Back to Journals » International Medical Case Reports Journal » Volume 18
Fat Liquefaction and Lipo Particles in a CIED Pocket During Generator Change-Not an Infection: A Rare Case Report
Authors Guan A, He T, Huang X, Xia W, Shao Y
Received 10 November 2024
Accepted for publication 7 January 2025
Published 10 January 2025 Volume 2025:18 Pages 53—58
DOI https://doi.org/10.2147/IMCRJ.S505053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Aili Guan,1 Tao He,1 Xingang Huang,2 Wei Xia,1 Yibing Shao1
1Department of Cardiology, Heart Center, Qingdao Municipal Hospital, Qingdao, Shandong, 266071, People’s Republic of China; 2Department of Pathology, Qingdao Municipal Hospital, Qingdao, Shandong, 266071, People’s Republic of China
Correspondence: Yibing Shao, Email [email protected]
Abstract: A case of fat liquefaction and fat particles in the pacemaker pocket observed in a female patient 12 years after implantation. The patient had no symptoms and no signs of infection or other discomfort of the heart and pacemaker pocket. The biochemical analysis showed a slight increase in cardiac troponin T, 0.026 ng/mL (reference range, < 0.016 ng/mL), a high increase in total cholesterol, 8.70 mmol/L (reference range, < 5.18 mmol/L), and low density lipoprotein, 5.38 mmol/L (reference range, < 3.37 mmol/L). Thick yellow liquid was seen to flow out of the pacemaker pocket when the pocket was opened, and many fat particles were found adhering to the wall of the pacemaker pocket during the pacemaker replacement procedure. Fat and fibrillar connective tissue with a few inflammatory cells, local tissue degeneration and necrosis were shown on immunohistochemical staining and no bacterial growth including anaerobic bacteria was observed. The aseptic necrosis of post-implantation complications is helpful for differential diagnosis in CIED complication. Moreover, the identification of fat liquefaction has important clinical significance for patient management and surgical decision-making.
Keywords: fat liquefaction, fat particles, CIED pocket, CIED complications, CIED replacement
Introduction
The number of implanted cardiovascular implantable electronic devices (CIEDs) has increased significantly in the last 30 years, which has led to an upsurge in CIED complications, such as infection and lead malfunction requiring CIED extraction. Nearly one in ten patients experience complications in relation to CIED implantations.1 CIED complications have serious implications for patients and the healthcare system. In light of the rising rates in new implants and consistent rate of complications, primary prevention remains a major concern. In 2013, an analysis of 5918 consecutive cases found that 2.4% of patients required a lead-related re-intervention, 0.9% developed a pneumothorax, 0.8% developed infection, 0.6% developed a cardiac perforation and 0.2% developed a hematoma requiring re-operation.2 In resent review, FOLLOWPACE-trial, involving a broader patient base in varied hospital settings, had a higher acute complication rate of 12.4%, with 4.2% necessitating surgical intervention.3 Risk factors for CIED infection may be divided into patient-related, procedure-related, and device-related factors. The patient-related factors included: end-stage renal disease, renal insufficiency, diabetes mellitus, chronic obstructive pulmonary disease, corticosteroid use, history of previous device infection, malignancy, heart failure, pre-procedural fever, anticoagulant drug use, and skin disorders, but not age or gender.4 The most common bacterial in CIED infection is coagulase-negative staphylococci, S. aureus. Fat liquefaction in the CIED pocket is a minor complication. Aseptic fat liquefaction, as a main cause of prolonged healing of an aseptic post-surgical incision, is the necrosis of adipose tissue without infection and has an incidence of 0.52–1.11% in all postoperative wounds. It’s occasionally happened in older or over-weight patients complicated by diabetes or malnutrition.5 The CIED pocket is a histopathologically dynamic environment, given the coexistence of both a subacute foreign body response and fibrous tissue growth, implying continuous remodeling due to an injury-repair mechanism. Strategies to interact with foreign body response might minimize inflammatory pocket activity, especially device encapsulation by tight fibrous tissue, and possibly complications related to repeated CIED procedures.6 Using a high-frequency electric knife during surgery may also lead to adipose cells burst, lead to fat liquefaction.7 Although, a total of 100mL of serosanguinous fluid is drained from the pacemaker pocket with no abnormal cells, and a painless fluid accumulation in the implantable cardiac defibrillator (ICD) pocket site is reported caused by an allergic reaction.8,9 Few cases of fat liquefaction and fat particles in the CIED pocket have been reported. Here, we report a case of fat liquefaction and fat particles in the pacemaker pocket approximately 12 years after implantation. Meanwhile, the identification of fat liquefaction has important clinical significance for patient management and surgical decision-making.
Case Presentation
A case of fat liquefaction and fat particles in the pacemaker pocket observed in a female patient 12 years after implantation. Antibiotic prophylaxis was administered before the procedure (cefazolin 1 g). The standard procedure for device replacement in our center includes lead debridement and pocket enlargement to fit the new device comfortably, according to the EHRA recommendations.10 Regarding to radiological and imaging examination. An electrocardiogram on admission showed an atrial pacing rate with narrow QRS, low T-wave amplitude in lead V3-V6, lead II, lead III, and lead avF (Figure 1). Chest CT scan showed bronchiectasis and no cardiomegaly. Echocardiography showed left atrial enlargement (the anteroposterior diameter of the left atrium was 39 mm), and left ventricular ejection fraction was 60%. The location of the pacemaker was identified by X-ray when the patient lay on the bed in the heart catheter room (Figure 2). Thick yellow liquid was seen to flow out of the pacemaker pocket when opened during the pacemaker replacement procedure (Figure 3A). Many fat particles were observed adhered to the wall of the pacemaker pocket (Figure 3B).
 |
Figure 1 Electrocardiogram (ECG) on admission. |
 |
Figure 2 Location of the pacemaker shown by X-ray. |
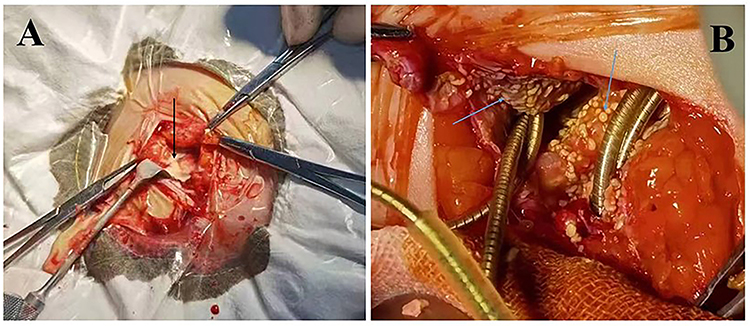 |
Figure 3 Fat liquefaction and fat particles in pacemaker pocket. (A) Fat liquefaction in the pacemaker pocket shown by the black arrow; (B) Fat particles adhered to the wall of the pacemaker pocket shown by the other blue arrows. |
We also performed a tissue biopsy from the wall of the pacemaker pocket for early diagnosis, and the samples were analyzed by the Pathology Department, blinded to the clinical data. Two tissue samples 5 mm in size were obtained from different areas of the pacemaker pocket incision. Fat and fibrillar connective tissue with a few inflammatory cells, local tissue degeneration and necrosis were shown on immunohistochemical staining (Figure 4A and B). Location of the pacemaker was also identified by X-ray after the procedure (Figure 5).
 |
Figure 4 Pathology of the pacemaker pocket wall. Two tissue samples 5 mm in size were obtained from different areas of the pacemaker pocket incision. Both samples showed fat and fibrillar connective tissue with a few inflammatory cells, local tissue degeneration and necrosis on immunohistochemical staining (A and B). |
 |
Figure 5 New X-ray image after replacement procedure. |
Laboratory testing showed elevated cardiac troponin T at 0.026 ng/mL (reference range, <0.016 ng/mL), total cholesterol at 8.70 mmol/L (reference range, <5.18 mmol/L) and low density lipoprotein at 5.38 mmol/L (reference range, <3.37 mmol/L). The level of B-type natriuretic peptide was within the normal range at 89.3 pg/mL (reference range, <100 pg/mL), hemoglobin was 133 g/L (reference range, 115~150 g/L), albumin was 42.44 g/L (reference range, 40~55 g/L), and fasting blood glucose was 4.3 mmol/L (reference range, 3.9~6.1 mmol/L). Inflammatory parameters showed that white blood cell was within normal range at 5.9*109/L (reference range, 3.5~9.5*109/L), and C-reactive protein was 4.21 mg/L (reference range, 0~6 mg/L) after the procedure (Table 1). We also cultured the yellow liquid, and no bacterial growth including anaerobic bacteria was reported.
 |
Table 1 The Results of Biochemical and Hematology Parameters |
Discussion
Cardiovascular implantable electronic devices (CIEDs) have helped with advanced technological improvements in the cardiac field and are a long-term alternative to medical management. There are different forms of CIEDs such as pacemakers, implantable cardioverter-defibrillators, and cardiac resynchronization therapy. These devices are efficient in establishing near-normal hemodynamics and circulation that ultimately aid physicians to improve patient quality of life. However, there are risk factors that can result in postoperative complications, including infection, lead and pulse generator complications, heart complications, medication-related complications, and psychosocial complications.11 CIED infection is one of the most important device-related complications and has a major impact on mortality, quality of life, healthcare utilization, and cost.12 Culture of the yellow liquid from the wound revealed no bacterial growth including anaerobic bacteria, and the patient had no signs of infection. No clinical characteristics of infection were found, although the thick yellow liquid was seen in the pacemaker pocket.
Research has shown that factors contributing to fat liquefaction in postoperative wounds include obesity, unnecessary and overuse of an electrotome during surgery, prolonged exposure of the incision, old age and chronic diseases.5 These chronic diseases include anemia, hypoproteinemia and diabetes. An electrotome was not used during primary implantation, and exposure of the incision was not prolonged in our patient. The surgery time was approximately 1 h. In addition, the patient did not have anemia, hypoproteinemia or diabetes. The fat liquefaction which formed in the CIED pocket might have been related to obesity, or the location of the pacemaker adjacent to breast tissue. Necrotic adipocytes may release compounds inducing inflammation and even multiple complications, such as oil cysts, hematoma, calcifications, or tissue depressions.13 In a study on the morpho-histologic characteristics of CIED pockets in non-infected cases, most device capsules were characterized by the formation of a thin scar tissue layer on the anterior and posterior walls, sometimes a slightly thicker posterior wall, while a small percentage showed a hard, calcified structure.14 Pocket creation at implant is associated with tissue trauma and cell damage, including the extracellular matrix, nerve fibers, and blood vessels, followed by gradual tissue remodeling into a fibrotic capsule.14–16 One recent study showed that the CIED pocket is a histopathological dynamic environment, given the co-existence of both a subacute foreign body response and fibrous tissue growth implying continuous remodeling due to an injury-repair mechanism. Strategies to interact with the foreign body response might minimize inflammatory pocket activity, especially device encapsulation by tight fibrous tissue, and possibly complications related to repeated CIED procedures.6 We have no experience of fat liquefaction and fat particle complications in the CIED pocket during re-implantation in our center. A tissue biopsy from the pacemaker pocket incision was performed. The infiltration of a few inflammatory cells, degeneration and necrosis of local cells were found in the fat and fibrillar connective tissues. This phenomenon might be related to fat necrosis, perhaps also related to the patient-specific health conditions, is only focused on the single-patient, lack of longitudinal data to assess long-term outcomes, and has inability to generalize findings to larger populations. We have no idea about whether the patient has any undiagnosed diseases, such as transthyretin cardiac amyloidosis (TTR-CA) reported recently,17 other tests may be needed in future.
Conclusion
Fat liquefaction and fat particle complications in the CIED pocket could be an aseptic reaction of the organization, which related to fat necrosis. In spite of complications related with the implantation of CIED, CIEDs are very important in the cardiovascular field. The management of CIED implantation should be improved in order to reduce the occurrence of complications.
Ethical Approval
The patient gave written informed consent for this case report and any related images to be published. Approval by the Medical Ethics Committee of Qingdao Municipal Hospital was received for publication of this case report.
Acknowledgments
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-3786059/v1.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Frausing MHJP, Mads BK, Jens BJ, et al. Avoiding implant complications in cardiac implantable electronic devices: what works? Europace. 2021;23(2):163–173. doi:10.1093/europace/euaa221
2. Kirkfeldt RE, Johansen JB, Nohr EA, et al. Complications after cardiac implantable electronic device implantations: an analysis of a complete, nationwide cohort in Denmark. Eur Heart J. 2014;35:1186–1194. doi:10.1093/eurheartj/eht511
3. Anil S, Shruti KI, Komandoor S. Navigating complications in cardiac pacemakers: a comprehensive review and management strategies. Rev Cardiovasc Med. 2024;25(8):299. doi:10.31083/j.rcm2508299
4. Carina BL, Vassil T, Paola AE, et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society(APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Europace. 2020;22:515–516. doi:10.1093/europace/euz246
5. Shi ZJ, Lin ML, Wang H, et al. Insulin and hypertonic glucose in the management of aseptic fat liquefaction of post-surgical incision: a meta-analysis and systematic review. Int Wound J. 2013;10(1):91–97. doi:10.1111/j.1742-481X.2012.00949.x
6. Massaro G, Leone O, Valzania C, et al. Pocket histology at cardiac implantable electronic devices replacement: what’s new? Heart Rhythm. 2023;20(2):198–206. doi:10.1016/j.hrthm.2022.10.017
7. Zhang MS, Sun PY, Liu MZ, et al. A case report of a woman after childbirth with a dehisced abdominal wound as well as fat liquefaction and large skin necrosis. Ann Palliat Med. 2020;9(2):493–496. doi:10.21037/apm.2020.03.15
8. Praveen GP, Kirun G, Nischal NH. A case of delayed non-infective cystic swelling at the pacemaker pocket site. Cureus. 2022;14(2):e22299. doi:10.7759/cureus.22299
9. Rana AZ, Safa A, Ryan I, et al. A new solution to a rare problem of implantable cardiac device hypersensitivity. Cureus. 2021;13(9):e17882. doi:10.7759/cureus.17882
10. Sticherling C, Marin F, Birnie D, et al. Antithrombotic management in patients undergoing electrophysiological procedures: a European Heart Rhythm Association (EHRA) position document endorsed by the ESC Working Group Thrombosis, Heart Rhythm Society (HRS), and Asia Pacific Heart Rhythm Society (APHRS). Europace. 2015;17:1197–1214. doi:10.1093/europace/euv190
11. Crystal JR, John P, Kyle SG, et al. Surgical techniques, complications, and long-term health effects of cardiac implantable electronic devices. Cureus. 2021;13(1):e13001. doi:10.7759/cureus.13001
12. Phillips P, Krahn AD, Andrade JG, et al. Treatment and prevention of Cardiovascular Implantable Electronic Device (CIED) infections. CJC Open. 2022;4(11):946–958. doi:10.1016/j.cjco.2022.07.010
13. Zhu MS, Zhu MH, Wu XL, et al. Porcine acellular dermal matrix increases fat survival rate after fat grafting in nude mice. Aesthet Plast Surg. 2021;45(5):2426–2436. doi:10.1007/s00266-021-02299-z
14. Steckiewicz R, Świętoń EB, Kołodzińska A, et al. Morphometric parameters of cardiac implantable electronic device (CIED) pocket walls observed on device replacement. Folia Morphol. 2017;76(4):675–681. doi:10.5603/FM.a2017.0048
15. Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials. Semin Immunopathol. 2008;20(2):86–100. doi:10.1016/j.smim.2007.11.004
16. Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol. 2008;214(2):199–210. doi:10.1002/path.2277
17. Takano R, Ueda N, Okada A, et al. Fat biopsy from a pocket of cardiac implantable electronic device: an alternative diagnostic option for cardiac amyloidosis. HeartRhythm Case Rep. 2022;8(8):554–557. doi:10.1016/j.hrcr.2022.05.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.