Back to Journals » Patient Preference and Adherence » Volume 18
Factors Predicting Obesity Prevention Behaviors Among Overweight Late Primary School Students in Nakhon Si Thammarat Province, Thailand
Authors Hludhla C, Kusol K, Eksirinimit T
Received 6 June 2024
Accepted for publication 5 October 2024
Published 11 October 2024 Volume 2024:18 Pages 2109—2121
DOI https://doi.org/10.2147/PPA.S472380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Chadaporn Hludhla,1 Kiatkamjorn Kusol,2 Thidarat Eksirinimit2
1School of Nursing, Graduated Master of Nursing Science Program in Community Nurse Practitioner, Walailak University, Nakhon Si Thammarat, Thailand; 2School of Nursing and the Excellence Center of Community Health Promotion, Walailak University, Nakhon Si Thammarat, Thailand
Correspondence: Kiatkamjorn Kusol, School of Nursing and the Excellence Center of Community Health Promotion, Walailak University, Nakhon Si Thammarat, Thailand, Tel +66-81-979-6565, Email [email protected]
Purpose: Obesity is a significant global public health issue affecting late primary school students’ health and learning processes. This research aimed to predict factors influencing the prevention behaviors of obesity among overweight 9 to 12-year-old students.
Samples and Methods: This cross-sectional predictive correlational study involved 216 overweight students in grades 4– 6 and used a multi-stage sampling method. Comprehensive questionnaires meticulously collected data on demographics, self-perception, and obesity prevention behaviors. The data were analyzed using descriptive statistics, chi-square, and binary logistic regression.
Results: The mean scores for self-perception of food consumption and physical activity were moderate (M = 19.13, S.D. = 5.68; M = 19.53, S.D. = 5.64, respectively). Similarly, obesity prevention behaviors were moderate (M = 42.90, S.D. = 8.48). The study identified factors significantly related to obesity prevention behaviors, including gender, grade point average (GPA), self-perception of food consumption and physical activity, daily allowance from family, and nutrition education (p < 0.05). Binary logistic regression confirmed that self-perception of food consumption (OR = 4.29; 95% CI: 1.72– 10.73) and physical activity (OR = 2.585; 95% CI: 1.02– 6.56), grade point averages (OR = 0.38; 95% CI: 0.18– 0.82), daily allowance received from family (OR = 0.402; 95% CI: 0.17– 0.94), nutrition education (OR = 0.352; 95% CI: 0.15– 0.84), and male (OR = 0.113; 95% CI: 0.02– 0.56) were significant predictors (p < 0.05), providing valuable insights into the factors influencing obesity prevention behaviors among overweight students.
Conclusion: Male students who have good GPAs, high self-efficacy in food consumption and physical activity, nutrition education, and adequate financial support were more likely to engage in obesity prevention behaviors. Thus, educators and healthcare professionals should focus on enhancing self-perception, providing comprehensive nutrition education, and offering additional support to female students with lower GPAs. These measures will help improve behavior adjustment and support obesity prevention efforts.
Keywords: overweight, obesity prevention behaviors, late primary school students
Graphical Abstract:

Introduction
The nutrition situation has currently shifted towards an increasing prevalence of obesity. The global population with obesity is estimated to be around 1 billion, with children aged 5–19 accounting for over 340 million, approximately 29%.1 The World Health Organization (WHO) estimates that approximately 167 million adults and children will suffer from health problems due to overweight and obesity in the year 2025 (World Health Organization.2 Therefore, a global target was established that children and adolescents should not experience increasing rates of overweight and obesity by 2025.2 Thailand is one of the countries attempting to reduce the number of obese children. The prevalence of overweight and obesity among Thai students aged 6–14 from 2017 to 2021 gradually increased to 11.1%, 11.7%, 13.6%, 12.5%, and 13.3%, respectively.3 There was a similar trend in the prevalence of overweight and obesity among children aged 6–14 in Nakhon Si Thammarat Province. Notably, the Nutrition Division, Department of Health, Ministry of Public Health, aims to keep the prevalence of overweight and obesity among Thai children aged 6–14 below 10% (Nutrition Division, Department of Health, Ministry of Public Health, 2022).3 The percentages in this province from 2019 to 2022 were higher than the national statistics and the Nutrition Division, Department of Health, and Ministry of Public Health indicator, which were at 15.3%, 14.0%, 13.4%, and 14.6%, respectively.4
Childhood obesity negatively impacts physical health, mental well-being, and learning. Regarding physical impact, school children are more likely to have sleep apnea, which can lead to low oxygen levels and high carbon dioxide levels, initiating brain arousal.5 This problem could result in slow breathing, reduced attention span, and potential for disruptive behaviors. This may also reduce physical activity due to difficulties climbing stairs.6,7 The likelihood of accumulating liver fat, type 2 diabetes, and cardiovascular diseases in adolescence and adulthood tends to increase among those who lack physical activity.8,9 The negative consequences are not limited to physical problems but also mental complications. Obese children are prone to lack self-esteem because they are often subject to bullying on body image. Consequently, they could develop stress and anxiety easily.10 Severe obesity is also a cause of delayed perception, thinking, memory, and intelligence in schoolchildren. They could experience daytime drowsiness, further impacting their ability to concentrate and resulting in poor academic performance.11
The primary cause of obesity among this particular group is eating behavior. Previous studies have found that primary school students had fair-level food consumption behaviors, mainly sweetened beverages and high-carbohydrate foods.7,12 Another essential cause is a lack of physical activity, as previous studies have indicated that primary school students tended to lack physical activities due to having high screen time.13 To reduce the number of obese schoolchildren, health professionals should promote healthy behaviors related to obesity prevention, mainly eating habits and physical activities. Meanwhile, schoolchildren must be encouraged to increase physical activity and nutritional skills to prevent obesity.10 Even though health professionals and school personnel attempt to promote these behaviors among schoolchildren, the number of those with obesity remains higher than expected due to resource, budget, and human resource constraints.13 Therefore, the potential solution should be to promote healthy behaviors to prevent obesity.
To develop potential solutions, health professionals must understand factors associated with healthy behaviors to prevent obesity in schoolchildren. These factors can be classified into two categories: personal and environmental factors. Individual characteristics, including gender, age, study performance, and self-perception, were associated with behaviors to prevent obesity in schoolchildren. The incidence of obesity in male schoolchildren was higher than in females.14 The ability to prevent obesity increases constantly with age.7,12 Students with higher academic performance were 3.64 times more health-conscious and better able to prevent obesity than those with lower academic performance.7 Self-perception was also positively associated with healthy and obesity-prevention behaviors in school-aged children.15,16 Moreover, overweight school-aged children who were able to manage their food expenses and make appropriate food choices were more likely to control their obesity. Environmental factors, including the amount of daily allowance received from family and nutrition education, also significantly prevented obesity among this target group. Support from families regarding the amount of money received from parents increased opportunities for students to purchase unnecessary foods, contributing to excessive weight gain.17 Moreover, receiving nutrition education from school personnel helped schoolchildren control their weight and nutritional status.18 Children who participated in the physical activity program were likelier to adopt healthy behaviors that prevent childhood obesity.19
Personal and environmental factors related to obesity prevention behaviors align well with Bandura’s concept of perceived self-efficacy, indicating a positive relationship between self-perception and healthy eating behaviors in schoolchildren and obesity prevention behaviors.15,16 According to the developmental stage of children, primary school students may demonstrate efforts to overcome their weaknesses in pursuit of success. Promoting self-awareness, therefore, could potentially reduce the incidence of obesity in this target group. However, according to the literature review, only a few studies have focused on the prevalence and factors related to overweight and obesity among primary school students.20 Most studies have examined knowledge and health literacy predictors in caregivers of young children, adolescents, and adults. Therefore, little is known about predictors of obesity prevention behaviors among overweight late primary school students, particularly regarding family and school support combined with self-perception.
Given the rising trend of obesity in schoolchildren and its negative multifaceted health impacts, it is imperative to explore factors predicting obesity prevention behaviors among overweight 9–12-year-old students as input for developing potential care solutions to address this problem. By investigating these comprehensive factors, the research findings will be valuable for establishing potential strategies to prevent obesity in overweight late primary school students at individual, family, school, and societal levels. Past research has mainly focused on obesity prevalence, the factor that causes overweight and obesity among primary school students.20 However, the study of factors predicting obesity prevention behavior covers factors within the individual; environmental factors and self-efficacy regarding diet and physical activity were less common. The age period is 9–12 years. They want to develop themselves, especially in terms of social, emotional, and mental transition from primary to secondary school. It is a connection that students will have to face. Promoting readiness for students helps reduce problems during the connection between generations.21 This study aimed to use Bandura’s Perceived Self-Efficacy Theory (1997)22 as a framework to explain how one’s belief in their abilities affects behavior change. This theory suggests that individuals’ confidence in their abilities can influence their problem-solving efforts and, ultimately, their success. Among overweight late primary school students, obesity prevention behaviors are influenced by personal and environmental factors. Students who believe in their ability to manage their food consumption, engage in physical activities, and receive nutrition education and support from family and school are likelier to exhibit positive obesity prevention behaviors.7,15
Materials and Methods
Study Design and Sample
This cross-sectional predictive correlational study focused on overweight students aged 9–12 years studying grades 4–6 in late primary school under the Nakhon Si Thammarat Provincial Primary Education Office. The sample size was determined by G*Power software by Logistic Regression with a one-tailed statistical significance test, effect size = 0.15, significance level = 0.05, power of 1-β = 0.95, and number of predictors. The initially calculated sample was 160; however, 35% of the minimum required samples were added to avoid potential sample loss. Thus, the total sample size was 216. Samples were chosen using the multi-stage sampling method and inclusion criteria.
The following criteria were used to include the participants in the study: 1) excess weight from two times but no more than three times the median weight-for-height in the standards for the growth of children aged 6–19 years in the Department of Health23 2) no history of chronic disease affecting hemoglobinopathy, kidney disease, heart disease, and diabetes; 3) ability to read and write; and 4) willingness to participate in the study after being fully informed, including signed consent and parental consent given.
Select and survey a sample of students from student health files. Randomize the sample according to the specified method and quantity. Then, height and weight were measured again using a weight scale provided by the researcher and calibrated before use. The data was then compared in a graph using the growth reference criteria for children aged 6–19 years, height according to age criteria. If the inclusion criteria were met, they were taken as a sample. The researchers conducted the study following the Declaration of Helsinki. All of the personal information was recorded and kept confidential.
Research Instrument
The research instrument used to collect data in this current study consisted of four questionnaires combined into a single set and the test all at once as follows:
The first questionnaire, which the researchers developed, comprised seven demographic items and seven items on nutritional and health status. The questions were multiple-choice and open-ended. Participants were asked to answer questions about their gender, age, educational level, grade point average, religion, and money allowance and received nutrition education. Participants were also assessed for their weight, height, nutritional status, chronic diseases, hospitalization history in the past six months, sleep problems, and sleep duration in a day.
The second and third questionnaires comprised seven items on self-perception of food consumption and seven items on physical activity for obesity prevention, adapted from the self-perception of food consumption and physical activity measurement for overweight adolescents by Chaboonruang (2014).24 The Likert scale used in these questionnaires included four levels ranging from “Lack of confidence” (1) to “Very confident” (4). Scores on these scales ranged from 7 to 28. The self-perception scores were divided into three levels to interpret the results. A score range of 21.00–28.00 meant a high self-perception level, while a score range of 14.00–20.99 and 07.00–13.99 indicated moderate and low self-perception, respectively.
The fourth questionnaire comprised 15 items on obesity prevention behaviors, which included 10 positive and five negative statement items. It was adapted from the obesity prevention behavior assessment for students aged 9–14, developed by the Health Promotion Division, Department of Health, Ministry of Public Health (2019).25 The questionnaire utilized a five-point Likert scale rating frequency of behavior practice in which scores ranged from 1 (never did it) to 5 (always did it 6–7 days per week). The total score ranged from 15 to 75 points. The researchers were applied to interpret obesity prevention behaviors into three levels. High-level behaviors were indicated by an average score that ranged from 55.00 to 75.00, moderate levels ranged from 35.00 to 54.99, and low levels ranged from 15.00 to 34.99.
Validity and Reliability
Five experts assessed the content validity of the research instrument. The Content Validity Index (CVI) for the self-perception of food consumption, self-perception of physical activity, and obesity prevention behaviors ranged from 0.94 to 1.00, indicating high content validity. The questionnaires were tested for reliability with a sample of thirty overweight late primary school students who were not studying in the selected schools. Cronbach’s alpha coefficients for the self-perception of food consumption, self-perception of physical activity, and obesity prevention behaviors were equal to 0.75, 0.78, and 0.82, respectively. These coefficients demonstrated satisfactory internal consistency for each instrument.
Statistical Analysis
Data were analyzed using SPSS software (Version 26) for Windows™ (IBM Corporation, New York, NY, USA). The authors verified the normal distribution of data before conducting the statistics. Statistics were used to analyze demographic data, self-perception of food consumption, self-perception of physical activity, and obesity prevention behaviors. It is descriptive statistics, including frequencies, percentages, means, and standard deviations, and it analyzes the association between factors and obesity prevention behaviors using chi-square. Then, the variables related to obesity prevention behaviors were analyzed using binary logistic regression statistics to find factors predicting obesity prevention behaviors among overweight late primary school students.
Results
Demographic Data of Samples
The participants were males (67.6%) and practiced Buddhism (90.9%). The mean age, weight, and height were ten years (S.D. = 0.88), 58.3 kilograms (S.D. = 10.31), and 148.6 centimeters (S.D. = 9.04), respectively. 51.4% of the samples were classified as getting obese. Most participants reported no chronic illnesses (83.8%), no sleep problems (84.7%), and no record of hospitalizations in the past six months (95.8%). The average daily sleep duration and food allowance received from families were 8.7 hours (S.D. = 1.12) and 46.27 baht (S.D. = 18.18), respectively. The grade point average was 3.41 (S.D. = 0.46). Almost two-thirds (62.5%) of the samples reported receiving nutrition education. At the same time, over eighty percent (88.4%) of the participants claimed to have participated in physical activities organized by the school for at least an hour a week (Table 1).
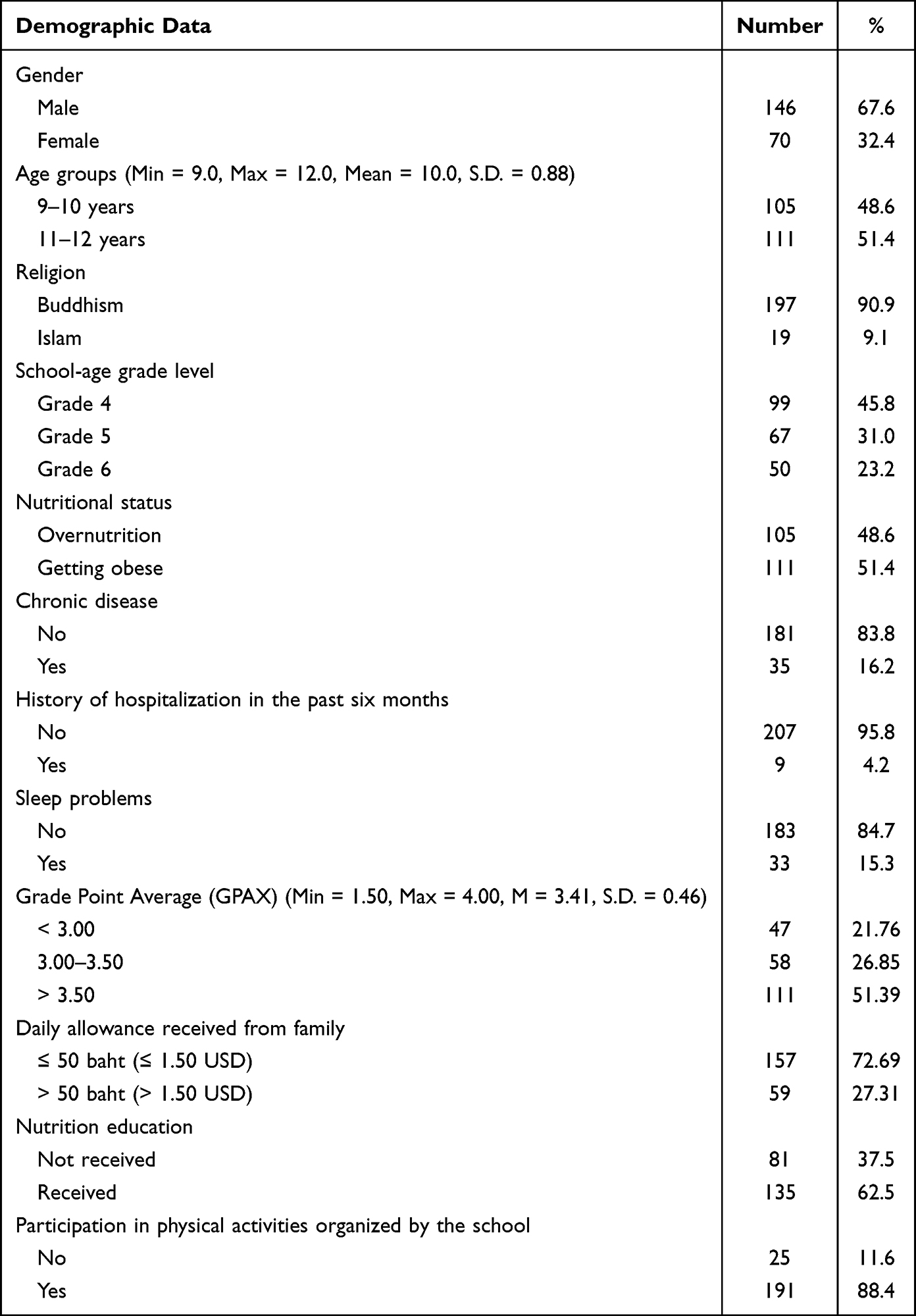 |
Table 1 Number and Percentage of the Samples’ Demographic Data (n = 216) |
Self-Perception of Food Consumption and Physical Activity
The participants reported their self-perception of food consumption at a moderate level (M = 2.89, S.D. = 0.47). Participants reported two food consumption items at high levels, including having three meals a day and having rice or starchy foods at six servings a day (Table 2). In terms of self-perception of physical activity, the participants reported their self-perception of physical activity at a moderate level (M = 2.86, S.D. = 0.58). Only one physical activity item was rated high: doing household chores for 30 minutes (Table 3).
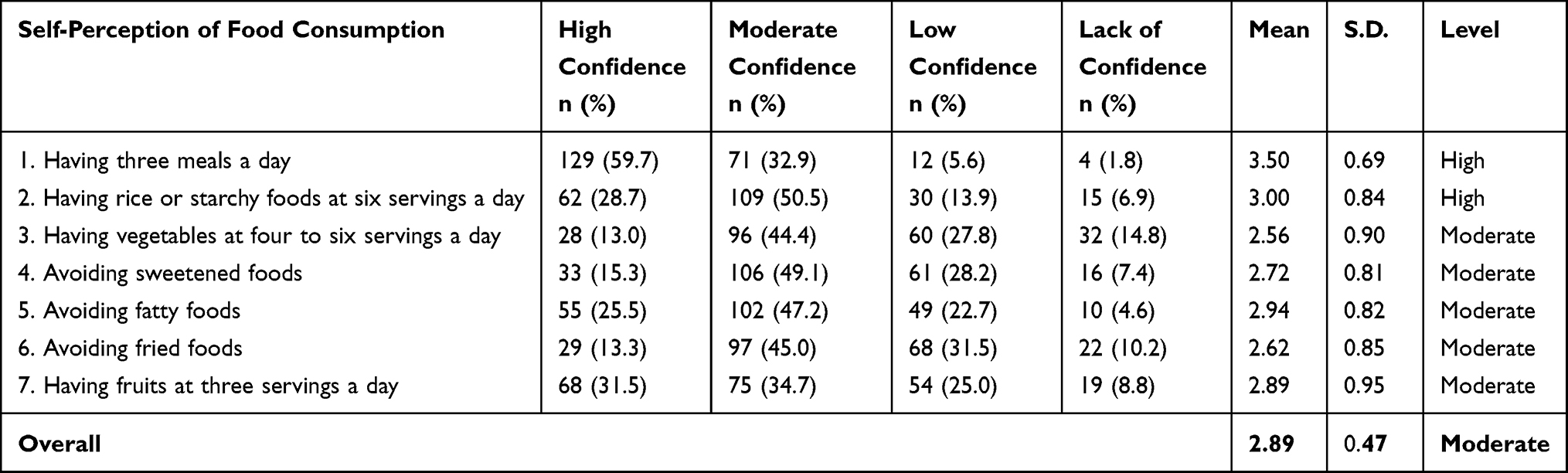 |
Table 2 Number, Percentage, and Mean of Self-Perception of Food Consumption (n = 216) |
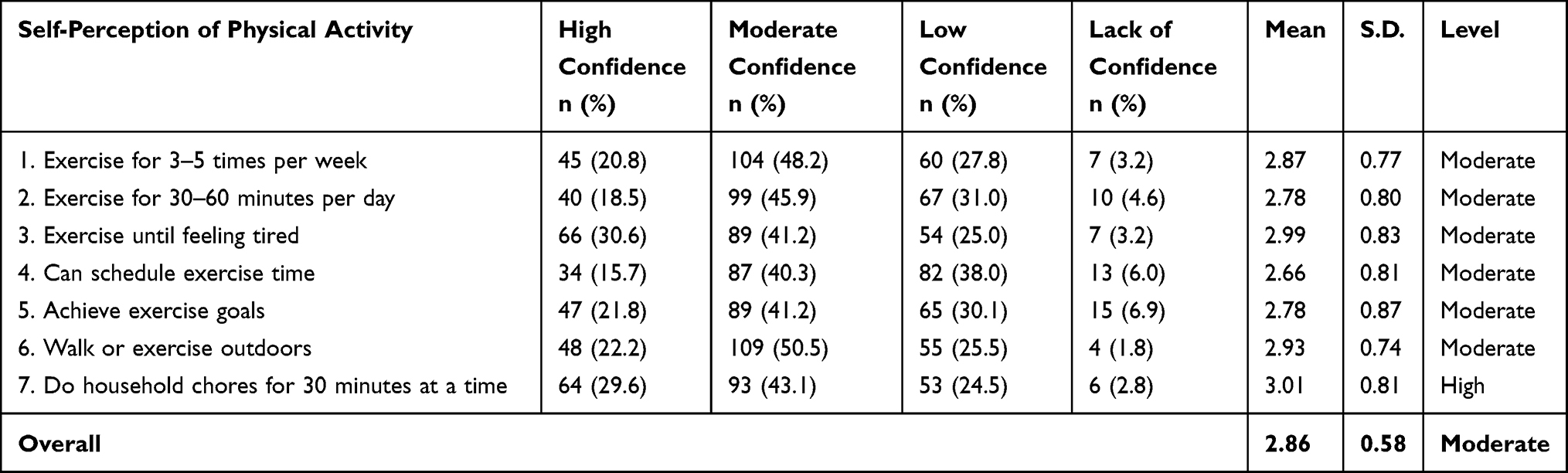 |
Table 3 Number, Percentage, and Mean of Self-Perception of Physical Activity (n = 216) |
Obesity Prevention Behaviors
The findings revealed that the participants demonstrated overall moderate levels of obesity prevention behaviors (M = 3.00, S.D. = 0.66). The top five highest mean scores for obesity prevention behaviors were as follows: 1) engaging in physical activities, 2) moving the body until sweating, 3) running or playing sports after school or on weekends, 4) reducing consumption of fried foods, fast foods, or dishes cooked with coconut milk, and 5) avoiding drinking carbonated beverages or sugary drinks. The behavior with the lowest mean score was reducing the addition of fish sauce or sugar to meals before eating (Table 4).
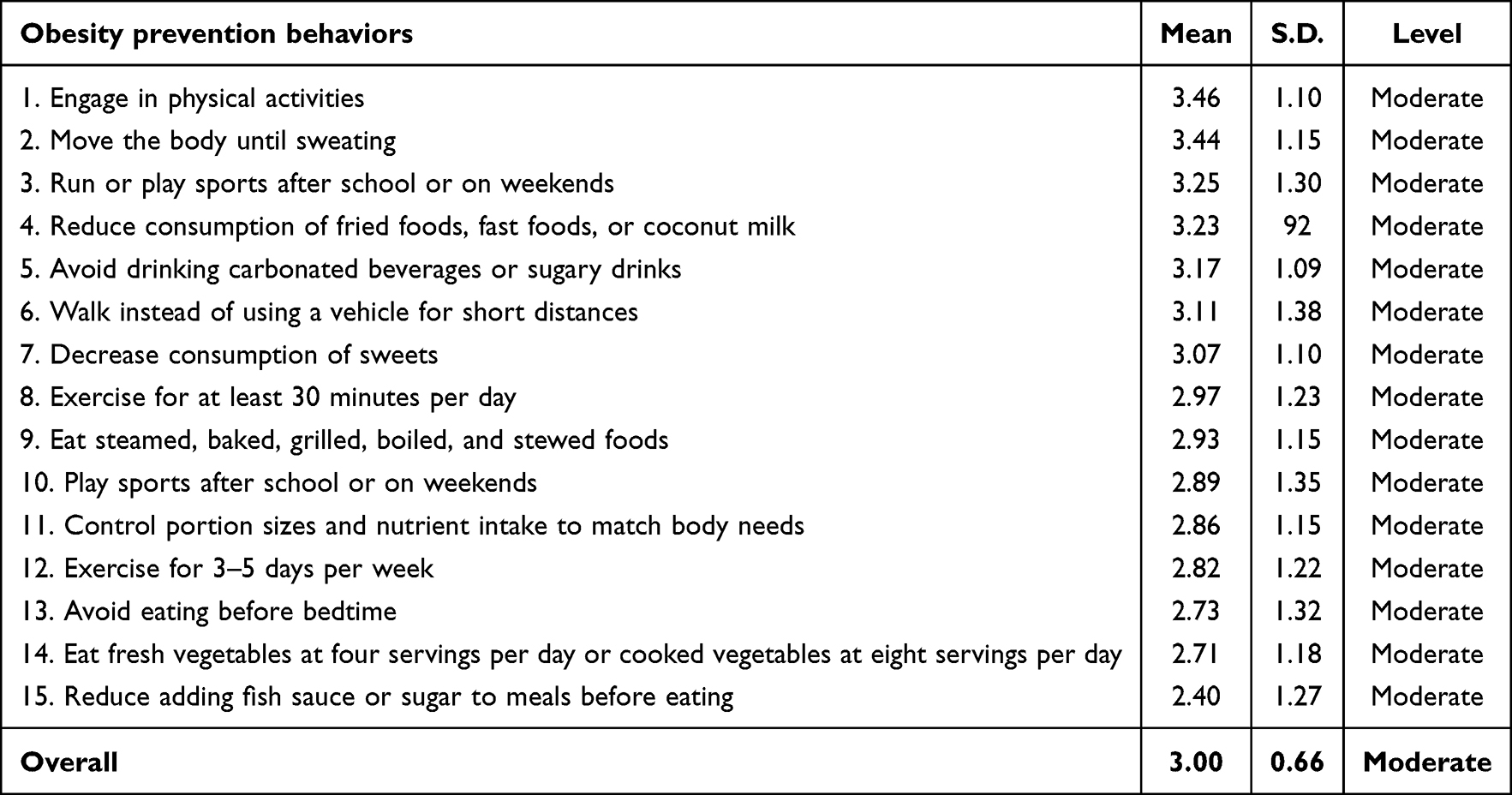 |
Table 4 Obesity Prevention Behaviors (n = 216) |
Self-Perception and Obesity Prevention Behaviors
Nearly half of the participants (49.54%) rated their self-perception of food consumption high. In comparison, over half of them reported their self-perception of physical activity (51.39%) and obesity prevention behaviors (67.59%) at moderate levels (Table 5).
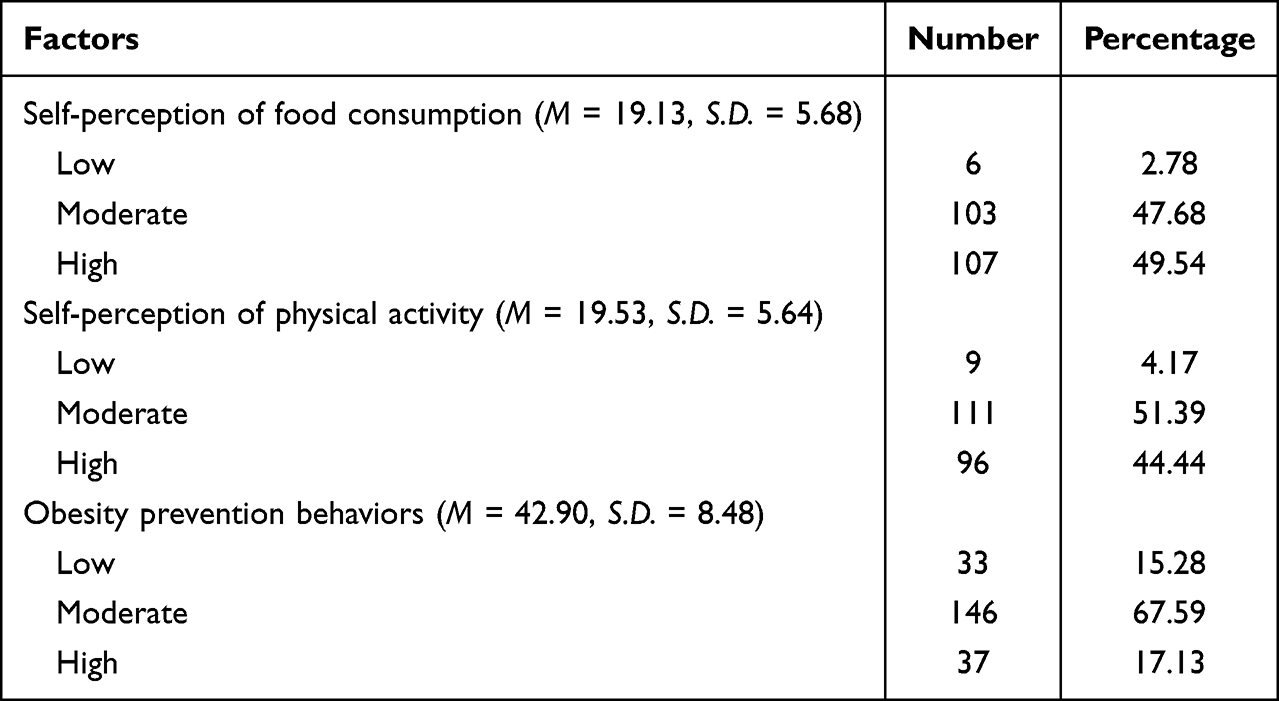 |
Table 5 Number, Percentage, Mean, and Standard Deviation of Self-Perception and Obesity Prevention Behaviors (n = 216) |
Associations Between Demographics, Environmental Factors, and Obesity Prevention Behaviors Among Participants
Factors significantly related to obesity prevention behaviors among overweight late primary school students included gender, grade point average, self-perception of food consumption, self-perception of physical activity, daily allowance received from family, and nutrition education received (p < 0.05) (Table 6).
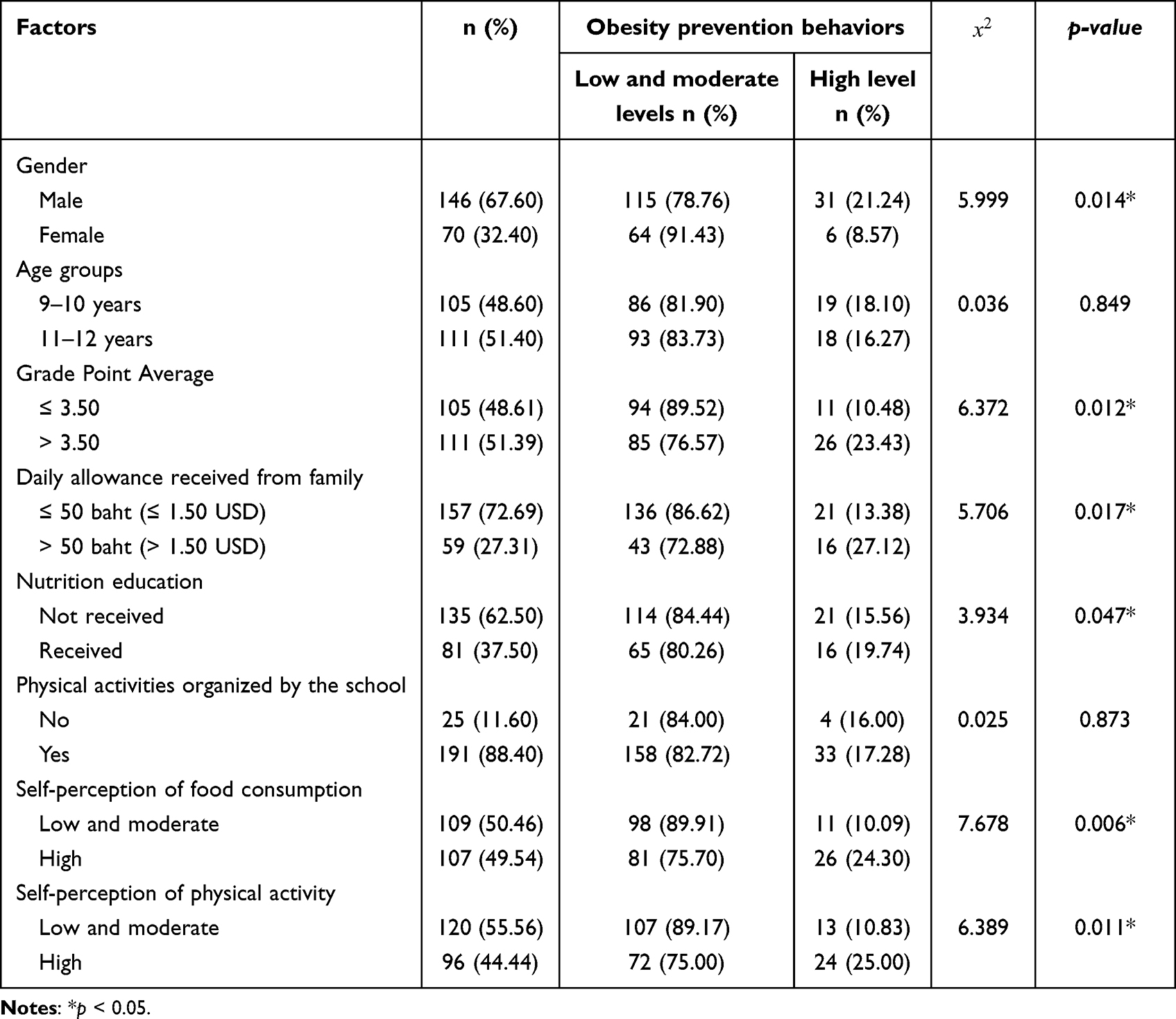 |
Table 6 Factors Related to Obesity Prevention Behaviors (n = 216) |
Predictors of Obesity Prevention Behaviors
The results revealed that gender, GPA, self-perception of food consumption, physical activity, daily allowance received from family, and nutrition education were significant predictors of obesity prevention behaviors (p < 0.05). Male students showed an 11.3% higher likelihood of having obesity prevention behaviors than females (OR = 0.113; 95% CI: 0.02–0.56). Moreover, students with a better grade point average showed a 38.3% higher probability of practicing obesity prevention behaviors than those with a lower grade point average (OR = 0.383; 95% CI: 0.18–0.82). Furthermore, students who perceived themselves as having high levels of food consumption and physical activity were 4.289 times (OR = 4.289; 95% CI: 1.72–10.73) and 2.585 times (OR = 2.585; 95% CI: 1.02–6.56) more likely to practice obesity prevention behaviors, respectively, compared to those with low and moderate self-perception levels. Students who received a daily allowance of more than 50 baht had a 40.2% higher likelihood of performing obesity prevention behaviors than those receiving less than 50 baht (OR = 0.402; 95% CI: 0.17–0.94). Furthermore, students who received nutrition education were 35.2% more likely to practice obesity prevention behaviors than those who had not received nutrition education (OR = 0.352; 95% CI: 0.15–0.84) (p < 0.05) (Table 7).
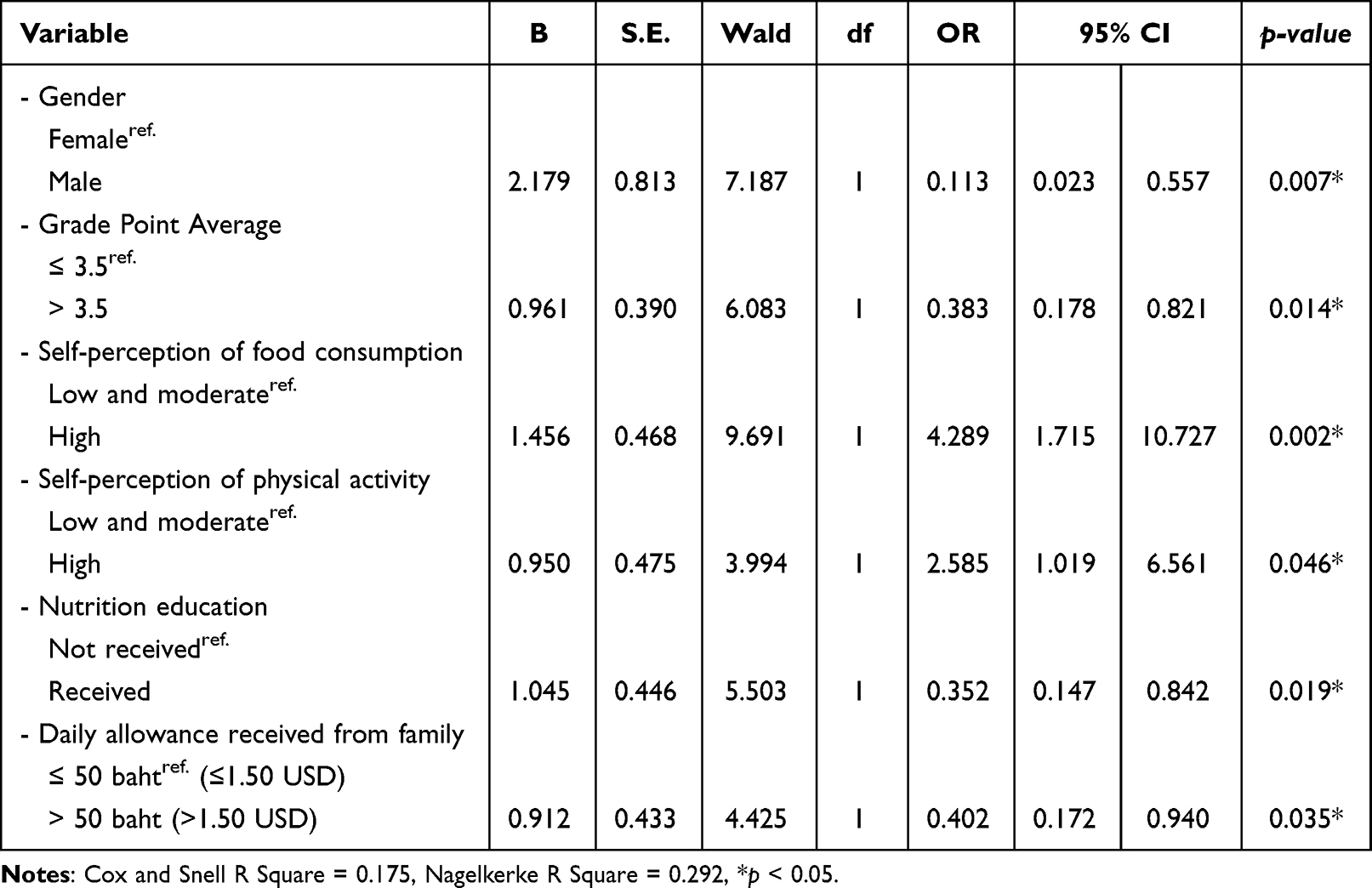 |
Table 7 Predictors of Obesity Prevention Behaviors (n = 216) |
Discussion
The findings revealed that the students, 67.59%, had overall obesity prevention behaviors at a moderate level. This finding was consistent with previous studies, indicating such obesity prevention behaviors among this particular group were generally acceptable.26 This finding was consistent with the current study, where the top five highest mean scores for obesity prevention behaviors were associated with physical activity rather than food consumption.7 Overweight students who actively engaged in various physical activities, such as exercise and sports after school or on weekends, were likelier to have obesity prevention behaviors. Given that most schools organize physical activities for students for at least an hour per week, including exercises, sports, recreational activities, and daily tasks for preventing obesity, students are encouraged to participate in physical activity.27 Regarding food consumption, students who avoided fatty and sugary foods could further contribute to preventing obesity. However, Saeloo and Wiriyasirikul (2020) revealed that students did not consistently practice food consumption behaviors due to many factors, including family and environmental influences.26 Typically, students can access and purchase unhealthy foods, especially fatty and sugary snacks, from shops near schools. Furthermore, some parents, due to work obligations, may lack the time to prepare healthy meals, leading students to consume convenient foods and sugary beverages.13
According to the findings, the percentages of the participants with moderate (47.68%) and high (49.54%) self-perception of food consumption were almost equal. On the contrary, the number of participants with a moderate self-perception regarding physical activity (51.39%) exceeded those with a high level (44.44%). However, nearly half of the students need to improve their self-perception of food consumption and physical activity to attain a higher level. Even though the current educational environment and technological advancements allow late primary school students to conveniently access health information regarding healthy food consumption and physical activity, students’ confidence in controlling these two behaviors remains moderate. Meanwhile, participants with grade point average scores equal to or greater than 3.00 should possibly contribute to increased self-perception and confidence. A possible reason for the gap in self-perception levels of these two behaviors could be the influence of health literacy. Chookunhum, Sriyasak, Boontham, Chinglek, and Sangartit (2024) mentioned that although primary school students perceived the risk of obesity, they were unable to control their behaviors due to a lack of self-management skills and information literacy.28 Similarly, Ayuwat, Montaki, Boonpob, Yamtim, Parunggul, and Roopmok (2023) supported that most primary school students knew the causes and impacts of obesity. However, they still cannot control their eating and physical activity behaviors because they cannot integrate knowledge into practice, such as balancing intake and burning energy.29 While the findings suggest an opportunity for improvement in the self-perception levels of late primary school students regarding food consumption and physical activity, there are also opportunities for addressing factors influencing these behaviors.
According to the findings, significant predictors for obesity prevention behaviors among overweight primary school students included gender, grade point average, self-perception of eating habits, self-perception of physical activity, daily allowance received from family, and nutrition education. Gender was a significant factor in predicting obesity prevention behaviors among this target group. This was consistent with previous studies revealing that male late primary school students were likelier to have better obesity prevention behaviors than females.7,14,30,31 These studies claimed that boys were likelier to engage in obesity prevention behaviors, possibly due to their preference for outdoor activities and sports. Still, girls preferred participating in sedentary activities such as reading or socializing with friends. Moreover, boys demonstrated greater physical agility and speed than girls, increasing their engagement in obesity prevention behaviors.32 Grade point average was also one of the predictors of obesity prevention behaviors. This was consistent with previous studies, which claimed that students who performed well with a grade point average were prone to engage in obesity prevention behaviors.33 Students with higher grade point average achievement were likelier to have better cognitive abilities and decision-making skills, enabling them to perform healthier habits.34 Meanwhile, students who rigorously practiced obesity prevention behaviors tended to demonstrate healthy eating behaviors and engage in physical activity, contributing to a better grade point average because they received sufficient nutrients and had good physical health.
Per the findings, self-perception of food consumption and physical activity significantly predicted obesity prevention behaviors. These findings are consistent with prior studies, suggesting that the likelihood of primary school students engaging in obesity prevention behaviors increased when they perceived their confidence in managing food consumption and physical activity at moderate to high levels.35 Primary school students with a higher self-perception of food consumption and physical activity were more likely to reduce their unhealthy food consumption and increase physical activity to balance energy.15 Moreover, those with more fantastic self-perceptions of such behaviors could select appropriate food types, quantities, and cooking methods to prevent obesity.36 Self-perception of food consumption may be associated with nutrition education, which was one of the predictors of this target behavior. Students who received nutrition education demonstrated a higher likelihood of engaging in obesity prevention behaviors.26,37 Students who participated in nutrition training programs received the necessary nutrition knowledge to enhance their awareness and attitude toward obesity prevention, giving them more confidence in making their own decisions for managing their nutritional health.38
The last predictor of obesity prevention behaviors was environmental factors, specifically the daily allowance received from family and nutrition education. These results align with previous research, which suggests that the cheapest food options are often not the healthiest. Taxing unhealthy foods poses challenges and has its limitations.39 Healthy food tends to be more expensive, limiting access for families with fewer resources. As a result, children may receive foods that are high in energy, fat, and sugar, which can lead to fewer obesity prevention behaviors.40
However, the results of testing the hypothesis found that age and participation in physical activities organized by the school had no difference in obesity prevention behaviors. Students aged 9–12 years had no difference in obesity prevention behaviors. Because the sample consisted of students aged 9–12. There is evidence of a slight increase in brain function in childhood at this age.41 Conflicts with studies that have found age were significantly related to obesity prevention among upper primary school students.7,12 Participating in physical activities organized by the school made no difference in obesity prevention behaviors because each school has a policy to prevent student obesity. In addition, schools that organized activities to promote exercise provided different sports areas and support from friends.42 This corresponds to studies that have found increasing the number of hours for physical education in schools and providing interventions in schools (eg, healthy nutrition behaviors, physical activity, and self-perception, as well as the involvement of the parents) were the most appropriate strategies for school-based intervention to prevent obesity.43 However, this study collected data on overweight students studying at eight schools under the Nakhon Si Thammarat Provincial Primary Education Office. The characteristics and contexts of overweight students outside this sample may differ significantly from those in this research.
Conclusions
Male students with a higher GPA, positive self-perception regarding diet and physical activity, prior nutrition education, and sufficient pocket money for school expenses were likelier to demonstrate effective obesity prevention behaviors than others. Given that late primary school students are currently transitioning to adolescence and forming lifelong habits, it is essential to implement strategies to prevent obesity from happening by considering these factors. Modifying health behaviors among overweight students is necessary to avoid further weight gain and the onset of obesity. Health professionals must improve among late primary school students, who must be provided nutrition education. Female individuals and late primary school students with low grade point averages require more special support. Health-care professionals should also encourage parents to give their children daily pocket money. These strategies will assist students in modifying their health behaviors and preventing obesity.
Data Sharing Statement
Additional data are not available.
Ethical Approval and Consent to Participate
The researchers conducted the study following the Declaration of Helsinki. All procedures performed in this study involving human participants followed the ethical standards of the Ethical Institutional Consideration. This study received approval from the Ethics Committee on Human Research at Walailak University on 12 June 2023 (WUEC-23-150-01) as required by the process before data collection. Informed consent was obtained by the researchers from all individual participants and the parents or guardians before they were included in the study. The children aged 9–12 years and parents will provide written consent. Research information will be stored securely, with data coded for confidentiality.
Acknowledgments
The researchers thank the Research Institute for Health Sciences and the Excellence Center of Nursing Institute, Walailak University, for providing invaluable support. We also thank the School of Nursing, Walailak University, and the target group participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding support.
Disclosure
The authors report no conflicts of interest regarding the publication of this paper or this work.
References
1. World Obesity Federation. World Obesity Day 2022 – accelerating action to stop obesity. Available from: https://www.who.int/news/item/04-03-2022.
2. World Health Organization. A new report shows progress and missed opportunities in controlling NCDs nationally. Available from: https://www.who.int/news/item/12-05-2022.
3. Bureau of Nutrition, Ministry of Public Health. Report performance results according to 1.11 The restaurants here are 6-14 years old, and the rest are proportionately good. Available from: https://nutrition2.anamai.moph.go.th.
4. Nakhon Si Thammarat Provincial Public Health Office. A percentage of students in grades 1-6 who are beginning to become obese and are obese have been screened for risk in health zone 11, Nakhon Si Thammarat Province. Academic year 2022. Available from: https://nrt.hdc.moph.go.th.
5. Kang KT, Weng WC, Lee PL, Hsu WC. Age- and gender-related characteristics in pediatric obstructive sleep apnea. Pediatr Pulmonol. 2022;57(6):1520–1526. doi:10.1002/ppul.25900
6. Powell SB, Engelke MK, Swanson MS. Quality of life in school-age children with obesity. Pediatr Nurs J. 2018;44(4):183–189.
7. Chuaysrinuan J, Chaimay B, Woradet S. Factors associated with health literacy towards obesity prevention among primary school students in Cha-Uat District, Nakhon Si Thammarat Province. J Acad J Commun Public Health. 2020;5(1):1–9.
8. Cui X, You L, Zhu L, et al. Change in circulating microRNA profile of obese children indicates future risk of adult diabetes. Metabolism. 2018;78(1):95–105. doi:10.1016/j.metabol.2017.09.006
9. Chung ST, Krenek A, Magge SN. Childhood obesity and cardiovascular disease risk. Curr Atherosclerosis Rep. 2023;25(1):405–415. doi:10.1007/s11883-023-01111-4
10. Wang S, Sun Q, Zhai L, Bai Y, Wei W, Jia L. The prevalence of depression and anxiety symptoms among overweight/obese and non-overweight/non-obese children/adolescents in China: a systematic review and meta-analysis. J Environ Res Public Health. 2019;16(3):340. doi:10.3390/ijerph16030340
11. Gomaa M, Mohamed H, Zaky E, Mahmoud Z, El-Hakeem W. The effect of adenotonsillectomy in intelligence quotient in children with obstructive sleep apnea. Minia J Med Res. 2020;31(1):257–261. doi:10.21608/MJMR.2022.221516
12. Wannala U. Factors influencing the health status of late adolescents in Muang District, Lampang Province. J Health Sci Sch. 2021;8(2):197–215.
13. Li B, Pallan M, Liu WJK, et al. The CHIRPY DRAGON intervention in preventing obesity in Chinese primary-school-aged children: a cluster-randomized controlled trial. PLoS Med. 2019;16(11):e1002971. doi:10.1371/journal.pmed.1002971
14. Shah B, Cost KT, Fuller A, Birken CS, Anderson LN. Sex and gender differences in childhood obesity: contributing to the research agenda. BMJ Nutr Prev Health. 2020;3(2):387–390. doi:10.1136/bmjnph-2020-000074
15. Kulik N, Moore W, Mc Caughtry M. Knowledge, attitudes, self-efficacy, and healthy eating behavior among children: results from the building healthy communities trial. Health Educ Behav. 2019;46(4):602–611. doi:10.1177/1090198119826298
16. Prasitnarapun B, Wuttijurepan A, Jooprempree K, Wannakhao S. The relationships between health literacy, perceived self-efficacy and preventing obesity behavior of school students, grade 4-6. Boromarajonani College Nurs Uttaradit J. 2020;12(2):216–226.
17. Pichaitum S, Juntarawijit Y, Hanrongcharotorn U. Association between family factors and parenting style and nutritional status among students grade 4-6 in schools under the office of the basic education commission. J Nurs Div. 2020;47(4):88–96.
18. Namyota C, Wongprachum K, Toontom N, Bourneo C. Effects of a nutritional-promoting program on reducing the prevalence of overweight and obesity in school-age children. J Sci Technol MSU. 2022;41(1):40–59.
19. Kittiboonthawal P, Chernchum J, Cheutong S. Health literacy and health behaviors of school-aged children. J MCU Soc Dev. 2022;7(2):71–84.
20. Manoprasertkul T, Pongrangsarn P. Prevalence and related factors of overweight and obesity among primary school children. Buddhachinaraj Med J. 2020;37(2):159–167.
21. Kangsanun C, Khuvasanond K. Guidelines in a transition from primary to secondary grades: multi-case studies in international school contexts. J Silpakorn Edu Res J. 2020;12(2):343–358.
22. Bandura A Self-efficacy: the exercise of control (1997). New York: W.H. Freeman. Available from: https://www.scribd.com/document/392014248/Self-efficacy-The-Exercise-of-Control-1997.
23. Bureau of Nutrition, Ministry of Public Health. A guide to using growth benchmarks for children aged 6 - 19 years. Available from: https://multimedia.anamai.moph.go.th/associates/guide-using-The-growth-criteria-for-children-ages6_19/.
24. Chaboonruang S. Results of the program to promote awareness of self-efficacy by peer groups and consumption and exercise behavior of early adolescents with overnutrition. J Nurs Health Care. 2014;32(3):119–126.
25. Division of Health Education, Department of Health Service Support: evaluation of health knowledge to prevent obesity for students aged 9-14. (Upper elementary and middle school students). Available from: file:///C:/Users/Acer/Downloads/071120190819395574_linkhed%20(8).pdf.
26. Saeloo J, Wiriyasiriku N. The relationship between health literacy and obesity prevention behaviors of school-age children with overweight and obesity in schools under primary educational service area office Mueang District, Nakhon Si Thammarat Province. J MCU Nakhondhat. 2020;7(11):1–14.
27. Liu Z, Xu H, Wen L, et al. A systematic review and meta-analysis of the overall effects of school-based obesity prevention interventions and effect differences by intervention components. Int J Behav Nutr Act. 2019;16(1):95. doi:10.1186/s12966-019-0848-8
28. Chookunhum P, Sriyasak A, Boontham S, Chinglek W, Sangartit S. Health literacy and obesity health behaviors among primary school students. J Health Res Innov. 2024;7(1):1–12.
29. Ayuwat T, Montaki S, Boonpob P, Yamtim P, Parunggul C, Roopmok S. Solution of over nutrition among primary school students in private school of U-Thong District, Suphanburi Province. J Sirindhornparidhat. 2023;24(1):355–366.
30. Tongwat P, Kitreerawutiwong N. Factors predicting physical activity behaviors among grade 4-6 students in Nongkula Sub-district, Bang Rakam District, Phitsanulok Province. Nurs J Ministry Public Health. 2019;29(2):24–34.
31. Zhang J, Yi Z, Feng XQ, et al. Gender differences in the prevalence of overweight and obesity, associated behaviors, and weight-related perceptions in a national survey of primary school children in China. Biomed Environ Sci. 2018;31(1):1–11. doi:10.3967/bes2018.001
32. Tomkinson GR, Carver KD, Atkinson F, et al. European normative values for physical fitness in children and adolescents aged 9-17 years: results from 2 779 165 Eurofit performances representing 30 countries. Br J Sports Med. 2018;52(22):1445–1456. doi:10.1136/bjsports-2017-098253
33. Injan J, Saenbutr S, Dibyamadala J, Mangkhang C. Guidelines of integrated system thinking learning management in social studies for primary school students. J Humanit Soc Sci Univ Phayao. 2021;9(2):41–50.
34. Doustmohammadian A, Omidvar N, Mohammadi NK, Zinab HE, Amini M, Abdollahi M. The association and mediation role of food and nutrition literacy (FNLIT) with eating behaviors, academic achievement and overweight in 10–12 years old students: a structural equation modeling. Nutr J. 2022;21(45). doi:10.1186/s12937-022-00796-8
35. Paddanja P, Toontom N, Kaewpitoon N. Effects of behavior modification program on reducing overweight among school-aged students between 12 and 14 years old in Nong Bunnak Subdistrict, Nong BunMak District, Nakhon Ratchasima Province. J Off DPC 7 Khon Kaen. 2020;27(2):103–114.
36. Suwanumpa N, Salawongluk T. The effect of dietary and exercise modification program for obesity prevention among primary schools in Nakhon Ratchasima Municipality. Ratchaphruek J. 2019;17(1):111–120.
37. Subongkot P, Jirasathit S, Sirisophon N, Onsiri S, Nithitham O. The effectiveness of health education program to change dietary behavior of overweight students at the elementary school level at Watklangklongsi School Pathum Thani Province. J Health Phys Edu Rec. 2019;45(2):100–108.
38. Francis LA, Nix RL, BeLue R, et al. Designing a childhood obesity preventive intervention using the multiphase optimization strategy: the healthy bodies project. PMC Clin Trials. 2023;20(4):4340446. doi:10.1177/17407745231167115
39. Walque DD. The use of financial incentives to prevent unhealthy behaviors: a review. J Soc Sci Med. 2020;261:112236. doi:10.1016/j.socscimed.2020.113236
40. Yaemborisut U. Food insecurity and childhood obesity: mini-review. J Public Health. 2018;48(1):95–107.
41. Miguel PM, Pereira LO, Silveira PP, Meaney MJ. Early environmental influences on the development of children’s brain structure and function. Dev Med Child Neurol. 2019;61(10):1127–1133. doi:10.1111/dmcn.14182
42. Bluher SW, Hauschild KK, Graf C, et al. Current guidelines for obesity prevention in childhood and adolescence. Obese Facts. 2018;11(3):263–276. doi:10.1159/000486512
43. Joyrod S, Songthap A Development of a model for overweight prevention among junior high schools by multilateral participation in the Eastern Economic Corridor Chachoengsao. Available from: https://nuir.lib.nu.ac.th/dspace/bitstream/123456789/5608.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.