Back to Journals » Journal of Pain Research » Volume 12
Failed dural puncture during needle-through-needle combined spinal–epidural anesthesia: a case series
Authors Doo AR ![]() , Shin YS
, Shin YS ![]() , Choi JW, Yoo S
, Choi JW, Yoo S ![]() , Kang S, Son JS
, Kang S, Son JS ![]()
Received 29 June 2018
Accepted for publication 7 December 2018
Published 17 May 2019 Volume 2019:12 Pages 1615—1619
DOI https://doi.org/10.2147/JPR.S178640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
A Ram Doo,1,2 Yu Seob Shin,2,3 Jin-wook Choi,1 Seonwoo Yoo,1 Sehrin Kang,1 Ji-seon Son1,2
1Department of Anesthesiology and Pain Medicine, Chonbuk National University Medical School, Jeonju, South Korea; 2Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, South Korea; 3Department of Urology, Chonbuk National University Medical School, Jeonju, South Korea
Objective: Combined spinal–epidural (CSE) anesthesia is a widely used neuraxial anesthetic technique. In clinical practice, failed dural puncture during needle-through-needle technique occasionally occurs, with incidence of 5%–29%. We radiologically evaluated four cases of failed dural puncture during needle-through-needle CSE anesthesia.
Case series: Four patients received CSE anesthesia for elective orthopedic surgery. CSE procedures were performed in the same manner using a CSE device for needle-through-needle technique. An epidural needle was inserted in midline at L4/5 interspaces using loss of resistance to air whilst patients lay in the lateral decubitus position. The spinal needle was then inserted through the epidural needle for subarachnoid block, however, negative cerebrospinal flow was identified. Subsequently, radiographic imaging using C-arm fluoroscopy was performed to evaluate the status of needles. We found that epidural needles were considerably deviated from the midline, while spinal needles exited epidural needles, not through back holes, but through the Tuohy curve in three patients. In one patient, when the spinal needle was inserted to 12 mm, the anesthesiologist felt the needle touching the bony structure. The spinal needle was in contact with the superior articular process of the fifth lumbar vertebra, which was confirmed by C-arm radiography.
Conclusion: Excessive paramedian deviation of the epidural needle may affect dural puncture during needle-through-needle CSE technique. Moreover, wrong passage of the spinal needle through Tuohy curve instead of the back hole, may contribute to failure of dural puncture.
Keywords: combined spinal–epidural anesthesia, dural puncture, fail
Introduction
Combined spinal–epidural (CSE) anesthesia is a widely used neuraxial anesthetic technique for orthopedic or obstetric surgery and labor analgesia, because it has great advantages, including rapid onset, profound regional blockade with ability of prolonged anesthesia via catheter, and the usage for postoperative epidural analgesia. CSE using reduced dose of spinal bupivacaine with epidural top up has been investigated to be associated with faster motor recovery after surgery.1
Several techniques as well as devices for CSE are available worldwide.2,3 Above all, needle-through-needle technique (single segment technique) is an increasingly popular technique in which intrathecal block is performed before epidural catheterization through the single route of needle entry. Needle-through-needle technique has been advanced technically with various safety devices, including spinal–epidural interlocking system and a “back hole” at the epidural needle curve.4–6 However, this technique still has some controversies about needle handling, the risk of catheter migration intrathecally, and relatively frequent failure of subarachnoid block. In clinical practice, cerebrospinal fluid (CSF) flow is not observed occasionally despite the spinal needle is advanced enough to reach dura and intrathecal space through the epidural needle during needle-through-needle technique. Reported incidence of failed dural puncture during needle-through-needle technique ranges from 5% to 29%.3,6,7
We experienced four cases of failed dural puncture during needle-through-needle CSE technique for elective orthopedic surgery. The status of needle position was radiologically evaluated based on anteroposterior X-ray image using C-arm fluoroscopy. Possible explanation for the failed dural puncture during CSE is discussed in this report.
Case series
Written informed consent for disclosing this case report was obtained from each patient. Due to the retrospective nature of the study and the fact that CSE using needle-through-needle technique has been approved for orthopedic or obstetric surgery and labor analgesia in Korea, the study did not require approval by the local ethics committee. Nevertheless, our study was conducted in line with the Good Clinical Practice guidelines and the ethical principles laid down in the latest version of the Declaration of Helsinki. We experienced four cases of failed dural puncture during CSE using needle-through-needle technique for elective orthopedic surgery. Patient characteristics and details for these procedures are described in Tables 1 and 2, respectively. CSE procedures were performed in the same manner using CSE set (Espocan®; B.Braun Medical Inc., Daytona Beach, FL, USA) by third- or fourth-year anesthesia resident under supervision of an anesthesia professor in all cases. Espocan® CSE set consists of epidural needle (18 G, 88 mm in length, Tuohy needle with back hole), spinal needle (27 G, 138.5 mm in length, pencil point needle), and epidural catheter (20 G, 1,000 mm in length, multiorifice catheter). Patient was placed in the lateral decubitus position with the operative leg down. The spine of patient was flexed to facilitate exposure of interspinous space. Epidural needle was inserted in midline approach at L4/5 interspaces identified by Tuffier’s line palpation method. After confirming epidural space using loss of resistance to air, the spinal needle was inserted through the epidural needle until the manufacturer’s gradation line indicating protrusion beyond the epidural needle tip for subarachnoid block. If CSF flow was negative, the spinal needle was advanced further stepwise up to maximal protrusion length of 17 mm while checking CSF flow frequently.
 | Table 1 Patient characteristics Abbreviation: ASA/PS, American Society of Anesthesiologists classification of physical status. |
 | Table 2 Procedure details Notes: aTransient paresthesia during spinal needle insertion in case 3. bThe spinal needle was touching a bony structure at the protrusion length of 12 mm. |
In cases 1–3, CSF flows through spinal needles were negative despite needles were advanced stepwise up to 17 mm. We promptly performed radiographic imaging using C-arm fluoroscopy to evaluate the reason why subarachnoid block failed. We found that epidural needles were considerably deviated from the midline, although the anesthesiologists intended to approach needles straight in midline as our usual practice. Moreover, spinal needles exited epidural needles not through back holes, but through the Tuohy curves as presented in Figure 1(A–C). In case 4, CSE procedure was performed in the same manner as other cases. When the spinal needle was inserted to 12 mm, the anesthesiologist felt the needle touching bony structure. The spinal needle was in contact with the superior articular process of the fifth lumbar vertebra, which was confirmed by C-arm radiography (Figure 2). Finally, CSF flow was not obtained through the spinal needle.
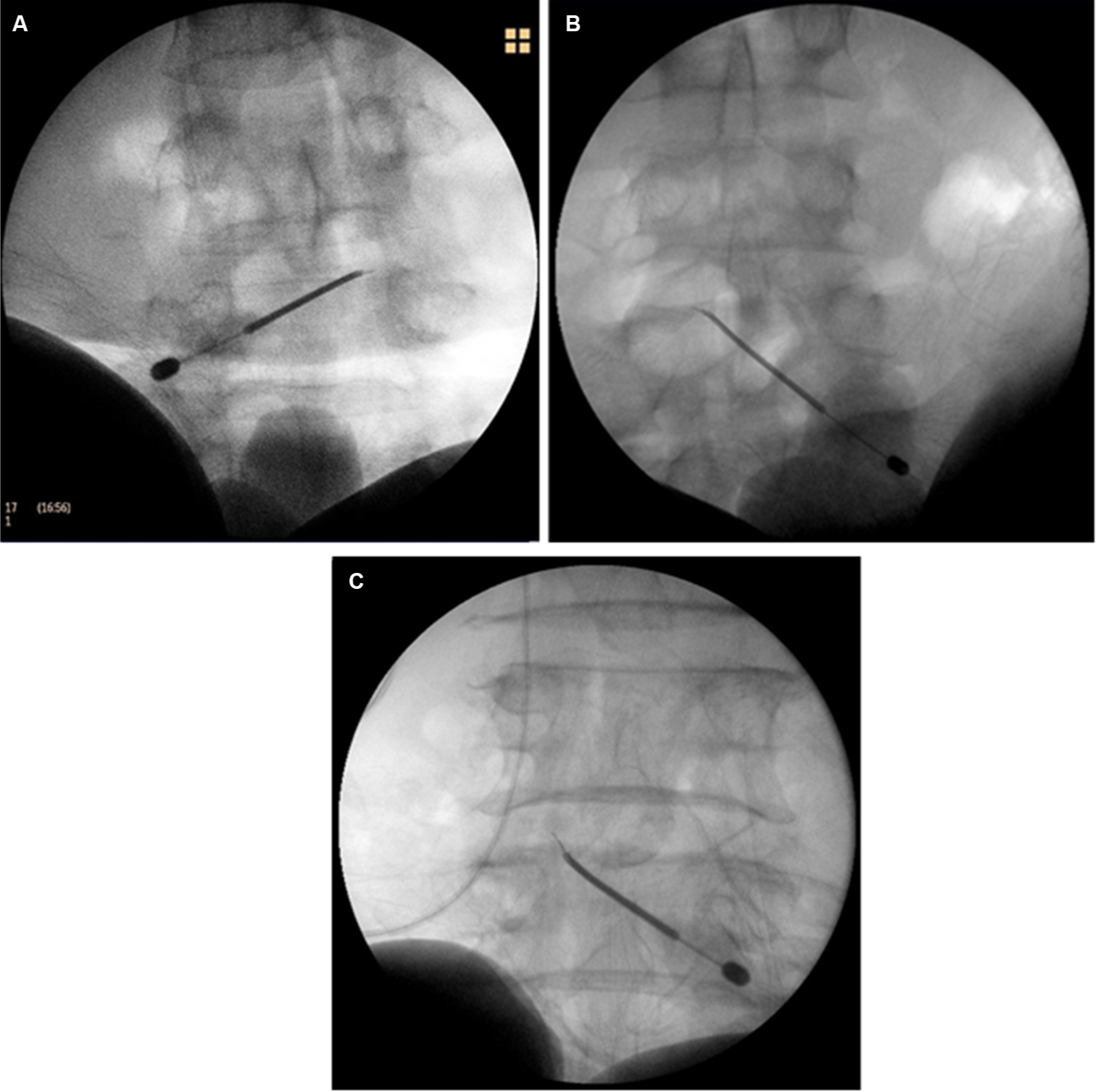 | Figure 1 Anteroposterior radiographs of patients with failed dural puncture during needle-through-needle technique for combined spinal–epidural anesthesia. Notes: Images showing excessive paramedian deviation of the epidural needle and the wrong passage of the spinal needle through Tuohy curve in cases 1 (A), 2 (B), and 3 (C). |
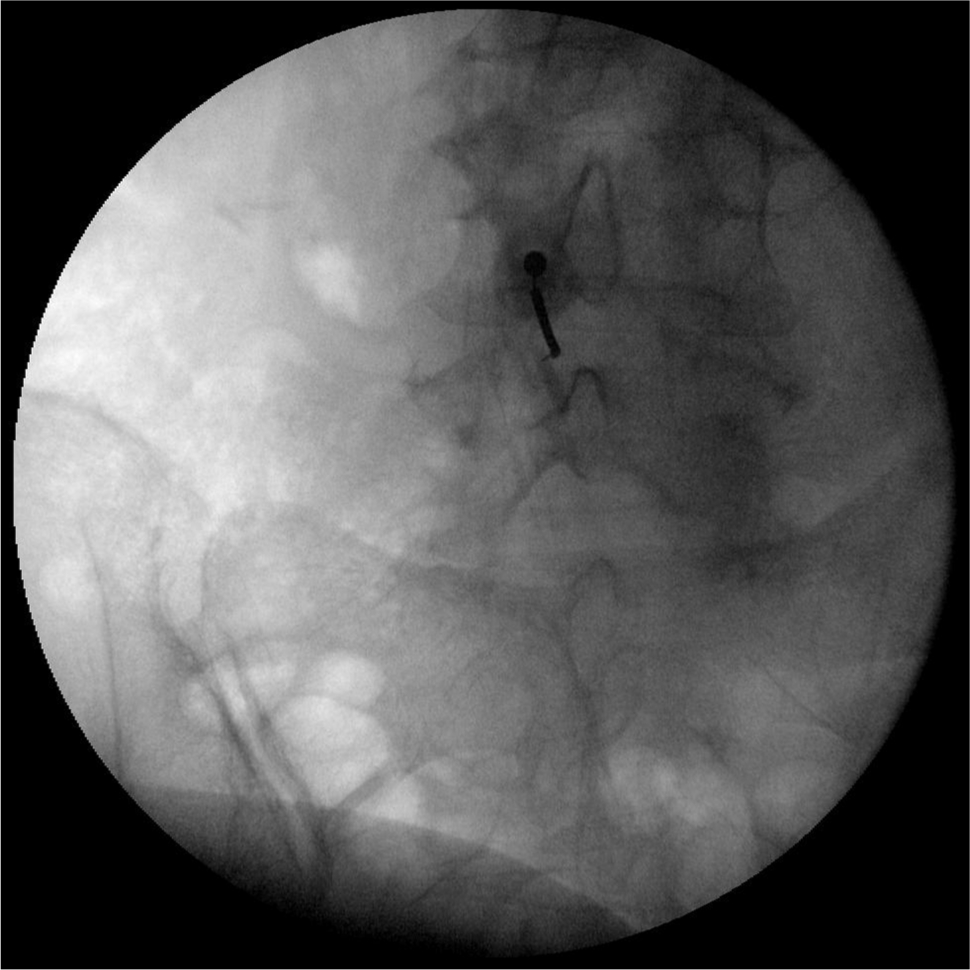 | Figure 2 Anteroposterior radiograph showing the spinal needle being in touch with the superior articular process of the fifth lumbar vertebra in case 4. |
In all cases, after removal of the spinal needle, epidural catheter was inserted by 3 to 5 cm into epidural space and fixed. Subarachnoid block was successfully performed using a separate spinal needle at L3/4 interspace uneventfully. The level of regional blockade and qualities of anesthesia were satisfactory. Orthopedic surgeries were completed without any complication. Although the patient in case 3 complained of transient paresthesia during insertion of spinal needle, there were no neurologic complications that developed subsequent to the procedure.
Discussion
CSE anesthesia is a popular neuraxial anesthetic technique for orthopedic or obstetric surgery and labor analgesia. It is well understood that CSE improves the quality of regional anesthesia. Recently, several authors have reported that reduced spinal dose with concomitant epidural supplementation, as a regional anesthetic method, is associated with faster motor recovery after surgery.1,8,9,10 It might be used as a valuable regional anesthetic technique, especially in ambulatory surgery.
Various techniques and devices for CSE have evolved considerably over the past few years. However, ideal CSE technique still remains controversial.2,3,5 Although double space technique has higher success rate than needle-through-needle technique,7,11 the needle-through-needle technique is still a popular technique because of its advantages such as short performance time, reduced patient discomfort and tissue trauma by single needle entry, and convenience in its usage.7,12 The incidence of failed dural puncture during needle-through-needle CSE technique has been reported to be 5%–29%.3,6,7 However, these studies only presented clinical outcomes including success rate or complications of needle-through-needle technique compared to traditional double segment technique. To the best of our knowledge, this is the first report that suggests a possible explanation for failed dural puncture during needle-through-needle CSE technique with radiological findings.
In this case report, the reason for failed dural puncture might be explained partly by wrong passage of the spinal needle through the Tuohy curve instead of the back hole and excessive displacement of epidural needle. Needle-through-needle CSE technique has been advanced to improve success rate and reduce complications with several safety devices including spinal–epidural interlocking system, which helps immobilize the spinal needle during intrathecal drug injection and a “back hole” at the epidural needle curve.4–6 Back hole provides an independent channel for spinal needle to facilitate the spinal needle to advance straight through the back hole and penetrate dura. Moreover, it may prevent migration of epidural catheter intrathecally by separating the route for epidural catheter from spinal needle. Nevertheless, there is still possibility of the wrong passage of the spinal needle as shown in this report. The authors found that the spinal needle exited the epidural needle not through the back hole, but through the Tuohy curve as shown in anteroposterior radiographic images (Figure 1A–C). For these cases, the spinal needle might have been unintentionally bent while passing through the Tuohy curve, thus failing to puncture dura matter appropriately.
In cases 1–3, CSF flows through the spinal needle were negative despite needles being advanced up to 15 mm beyond the epidural needle tip. Spinal needle of CSE set (Espocan®, B.Braun Medical Inc.) used in the study has a protrusion length of 17 mm, which is sufficient to reach the dura. However, excessive deviation of the epidural needle from the midline may lengthen the distance between the tip of the epidural needle and the dura, thus disturbing the spinal needle penetrating dura. In the extreme, the tip of the spinal needle might glide on the posterior dura because the needle would be running parallel to the dura. Several authors have assumed that the failure of dural puncture during CSE might be caused by unintentional paramedian placement of the epidural needle, incorrect (not epidural) placement of the epidural needle, or tenting of the dura.3,6,13 In this report, we demonstrated such hypothesis by radiological findings. In addition, it is quite difficult to handle and keep the long, thin, and flexible 27 G spinal needle straight. Consequently, the spinal needle cannot approach the dura at an appropriate angle to penetrate the dura.
The relevance between certain radiographic factors, which quantify the spatial relationship between the needle and spinal structure, and clinical outcomes including success or complication rate of CSE may be investigated in the future. If we had obtained lateral radiographs in addition to anteroposterior images, it would be easier to predict the location of the needle tip in the spinal canal. This is a limitation of this case report. Meanwhile, it might be uncertain to conclude that placements of epidural needles were appropriate in these cases of failed dural puncture, although we used loss of resistance to air methods to perceive epidural needles reaching into the epidural space. However, all procedures were supervised by skilled anesthesia professor with experience of regional anesthesia for more than 10 years, and epidural catheter secured in the original position was used postoperatively and it resulted in the expected block for all patients.
Conclusion
Excessive paramedian deviation of the epidural needle may affect dural puncture during needle-through-needle CSE technique. Moreover, wrong passage of the spinal needle through Tuohy curve instead of the back hole may contribute to the failure of dural puncture.
Acknowledgment
This study was supported by funds from the Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, South Korea.
Author contributions
All authors contributed toward data analysis, drafting, and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Yun MJ, Kwon MY, Kim DH, Lee JW. Combined spinal-epidural anesthesia using a reduced-dose of spinal bupivacaine and epidural top up leads to faster motor recovery after lower extremity surgeries. Korean J Anesthesiol. 2014;66(1):28–33. | ||
Cook TM. Combined spinal-epidural techniques. Anaesthesia. 2000;55(1):42–64. | ||
Saigal D, Wason R. Paramedian epidural with midline spinal in the same intervertebral space: an alternative technique for combined spinal and epidural anaesthesia. Indian J Anaesth. 2013;57(4):364–370. | ||
Stocks GM, Hallworth SP, Fernando R. Evaluation of a spinal needle locking device for use with the combined spinal epidural technique. Anaesthesia. 2000;55(12):1185–1188. | ||
Puolakka R, Pitkänen MT, Rosenberg PH. Comparison of technical and block characteristics of different combined spinal and epidural anesthesia techniques. Reg Anesth Pain Med. 2001;26(1):17–23. | ||
Browne IM, Birnbach DJ, Stein DJ, O’Gorman DA, Kuroda M. A comparison of Espocan and Tuohy needles for the combined spinal-epidural technique for labor analgesia. Anesth Analg. 2005;101(2):535–540. | ||
Backe SK, Sheikh Z, Wilson R, Lyons GR. Combined epidural/spinal anaesthesia: needle-through-needle or separate spaces? Eur J Anaesthesiol. 2004;21(11):854–857. | ||
Powell MF, Blakely CM, Sakawi Y, Frölich MA. Comparing low-dose bupivacaine with epidural volume extension to standard bupivacaine dosing for short obstetric procedures: a prospective, randomized study. Minerva Anestesiol. Epub 2018 Sep 18. | ||
Heesen M, Weibel S, Klimek M, Rossaint R, Arends LR, Kranke P. Effects of epidural volume extension by saline injection on the efficacy and safety of intrathecal local anaesthetics: systematic review with meta-analysis, meta-regression and trial sequential analysis. Anaesthesia. 2017;72(11):1398–1411. | ||
Kim DY, Han JI. Effects of saline and bupivacaine for epidural top-up on sensory blockade level during combined spinal epidural anesthesia. Korean J Pain. 2000;13(1):84–88. | ||
Ahn HJ, Choi DH, Kim CS. Paraesthesia during the needle-through-needle and the double segment technique for combined spinal epidural anaesthesia. Anaesthesia. 2006;61(7):634–638. | ||
Casati A, D’Ambrosio A, de Negri P, Fanelli G, Tagariello V, Tarantino F. A clinical comparison between needle-through-needle and double-segment techniques for combined spinal and epidural anesthesia. Reg Anesth Pain Med. 1998;23(4):390–394. | ||
Holmström B, Rawal N, Axelsson K, Nydahl PA. Risk of catheter migration during combined spinal epidural block: percutaneous epiduroscopy study. Anesth Analg. 1995;80(4):747–753. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.