Back to Journals » Risk Management and Healthcare Policy » Volume 18
Family Physicians as Street-Level Bureaucrats: An Interview-Based Study of Service Supply Challenges in Shanghai, China During Public Health Emergencies
Authors Wang G ![]() , Tang M, Zhang T, Luo L
, Tang M, Zhang T, Luo L
Received 21 July 2025
Accepted for publication 7 October 2025
Published 15 October 2025 Volume 2025:18 Pages 3343—3357
DOI https://doi.org/10.2147/RMHP.S555229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Gan Wang,1,2 Man Tang,3 Tiantian Zhang,1,2 Li Luo1,2
1Shanghai Institute of Infectious Disease and Biosecurity, Fudan University, Shanghai, 200032, People’s Republic of China; 2School of Public Health, Fudan University, Shanghai, 200032, People’s Republic of China; 3School of Government, Peking University, Beijing, 100871, People’s Republic of China
Correspondence: Li Luo, Email [email protected]
Objective: This study aims to analyze the service supply challenges for Family Physicians during public health emergencies through the lens of street-level bureaucracy.
Methods: Guided by street-level bureaucracy theory within a three-tier analytical framework (micro-, meso-, and macro-levels), this qualitative study employed semi-structured interviews with 36 Family Physicians in Shanghai regarding their responses to a public health emergency. Interviews were recorded, transcribed verbatim using “iFlytek Hearing” software, manually reviewed, and analyzed thematically using NVivo 10.
Results: The analysis revealed multi-level challenges. At the micro-level, Family Physicians faced dual role pressures as “state agents” and “public agents”, leading to reduced discretionary power and a tendency for prosocial deviant behavior; their understanding of policies and effectiveness of communication with the public directly impacted policy implementation outcomes. At the meso-level, resource scarcity created supply-demand contradictions, triggering adaptive policy implementation, where Family Physicians innovatively met service needs under constraints and participated in community collaborative governance. At the macro-level, policy ambiguity was prominent, essential medicine supply chains faced difficulties, and training and career development pathways in general practice remained underdeveloped.
Conclusion: This study provides a deep understanding of the service supply challenges faced by Family Physicians during public health emergencies, offering a scientific basis for optimizing service supply strategies, and this theoretical framework can be extended to the analysis of other street-level bureaucrats.
Keywords: street-level bureaucracy, family physician, public health emergencies, primary health care, health policy
Introduction
During the ongoing pandemic, family physicians have served as pivotal primary healthcare providers, playing a multidimensional role in optimizing medical resource allocation and enhancing public health response.1 Drawing on experiences from the COVID-19 pandemic and previous outbreaks, their core functions have primarily encompassed six key aspects: (1) triage and clinical management of suspected/confirmed cases, (2) rational allocation of medical resources, (3) community-based disease surveillance and epidemiological monitoring, (4) implementation of preventive health interventions, (5) provision of accessible healthcare services, and (6) maintenance of continuous care for non-COVID patients (including acute and chronic conditions).2 Through their continuous, accessible, and family-centered care model, family physicians significantly improved health screening coverage while effectively alleviating the burden on secondary and tertiary healthcare facilities via home visits, teleconsultations, and tiered diagnosis-treatment systems, thereby reducing overall healthcare costs.3 The COVID-19 pandemic placed immense professional and psychological strain on family physicians. Critical shortages of personal protective equipment (PPE) often forced them to ration and reuse supplies—practices that generated significant anxiety and personal safety concerns.4 For example, this high-risk environment increased the profession’s susceptibility to mental health disorders (MHDs). To cope with these challenges, the most frequently adopted adaptive strategies included spending time with family and engaging in physical exercise.5
Family Physicians belong to the category of “people who interact directly with citizens, face the people, and represent the government”, referred to by the renowned American political scientist Michael Lipsky as street bureaucrats (Street-level Bureaucracy, SLB). Throughout the pandemic control process, although working in various medical institutions, Family Physicians still possessed considerable independence, including but not limited to discretionary power, which had a broad potential impact on citizens when providing medical services.6 In the pyramid structure of the entire medical service system, Family Physicians are at the bottom with little power and relatively low status, and their salary is not as high as that of secondary and tertiary public hospitals, with relatively narrow career advancement channels. At the same time, Family Physicians are at the end of policy implementation, and each medical service they provide directly constitutes the output of government agencies, influencing the governments image, administrative capabilities, and the relationship between officials and the public (including doctor-patient relationships).
One of the key factors contributing to Chinas success in controlling the epidemic was the governments swift response. For example, 14,000 health monitoring sites were established in the public transportation system, and Wuhan completed 9 million tests in just a few weeks. It is estimated that the public health measures implemented between January 29 and February 29,2020, effectively prevented approximately 1.4 million new cases and 56,000 deaths nationwide.7 The impact of the COVID-19 pandemic exposed and exacerbated inherent weaknesses in the primary healthcare system. These primarily included: insufficient training and educational opportunities for practitioners; a fee-for-service model that incentivized unnecessary diagnostic and treatment procedures; poor coordination and integration between clinical care and public health services, as well as among healthcare institutions at different levels; and a systemic lack of care continuity throughout the healthcare delivery process.8 While some studies have explored China’s primary healthcare response to public health crises, there remains a paucity of micro-qualitative research focusing on the on-the-ground operational challenges faced by Family Physician teams within the Chinese context.
Against this backdrop, this study aims to analyze the service supply challenges for Family Physicians during public health emergencies through the lens of SLB, based on data from semi-structured interviews collected in Shanghai during the COVID-19 pandemic. Chinese family physicians serve as a critical interface between national public health policies and individual citizens. During public health emergencies, they must exercise discretion in applying standardized guidelines to complex realities, a core principle of street-level bureaucracy theory. The theory’s micro-, meso-, and macro-level analytical framework systematically reveals the multi-tiered influences shaping their actions, thereby providing a profound understanding of the challenges they face.
The research question is: How did the inherent dynamics of street-level bureaucracy—such as discretion, coping mechanisms, resource management, and policy interpretation—manifest among Family Physicians in Shanghai during the COVID-19 pandemic, and what specific service supply challenges emerged from these dynamics? Employing an SLB lens to analyze these specific operational and experiential aspects, this research aims to foster a nuanced understanding of the challenges confronting the primary care frontline. Ultimately, this theoretically grounded examination of service supply issues among Shanghai’s Family Physicians seeks to generate actionable insights for enhancing the effectiveness of these street-level bureaucrats and strengthening overall public health crisis response capacity.
Methods
Qualitative Approach and Research Paradigm
This study adopted a constructivist/interpretivist paradigm, utilizing semi-structured interviews guided by Lipsky’s (1980) street-level bureaucracy theory. The research focused on examining how family physicians interpreted and implemented policies during public health emergencies, with particular emphasis on the challenges they encountered in service delivery throughout the COVID-19 pandemic. The SLB theory informed the development of the interview guide, but not the design of the coding structure.
This study reveals the challenges faced by the “implementation process” of family physician services under the dual pressures of rules and resources. Institutional logics theory is more suitable for macro-level analysis, whereas SLB theory precisely bridges macro-level policies with micro-level practices, focusing on key mechanisms such as discretion. Compared to resilience frameworks’ emphasis on “outcomes”, SLB better explains the “process”; and relative to role theory’s focus on “cognition”, SLB places greater emphasis on how “cognition” translates into “action” during interactions with patients.9–11 Therefore, SLB theory provides the most direct and powerful analytical framework for examining the unique dilemmas faced by family physicians on the crisis frontlines and their coping strategies.
Sampling Strategy
We employed purposive sampling to recruit 36 family physicians from two community health centers in Shanghai. The selection criteria included: (1) substantial involvement in pandemic response efforts; (2) service to diverse patient populations, with each center covering approximately 100,000 residents; and (3) well-established family physician systems, achieving 90% contract coverage rates among key populations. Theoretical saturation was reached after 30 interviews, and an additional six interviews were conducted to ensure comprehensive data collection without emerging new themes.
Ethical Considerations
The study protocol received ethical approval from the Institutional Review Board of Fudan University (IRB#2025-01-1199). All participants provided written informed consent and received compensation of 200 RMB for their time. To ensure confidentiality, all data were anonymized, and audio recordings were used exclusively for research purposes.
Data Collection
Between November and December 2024, face-to-face interviews were conducted by trained doctoral researchers using a pilot-tested interview guide (see Appendix 1). To ensure neutrality, the semi-structured interview guide was piloted and refined prior to the formal interviews. During the interviews, the technique of bracketing was employed to set aside the researchers’ preconceptions. Each interview lasted 35–45 minutes and explored key dimensions, including professional discretion, resource constraints, and policy implementation tensions. For example, participants were asked to describe how they prioritized patient care when clinical guidelines conflicted with individual needs.
Data Analysis
We conducted a theory-guided thematic analysis using NVivo 10 software, applying Lipsky’s framework across three analytical levels: micro (individual decision-making), meso (organizational processes), and macro (policy environment). Three researchers independently coded the transcripts, and inter-coder reliability was assessed to ensure consistency. Illustrative quotations were systematically selected as the most representative examples of the key themes that emerged from the analysis across the micro, meso, and macro levels. All quotations were translated from Chinese (Shanghainese/Mandarin) to English by a bilingual researcher, and the translations were then cross-checked by a second independent translator to ensure conceptual accuracy and contextual meaning were preserved. To guarantee anonymity, all participants were assigned unique alphanumeric codes (eg, N1, N2) in place of any identifiable information Key findings were supported by representative quotations; for instance, 28 out of 36 physicians reported experiencing limitations in their discretionary authority.
This study strictly adhered to qualitative research standards (see Appendix 2), employing theoretically guided sampling, expert-validated interview instrument development, a three-level coding framework, and member checking to systematically examine family physicians’ policy implementation challenges during COVID-19 containment (see Appendix 3).
Results
This section begins with an analysis of the characteristics of the research subjects (Table 1). Subsequently, a detailed examination of the challenges in Family Physician service delivery during public health emergencies is conducted, structured across micro-, meso-, and macro-level perspectives (Table 2).
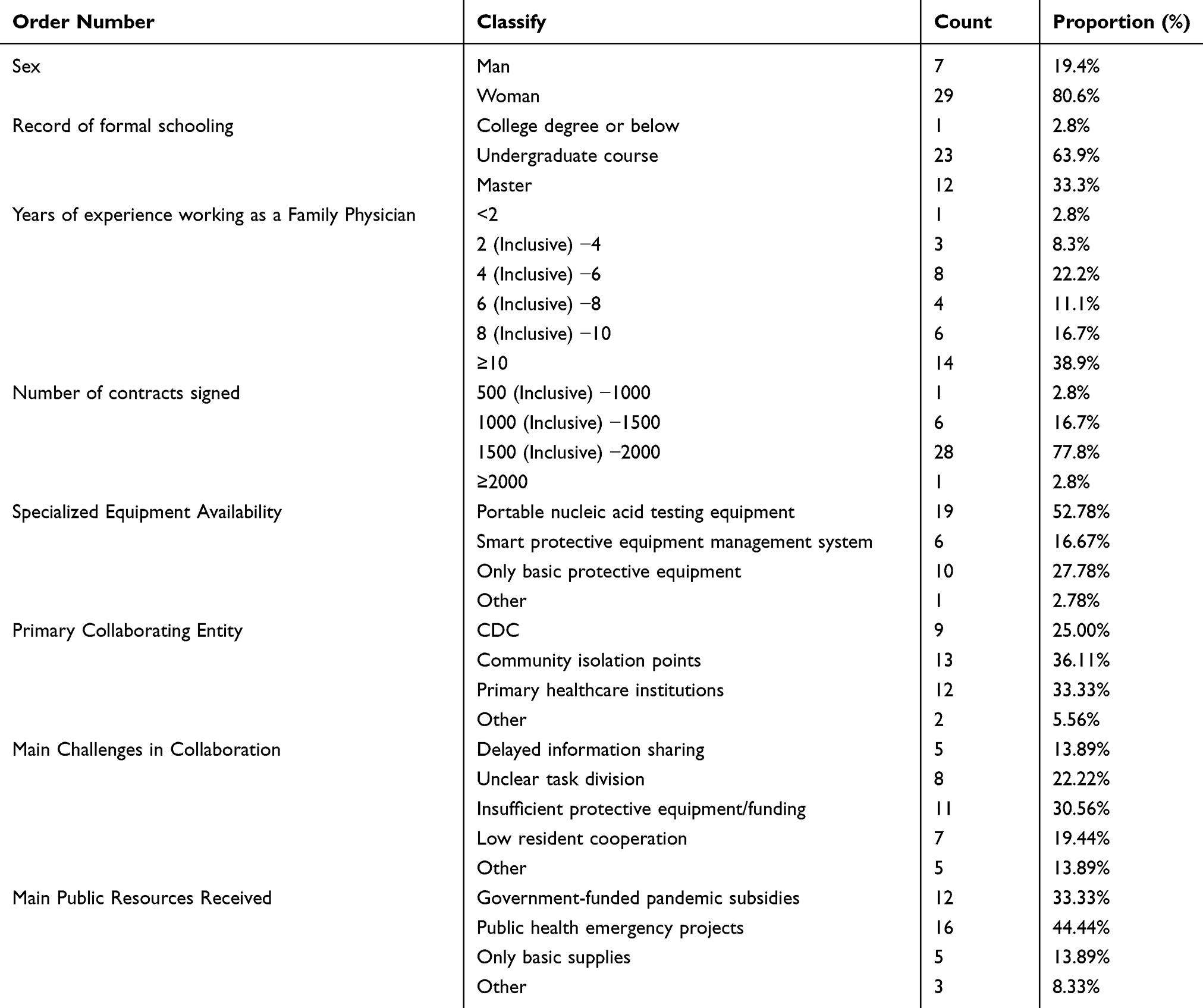 |
Table 1 Demographic Characteristics of the Respondents |
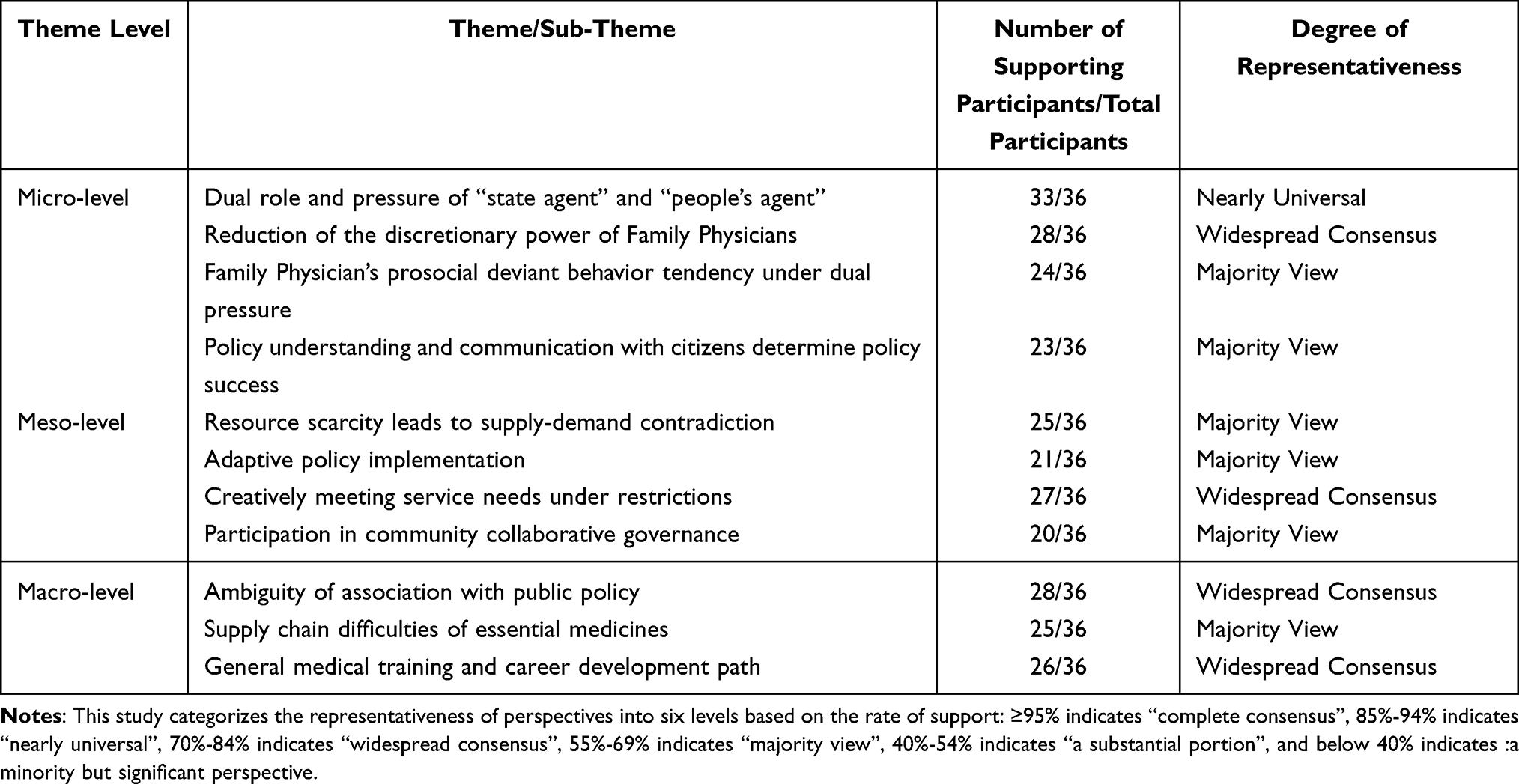 |
Table 2 Analysis of Core Themes and Their Representativeness: The Dilemmas of Family Physicians in COVID-19 Prevention and Control |
Characteristics of the Research Subjects
The study included 36 Family Physicians, with a majority being women (80.6%) and a smaller proportion of men (19.4%). Most participants held an undergraduate degree (63.9%), while 33.3% had a master’s degree, and only 2.8% reported a college degree or below. Regarding work experience, 38.9% had ≥10 years of experience, followed by 22.2% with 4–6 years and 16.7% with 8–10 years. The majority (77.8%) had signed 1,500–2,000 service contracts, with very few (2.8%) exceeding 2,000 contracts. Over half (52.78%) had access to portable nucleic acid testing equipment, while 27.78% relied only on basic protective equipment. Primary collaboration partners included community isolation points (36.11%) and primary healthcare institutions (33.33%). Key challenges in collaboration were insufficient protective equipment/funding (30.56%) and unclear task division (22.22%). Public resources primarily came from public health emergency projects (44.44%) and government-funded pandemic subsidies (33.33%).
Micro-Level Influences
Dual Role and Pressure of “State Agent” and “People’s Agent”
Family Physicians, who played the role of “national agents” in enforcing policy regulations, also fulfilled the role of “public agents” by addressing patient needs. They sought to strike a balance between conforming to policy regulations, as national agents, and satisfying patients’ actual needs, as public agents. This delicate balancing act required them to manage the tension between the pressure to execute policies and the pressure to be responsive to patient demands.
The CDC has special follow-up measures for patients who have been discharged from makeshift hospitals, and once they return home, we need to follow up with them regularly. (N 16)
The emergency support was utilized for weekend community nucleic acid screening and routine nucleic acid sampling. It was uniformly allocated by the district nucleic acid screening task force under a flat management system. The district-level emergency sampling teams were required to deploy within 30 minutes, while township-level emergency sampling teams had to deploy within 15 minutes. Each community health center’s sampling team consisted of approximately 10 personnel, including family physicians. (N 7)
Family Physicians encountered significant psychological stress during the pandemic. They had to address the anxiety and panic of patients and their families while also grappling with their own fears about infection risks. Some residents were uncooperative with the pandemic control measures implemented by Family Physicians, creating personal challenges for them. This ongoing psychological strain could lead to burnout, anxiety, and depression, potentially impacting their career progression.
Given our circumstances, we did not return home to live but chose to stay in a hotel. Since our unit provided the hotel accommodation, we settled there. Then, when the hotel accommodation ended, we moved to the hospital. (N 8)
When we received the request from the higher authorities to collect nucleic acid samples or visit residents at home, some residents were worried about the increased risk of infection and were unwilling to open their doors to cooperate with our work. (N 28)
Reduction of the Discretionary Power of Family Physicians
Epidemic prevention and control has an emergency and special nature, in order to protect citizens right to life and health, it is necessary to take public measures to restrict freedom, including quarantine measures for patients or suspected individuals and codes of conduct for medical workers. These measures constrained the discretionary power of Family Physicians in delivering services to ensure effective epidemic control. Many Family Physicians frequently sought a balance between flexibility and the stringent implementation of public health policies while rendering medical care.
During the lockdown period, some residents required cross-district chemotherapy treatment, which contradicted the containment measures stipulating that chemotherapy must be administered within their residential district. In such cases, we had to obtain their understanding through communication. (C 8)
In clinical practice, apart from their routine duties, healthcare workers also had to manage issues stemming from the temporary lockdown of neighborhoods due to the pandemic. For instance, patients were unable to freely select healthcare facilities when seeking medical services because of stringent pandemic control measures. In these circumstances, Family Physicians often had to carry out necessary verification tasks. (N 25)
During the nucleic acid screening process, should an abnormal result emerge, our on-duty Family Physicians, day or night, would swiftly reach the patient’s location to perform a follow-up nucleic acid test. (N 19)
Family Physician’s Prosocial Deviant Behavior Tendency Under Dual Pressure
Family Physicians demonstrated “prosocial misconduct”, a behavior characterized by the intentional breach of formal organizational policies and regulations driven by altruistic motives. At times, they prioritized the continuity of medical services, even if this involved contravening established guidelines or protocols. This behavior reflects the ethical and operational challenges that street bureaucrats may face in their practical work.
During nucleic acid testing, the guidelines required changing gloves after each individual’s sampling, but this proved impractical in reality. Therefore, we typically disinfected the gloves with alcohol spray between each test before calling the next person for sampling. This approach maintained basic safety standards while improving efficiency – otherwise, it would have been impossible to complete the massive multi-round screening targets. (C 12)
The state mandated that medical personnel wear N95 masks to prevent infection, yet during periods when protective supplies were most scarce, individuals often donned only regular medical surgical masks for nucleic acid testing or home visits. In an effort to better understand patients’ health conditions, we occasionally disregarded pertinent hygiene and safety regulations to conduct home visits, which could have heightened the risk of cross-infection. (N 13)
At the beginning of the full resumption of the pandemic, our hospital had many medical staff infected, yet we still had to treat a large number of patients. Many doctors worked while sick, and some doctors who were infected only took one day off and immediately returned to work, hoping to treat more infected patients and prescribe medication, putting their own safety aside. (N 28)
The Understanding of Policies by Family Physicians and the Communication with Citizens Determine the Success of Policies
If medical staff had a deep understanding of the policy, they could more accurately translate the policy’s intentions into specific service actions, adjusting their services to meet the needs and actual situations of patients. With residents fully understanding and cooperating, the implementation effect of the policy could be effectively enhanced.
During the outbreak, my phone was frequently dialed to saturation, and each call lasted a long time, which made it difficult to get through some calls. Therefore, how to enable residents to quickly find doctors is indeed a question we need to think about. (N 36)
If doctors had gained insight into the diverse needs of patients and the medications they required, and if patients could clearly identify which doctors to consult, then communication, though not as frequent as emergency calls, would have been more efficient and smoother in other respects. However, due to the occurrence of emergencies, there was often a lack of an effective communication mechanism, leading to numerous barriers in communication. (N 30)
Regarding nucleic acid testing, we were required to adhere to the regulations and ensure that everyone was sampled. He emphasized the importance of cooperation. Initially, I was puzzled by the existence of such a requirement. Despite having worked tirelessly, going door-to-door and even climbing high-rise buildings, some individuals refused to be sampled without offering any reason for their refusal. (N 23)
Meso-Level Influences
Resource Scarcity Leads to Supply and Demand Contradiction
During a mass nucleic acid test, it was not always possible to manage all tasks simultaneously, highlighting the resource shortages that street-level bureaucracies often encountered, and the conflict between supply and demand.
At that time, the supply of rabies vaccine could not be guaranteed, because it was initially supplied by a nearby secondary hospital, but later the hospital was temporarily closed for disinfection due to a confirmed patient, resulting in the interruption of vaccine supply, and there was no other place to obtain it. (N 12)
At that time, an elderly woman had a fever of 39.5 degrees, despite taking the medication as directed, her temperature could not come down. We immediately called 120 for help, but the ambulance took a long time to arrive, and we had to wait for several hours. Due to the shortage of ambulance resources, everyone was very anxious. (N 1)
Family Physicians sustained direct engagement with patients via online health consultation services. However, due to quarantine control measures, there was a significant surge in the number of online consultations, which even encroached upon the leisure time of Family Physicians.
During the lockdown period caused by the epidemic, we provided a large number of online health consultation services, including telephone consultations. In fact, our working hours extended to cover the entire day, being on standby 24 hours a day, ready to answer calls at any time. (N 33)
Adaptive Policy Implementation
During the pandemic lockdown, Family Physicians demonstrated adaptive capacities in policy implementation by coordinating with medical department colleagues to modify service delivery processes according to evolving circumstances and public health needs. This operational flexibility aimed to maintain patient care continuity amidst pandemic challenges. Empirical observations revealed several implementation adaptations: when tiered diagnosis and treatment pathways were disrupted, when designation of COVID-19 hospitals was unclear, or when temporary hospital closures occurred for disinfection after positive cases. Additional adjustments were made when the 120 emergency system became overloaded, all of which threatened uninterrupted medical service provision. These modifications represented context-specific operational responses rather than fundamental policy changes, with implementation decisions remaining constrained by existing policy frameworks and resource limitations.
At the beginning of the outbreak, the designation of designated hospitals was unclear. Our Family Physician could only connect with nearby hospitals to determine if there were available beds for referral; during the lockdown management period, nearby secondary hospitals were gradually designated as designated hospitals for pediatric, hemodialysis patients, and peritoneal dialysis patients. (N 27)
Although our hospital had previously developed contingency measures—such as protocols for handling positive cases, with tertiary hospitals also formulating response plans based on past experience, including nosocomial infection control procedures—the actual implementation during real-world scenarios significantly diverged from these prepared plans. (C 1)
Family physicians played an instrumental role in developing a comprehensive suite of institutional protocols for community health centers to support vaccination efforts, including the Personnel Responsibilities at Temporary Vaccination Sites that outlined staff roles and duties, Adverse Event Management Protocols to address potential complications, Post-Vaccination Observation Procedures for patient monitoring, Clinical Pathways for Mild Vaccine Reactions and Treatment Protocols for Severe Vaccine Reactions to guide clinical responses, as well as Anaphylactic Shock Resuscitation Flowcharts for emergency situations - collectively establishing a robust operational framework for safe and effective community-based vaccination implementation. (C 4)
Creatively Meet the Needs of Service Objects Under Restrictions
The main issues were reflected in the constraints on the essential medicines list and examination equipment. Community health service centers were limited by the drug reserves within the essential medicines list, offering a limited variety of drugs that could not meet all demands, especially during the pandemic and lockdown management phases, where drug shortages were particularly pronounced. Community health service centers were unable to provide high-demand drugs such as warfarin and had restrictions on examination items like coagulation tests and echocardiograms, which led residents to frequently visit secondary and tertiary hospitals.
Restricted by the essential medicines list, the variety of drugs available at community health service centers was limited, such as warfarin. As the demand for medication increased, even common drugs became scarce, and volunteers had to go to secondary or tertiary hospitals to obtain them. These hospitals planned to set up convenient clinics later to specifically address the medication needs collected and organized by residents’ committees. There were also limitations in providing services like coagulation tests or echocardiograms at community health service centers. (N 36)
The long prescription policy primarily focused on managing the long-term medication needs of patients with hypertension and diabetes, and was limited to therapeutic drugs. The implementation of long prescriptions aimed to facilitate patients, reducing their need to frequently visit doctors for medication, but also required ensuring medication safety to prevent misuse and abuse. (N 19)
Regarding the issue of long-term and extended prescriptions, most long-term prescriptions were currently focused on two diseases: hypertension and diabetes. For these conditions, the prescriptions were typically limited to therapeutic medications and did not encompass auxiliary drugs or traditional Chinese medicine. (N 10)
Family Physicians Participate in Community Collaborative Governance
The delivery of Family Physician services was intertwined with community governance issues, particularly concerning the role of residents’ committees as both administrative and self-governance entities. Interviews highlighted the activities of residents’ committees in community governance and their efforts to connect with and serve neighborhood residents. However, during the process of community collaborative governance, the coordination of prevention and control efforts was not always smooth, as evidenced by information discrepancies between Family Physicians and residents’ committees regarding nucleic acid testing information.
The first pertained to information communication; for instance, there was often a discrepancy in the timing when the community committee and our center received abnormal nucleic acid test results. This inconsistency frequently led to patients receiving notifications from one entity and then seeking to verify the information with the other. Over a brief period, this could cause patients who tested positive to lose trust in the information, resulting in them remaining outside for an extended time. (N 29)
The neighborhood committee, functioning as a grassroots governance unit, directly influences the efficiency and quality of service in governance. The responsibilities and workload of Family Physicians, who collaborate with neighborhood committees to fulfill residents’ daily needs, are substantial. This indirectly mirrors the high level of dependence residents have on the services provided by the neighborhood committees. (N 32)
The community committee managed a large population, often exceeding 3,000 residents. Typically, we processed 40 to 50 medication requests from auxiliary Family Physicians every two or three days, which meant that, on average, over 20 individuals required medication daily. (N 36)
When managing the treatment of common chronic diseases in the community, we initially tasked volunteers with collecting the patients’ health insurance cards. Once the collection was completed, the volunteers would inquire about the types of medications the patients typically used. Following this, the patients’ information and medication requirements were compiled and presented to me. In my spare time, I would then match their medications to their needs. (N 19)
Macro-Level Influences
Ambiguity of Family Physicians Association with Public Policy
Policy updates were frequent, with COVID-19 prevention and control policies often revised at different times and in different regions, posing challenges for Family Physicians to swiftly adapt to new requirements in practice. The frequent changes in policies could lead to confusion and inconsistency among frontline Family Physicians during implementation, impacting the efficiency and accuracy of epidemic control. Standards were not uniform, with policy standards varying across different regions and levels. This made it difficult for Family Physicians to maintain consistent implementation criteria in practice, increasing the difficulty and risk of execution.
COVID-19 prevention and control documents were frequently updated, requiring us to swiftly determine which measures to tighten and which to relax. For instance, concerning the scientific and precise prevention and control, as well as the 20 measures document, the isolation for close contacts was altered from 7 days of centralized quarantine followed by 3 days of home monitoring to 5 days of centralized quarantine and 3 days of home quarantine. The isolation for secondary contacts was changed from 7 days of home quarantine without further tracing back to their close contacts. Regarding risk areas, the classification was adjusted from high, medium, and low to just high and low. There were numerous such policy updates and adjustments, and often we had not fully grasped them yet, necessitating us to repeatedly explain them to residents. (N 10)
The frequency of disinfection for hospital infections also faced the challenge of frequent updates. High-frequency contact areas, such as touch screens, door curtains, doorknobs, escalators, and elevator buttons, as well as spaces like elevators, were required to be disinfected at least once every two hours. However, the frequency would sometimes extend to four hours, and at other times, it would be changed to three times a day. (N 29)
The specific prevention and control policies pertaining to Family Physicians had transitioned from political to administrative implementation. For instance, community health service centers had developed specific operational pathways in line with the overarching policy program requirements.
For each version of the Novel Coronavirus infection control plan, our center has formulated a series of work tips documents for these key groups, turning specific policies into clear papers in the health field. (N 32)
Supply Chain Difficulties of Essential Medicines
Family Physicians primarily encountered issues such as drug shortages, supply chain disruptions, cross-regional delivery challenges, and limitations in service capacity during public health emergencies, which impacted the continuity and effectiveness of medical services. To enhance the emergency response and service quality of Family Physicians, the management of essential medicines, supply service capacity, cross-regional delivery, and information system integration capabilities needed to be strengthened.
As for the extension of prescriptions, we did not issue them during the risk control period because we lacked the support of pharmaceutical companies. Our prescriptions were delivered directly to patients homes by pharmaceutical companies, but at that time, they could not be realized due to the need for cross-regional delivery. (N 36)
At first, due to our usual prescription of one to two months worth of medication, in March, we did not have as much medication due to insufficient inventory. At that time, suppliers delivering the medication also faced stock shortages, so we had to limit the quantity of prescription drugs, typically to two to four weeks. By April, with some deliveries resuming, we were able to issue medication for nearly two months worth of prescriptions. (N 6)
Regarding long-term and extended prescriptions, current practices primarily focus on just two chronic conditions - hypertension and diabetes. For these diseases, the prescribed medications are typically limited to therapeutic drugs only, explicitly excluding both adjuvant medications and traditional Chinese patent medicines. (C11)
General Medical Training and Career Development Path
Currently, an increasing number of Family Physicians were entering the profession through general practitioner training. Unlike previous studies on the general practitioner training system, which concentrated on patients with chronic infectious diseases, the recent training included additional content to address public health emergencies. This expansion aimed to enhance the early warning awareness and response capabilities of general practitioners.
I underwent a three-year standardized training program for general practitioners, which covers the field of general medicine. During the pandemic, I participated in epidemiological investigations, patient transfers, and fever patient classification among other frontline tasks. We also had many online courses on epidemic prevention and control as well as physician training, which gave me more confidence in handling various emergencies. (N 3)
Wearing and removing isolation garments and protective attire, collecting nasal and pharyngeal swabs, conducting epidemiological investigations, and implementing infection prevention and control measures in hospitals and quarantine locations were all integral components of our daily general practitioner training and educational curriculum, which were closely tied to epidemic prevention and control efforts. (N 26)
The low professional identity of primary healthcare workers can easily lead to occupational burnout and severe talent loss, affecting the stability of primary healthcare institutions. During the pandemic, primary healthcare institutions grappled with not only shortages such as a lack of beds and medical equipment but also challenges like insufficient epidemic prevention personnel and inadequate emergency response capabilities.
I noticed that many primary healthcare workers feel their work does not receive adequate social recognition and respect.This may be due to high work pressure, income that does not match the effort, and unclear career prospects.Long-term high-intensity work and continuous work pressure have led many primary healthcare workers to feel exhausted and disheartened. (N 14)
Many general practitioners had taken on additional responsibilities beyond their routine duties during the pandemic, such as temporarily becoming specialists in COVID-19 and engaging in community control efforts. While this role transition helped address immediate emergencies, it might have also led to a decline in their general medical skills, potentially affecting their long-term career development. Furthermore, the long-term impact of the pandemic on the healthcare industry was still unclear at that time, possibly necessitating adjustments to the curriculum and career paths for general practitioner training programs. (N 12)
Discussion
Micro-Level Influences
Family Physicians have seen a reduction in their discretionary power during the COVID-19 pandemic. Therefore, in this process of responding to the epidemic, Chinese medical personnel did not fully exercise their discretionary powers and autonomy.12 In countries where the outbreak is out of control, such as Brazil and the United States, health care workers have had to rely on personal experience to make decisions because the guidelines set by the governments of the two countries were not clear or specific enough.7,13,14 Instead, Family Physicians had more discretion. Research has shown that rapidly evolving bureaucratic structures relied heavily on Ministry of Health regulations, while frontline workers adopted coping strategies in response to pandemic-induced challenges such as fear, information gaps, and staff shortages.15 The difference in discretionary power can be partly attributed to the highly explicit yet stringent policy environment facing Chinese physicians. This environment led to their discretion being manifested as nuanced interpretation and communication of policies, rather than autonomy in clinical decision-making.
Family Physicians selectively provided services to various scenarios and recipients during public health emergencies. Under the mandatory requirement for nucleic acid testing resumption, they were concerned about the potential rupture of doctor-patient relationships, which could undermine the long-term trust established before the pandemic, while also facing the pressure of comprehensive epidemic prevention and control screening. For instance, when general practitioners in the UK encountered women affected by female genital mutilation and their families, the complexity of consultations and potential trust issues caused by the mandatory reporting obligation often led general practitioners to provide documentation and patiently explain the basis and necessity of policy enforcement to repair the resulting tension.16 Therefore, the extent to which Family Physicians understand policies and communicate with citizens determines policy success. The safety and well-being of the working environment for Family Physicians is another challenge. The pandemic has exacerbated the anxiety, stress, and fear of personal safety, health, and the lives of relatives and patients among Family Physicians. Physician burnout is characterized by a lack of agency and alienation, which can lead to irritability, poor decision-making, and negative impacts on interpersonal relationships.17 Young Family Physicians tend to take on more work abuse.18
The disparity in discretionary power is crucial within the unique context of China’s pandemic response: the core challenge for family physicians was not a lack of clinical autonomy, as often seen in Western contexts, but rather the communicative pressure and role conflict they faced as “policy mediators” operating within a highly explicit yet rigid policy environment. This difference reveals the essence of grassroots healthcare work under strong state capacity—the key role of family physicians shifted from clinical decision-making to policy interpretation and trust maintenance. The inherent tension lies in the conflict between the efficient top-down implementation of public health mandates and the preservation of long-term doctor-patient relationships. This finding suggests that addressing their challenges and formulating supportive policies should move beyond conventional approaches of enhancing clinical autonomy, and instead focus on strengthening communication skills, optimizing policy buffering mechanisms, and establishing systematic psychological support systems.
Meso-Level Influences
During public health emergencies, general practitioners demonstrated adaptive capacities in policy implementation under resource-constrained conditions. A UK study found that micro-level rapport and common sense, meso-level workplace culture and procedural practices, and macro-level service capacity limitations and digital technology adoption shaped policy implementation and service delivery.19 When upward referral mechanisms were disrupted due to inadequate contingency plans or sudden closures of designated hospitals, frontline healthcare workers developed pragmatic solutions to maintain medical services. Empirical observations revealed that when encountering referral obstacles, some general practitioners proactively established direct contact with receiving hospitals, while neighborhood committees occasionally arranged alternative transportation using municipal vehicles when emergency response systems were overloaded. These operational adaptations, though limited to administrative jurisdictions, ensured the provision of essential healthcare services during lockdown periods.
The coordination gaps between primary healthcare systems, clinical systems, and public health institutions necessitated the establishment of temporary communication channels.20 Among 36 interviewed general practitioners, 29 reported having established provisional information-sharing mechanisms with tertiary hospitals (particularly for COVID-19 case management). Service delivery models were flexibly adjusted, with most community health centers implementing telemedicine services. Health commission data indicated significant growth in the utilization of WeChat communication groups during lockdowns.21 It must be emphasized that these adjustments constituted emergency operational modifications rather than systematic policy redesign, with decision-making authority consistently residing at the municipal health administration level in all documented cases. This finding is consistent with previous studies, which highlighted incompatibilities between street-level bureaucracy (SLB) policies and implementation systems by demonstrating how frontline workers improvised strategies—such as ad-hoc extracorporeal membrane oxygenation (ECMO) delivery—under resource constraints and environmental challenges, ultimately leading to inconsistent service quality and delayed responses.22
Macro-Level Influences
Family Physicians encountered ambiguities when executing tasks concerning public health policies. Given the urgency and severity of COVID-19, they had to devote a considerable amount of time to reading and processing the pandemic-related guidelines and information. Because of the diversity of information sources and the frequent updates of guidelines,it is difficult to maintain up-to-date knowledge of the latest guidelines and implement them.20 The Royal Australian College of General Practitioners, the Australian General Practitioners Association, and local general practitioner groups continued to promote and update their services daily to meet the health service needs of residents. Meanwhile, primary health networks assumed roles in state and national contact coordination and supply chain management.23 When the Family Physician policy and implementation system were incompatible, Family Physicians faced challenges such as insufficient resources and a suboptimal service environment. These issues led to a sluggish response in medical services and made it difficult to ensure the quality of medical care.22
At the policy level, the National Medical Reserve Management Measures24 faced challenges due to the absence of clear regulations governing the operational aspects of the national pharmaceutical reserve system, which complicated implementation. Key issues included the lack of defined application and approval processes, as well as comprehensive operational guidelines for reserve logistics. These gaps could lead to critical problems such as reserves being available but not distributed, and supplies being distributed without proper replenishment. Economic constraints also affected pharmaceutical reserves, often resulting in inadequate funding that caused incomplete and insufficient stock varieties and quantities. This was especially problematic during the early phases of major disasters or pandemics, where achieving effective control was particularly challenging. The national regulations stipulate that the total physical reserve must not be less than 70% of the planned total, but actual surveys show that over 40% of units only maintain physical reserves, with very few adopting capacity-based reserves or other forms.25 In addition, the improper use of pharmaceutical reserve funds, such as misappropriation of reserve funds and the lack of dedicated accounts, increases the risk that physical reserves cannot be timely supplied in the event of major disasters or pandemics. The lag in the construction of integrity mechanisms is also an issue, making it difficult to implement the principles of “use first, then replenish” and “paid requisition” for pharmaceutical reserve materials in practice, leading to a loss of enthusiasm among storage enterprises and their supervisory authorities, which affects the effective procurement of pharmaceutical reserve materials.25
The pandemic has posed new challenges to the field of family medicine/primary care education, particularly in medical education, research and quality assurance.26 European general and family medicine education is based on the six core competencies of family medicine, and pandemic prevention measures are included in the educational agenda of the European General and Family Medicine Teachers Association (European Academy of Teachers in General Practice and Family Medicine, EURACT).27 During the COVID-19 period, teaching content and methods were undergoing significant changes, including the evaluation and validation of new teaching methods such as online lectures and online exams to adapt to the current teaching environment. Additionally, it is necessary to impart this knowledge to teachers so they can acquire the new skills required to cope with all these changes, ensuring the quality of future teaching.26
China’s COVID-19 response adopted a “central-local” tiered governance model. At the national level, the National Health Commission and State Council formulated unified prevention and control guidelines, encompassing containment measures, testing strategies, and vaccine distribution plans.28 Local governments, meanwhile, adapted these policies flexibly according to actual circumstances, such as modifying quarantine durations or mobilizing community healthcare workers for epidemiological investigations. The Chinese healthcare system operates under a hierarchical diagnosis and treatment framework: primary medical institutions like community health centers serve as first-contact facilities, while secondary/tertiary hospitals handle complex and severe cases. During the pandemic, this system facilitated tiered case management - mild cases were treated at primary institutions, with severe cases referred to higher-level hospitals. Resource allocation similarly reflected this hierarchical approach: the central government coordinated the production and distribution of critical supplies (eg, PPE, ventilators), while local governments managed regional stockpiles and personnel deployment. This multi-level governance structure enabled both standardized policy implementation and localized operational flexibility in pandemic response.28
Policy Implications
At the micro-level, it is necessary to clarify role boundaries and enhance frontline empowerment. Addressing the dual role pressures and reduced discretionary power faced by family physicians, we recommend defining flexible decision-making space in emergency response plans, such as allowing medication regimen adjustments within a certain range based on patient conditions. Simultaneously, policy interpretation and emergency communication skills should be integrated into the family physician training system to improve their effectiveness in explaining containment policies to residents and alleviate implementation conflicts arising from comprehension gaps.
At the meso-level, dynamic resource allocation and collaborative governance mechanisms should be established. To address supply-demand contradictions caused by resource shortages, we recommend creating a “peacetime-emergency integrated” healthcare resource coordination platform for intelligent monitoring and emergency allocation of primary-level supplies. Furthermore, family physicians should be incorporated into the community-level joint prevention and control command system, fully leveraging their expertise in pandemic risk assessment and key population management, and facilitating their transition from passive executors to active coordinators.
At the macro-level, institutional supply and systematic support must be strengthened. Targeting issues such as policy ambiguity and fragile drug supply chains, we recommend clearly defining the role and responsibility positioning of family physicians in national public health policies and improving emergency operation guidelines compatible with their roles. Concurrently, the security of essential drug supply chains should be integrated into urban resilience construction planning, and the vitality of the general practitioner workforce should be stimulated by improving career development pathways, providing promotion incentives for those demonstrating outstanding performance during emergencies. In summary, policy design should shift from a “control logic” to an “empowerment logic”. By institutional decentralization, flexible resource allocation, and professional value recognition, a new primary care service landscape that maintains baseline standards while fostering vitality can be constructed.
Limitations
This study has several limitations that warrant acknowledgment. First, the reliance on retrospective accounts during interviews may introduce recall bias. As participants reflected on their experiences during the public health emergency—in some cases, several months after the events—their recollections could have been influenced by the passage of time, subsequent policy changes, or personal reflections, potentially affecting the accuracy and completeness of the data. Second, the focus on family physicians from only two community health centers in Shanghai, while allowing for in-depth qualitative analysis, limits the generalizability of the findings. Shanghai’s healthcare infrastructure and resource distribution are not fully representative of other regions in China, particularly rural or less-developed areas. This narrow scope may overlook significant regional heterogeneity in terms of resource availability, policy implementation, and operational challenges, thus constraining the broader applicability of the results.
Although this study applied a multi-level (macro-meso-micro) analytical framework, the interactions between these levels were not fully explored. The complex, dynamic relationships between individual discretion, organizational support, and national policy remain an area for further investigation. Future research could employ mixed-methods or longitudinal designs to capture real-time data during emergencies and expand sampling to include more diverse geographical and institutional settings, thereby strengthening the external validity and theoretical integration of findings.
This study’s emphasis on micro-level challenges naturally stems from its empirical grounding in frontline experiences; however, a comprehensive understanding of health system resilience necessitates future research that deliberately integrates meso- and macro-level analyses, particularly concerning supply chain logistics, national policy design, and long-term training pathways.
Conclusion
This study deepens the understanding of service supply challenges for family physicians during public health emergencies by systematically applying the street-level bureaucracy theory across micro-, meso-, and macro-analytical levels. Compared with prior research, our unique contribution lies in revealing the intrinsic connections among the multi-level challenges faced by family physicians. At the practical level, the findings emphasize the need for systematic interventions, including clarifying policy directives, strengthening the supply chain保障 of essential medicines, and improving career development pathways for general practitioners. Additionally, institutional mechanisms supporting adaptive implementation should be established, rather than relying solely on individual prosocial innovative behaviors. Looking ahead, the three-tier analytical framework developed in this study provides a transferable theoretical tool for analyzing other street-level bureaucrats (such as public health nurses and social workers) in crisis contexts. Future research could apply this framework to compare emergency response practices across different governance settings.
Patient and Public Involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, Li Luo, upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethics Committee for Medical Research of the School of Public Health, Fudan University (Approval No. IRB#2025-01-1199, valid until June 30, 2025), and written informed consent was obtained from all participants. Informed consent was obtained from participants for the publication of their anonymized responses and direct quotes.
Acknowledgments
We would like to express our sincere gratitude to the Xie Tu Street and Kang Jian Street Community Health Service Centers in Xuhui District, Shanghai, for their invaluable assistance in conducting interviews with Family Physicians.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research is funded by the “Research on Reconstructing the Family Physician Service Model in the Context of Regional Medical Care” project, which is a major research project in philosophy and social sciences launched by the Ministry of Education (Grant No. 20JZD027).
Disclosure
The authors declare no competing interests in this work.
References
1. Garg S, Engtipi K, Kumar R, Garg A. Role of family physicians in providing primary healthcare during COVID-19 pandemic. J Family Med Prim Care. 2022;11(11):6687–6689. doi:10.4103/jfmpc.jfmpc_2209_20
2. Lee JQ, Loke W, Ng QX. The role of family physicians in a pandemic: a blueprint. Healthcare. 2020;8(3). doi:10.3390/healthcare8030198
3. Phillips RLJ, Bazemore AW. Primary care and why it matters for U.S. health system reform. Health Aff. 2010;29(5):806–810. doi:10.1377/hlthaff.2010.0020
4. Mathews M, Ryan D, Hedden L, et al. Family physicians’ responses to personal protective equipment shortages in four regions in Canada: a qualitative study. BMC PRIMARY CARE. 2023;24(1). doi:10.1186/s12875-022-01958-7
5. Vilovic T, Bozic J, Zuzic Furlan S, et al. Mental health well-being and attitudes on mental health disorders among family physicians during COVID-19 pandemic: a connection with resilience and healthy lifestyle. J Clin Med. 2022;11(2):438. doi:10.3390/jcm11020438
6. Lipsky M. Street Level Bureaucracy: Dilemmas of the Individual in Public Services. Russell Sage Foundation; 1980. Available from: http://www.jstor.org/stable/10.7758/9781610447713.
7. Burki T. China’s successful control of COVID-19. Lancet Infect Dis. 2020;20(11):1240–1241. doi:10.1016/S1473-3099(20)30800-8
8. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395(10239):1802–1812. doi:10.1016/S0140-6736(20)30122-7
9. Biddle B. Recent Development in Role Theory. Annu Rev Sociol. 2003;12:67–92. doi:10.1146/annurev.so.12.080186.000435
10. Sutcliffe K, Vogus TS, M K, Vogus TJ.Organizing for resilience. positive organizational scholarship: foundations of a new discipline;San Francisco, CA, Berrett-Koehler;2003.94–110
11. García L. Institutional Logics and the Historical Contingency of Power in Organizations; 2016. doi:10.13140/RG.2.1.4264.5367
12. Méndez D, Gómez S, Camargo Y. Healthcare workers during the COVID-19 pandemic from a street-level bureaucracy perspective - a narrative review of literature. Universitas Médica. 2021;62:135–150. doi:10.11144/javeriana.umed62-4.call
13. Lasco G. Medical populism and the COVID-19 pandemic. Global Public Health. 2020;15:1417–1429. doi:10.1080/17441692.2020.1807581
14. Lotta GS, Coelho VSP, Brage ET. How COVID-19 has affected frontline workers in brazil: a comparative analysis of nurses and community health workers. J. Comp. Policy Anal. 2020;23:63–73.
15. Civinskas R, Dvorak J, Sumskas G. Beyond the front-line: the coping strategies and discretion of lithuanian street-level bureaucracy during covid-19. Corvinus J. Sociol. Soc. Policy. 2021;12(1):3–28. doi:10.14267/CJSSP.2021.1.1
16. Dixon S, Hinton L, Ziebland S. Supporting patients with female genital mutilation in primary care: a qualitative study exploring the perspectives of GPs’ working in England. Br J Gen Pract. 2020;70(699):E749–E756. doi:10.3399/bjgp20X712637
17. Marshall M, Howe A, Howsam G, Mulholland M, Leach J. COVID-19: a danger and an opportunity for the future of general practice. Br J Gen Pract. 2020;70(695):270–271. doi:10.3399/bjgp20X709937
18. Azam K, Khan A, Alam MT. Causes and adverse impact of physician burnout: a systematic review. J. Coll. Physicians Surg. Pak. 2017;27(8):495–501.
19. Litchfield I, Gale N, Burrows M, Greenfield S. “You’re only a receptionist, what do you want to know for?”: street-level bureaucracy on the front line of primary care in the United Kingdom. Heliyon. 2023;9(11):e21298. doi:10.1016/j.heliyon.2023.e21298
20. Andersen JH, Moller A, Due TD. Making sense of and working with COVID-19 related guidelines and information in Danish general practice-A qualitative study. PLoS One. 2023;18(2):e0281579. doi:10.1371/journal.pone.0281579
21. Burn E, Fisher R, Locock L, Smith J. A longitudinal qualitative study of the UK general practice workforce experience of COVID-19. Prim. Heath Care Res. Dev. 2022;23. doi:10.1017/S1463423622000391
22. Mukuru M, Kiwanuka SN, Gibson L, Ssengooba F. Challenges in implementing emergency obstetric care (EmOC) policies: perspectives and behaviours of frontline health workers in Uganda. Health Policy and Planning. 2021;36(3):260–272. doi:10.1093/heapol/czab001
23. Jackson CL. Living with COVID-19 in 2022: the impact of the pandemic on Australian general practice. Med j Aust. 2022;216(9):
24. Central People’s Government of the People’s Republic of China. Circular on the issuance of the measures for the management of national pharmaceutical stockpiles (Revised in 2021). Available from: https://www.gov.cn/zhengce/zhengceku/2021-12/11/content_5659979.htm.
25. Zhou J, Wu Y, Dong Z, Sun G. Problems and suggestions for improving China’s medical reserve system under the COVID-19. Pharm Today. 2020;30(9):4.
26. Windak A, Frese T, Hummers E, et al. Academic general practice/family medicine in times of COVID-19-Perspective of WONCA Europe. Eur J Gener Pract. 2020;26(1):182–188. doi:10.1080/13814788.2020.1855136
27. Heyrman J. EURACT the European Academy of Teachers in General Practice. Eur. J. Gen. Pract. 2001;7:122–124.
28. The Central People’s Government of the People’s Republic of China. China’s actions in the fight against COVID-19. Available from: https://www.gov.cn/zhengce/2020-06/07/content_5517737.htm.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.