Back to Journals » Patient Preference and Adherence » Volume 16
Factors Related to Diabetes Self-Management Among Patients with Type 2 Diabetes: A Chinese Cross-Sectional Survey Based on Self-Determination Theory and Social Support Theory
Authors Chen M, Yun Q, Lin H, Liu S, Liu Y, Shi Y, Ji Y, Chang C
Received 26 August 2021
Accepted for publication 22 December 2021
Published 6 April 2022 Volume 2022:16 Pages 925—936
DOI https://doi.org/10.2147/PPA.S335363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Meijun Chen,1 Qingping Yun,1 Haoxiang Lin,1 Shenglan Liu,2 Yihua Liu,1 Yuhui Shi,1 Ying Ji,1 Chun Chang1
1School of Public Health, Peking University, Beijing, People’s Republic of China; 2Department of Social Development, Development Research Center of the State Council, Beijing, People’s Republic of China
Correspondence: Chun Chang School of Public Health, Peking University, Beijing, People’s Republic of China Tel +8613601235974 Email [email protected]
Purpose: Self-management behavior (SMB) plays a significant role in glycemic control. This study aimed to explore the factors related to SMB among patients with type 2 diabetes and how these factors interacted with each other.
Patients and Methods: Patients diagnosed with type 2 diabetes were recruited from 18 community healthcare stations (CHSs) from six community healthcare centers (CHCs) in Beijing, China from April to May in 2017. Motivation, competence, autonomy support, social support, self-management skills, adherence to self-monitoring of blood glucose (SMBG) and haemoglobin A1c (HbA1c) measurement were tested by questionnaire. Correlation analysis and path analysis were performed so as to identify the factors associated with patients’ SMB.
Results: A total of 532 participants completed this study. Participants who have good compliance to SMBG got higher scores in social support (F = 7.68, p = 0.01), competence (F = 10.47, p = 0.01), and skills (F = 12.34, p < 0.01). Higher competence (β = 0.03, P < 0.001), higher social support (β = 0.01, P < 0.001), better skills(β = 0.01, P < 0.001) directly led to better adherence to SMBG. Social support had a positive effect on autonomy support (β = 0.69, P < 0.001), motivation (β = 0.45, P < 0.001), competence (β = 0.28, P < 0.001), skills (β = 0.14, P < 0.001), which was also indirectly linked to better adherence to SMBG. Better self-management skills directly led to better adherence to HbA1c measurement (β = 0.03, P < 0.001). Social support had a positive effect on autonomy support (β = 0.69, P < 0.001), motivation (β = 0.45, P < 0.001), competence (β = 0.28, P < 0.001), skills (β = 0.14, P < 0.001), which was also indirectly linked to better adherence to HbA1c measurement.
Conclusion: Self-determination theory and social support theory were practical in explaining SMB in Chinese population. Competence, motivation and social support played an important role in diabetic self-management. Paying attention to the promotion of individual’s intrinsic motivation and self-efficacy may be able to help patients maintain self-management behavior in the long-term routine.
Keywords: self-determination theory, social support theory, self-monitoring of blood glucose, motivation, diabetes
Introduction
Diabetes have grown into a global epidemic and is affecting an increasing proportion of population worldwide. According to a national research conducted in China in 2010, the estimated prevalence of diabetes and pre-diabetes in adults was 11.6% and 50.1%.1
In diabetes treatment, self-management of diabetes is an effective way to minimize the risk of developing complications and improve their quality of life. Self-management behaviors (SMB) includes taking medications regularly, following a healthy diet, being physical active, foot care, smoking cessation and self-monitoring of blood glucose (SMBG) and hemoglobin A1c (HbA1c).2 According to previous researches, SMBG and HbA1c measurement are crucial SMB and could effectively assist patients in controlling blood glucose levels.3,4 For example, Bartolo et al found that increasing the number of SMBG tests from 1 to 2 per day was associated with HbA1c reduction in young adult patients.5 Besides, previous research showed that SMBG could reduce the incidence and progression of micro-vascular disease in both type 1 (T1D) and 2 diabetes (T2D).6 Patients with regular SMBG also reported a better quality of life.7,8 Furthermore, persons with type 2 diabetes and type 1 diabetes also require regular measurement of HbA1c.9 Therefore, SMBG and HbA1c measurement play a significant role in glycemic control and routine care for diabetic patients.
Despite the health benefits associated with SMB, many diabetics only perform it at a frequency lower than that suggested by health care providers.10 In a Chinese study, only 18.98% respondents performed SMBG at the recommended frequency, and 35.36% reported never performing SMBG.11 It is well recognized that non-adherence to SMBG and HbA1c measurement is a multifaceted problem. Previous studies identified several barriers including demographic,2 objective factors (such as lack of health education, insulin treatment, infrequent hospitalization, lack of blood glucose meter), and subjective factors (like low self-efficacy, decreased social support).12–14 Subjective factors were believed to be one of the critically dimensions of diabetic intervention strategies. For example, Patton et al conducted a review and found that health education, problem solving, contingency management, goal setting were useful interventions in improving patients’ short-term adherence to SMBG.15 Hortensius et al believed that it was useful to make patients understand both the positive and the potentially negative aspects of SMBG, thereby enhancing positive perceptions of SMBG.16 A meta-analysis also showed that stronger perceptions of personal control over diabetes showed a significant correlation with lower HbA1c levels.17 Perceptions that individuals had of the importance of those behaviors and the confidence they had seemed to play a substantial role in performing SMB.
In order to assess the determinants of diabetes self-management, De Man et al18 developed a SMART2D model (a person-centred approach to Self-Management And Reciprocal learning for the prevention and management of Type 2 Diabetes), which integrated behavioral change theories with chronic care models, health systems theory, and the influence of the environment. According to this model, self-management behavior requires self-management skills, and is facilitated by the five mediators, including perceived autonomy, perceived relatedness, and self-efficacy. These mediators are identified by Ryan and Deci’s self-determination theory (SDT),19 and they are three basic psychological needs that foster motivation and engagement for the adoption of healthy behavior. With autonomous motivation, patients would perceive themselves to be the initiator of their behavior change; their health-related behaviors were more likely to be internalized; and thus, behavior changes would be better maintained.20 SDT proposed a promising explanatory framework to predict self-regulated behavior which had been shown to be particularly relevant for SMBG. Researches based on SDT has highlighted the role that psychological factors play in determining health outcomes. A cohort study reported that patients who received autonomy supportive by health care providers felt more able to regulate their glucose, and showed improvements in their HbA1c levels.21 According to a systematic literature review, health-related interventions based on SDT are assumed to be effective in different contexts and countries.22
According to SMART2D model, the individual with T2D is also closely connected to their family and friends. In previous studies, social support has long been acknowledged as a necessary and an important part of ongoing diabetes care.23 Social support from relatives, friends, colleagues, partners and other social people promoted self-management practices among patients in a variety of ways, such as subjective support and objective support.24 Objective support includes direct assistance materially from social network of stable social connections (ie, family, friends, colleagues) and unstable connections (ie, informal support groups), while subjective support refers to the emotional and subjective experience of being supported, and understood. Due to the relevance of this issue, social support theory (SST) was employed in this study. Accordingly, social support mainly emphasizes the promoting effect of external support on individuals, and it refers to relationships that can be categorized into four different groups: emotional support, which means the availability of someone to rely on and trust in when needed; instrumental support, indicating real financial assistance from others; informational support, defined as obtaining essential information through social interactions with others; and appraisal support, which means feedback provided by others on how to act.25 For diabetics, social support provided by peers, families and professionals could provide emotional support, stimulate their behavioral motivation and improve their self-efficacy to keep self-monitoring of blood glucose. For example, a study found that directive support, which means that supporter guided the patients to complete the goal and were responsible for the daily task arrangement, had positive correlation with better self-management behaviors.26 Koetsenruijter et al found that extensive informational networks (exchanging information related to dealing with someone’s illness), emotional networks (talking about health problems or other personal issues), and attendance of community organizations were linked to better self-management capabilities in diabetes patients, especially strong in the low education group.27 Charlotte found an intensive support group and simultaneously involving significant others might improve diabetes self-management behavior.28 Besides, the importance of family support as an enabler to improve medication adherence and blood glucose testing in people with diabetes was reported.29
Although many studies explored the influencing factors of self-management behavior towards diabetes, few studies focused on the patients’ self-monitoring of blood glucose and HbA1c in China. Thus, this paper extends prior research along two dimensions. First, to our best knowledge, this is the first research that applied SDT and SST, western-developed theories, in examining SMBG behaviors among patients with type 2 diabetes in mainland China, which also provides new evidence supporting the utility of behavioral theories developed in the west to promote diabetic intervention strategies in China and other Asian countries. Second, we identify the influential factors in blood glycemic control and explore how these factors interact with each other, which has significant implications for better performing preventative strategies.
According to the SMART2D model, SST and SDT, we proposed the theoretical framework (Figure 1) and following hypotheses:
H1: Autonomy support, motivation and competence was positively associated with the adherence to SMBG and HbA1c measurement among patients with T2D. H2: Higher social support had a positive effect on adherence to SMBG and HbA1c measurement. H3: SMGB skills were positively associated with patients’ adherence to SMBG and HbA1c measurement.
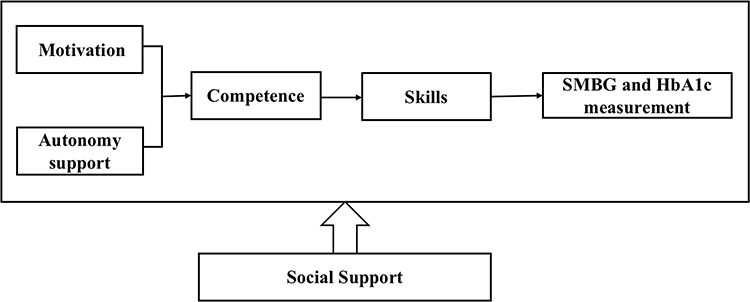 |
Figure 1 Theoretical framework of factors related to the SMB of diabetes. |
Methods
Study Design and Participants
This was a cross-sectional study conducted from April to May in 2017 by The School of Public Health, Peking University. Eighteen community healthcare stations (CHSs) from six community healthcare centers (CHCs), Beijing, China were chosen. Chinese CHCs are set up according to subdistrict boundaries, and each CHC has several CHSs to provide healthcare service for the neighborhood residents. Participants who met the following criteria were recruited: (1) aged between 18 and 75 years old; (2) diagnosed with type 2 diabetes by CHCs since at least 3 months; (3) agreed to participate in the survey. Exclusion criteria were as follows: (1) dementia or mental disorders; (2) other types of diabetes patients; (3) patients with severe heart, brain, kidney, eye, foot and nervous system complications.
Procedures
Data were collected using verified scales and self-designed questionnaire. The questionnaire was designed to ascertain the participants’ motivation, competence, relatedness, social support, diabetic skills and self-monitoring behavior. We invited professors from the School of Public Health of Peking University to attend the expert conference to improve the quality of the questionnaire. Before the formal survey, we carried out a preliminary survey of 50 people in a CHC of Beijing to test the reliability and validity of the questionnaire. Questionnaire surveys were carried out at CHCs.
Recruitment was conducted by community doctors from April to May 2017. Recruitment commenced with posters at community public places and was followed by telephone recruitment based on the patients’ health-care record. All the participants in each health-care station were invited to an information meeting, and the details of this study were delivered, including research purpose, research content, intervention methods, benefits and risks of participating in the study. The investigators were graduate students of the School of Public Health, Peking University. Before the investigation, unified training was carried out for the investigators.
The survey took for approximately 15–20 minutes for each participant to complete. A total of 532 valid questionnaires were received.
Main Measurements
A Health Care Climate Questionnaire (HCCQ) developed by Williams30 was used to measure the autonomy support. Participants were asked to respond a 5-point Likert scale ranging from “strongly disagree” to “strongly agree”. It has been widely used in previous researches, such as exercises31 and glucose control,32 which shows a good validity. HCCQ includes six items: “Doctors provide me with my choices about SMB”, “Doctors understand how I feel about SMB of diabetes”; “Doctors give me confidence, and make me believe that I am able to perform SMB”; “Doctors listen to how I would like to do SMB”; “Doctors encourage me to ask questions about SMB”; “After understanding my views on SMB of diabetes, Doctors will give me some suggestions”.
Autonomous and controlled motivation towards SMB were assessed through the Treatment Self-Regulation Questionnaire (TSRQ), which focuses on why patients adopted certain healthy behaviors. Based on SDT, the motivation of SMB was measured with the question “What is the reason for your SMBG and HbA1c measurement?”, and 8 items that the respondents could select. Four of them were used to measure autonomous motivation, such as “I personally believe it is the best thing for my health”; and another four were used to measure controlled motivation, like “others would be upset with me if I did not”. Each item was a 7-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree).
Self-efficacy was initially defined by Bandura as “people’s beliefs about their capabilities to produce designated levels of performance that exercise influence over events that affect their lives”. In SDT, the term competence was used, but the concept corresponds to Bandura’s self-efficacy. Hence, self-efficacy for diabetes scale (SED)33 developed by Hauser was used in this study. The participants were asked 4 questions focused on self-management performance, including “I usually have the ability to measure blood glucose or urine glucose as instructed”, “When I’m away, I’m still able to measure my blood glucose or urine glucose as usual”, “When I’m not feeling well, I will check my blood glucose or urine glucose more often than usual”, and “I have the ability to record the results of every blood glucose or urine glucose test”. Each item was ranging from 1 (“Can’t do it at all”) to 10 (“I can do it”).
Social support for diabetic patients includes family support, peer support and professional support. Family Support Scale was designed based on Schafer’s family member behavior scale of diabetic patients.34 Using a 5-point Likert scale (from “never” to “always”), participants were asked about four items: “Did your family members complain about you during SMB?”, “Would your family members help you decide what to do based on the test result of blood glucose?”, “Would your family criticize you if you failed to do SMB?”, “Would your family help you with your SMB?”. Peer support mainly came from other patients, and was measure by two items: “In the past three months, have you exchanged relevant experiences with other patients with diabetes?”, and “In the past three months, have you helped other patients with diabetes?”. Professional support was measured by four questions: “In the past three months, have your doctors discussed diabetes treatment with you?”, “In the past three months, have your doctors carefully listened to your description of your health condition?”, “In the past three months, have your doctors told you the results of the blood glucose test in understandable way?”, “Did doctors play an important role in your SMB?”. The total social support score was the sum of all items.
The scale used to assess the participants’ diabetic skills includes three questions, “Can you measure your blood glucose with a glucometer?”, “When do you need to test your blood glucose”, and “Will you adjust your exercise and diet plan based on the blood glucose level?”. A 5-point Likert-type scale ranges from 1 (“Not completely”) to 5 (“Very skilled”).
SMB refers to SMBG and HbA1c measurement in our study. Participants were asked the following questions, “In the past 6 months, have you measured your blood glucose as often as required by your doctor?”, and “Will you follow the doctor’s guidance and measure HbA1c every 3–6 months?”. A 5-point Likert-type scale ranging from 1 (Never) to 5 (Always) was used. If the answer was “4=usually” and “5=always”, it would be considered to be a patient with good SMB.
Data Analysis
Firstly, descriptive analysis was used to describe and compare characteristics of participants among different groups. Categorical variables were presented as proportions and were compared with Pearson χ2 test. In order to explore the factors influencing SMB, t-test was used to compare the mean score of variables.
Secondly, Pearson’s correlation coefficients were used to assess correlations among SDT constructs, social support, diabetic skills and SMBG. Spearman correlations were used to examine the bivariate relationship of SMBG, HbA1c measurement, sex and perceived health. The variables to the correlation models were chosen on theoretical and statistical basis. Cronbach’s alpha coefficient was used to assess the reliability of the individual SDT constructs, social support and diabetic skills. A Cronbach’s alpha coefficient >0.7 indicated good internal consistency.35
Thirdly, path analysis was performed to test the hypotheses. Only variables that were statistically significant in the correlation analysis were selected to the path analysis. Model’s goodness of fit was determined by several indices, including comparative fit index (CFI), Tucker-Lewis index (TLI), incremental fit index (IFI), and root mean square error of approximation (RMSEA) with a 90% confidence interval. Acceptable model fit was defined by the following thresholds: RMSEA (≤0.05), CFI, IFI and TLI (≥0.95).35
Data management and analysis were performed using SPSS 24.0 and AMOS 24.0.
Results
Basic Participant Characteristics
Demographic characteristics of the sample are presented in Table 1. 532 participants completed this study, and 64.7% were female. Most of the respondents were elderly, and the average age was 64.56 ± 8.56 years. Almost half (47.9%) did not obtain an upper secondary or higher degree in education. 81.2% were married, and 68.3% patients were overweight or obesity. The average duration of diabetes was 10.61 (SD ± 8.12) years.
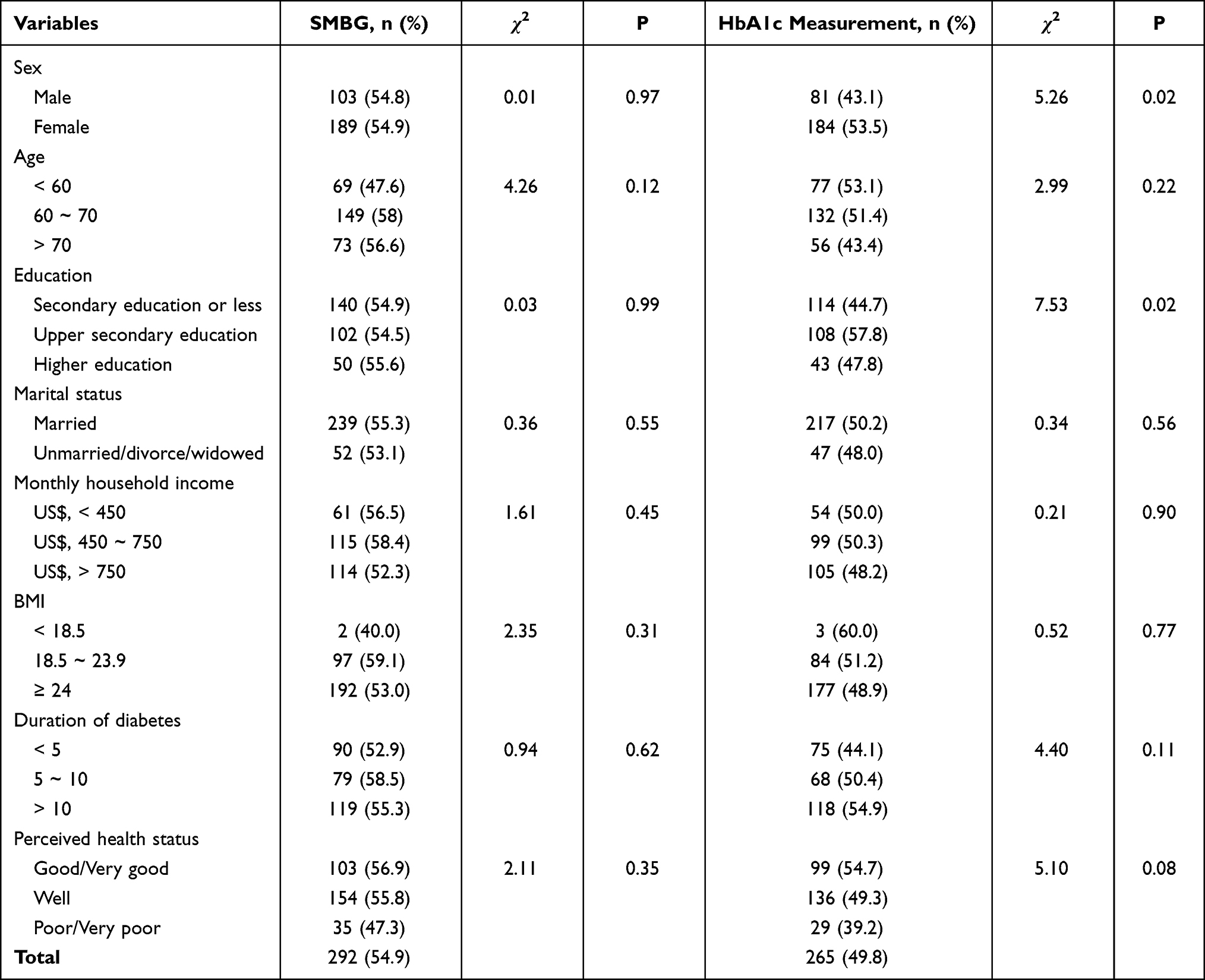 |
Table 1 Demographic Characteristics of the Sample |
There were no statistically differences of SMBG in different gender, age, education level, marital status, income level, BMI, duration of diabetes and perceived health status. However, gender, education level and perceived health status were found significantly different in HbA1c measurement among patients with T2D. Participants who were female (53.5%), with upper secondary education (57.8%) and with good/very good perceived health status (54.7%) reported better HbA1c measurement, which showed statistical significance.
Factors Influencing Participants’ SMB
Participants who had a good performance in SMB got higher scores in terms of social support, autonomy support, motivation, competence and diabetic skill. As shown in Figure 2, participants who have good SMBG adherence got higher scores in social support (F=7.68, p=0.01), competence (F=10.47, p=0.01), and skills (F=12.34, p<0.01). And participants who follow a regular HbA1c measurement got higher scores in autonomy support (F=4.44, p=0.04), competence (F=9.17, p=0.01), and skills (F=10.77, p<0.01) (Figure 3).
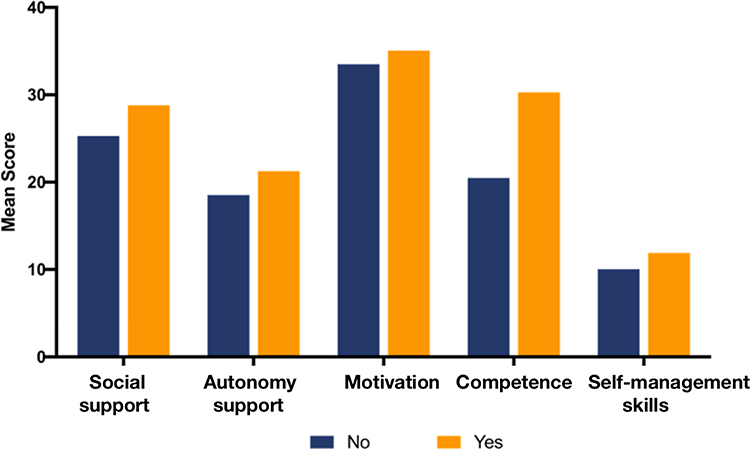 |
Figure 2 Factors influencing participants’ SMBG. |
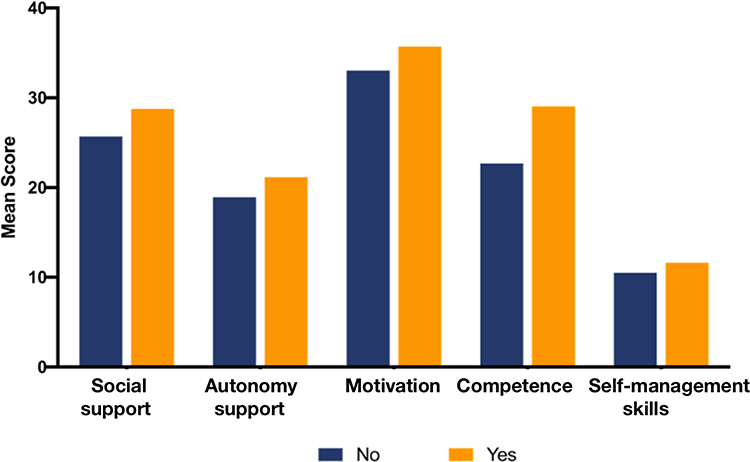 |
Figure 3 Factors influencing participants’ HbA1c measurement. |
Association Between the SDT Constructs, Social Support, Self-Management Skills and SMB
The mean scores, Cronbach’s alpha coefficients are shown in Table 2. The Cronbach’s alpha coefficients of the HCCQ scale, TSRQ scale, PCDS scale, Social support scale and self-management skills scale ranged from 0.72 to 0.93, which showed good internal consistency.
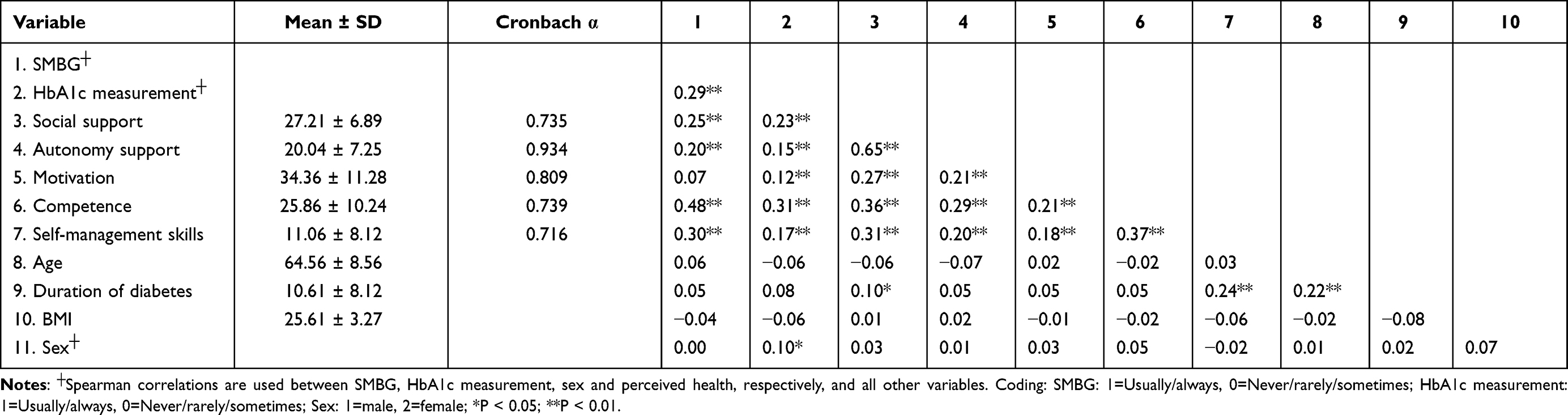 |
Table 2 Correlations Matrix Between Variables |
Table 2 presents bivariate correlations between observed variables and outcome variables. The model was tested as it was hypothesized in the introduction. SMBG was significantly associated with higher social support (β = 0.25, P < 0.01), autonomy support (β = 0.20, P < 0.01), competence (β = 0.48, P < 0.01), and self-management skills (β = 0.30, P < 0.01). HbA1c measurement was significantly associated with higher social support (β = 0.23, P < 0.01), autonomy support (β = 0.15, P < 0.01), motivation (β = 0.12, P < 0.01), competence (β = 0.31, P < 0.01), and self-management skill (β = 0.17, P < 0.01).
Testing the Path Analysis Model
Based on the hypotheses in the introduction, we built two model to explore the influencing factors of SMBG and HbA1c measurement. After conducting SEM several times, final models that satisfied fit indices were identified. The standardized regression coefficients of the model are illustrated in Figures 4 and 5. The path model of SMBG had acceptable fit indices, which were χ2 (df = 5; N = 532) = 7.653, P = 0.176; χ2/df = 1.531; CFI = 0.996; IFI = 0.996; TLI = 0.988; RMSEA = 0.032 < 0.05, indicating a good-fitting model. Higher competence directly led to better adherence to SMBG (β = 0.03, P < 0.001); social support had direct positive effect on adherence to SMBG (β = 0.01, P < 0.001); better self-management skills directly led to better adherence to SMBG (β = 0.01, P < 0.001). Higher motivation was indirectly linked to better adherence to SMBG through competence (P < 0.01); social support had a positive effect on autonomy support (β = 0.69, P < 0.001), motivation (β = 0.45, P < 0.001), competence (β = 0.28, P < 0.001), skills (β = 0.14, P < 0.001), which was also indirectly linked to better adherence to SMBG.
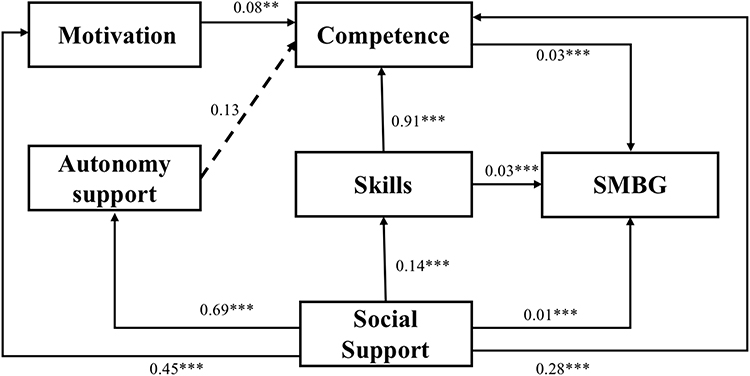 |
Figure 4 Path model with standardized parameter estimates between SMBG and related factors. **P < 0.01; ***P < 0.001. |
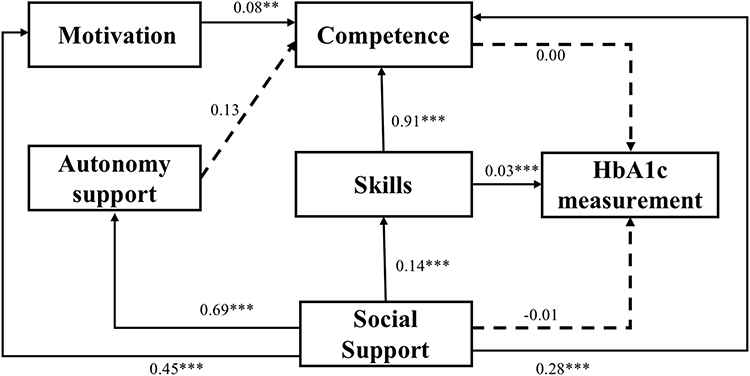 |
Figure 5 Path model with standardized parameter estimates between HbA1c measurement and related factors. **P < 0.01; ***P < 0.001. |
In the path model of HbA1c measurement, χ2 (df = 5; N = 532) = 8.131, P = 0.149; χ2/df = 1.626; CFI = 0.994; IFI = 0.994; TLI = 0.975; RMSEA = 0.034< 0.05, suggesting a good fit to data. Better self-management skills directly led to better adherence to HbA1c measurement (β = 0.03, P < 0.001). Social support had a positive effect on autonomy support (β = 0.69, P < 0.001), motivation (β = 0.45, P < 0.001), competence (β = 0.28, P < 0.001), skills (β = 0.14, P < 0.001), which was also indirectly linked to better adherence to HbA1c measurement.
Discussion
This study focused on SMB among patients with T2D, which provides evidence from a more general perspective. Based on SDT and SST, this study used Chinese data to provide a comprehensive picture of the possible factors related to SMB and how these influencing factors interacted with each other.
As hypothesis 1, autonomy support, motivation and competence were positively associated with the adherence to SMB. According to SDT, human motivation can be classified as autonomous or controlled. Autonomous motivation indicates identified regulation, integrated regulation and intrinsic motivation. For example, people exercise regularly because it is perceived as personally important, and coherent with one’s values. By contrast, controlled motivation refers to introjected regulation and external regulation. For example, people have to do self-management activities because of external pressure or rewards.36 In this study, the increase of personal motivation led to the higher competence in patients with T2D, which ultimately improve patients’ SMB. This finding was consistent with previous research. A literature review indicated that motivation was an underlying determinant of lifestyle behaviors for all people with diabetes.37 In SDT model, not only the motivation that was important, but also the type of motivation. Pfoh et al found that the most common reason for SMBG was the request from doctor, which turned out to be a controlled motivation. However, patients who “feel more in control of my diabetes”, “want to avoid damaging my body”, and “want to understand my diabetes better” were more likely to continue to monitor their blood sugar.38
In this study, higher competence was directly led to better adherence to SMBG, while it shows no direct effect on HbA1c measurement adherence. A cross-sectional study found that glycemic control was strongly associated with perceived competence in diabetes care,39 which was consistent with our study. We also observed indirect link between competence and SMB. Koponen et al also reported that the effect of autonomous motivation on glycemic control was mediated by perceived competence.39. Cho et al found that self-efficacy for SMB for diabetic patients was positively correlated with patients’ quality of life and their acceptance and action.40 This supports the idea that self-efficacy was an important factor affecting health behaviors for patients.
However, the association between autonomy support and other factors was not significant in path analysis. A possible explanation for this might be that family members and peers were the main supporters for patients with T2D in long-term self-care while support from medical staff was limited. There lied some debates about whether autonomy support was useful in healthy lifestyle maintenance. A previous study found that patients felt supported when the doctors make their blood glucose control plans based on their health conditions.41 Data from Weigensberg et al strongly suggested that autonomy support was increased in the group of self-management participants.42 However, another study showed that autonomy support had no statistical significance in dietary self-management among patients with T2D, because the effect of autonomy support was mediated by autonomous motivation and self-care competence.43
Hypothesis 2 was supported. Social support had both direct and indirect effect on better adherence to SMBG and HbA1c measurement. Moreover, social support showed great positive effect on autonomy support, motivation, competence and self-management skills, which indicates that social support plays an important role in the self-management intervention of diabetic patients. Prior studies have noted that the involvement of families and spouses could be beneficial or detrimental. On the one hand, high warmth and autonomy support from family and peers would be helpful for patients to maintain self-management behaviors. On the other hand, behaviors with features of hostility (or low warmth) and control (eg, criticism, undermining, nagging) was harmful44.
Hypothesis 3 was supported. Better self-management skills directly led to better SMBG and HbA1c measurement adherence. Thomas et al indicated that coping skills will positively impact diabetes self-care.45 A systematic review found that skills were one of the most frequently reported facilitators of diabetes self-management.46 These findings were consistent with our results.
Additionally, to our best knowledge, this is the first research that applied SDT and SST, western-developed theories, in examining SMB among patients with type 2 diabetes in mainland China, and we explored the intrinsic pathways of patients in blood glycemic control, and identify the association between inner influential factors, which has significant implications in better performing preventative strategies.
Our study also has several limitations. First, we only used cross-sectional data for this estimation. As a result, causal relationship could not be inferred. Second, the patients recruited in this study were all voluntarily enrolled. It was a form of self-selection rather than random selection, thus there may be a volunteer bias, affecting the representativeness of the research. However, as the participants were recruited from different administrative districts of Peking, it is believed that the overall findings were meaningful.
Conclusion
SDT and SST were practical in explaining SMB among patients with T2D in China. Higher competence, higher social support and better self-management skills directly led to better adherence to SMBG, while better self-management skills directly led to better adherence to HbA1c measurement. Social support, autonomy support, motivation and competence were found indirectly linked to better adherence to SMBG and HbA1c measurement. Findings from this study may be useful in guiding the development of future blood glucose control programs. In diabetic intervention strategies, paying attention to the promotion of individual’s autonomy and control motivation and competence may be able to help patients maintain SMB in the long-term routine. Besides, social support from family, peers and professionals may have important implications in SMB for patients with T2D.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved from the Institutional Review Board of Peking University Health Science Center (Ethical approval number: IRB00001052-17017). After a brief description of the study’s purpose, risk, and benefits, participants signed informed consent form. Confidentiality during all phases of research activities was kept. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors thank the staff from the Center for Disease Control and Prevention in Chaoyang and Dongcheng Districts, Beijing, China, who gave a lot of support in the implementation of this research. The authors also thank the patients and their families who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Xu Y, Wang L, He J, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310(9):948–959. doi:10.1001/jama.2013.168118
2. Alyami M, Serlachius A, Mokhtar I, Broadbent E. Illness perceptions, HbA1c, and adherence in type 2 diabetes in Saudi Arabia. Patient Prefer Adherence. 2019;13:1839–1850. doi:10.2147/PPA.S228670
3. Kosar L, Alsabbagh W, Lu X, et al. Trends in blood glucose test strip utilization: a population-wide analysis in Saskatchewan, Canada. Can J Diabetes. 2018;42(1):5–10. doi:10.1016/j.jcjd.2017.01.004
4. Xu Y, Lim JH, Henry R, Lee YJ. The impact of provision of self-monitoring of blood glucose supplies on self-care activities among patients with uncontrolled type 2 diabetes mellitus: a prospective study. Diabetes Res Clin Pract. 2019;157:107873. doi:10.1016/j.diabres.2019.107873
5. Di Bartolo P, Nicolucci A, Cherubini V, Iafusco D, Scardapane M, Rossi MC. Young patients with type 1 diabetes poorly controlled and poorly compliant with self-monitoring of blood glucose: can technology help? Results of the i-NewTrend randomized clinical trial. Acta Diabetol. 2017;54(4):393–402. doi:10.1007/s00592-017-0963-4
6. Saudek CD, Derr RL, Kalyani RR. Assessing glycemia in diabetes using self-monitoring blood glucose and hemoglobin A1c. JAMA. 2006;295(14):1688–1697. doi:10.1001/jama.295.14.16887
7. Gilden JL, Casia C, Hendryx M, Singh SP. Effects of self-monitoring of blood glucose on quality of life in elderly diabetic patients. J Am Geriatr Soc. 1990;38(5):511–515. doi:10.1111/j.15325415.1990.tb02399.x
8. Mohan V, Mapari JA, Karnad PD, Mann JS, Maheshwari VK. Reduced diabetes mellitus-related comorbidities by regular self-monitoring of blood glucose: economic and quality of life implications. Indian J Endocrinol Metab. 2018;22(4):461–465. doi:10.4103/ijem.IJEM_216_1724
9. Carmienke S, Fink A, Baumert J, et al. Participation in structured diabetes self-management education programs and its associations with self-management behaviour - a nationwide population-based study. Patient Educ Couns. 2021. doi:10.1016/j.pec.2021.07.017
10. Chen CM, Chang Yeh M. The experiences of diabetics on self-monitoring of blood glucose: a qualitative metasynthesis. J Clin Nurs. 2015;24(5–6):614–626. doi:10.1111/jocn.12691
11. Yuan L, Guo X, Xiong Z, et al. Self-monitoring of blood glucose in type 2 diabetic patients in China: current status and influential factors. Chin Med J. 2014;127(2):201–207.
12. Ugwu ET, Orjioke CJG, Young EE. Self monitoring of blood glucose among patients with type 2 diabetes mellitus in Eastern Nigeria: need for multi-strategic interventions. Curr Diabetes Rev. 2018;14(2):175–181. doi:10.2174/1573399812666161014111618
13. Mostrom P, Ahlen E, Imberg H, Hansson PO, Lind M. Adherence of self-monitoring of blood glucose in persons with type 1 diabetes in Sweden. BMJ Open Diabetes Res Care. 2017;5(1):e000342. doi:10.1136/bmjdrc-2016-000342
14. Fisher WA, Kohut T, Schachner H, Stenger P. Understanding self-monitoring of blood glucose among individuals with type 1 and type 2 diabetes: an information-motivation-behavioral skills analysis. Diabetes Educ. 2011;37(1):85–94. doi:10.1177/0145721710391479
15. Patton SR. Adherence to glycemic monitoring in diabetes. J Diabetes Sci Technol. 2015;9(3):668–675. doi:10.1177/1932296814567709
16. Hortensius J, Kars MC, Wierenga WS, Kleefstra N, Bilo HJ, van der Bijl JJ. Perspectives of patients with type 1 or insulin-treated type 2 diabetes on self-monitoring of blood glucose: a qualitative study. BMC Public Health. 2012;12:167. doi:10.1186/1471-2458-12-167
17. Mc Sharry J, Moss-Morris R, Kendrick T. Illness perceptions and glycaemic control in diabetes: a systematic review with meta-analysis. Diabet Med. 2011;28(11):1300–1310. doi:10.1111/j.1464-5491.2011.03298.x25
18. De Man J, Aweko J, Daivadanam M, et al. Diabetes self-management in three different income settings: cross-learning of barriers and opportunities. PLoS One. 2019;14(3):e0213530. doi:10.1371/journal.pone.0213530
19. Ng JY, Ntoumanis N, Thøgersen-Ntoumani C, et al. Self-determination theory applied to health contexts: a meta-analysis. Perspect Psychol Sci. 2012;7(4):325–340. doi:10.1177/1745691612447309
20. Yun Q, Ji Y, Liu S, et al. Can autonomy support have an effect on type 2 diabetes glycemic control? Results of a cluster randomized controlled trial. BMJ Open Diabetes Res Care. 2020;8(1):e001018. doi:10.1136/bmjdrc-2019-001018
21. Williams GC, Freedman ZR, Deci EL. Supporting autonomy to motivate patients with diabetes for glucose control. Diabetes Care. 1998;21(10):1644–1651. doi:10.2337/diacare.21.10.1644
22. Phillips AS, Guarnaccia CA. Self-determination theory and motivational interviewing interventions for type 2 diabetes prevention and treatment: a systematic review. J Health Psychol. 2020;25(1):44–66. doi:10.1177/1359105317737606
23. Vorderstrasse A, Lewinski A, Melkus GD, Johnson C. Social support for diabetes self-management via eHealth interventions. Curr Diab Rep. 2016;16(7):56. doi:10.1007/s11892-016-0756-0
24. Fortier MS, Sweet SN, Tulloch H, et al. Self-determination and exercise stages of change: results from the diabetes aerobic and resistance exercise trial. J Health Psychol. 2012;17(1):87–99. doi:10.1177/1359105311408948
25. Smith JC, Alderman L, Attell BK, et al. Dynamics of parental opioid use and children’s health and well-being: an integrative systems mapping approach. Front Psychol. 2021;12:687641. doi:10.3389/fpsyg.2021.687641
26. Zhang X-X, Wu S-Y, Feng-bin WANG, et al. [Association between social support and self-management behaviors among patients with diabetes in community]. Beijing Da Xue Xue Bao Yi Xue Ban. 2017;49(3):455–461. Chinese.
27. Koetsenruijter J, van Eikelenboom N, van Lieshout J, et al. Social support and self- management capabilities in diabetes patients: an international observational study. Patient Educ Couns. 2016;99(4):638–643. doi:10.1016/j.pec.2015.10.02926
28. Vissenberg C, Nierkens V, van Valkengoed I, et al. The impact of a social network based intervention on self-management behaviours among patients with type 2 diabetes living in socioeconomically deprived neighbourhoods: a mixed methods approach. Scand J Public Health. 2017;45(6):569–583. doi:10.1177/1403494817701565
29. Bukhsh A, Goh BH, Zimbudzi E, et al. Type 2 diabetes patients’ perspectives, experiences, and barriers toward diabetes-related self-care: a Qualitative Study From Pakistan. Front Endocrinol. 2020;11:534873. doi:10.3389/fendo.2020.534873
30. Williams GC, Rodin GC, Ryan RM, Grolnick WS, Deci EL. Autonomous regulation and long-term medication adherence in adult outpatients. Health Psychol. 1998;17(3):269–276. doi:10.1037//0278-6133.17.3.269
31. Fenton SAM, Veldhuijzen van Zanten JJ, Metsios GS, et al. Testing a self-determination theory-based process model of physical activity behavior change in rheumatoid arthritis: results of a randomized controlled trial. Transl Behav Med. 2021;11(2):369–380. doi:10.1093/tbm/ibaa02227
32. De Man J, Wouters E, Absetz P, et al. What motivates people with (pre)diabetes to move? Testing self-determination theory in Rural Uganda. Front Psychol. 2020;11:404. doi:10.3389/fpsyg.2020.00404
33. Grossman HY, Brink S, Hauser ST. Self-efficacy in adolescent girls and boys with insulin-dependent diabetes mellitus. Diabetes Care. 1987;10(3):324–329. doi:10.2337/diacare.10.3.324
34. Schafer LC, McCaul KD, Glasgow RE. Supportive and nonsupportive family behaviors: relationships to adherence and metabolic control in persons with type I diabetes. Diabetes Care. 1986;9(2):179–185. doi:10.2337/diacare.9.2.179
35. Thrul J, Stemmler M, Buhler A, Kuntsche E. Adolescents’ protection motivation and smoking behaviour. Health Educ Res. 2013;28(4):683–691. doi:10.1093/her/cyt062
36. Gourlan M, Trouilloud D, Boiche J. Motivational profiles for physical activity practice in adults with type 2 diabetes: a self-determination theory perspective. Behav Med. 2016;42(4):227–237. doi:10.1080/08964289.2014.1001810
37. Lakerveld J, Palmeira AL, van Duinkerken E, Whitelock V, Peyrot M, Nouwen A. Motivation: key to a healthy lifestyle in people with diabetes? Current and emerging knowledge and applications. Diabet Med. 2020;37(3):464–472. doi:10.1111/dme.14228
38. Pfoh ER, Linfield D, Speaker SL, et al. Patient perspectives on self-monitoring of blood glucose when not using insulin: a cross-sectional survey. J Gen Intern Med. 2021. doi:10.1007/s11606-021-07047-2
39. Koponen AM, Simonsen N, Laamanen R, Suominen S. Health-care climate, perceived self-care competence, and glycemic control among patients with type 2 diabetes in primary care. Health Psychol Open. 2015;2(1):2055102915579778. doi:10.1177/205510291557977828
40. Cho MK, Kim MY. What affects quality of life for people with type 1 diabetes?: a Cross-Sectional Observational Study. Int J Environ Res Public Health. 2021;18(14):7623. doi:10.3390/ijerph18147623
41. Chen CM, Hung LC, Chen YL, Yeh MC. Perspectives of patients with non-insulin-treated type 2 diabetes on self-monitoring of blood glucose: a qualitative study. J Clin Nurs. 2018;27(7–8):1673–1683. doi:10.1111/jocn.14227
42. Weigensberg MJ, Vigen C, Sequeira P, et al. Diabetes empowerment council: integrative pilot intervention for transitioning young adults with type 1 diabetes. Glob Adv Health Med. 2018;7:2164956118761808. doi:10.1177/2164956118761808
43. Koponen AM, Simonsen N, Suominen S. How to promote fruits, vegetables, and berries intake among patients with type 2 diabetes in primary care? A self-determination theory perspective. Health Psychol Open. 2019;6(1):2055102919854977. doi:10.1177/2055102919854977
44. Wiebe DJ, Helgeson V, Berg CA. The social context of managing diabetes across the life span. Am Psychol. 2016;71(7):526–538. doi:10.1037/a0040355
45. Thomas JJ, Moring J, Bowen A, Rings JA, Emerson T, Lindt A. The influence of stress and coping on diabetes self-care activities among college students. J Am Coll Health. 2021;1–6. doi:10.1080/07448481.2021.1928142
46. Alexandre K, Campbell J, Bugnon M, et al. Factors influencing diabetes self-management in adults: an umbrella review of systematic reviews. JBI Evid Synth. 2021;19(5):1003–1118. doi:10.11124/jbies-20-00020
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.