Back to Journals » Journal of Blood Medicine » Volume 5
Fatal carboplatin-induced immune hemolytic anemia in a child with a brain tumor
Authors Haley K, Russell T, Boshkov L, Leger R, Garratty G, Recht M ![]() , Nazemi K
, Nazemi K
Received 14 December 2013
Accepted for publication 13 February 2014
Published 15 May 2014 Volume 2014:5 Pages 55—58
DOI https://doi.org/10.2147/JBM.S59192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Kristina M Haley,1 Thomas B Russell,2 Lynn Boshkov,3 Regina M Leger,4 George Garratty,4,† Michael Recht,1 Kellie J Nazemi1
1Division of Pediatric Hematology/Oncology, Department of Pediatrics, Oregon Health & Science University, Portland, OR, 2Division of Pediatric Hematology/Oncology, Department of Pediatrics, Wake Forest Baptist Health, Medical Center Blvd, Winston-Salem, NC, 3Departments of Pathology, Medicine and Pediatrics, Oregon Health and Science University, Portland, OR, 4American Red Cross Blood Services, Pomona, CA, USA
†George Garratty passed away March 2014
Abstract: Drug-induced immune hemolytic anemia (DIIHA) is an uncommon side effect of pharmacologic intervention. A rare mediator of DIIHA, carboplatin is an agent used to treat many pediatric cancers. We describe here, the first case of fatal carboplatin induced DIIHA in a pediatric patient and a brief review of the literature. Our patient developed acute onset of multi-organ failure with evidence of complement activation, secondary to a drug induced red cell antibody. Early recognition of the systemic insult associated with carboplatin induced hemolytic anemia may allow for future affected patients to receive plasmapheresis, a potentially effective therapy.
Keywords: hemolytic anemia, carboplatin, glioma, complement fixation, drug-induced hemolysis
Case
An 11-year-old female was being treated for low-grade astrocytoma with carboplatin and vincristine. The patient was also receiving levothyroxine for central hypothyroidism, ondansetron for chemotherapy-induced nausea, omeprazole for gastrointestinal reflux, and trimethoprim-sulfamethoxazole for Pneumocystis jirovecii pneumonia prophylaxis. Notably, she was not receiving any steroids. On day 15 of cycle five (carboplatin dose number 22), the patient reported acute lower back pain prior to receiving chemotherapy. Her physical exam was unremarkable. She had a stable macrocytic anemia and normal platelet count (Table 1). Thought to be of musculoskeletal origin, the back pain resolved with hydromorphone and ibuprofen. Vincristine 2 mg (max dose) and carboplatin 294 mg (175 mg/m2) were administered. She developed abdominal pain, diarrhea, chills, and tachypnea within approximately 8 hours of chemotherapy administration. The following morning, upon arrival at the local emergency room, she was afebrile, tachycardic, hypertensive, tachypneic, and hypoxemic. She had diffuse abdominal tenderness, delayed capillary refill time, and a normal neurologic exam. She had worsening anemia (with rouleaux formation but without schistocytes) and had acute renal failure and hepatitis (Table 1). Transfusion support and broad-spectrum antibiotics were initiated. She was started on continuous positive airway pressure, and remained alert and interactive.
 | Table 1 Vital signs and laboratory values before acute decompensation, on the day of therapy, at the referring hospital, and at our institution |
Possible explanations of the patient’s acute presentation include; hemolytic uremic syndrome (HUS), atypical HUS, viral hepatitis, autoimmune hemolytic anemia, sepsis with disseminated intravascular coagulation (DIC), and toxic exposure. Concurrent with this patient’s presentation, there was an epidemic of HUS occurring in her community. She denied similar exposures to those reported by the affected patients. Review of the peripheral smear did not demonstrate the typical significant schistocytosis found in HUS. Furthermore, stool cultures were negative. While the patient presented acutely with multi-organ failure, she was not febrile and did not have the characteristic distributive shock associated with bacterial sepsis. Blood culture at the time of admission grew non-typable Haemophilis influenzae; repeat cultures after 24 hours of cefepime were negative. It seemed that her severe illness could not be primarily attributed to this positive culture because she was not neutropenic, non-typeable H. influenzae is not typically associated with severe infection, and the culture cleared quickly with appropriate antibiotics.
Computed tomography (CT) of the chest, abdomen, and pelvis done on hospital day 2, demonstrated a small right pleural effusion, multi-focal nodular ground glass and tree-in-bud opacities in both lungs concerning for atypical infections or diffuse alveolar injury, hepatic steatosis versus edema, and edematous kidneys. An endotracheal aspirate culture grew Aspergillus. As she was not neutropenic and had not been on steroids previously, this appeared to be consistent with laboratory contaminant. Furthermore, her chest CT did not reveal the typical findings associated with invasive pulmonary aspergillosis. Serum viral studies were negative except for Epstein–Barr virus (EBV polymerase chain reaction: 320 copies/mL). Serum cortisol was normal at 46 μg/dL. Acetaminophen level was less than 10 μg/mL.
While undergoing dialysis on hospital day 2 the patient complained of severe headache, became lethargic, and required intubation. Her pupils became fixed and dilated. Head CT demonstrated diffuse cerebral and cerebellar edema (Figure 1). An external ventricular drain was placed. Approximately 40 hours into the hospitalization, she had no brain or brainstem activity. She was pronounced dead 64 hours after initial presentation to our hospital.
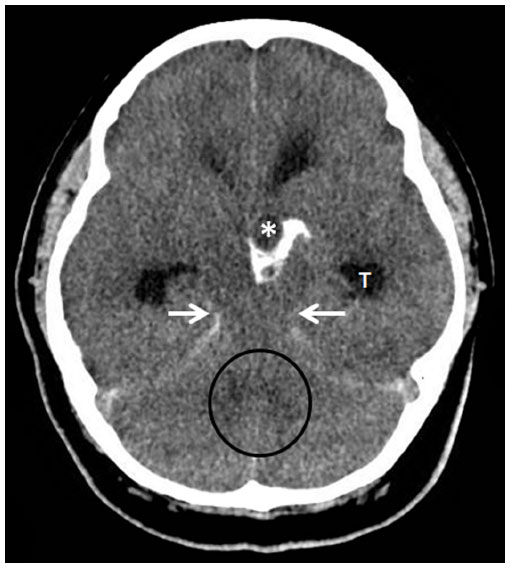 | Figure 1 An axial, non-contrast enhanced view of the brain shows severe diffuse cerebral and cerebellar edema. |
The temporal relationship between the patient’s acute deterioration and the administration of carboplatin and vincristine suggested that one of these agents or the fluids accompanying them was the cause for multi-organ failure and death. The hospital’s carboplatin and vincristine stock concentrations and the patient’s doses were verified. The patient had received the only dose of carboplatin from a specific manufacturer on that day, while many patients had received vincristine from the same supplier. The stock of carboplatin was quarantined. Evaluation for organismal and toxic contamination was unrevealing. An US Food and Drug Administration (FDA) MedWatch alert was placed. No other reports of hemolytic anemia or multi-organ failure were reported in patients receiving carboplatin from this specific manufacturer.
An initial direct anti-globulin test (DAT) at our institution was negative. Evidence of intravascular hemolysis associated with acute renal failure, hepatitis, and coagulopathy, plus concern that the other findings did not fully explain her severe clinical presentation prompted repeat DAT and collection of multiple samples for investigation of carboplatin drug-induced immune hemolytic anemia (DIIHA), by the American Red Cross in Pomona, CA, USA. The repeat DAT was strongly positive for immunoglobulin (Ig)G (3+) and C3 (3+) as well as weakly positive (1+) for IgM. The patient’s serum was found to contain strongly reactive carboplatin-dependent IgG and IgM antibodies that agglutinated (titer =2) and sensitized (titer =32) carboplatin-treated red cells but not untreated red cells. The patient’s serum also agglutinated (titer =16) and sensitized (titer =128) untreated red cells in the presence of a solution of carboplatin; there was no reactivity in the control without drug added. A weak drug-independent antibody was also found in an acid eluate prepared from the patient’s red cells. This testing confirmed carboplatin-induced immune hemolytic anemia.
A post-mortem exam was requested for the patient by our institution, but the family declined.
Discussion
DIIHA is a rare cause of hemolytic anemia with an estimated incidence of one per million individuals.2 Over 125 drugs have been implicated in DIIHA, with additional drugs reported to be associated with hemolysis but not meeting the full criteria for DIIHA.2 The mechanism and severity of hemolysis varies among different drugs. Approximately 15% of the implicated drugs are anti-neoplastic agents.2,3
These drugs cause immune hemolysis through drug-dependent and drug-independent mechanisms. Drug-dependent antibodies can result in hemolytic anemia through two mechanisms.3 In the first, a drug binds covalently to proteins on the red cell membrane, then anti-drug antibodies bind to the drug-red blood cell (RBC) membrane complex, resulting in extravascular hemolysis. Two hypotheses have been proposed to explain the second mechanism.3 According to the immune complex hypothesis; anti-drug antibody combines with the drug to form an immune complex. This immune complex then attaches to the RBC membrane and activates complement. Alternatively, the neoantigen hypothesis suggests that the drug binds to the RBC membrane and changes the membrane forming a novel antigen that is part red cell membrane and part drug. Specific anti-drug antibodies then bind to the neoantigen, which may fix complement.
The mechanism of antibody formation in drug-independent hemolytic anemia is poorly understood but has been attributed to molecular mimicry, drug adsorption causing red cell membrane alteration, or immune dysregulation.3 The antibody reacts in vitro in the absence of drug. Laboratory and clinical findings are identical to RBC autoantibodies and autoimmune hemolytic anemia (AIHA). The treatment of choice for DIIHA is supportive care and immediate withdrawal of the causative agent. Steroids or intravenous IgG are not indicated for drug-dependent DIIHA. However, these therapies may provide some benefit in treatment of drug-independent DIIHA given the similarities to AIHA.3,4 Hence, DIIHA may result in life-threatening or fatal hemolytic anemia.2,3
Platinum-based chemotherapies result in cytopenias through marrow suppression but may also cause cytopenias through immune mediated mechanisms.5,6 IgE mediated hypersensitivity reactions occur with platinum-based chemotherapies as well, but likely through a separate mechanism from immune-mediated cytopenias.7 There have been several reports of oxaliplatin-induced immune cytopenias in the literature;5,6,8–10 however, only three case reports of carboplatin-induced immune hemolytic anemia exist. Marani et al12 described an 8-year-old boy, treated with a carboplatin-based chemotherapy regimen, who complained of low back pain during his 26th dose of carboplatin with subsequent overt intravascular hemolysis with his 27th dose. His anemia responded to blood transfusion, and the hemolysis ceased without further intervention.11,12 Maloisal et al13 reported a 44-year-old female developing hemolytic anemia following carboplatin administration. Interestingly, her hemolysis did not worsen with additional doses. Dacha et al14 described a 72-year-old female who developed acute onset intravascular hemolysis during infusion of carboplatin and subsequently died of multi-organ failure. In our patient, carboplatin-dependent antibodies were identified. The clinical picture and laboratory evidence support the pathophysiologic mechanism of drug-dependent immune hemolytic anemia resulting in complement fixation and intravascular hemolysis prompting a systemic inflammatory response, resulting in acute multi-organ failure and death.
Conclusion
Although uncommon, DIIHA is often responsive to drug withdrawal and supportive care.3 Select drugs have been implicated in a more serious, often fatal form of DIIHA. Here we report the second case of fatal carboplatin-induced immune hemolytic anemia, the first in a pediatric patient. Despite its rarity, DIIHA must be included in the differential diagnosis of any patient receiving platinum-based chemotherapy that presents with overt hemolysis, sudden changes in serum chemistry values, or unexplained back pain. Along with supportive care, clearing the offending antibodies via plasma exchange may control the underlying cause and prevent the brisk and efficient complement fixation that characterizes this form of severe DIIHA.1 Due to the rapidity of clinical deterioration, plasma exchange was not performed in this case.
Acknowledgment
The authors wish to acknowledge the contributions of our colleague, Dr George Garratty, to the fields of immunohematology, hematology, and transfusion medicine. Dr Garratty sadly passed away during the preparation of this manuscript. Dr Garratty’s work and research propelled the field of immunohematology to new fronts, and his persistent curiosity and pure appreciation for the complex nature of transfusion medicine and immune hemolytic anemia was infectious and inspiring. Always available to clinicians and scientists across the world, Dr Garratty was the consummate teacher –guiding us through the complex and sometimes confusing answers to our clinical problems. Dr Garratty was always just a phone call or email away and always willing to help us explain our particular clinical conundrum while simultaneously shedding light on how we could apply the information to the next scenario. He will surely be missed.
Disclosure
The authors have no conflicts of interest to disclose.
References
Doratota S, Recht M, Garratty G, Krupicka M, Thomas GA, Boshkov L. Successful treatment of life-threatening ceftriaxone-induced hemolysis by plasmapheresis. Transfusion. 2009;49(S):13A abtr. | |
Garratty G, Arndt PA. Review: drug-induced immune hemolytic anemia – the last decade. Immunohematology. 2004;20(3):138–146. | |
Garratty G. Immune hemolytic anemia associated with drug therapy. Blood Rev. 2010;24(4–5):143–150. | |
Pierce A, Nester T. Pathology consultation on drug-induced hemolytic anemia. Am J Pathol. 2011;136(1):7–12. | |
Cobo F, De Celis G, Pereira A, Latorre X, Pujadas J, Albiol S. Oxaliplatin-induced immune hemolytic anemia: a case report and review of the literature. Anticancer Drugs. 2007;18(8):973–976. | |
Arndt PA, Garratty G, Isaak E, Bolger M, Lu Q. Positive direct and indirect anti-globulin tests associated with oxaliplatin can be due to drug antibody and/or drug-induced nonimmunologic protein adsorption. Transfusion. 2009;49(4):711–718. | |
Makrilia N, Syrigou E, Kaklamanos I, Manolopoulos L, Saif MW. Hypersensitivity reactions associated with platinum antineoplastic agents: a systematic review. Met Based Drugs. Epub September 20, 2010. | |
Hofheinz RD, Nguyen XD, Buchheidt D, Kerowgan M, Hehlmann R, Hochhaus A. Two potential mechanisms of oxaliplatin-induced haemolytic anemia in a single patient. Cancer Chemother Pharmacol. 2004;53:276–277. | |
Sorbye H, Bruserud O, Dahl O. Oxaliplatin-induced haematological emergency with an immediate severe thrombocytopenia and haemolysis. Acta Oncol. 2001;40(7):882–883. | |
Teng CJ, Hsieh YY, Chen KW, Chao TC, Tzeng CH, Wang WS. Sudden-onset pancytopenia with intracranial hemorrhage after oxaliplatin treatment: a case report and literature review. Jpn J Clin Oncol. 2011;41(1):125–129. | |
Marani T, Leatherbarrow HB, Armstrong KS, et al. Carboplatin-induced immune hemolytic anemia (CIHA) due to an antibody reaction with features of both the immune complex (IC) and drug-adsorption (DA) mechanisms [abstract]. Transfusion. 1994;34:20S. | |
Marani TM, Trich MB, Armstrong KS, et al. Carboplatin-induced immune hemolytic anemia. Transfusion. 1996;36(11–12):1016–1018. | |
Maloisal F, Kurtz JE, Andres E, Gorodetsky C, Dufour P, Oberling F. Platin salts-induced hemolytic anemia: cisplatin- and the 2nd case of carboplatin-induced hemolysis. Anticancer Drugs. 1995;6(2):324–326. | |
Dacha S, Reddivan AK, Latta S, Devidi M, Iroegbu N. Carboplatin- induced fatal autoimmune hemolytic anemia: first reported case. World J Oncol. 2010;1(4):173–175. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.