were the antibiotics most likely given empirically in this setting. Tigecycline and colistin, the only active agents remaining, could not reverse a trajectory nine days in the making.
Diagnostic Anchoring and Its Consequences
The label of uterine fibroid, applied on the first admission, was never revised. The bilateral hydronephroureter, the elevated admission lactate, and the clinical profile of a 21-year-old presenting with a 14.5 cm pelvic mass were each sufficient individually to prompt cross-sectional imaging. Together, they made the case with certainty. None of it led to further investigation.
Njoku et al and Al-Jefout et al both identified ultrasound as the initial modality and the diagnostic error as the first event in a chain leading to delayed management.4,5 The broader dangers of anchoring on a presumed fibroid diagnosis without adequate imaging characterization are further illustrated by reports of disseminated peritoneal leiomyomatosis following laparoscopic surgery with power morcellation — a complication arising directly from failure to characterize a pelvic mass before surgical intervention, and a reminder that the consequences of diagnostic anchoring on “fibroid” extend well beyond this case.18 For clinicians working where MRI is unavailable, contrast CT provides adequate characterization of retroperitoneal masses.19 It should be the minimum standard for any pelvic mass presenting with bilateral ureteric obstruction, regardless of how strongly the clinical picture points toward a fibroid.20
Management of Unresectable Intra-Abdominal DTF
Kasper et al recommend active surveillance as the initial strategy for newly diagnosed sporadic DTF, with systemic treatment reserved for progressive or symptomatic disease.21,22 That framework does not apply once there is fecal peritonitis. At that point, surgery is the only option, and the question is what can realistically be achieved.
The minimum was done here. Fecal diversion and colonic resection were accomplished. Debulking a 29 cm tumor fixed to the pelvic sidewall, with bilateral ureteric encasement and omental involvement, is neither curative nor palliative in any meaningful sense. It is damage control against established sepsis, and it was not enough. Had the patient survived, systemic options including nirogacestat, sorafenib, or imatinib would have been considered.23 That conversation never took place. Furthermore, following surgical resection of intra-abdominal tumors with involved margins, the risk of abdominal parasitic tumor implants must be considered and preventive measures discussed as part of the operative planning.18
Limitations
This case report has several limitations that should be considered. First, while the histopathological features were highly suggestive of desmoid-type fibromatosis (DTF), the diagnosis remains presumptive as confirmatory nuclear beta-catenin immunohistochemistry (IHC) was not performed. We acknowledge this as a diagnostic limitation, as IHC is the gold standard for differentiating DTF from other spindle cell neoplasms. Although tissue blocks were available, IHC could not be performed due to resource constraints at our institution prior to the patient’s death, and results therefore remained unavailable at the time of reporting.
Second, there is a lack of primary radiographic and intraoperative visual data. The original CT scan images (DICOM files) were not retrievable from the institutional archives; therefore, the description of the tumor’s extent and visceral compression relies solely on the formal radiologist’s report and the detailed intraoperative findings recorded in the surgical notes.
Conclusion
Retroperitoneal DTF can replicate the ultrasonographic appearance of a uterine fibroid with anatomical precision when it compresses but does not invade the uterus. Ultrasonography cannot reliably distinguish retroperitoneal DTF from a uterine fibroid, whereas contrast-enhanced CT provides immediate clarification of tumor origin and extent. A large pelvic mass, bilateral hydronephroureter, and an elevated admission lactate in a young woman without an obstetric history should prompt cross-sectional imaging before discharge. The diagnosis of fibroid is a working hypothesis, not a conclusion, until imaging proves it.
Once the colon perforates, prognosis depends on source control, which is rarely achievable in fixed retroperitoneal DTF. Sporadic DTF should be included in the differential diagnosis of large heterogeneous pelvic masses in young women, particularly when obstructive uropathy is present. Earlier cross-sectional imaging, prompt multidisciplinary review, and avoidance of diagnostic anchoring on ultrasound may, in future cases, allow the diagnosis to be made before catastrophic complications occur.
Abbreviations
FAP, familial adenomatous polyposis; DTF, Desmoid-type fibromatosis.
Ethics Approval
This case report was conducted in accordance with the principles of the Declaration of Helsinki. Formal ethics committee approval was not required for a single case report at this institution.
Patient Consent
Written informed consent for publication of this case report and accompanying images was obtained from the patient’s next kin.
Acknowledgment
This case report was prepared and reported in conformance with the 2020 SCARE (Surgical Case Report) guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this work.
Disclosure
The authors declare no competing interests in this work.
References
1. Master SR, Mangla A, Shah C. Desmoid tumor. StatPearls - NCBI Bookshelf. 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459231/.
2. Rampone B, Pedrazzani C, Marrelli D, Pinto E, Roviello F. Updates on abdominal desmoid tumors. World J Gastroenterol. 2007;13(45):5985. doi:10.3748/wjg.v13.45.5985
3. Charif MHE, Tarhini H, Dushfunian D, et al. Retroperitoneal desmoid-type fibromatosis: a case report. 2023. Available from: https://www.semanticscholar.org/paper/Retroperitoneal-desmoid-type-fibromatosis%3A-a-case-Charif-Tarhini/c211dce5be4460b146dd49498b8391a4e9d45ba0.
4. Howard JH, Pollock RE. Intra-Abdominal and abdominal wall desmoid fibromatosis. Oncol Therapy. 2016;4(1):57–9. doi:10.1007/s40487-016-0017-z
5. Al-Jefout M, H N, K M, et al. Abdominal wall desmoid tumor mimicking a subserosal uterine leiomyoma. Int J Gene Med. 2011;4:443. doi:10.2147/ijgm.s18951
6. Nguyen XL, Huynh QH, Nguyen PN. Assessing the clinical characteristics and the role of imaging modalities in uterine sarcoma: a single center retrospective study from Vietnam. Clin Ultrasound. 2025;53(7):1527–1537. doi:10.1002/jcu.24046
7. Ono H, Hori K, Tashima L, Tsuruta T, Nakatsuka SI, Ito K. A case of retroperitoneal desmoid-type fibromatosis that involved the unilateral ureter after gynaecologic surgery. Int J Surg Case Reports. 2018;47(C):30–33. doi:10.1016/j.ijscr.2018.03.039
8. Hajri M, Talbi G, Ferjaoui W, et al. Huge mesenteric desmoid-type fibromatosis with unusual presentation: a case report. Ann Med Surg. 2022;78:103741. doi:10.1016/j.amsu.2022.103741
9. Gregory SN, Satterwhite AA, Alexander HR, Blakely AM. Desmoid-type fibromatosis in the setting of malignant peritoneal mesothelioma: a case report of two rare diseases. World J Surg Oncol. 2022;20(1):317. doi:10.1186/s12957-022-02784-y
10. Eren S. A sporadic abdominal desmoid tumour case presenting with intermittent intestinal obstruction. Eur J Pediatr Surg. 2007;17(4):285–288. doi:10.1055/s-2006-924376
11. Agha RA, Franchi T, Sohrabi C, et al. The SCARE 2020 guideline: updating consensus surgical CASE report (SCARE) guidelines. Int J Surg. 2020;84:226–230. doi:10.1016/j.ijsu.2020.10.034
12. Hung YT, Huang YF, Wu PY. Desmoid-type fibromatosis mimicking uterine fibroid invade the urinary bladder: a case report and literature review. Taiwanese J Obstetrics Gynecol. 2023;62(1):158–162. doi:10.1016/j.tjog.2022.04.011
13. Nowosielski K, Witek A, Kapuśniak E, Stawicka-Ociepka E. Ultrasound diagnosis of adnexal masses: the practical usefulness of various malignancy risk prediction models. Ginekologia Onkologiczna. 2017;15(3):194–217. doi:10.15557/cgo.2017.0020
14. Kuwabara H, Katayanagi S, Koganezawa I, et al. Sporadic intra-abdominal desmoid tumor with a very unusual onset: two case reports. J Med Case Reports. 2021;15(1):457. doi:10.1186/s13256-021-03058-z
15. Yu PP, Liu XC, Yin L, Yin G. Aggressive fibromatosis of the sigmoid colon: a case report. World J Gastrointest Oncol. 2024;16(8):3716–3722. doi:10.4251/wjgo.v16.i8.3716
16. Shah M, Azam B. Case report of an intra-abdominal desmoid tumour presenting with bowel perforation. McGill J Med. 2020;10(2):90–92. doi:10.26443/mjm.v10i2.742
17. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (SEpsis-3). JAMA. 2016;315(8):801. doi:10.1001/jama.2016.0287
18. Pham TH, Nguyen VH, Nguyen PN. Abdominal parasitic fibroids after laparoscopic surgery using a power morcellation: a novel insight from vietnam and a narrative review of the literature. J Med Ultrasound. 2024;33(4):402–406. doi:10.4103/jmu.jmu_30_24
19. De Schepper AM, De Beuckeleer L, Vandevenne J, Somville J. Magnetic resonance imaging of soft tissue tumors. Eur Radiol. 2000;10(2):213–223. doi:10.1007/s003300050037
20. Kreuzberg B, Koudelova J, Ferda J, Treska V, Spidlen V, Mukensnabl P. Diagnostic problems of abdominal desmoid tumors in various locations. Eur J Radiol. 2007;62(2):180–185. doi:10.1016/j.ejrad.2007.01.034
21. Kasper B, Baumgarten C, Garcia J, et al. An update on the management of sporadic desmoid-type fibromatosis: a european consensus initiative between Sarcoma Patients Euronet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann Oncol. 2017;28(10):2399–2408. doi:10.1093/annonc/mdx323
22. Fiore M, MacNeill A, Gronchi A, Colombo C. Desmoid-Type fibromatosis. Surg Oncol Clin North Ame. 2016;25(4):803–826. doi:10.1016/j.soc.2016.05.010
23. Ibrahim R, Assi T, Khoury R, et al. Desmoid-type fibromatosis: current therapeutic strategies and future perspectives. Cancer Treat Rev. 2023;123:102675. doi:10.1016/j.ctrv.2023.102675
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.