Back to Journals » Patient Preference and Adherence » Volume 19
Factors Influencing Rehabilitation Exercise Behavior in Elderly Rotator Cuff Repair Patients: A Qualitative Study Based on the Theory of Behavior Change Wheel
Authors Tang Q, Hu F, Zhao J, Wang N
Received 13 June 2025
Accepted for publication 13 September 2025
Published 26 September 2025 Volume 2025:19 Pages 3037—3047
DOI https://doi.org/10.2147/PPA.S546831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Qi Tang,1,2 Fang Hu,1 Jie Zhao,2 Nan Wang2
1Department of Nursing, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China; 2Trauma Upper Limb Ward 1, Tianjin Hospital, Tianjin, People’s Republic of China;
Correspondence: Fang Hu, Email [email protected]
Purpose: With the incidence of elderly patients requiring rotator cuff repair, it is crucial to investigate the factors influencing rehabilitation exercise behavior. The theory of the behavior change wheel is used to analyze the factors that influence an individual’s health behaviors. This study aimed to explore factors that can influence rehabilitation exercise behavior in elderly rotator cuff repair patients based on the theory of behavior change wheel. This is a qualitative study using thematic analysis.
Methods: Data was collected through face-to-face interviews with 15 elderly rotator cuff repair patients in the traumatic upper limbs unit of the Tianjin Hospital. This study adhered to the targeted thematic analysis based on the theory of behavior change wheel.
Results: Three themes and seven sub-themes were identified, including rehabilitation exercise capability-related factors (rehabilitation exercises exacerbate postoperative pain, postoperative discomfort, lack of knowledge of rehabilitation exercises), the influence of external environmental opportunity-related factors (supervision and encouragement by primary family caregivers, support and guidance from healthcare professionals), and motivation-related factors for adherence to rehabilitation exercise behavior (health beliefs, rehabilitation expectations).
Conclusion: This study reveals that the rehabilitation exercise behavior in elderly rotator cuff repair patients is influenced by factors related to capability, opportunity, and motivation. Reducing postoperative pain, enhancing health belief, setting reasonable rehabilitation expectation, emphasizing social support, and expanding access to proactive information will contribute to improving the quality of rehabilitation exercises. Future research should expand the scope to include family members and caregivers to conduct a more comprehensive exploration of the influencing factors.
Keywords: rotator cuff repair, rehabilitation exercise, the theory of behavior change wheel, qualitative study
Introduction
Rotator cuff injury is a degenerative musculoskeletal disorder commonly observed in the elderly, with limited shoulder motion, pain, and weakness that worsens at night as the main clinical manifestations.1 Rotator cuff injuries account for approximately 50% of shoulder disorders,2 and their incidence is positively correlated with age,3 with prevalence rates of up to 31% in 60–69 year-olds and up to 65% in those over 80 years of age.4 By the end of 2022, China’s population aged 60 years and over, will reach 280 million,5 and the aging problem is becoming increasingly serious. The number of elderly patients requiring rotator cuff repair in China will increase rapidly.
Currently, Arthroscopic Rotator Cuff Repair (ARCR) is the predominant treatment method for clinical surgical treatment of patients with rotator cuff injury,6 which has the advantages of less trauma and quicker recovery compared with traditional open procedures.7 The rehabilitation process after ARCR promotes healing of the repaired tendons, minimizes shoulder stiffness and muscle atrophy.8 ARCR has a long postoperative rehabilitation period, which usually takes 20–26 weeks.9,10 Poor rehabilitation may lead to increased readmission rates and seriously affect the patients’ quality of life. Therefore, appropriate rehabilitation exercise behavior is critical in elderly rotator cuff repair patients. However, elderly rotator cuff repair patients lack the ability to master proper rehabilitation exercise behaviors, highlighting the need to investigate the factors influencing rehabilitation exercise behavior.
The theory of the behavior change wheel is commonly used to comprehensively analyze the factors and mechanisms that influence an individual’s health behaviors.11 The core layer is the COM-B model (Capability, Opportunity, Motivation, Behavior Model). According to the COM-B model, capabilities refer to behavioral norms, psychological skills, habitual attentiveness, and decision-making processes. Opportunity refers to all external factors that guarantee or promote the occurrence of individual behavior, such as social environment-social influence, physical environment-enviromental background, environmental background, and resources. Motivation refers to the brain activity process that stimulates and guides behavior, including reactive and spontaneous motivation. Reactive motivation refers to the belief requirements of social or professional roles on ability and outcome, whereas spontaneous motivation refers to optimism, reinforcement, and emotions. The motivation of motivating styles will more effectively promote the formation of behaviors.12 Individual behavior is the result of the combined actions of capability, opportunity, and motivation. Ability and opportunity can have both direct influence on behavior and an indirect influence on behavior through motivation. Research has been conducted to improve postoperative rehabilitation intentions on the theory of behavior change wheel in health behavior promotion.13
The study by Zhang has identified factors that affect shoulder joint function recovery in patients with T2DM following ARCR, based on the behavior change wheel theory and COM-B model.14 Consequently, the study has adopted the theory of behavior change wheel as a theoretical framework to explore the factors associated with rehabilitation exercise behavior in elderly rotator cuff repair patients.
Past researchers have identified poor adherence to postoperative rehabilitation exercises after ARCR and patient sex has a positive impact on rehabilitation exercise behavior.15,16 Given that post-operative rehabilitation behavior is influenced by the complex factors such as individual cognition, feedback information, and external resource environment, these quantitative studies are incomplete in their exploration of the factors influencing rehabilitation exercise behavior.17 Although some qualitative studies exist, the area of concern is different populations. Zhang et al18 identified the factors influencing the postoperative rehabilitation of type 2 diabetic patients with rotator cuff injuries. There is a lack of qualitative research on rehabilitation exercise behavior among elderly rotator cuff repair patients. Thus, the present study uses a qualitative research method and takes the theory of behavior change wheel as the framework to deeply explore the influencing factors of rehabilitation exercise behavior in elderly rotator cuff repair patients, so as to help understand the possible reasons behind rehabilitation exercise behavior, and provide content for the construction of the rehabilitation exercise program for elderly rotator cuff repair patients.
Materials and Methods
Design
We collected data by interviewing elderly rotator cuff repair patients. This study design was a qualitative research that used the targeted thematic analysis based on the theory of behavior change wheel to explore the factors influencing rehabilitation exercise behavior in hospital in elderly rotator cuff repair patients.
Participants and Recruitment
We used the maximum variation purposive sampling method to select participants in the traumatic upper limbs unit of the Tianjin Hospital as the study population. Maximum differentiation of the sample was obtained by selecting subjects with different educational qualifications, different work, and different medical payments. Tianjin Hospital is a tertiary general hospital located in Tianjin, China. The traumatic upper limbs unit of Tianjin Hospital has 36 beds and accepts patients with rotator cuff injuries, providing professional postoperative rehabilitation guidance. We have a professional rehabilitation team including doctors, rehabilitation nurses, and therapists.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (a) ≥60 years of age; (b) rotator cuff injury diagnosed on imaging and treated with the arthroscopic rotator cuff repair; (c) three or more sessions of rehabilitation training supervised by rehabilitation therapists and specialized nurses during hospitalization and each session lasts 30–60 minutes; (d) no cognitive or communication impairments.
The exclusion criteria were as follows: (a) a combination of serious postoperative complications or diseases; (b) mental illness or cognitive impairment. The sample size was based on information saturation with interview data.
Data Collection
Data were collected from April to September 2024. We collected information through face-to-face semi-structured in-depth interviews. Interviewers contacted the interviewees in advance and established a relationship of trust with them. To minimize researcher bias, reflexivity was maintained through bracketing and reflective journaling. To ensure a comfortable and private environments for participants, interviews were held in quiet places where they felt at ease, such as a hospital ward or ward showroom. The preliminary interview outline was developed based on a comprehensive review of relevant literature and in consultation with experts in joint surgery and nursing. The preliminary interview outline was designed around the three main elements of the theory of behavior change wheel, namely Capability, Opportunity, and Motivation. After determining the preliminary interview outline, two participants were selected for pre-interviews. After discussing the issues identified in the pre-interviews, the draft was revised by experts based on their professional knowledge and clinical experience through discussions held involving 2 physicians (with doctoral degrees and associate chief physician or higher titles) and 1 head nurse (with a bachelor’s degree and charge nurse or higher title). In case of disagreements, another 2 physicians and 1 head nurse would conduct further deliberations to reach a consensus. Finally, the final interview outline was as follows: (1) Capability: ”How do you do rehabilitation?”, “What are your feelings or experiences in the rehabilitation exercise process?”. (2) Opportunity: “What is the attitude of your family and friends towards your rehabilitation exercise”? Which people’s opinions do you feel influence your rehabilitation exercise”? To ensure the quality of your rehabilitation exercise, what help do you want?”. (3) Motivation: ”What factors do you think will affect your rehabilitation?”, “What difficulties have you encountered during the rehabilitation process? How did you solve them”? “How confident you are that you will be able to maintain your rehabilitation exercise behaviours”. The participants’ nonverbal reactions and the researcher’s feelings at the time were documented. With the consent of the participants, the entire interview was recorded using a voice recorder. After the interviews, the data were transcribed and analyzed within 24 hours. The interviews lasted between 20 and 40 minutes to share their feelings and experiences. The sample size was determined based on the principle of data saturation, which occurs when no new information emerges from the interview data. In this study, the information was saturated after interviewing 15 patients. No new content was generated after continuing to interview 2 patients.
Data Analysis
This study adhered to the targeted thematic analysis. The analysis was divided into three steps: (1) Read the interview data repeatedly to familiarize with the content of the data. The sentence reflecting the factors affecting the rehabilitation exercise of patients was taken as the segmentation point of the minimum unit to form the minimum analysis unit and code them. This step is performed by 1 coder; (2) Determine the classification outline according to the COM-B model. The meaningful units were then categorized according to the classification outline by two trained coders. For the categories that are prominent, we will summarize to form a theme. (3) Report the results of our analysis, interpret the results, and form relationships between data and themes. Representative examples were extracted from the data.
Quality Control
To ensure the rigor of the study, four criteria were adopted: credibility, dependability, confirmability and transferability. The credibility issue is addressed through member checks, and participants have the opportunity to review and verify the identified topics and sub-topics. The research team included experts in joint surgery and nursing, who reviewed and confirmed the topics. For dependability, two researchers independently analyzed and coded the data. To enhance confirmability, researchers held group discussions to explore and exchange their thoughts and insights on this study. For transferability, a detailed and clear description of the research design, participants, data collection and analysis was provided.
Ethical Considerations
The study was approved by the Tianjin Hospital Ethics Committee (2024–109), and it complies with the Declaration of Helsinki. All participants were informed about the study’s objectives and provided informed written consent including permission to publish anonymized direct quotes before the interview. During the study’s description participants had the right to withdraw.
Results
Participants
A total of 15 patients were formally interviewed for this study. To protect the privacy of the participants, they were coded as N1 to N15. More detailed demographic characteristics are presented in Table 1. With the guidance of the Behavior Change Wheel framework, the qualitative analysis of interview data identified three main themes influencing the rehabilitation exercise behavior among elderly rotator cuff repair patients: (1) Rehabilitation exercise capability-related factors; (2) The influence of external environmental opportunity-related factors; (3) Motivation-related factors for adherence to rehabilitation exercise behavior. The themes and subthemes are described below (Table 2).
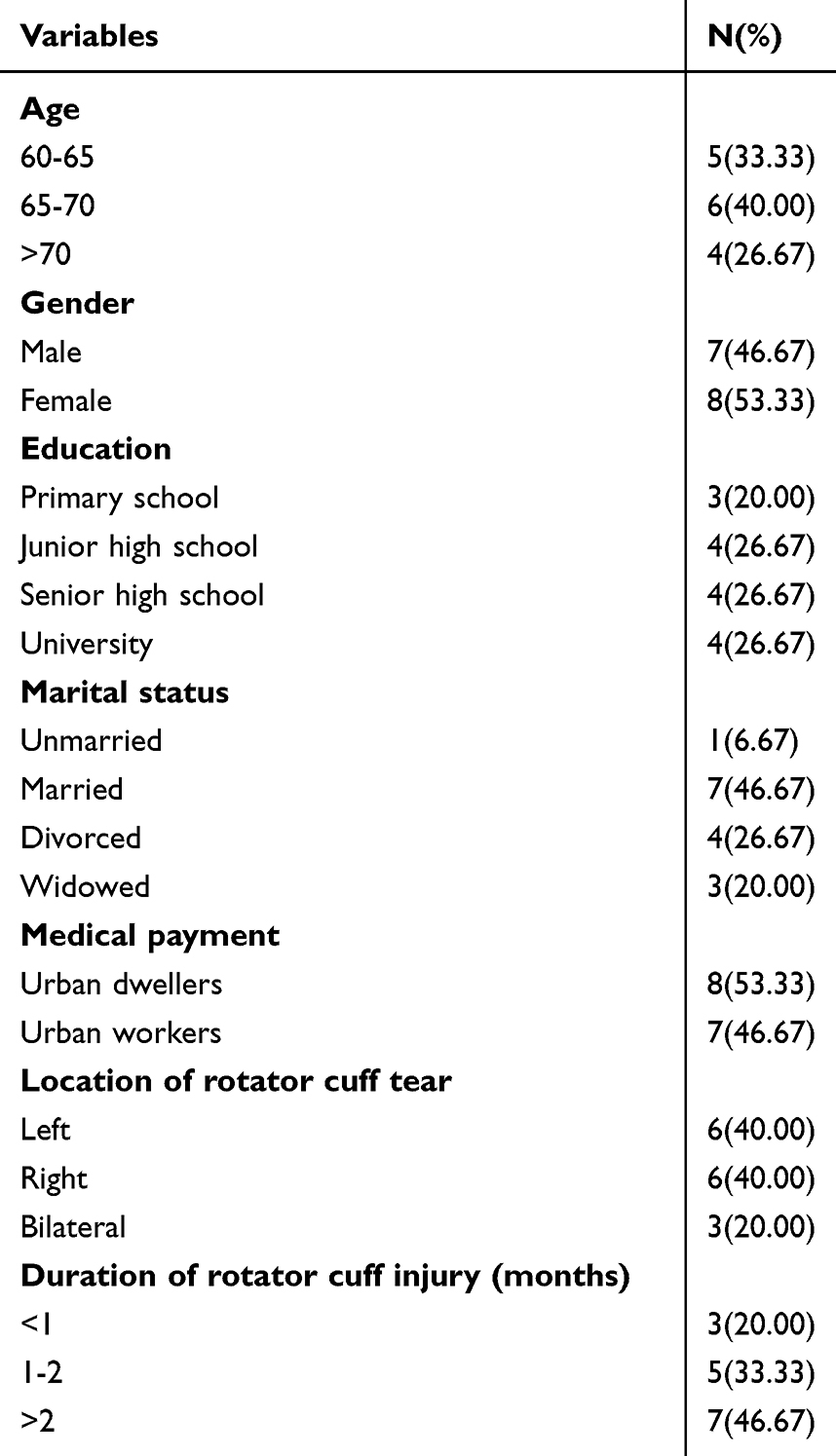 |
Table 1 Characteristics of Participants (N=15) |
 |
Table 2 Themes, Subthemes, and Representative Quotes From the Interviews |
Theme 1: Rehabilitation Exercise Capability-Related Factors
The rehabilitation exercise capability-related factors included physical ability and the psychological abilities. Participants reported that their physical skills and knowledge changed their rehabilitation exercise behavior.
Subtheme 1: Rehabilitation Exercises Exacerbate Postoperative Pain
Long-term adherence to rehabilitation exercises by patients after rotator cuff repair is a key prerequisite for functional recovery, but because the postoperative wounds have not yet healed, patients’ pain increases during rehabilitation exercises, which severely limits their ability to perform rehabilitation exercises, and some patients even interrupt rehabilitation due to fear of pain. (p1): The main difficulty in the rehabilitation exercise process was painful, and the neck pulling also felt painful after the surgery, making it difficult for me to keep going. (p9): “I am now afraid of rehabilitation exercises and the mental tension combined with the pain made me want to give up at one point. My rehabilitation therapist told me that the less I relax my muscles, the more tense they get and the more painful they become, but I cannot relax!” (p4): “I am sensitive to pain, the first exercise is very painful, once to give up, feel do not want to practice again, after taking painkillers feel much better.” (p5): Rehabilitation exercises don’t hurt when you don’t exert yourself, and they hurt when you do. No exercise when it hurts, exercise when it doesn’t hurt.
Subtheme 2: Postoperative Discomfort
Because of the fact that the elderly are physically weak and have not yet recovered their physical strength, postoperative patients commonly suffer from fatigue, lack of physical strength, dizziness, nausea, and other symptoms. Postoperative discomfort is an important factor that interferes with the execution of rehabilitation exercises, making it difficult for patients to complete the prescribed rehabilitation exercise tasks. (p6): I feel tired during every rehabilitation exercise, especially when lifting upwards, I feel exhausted after doing it, and I don’t want to exercise once I’m tired. (p10): I feel that my physical strength is poor and weak, and my postoperative reaction to general anesthesia is quite strong and my head is quite dizzy, which makes me have no strength in the process of rehabilitation and exercise, and it is quite difficult for me to persevere. (p3): “After the surgery, I felt weak, always sweating and not quite strong enough. Doing it twice a day was a bit overwhelming for me.” (p9): “I’m not that strong in my recovery to help my arms reach the required position, I just can’t practice it.”
Subtheme 3: Lack of Knowledge of Rehabilitation Exercises
Elderly rotator cuff repair patients are usually hospitalized for 3–5 days after surgery, but their rehabilitation cycle takes 3–6 months. Most patients had some knowledge about rehabilitation exercises, but most of them are not clear about their importance and specific content. Elderly patients generally suffer from memory loss, poor comprehension, and inability to actively learn the relevant knowledge, resulting in unsatisfactory rehabilitation results. (p1): “I’m old and have a bad memory, so I’m afraid that if I go home and don’t exercise in the right way it will affect my later recovery.” (p8): I feel like this workout would only take a few minutes, but when practicing it I’m not sure I’m practicing it correctly and still need to write it down on paper. (p12): I’m old enough to practice and forget the movements of my rehab exercises. Is the angle of lift for shoulder rehabilitation 160 degrees? I feel like I’m not lifting it properly. (p4): I looked up on the Internet about rehabilitation exercises related to the disease, I wonder if it’s right, it doesn’t feel the same as actually exercising it.
Theme 2: The Influence of External Environmental-Opportunity-Related Factors
The external environment including social opportunities and physical opportunities influenced rehabilitation exercise behavior in elderly rotator cuff repair patients.
Support from family members and healthcare professionals promoted rehabilitation exercises for elderly patients.
Subtheme 1: Supervision and Encouragement by Primary Family Caregivers
In the process of rehabilitation exercise, some patients are prone to inertia and lack of self-discipline, and it is beneficial to improve the quality of rehabilitation for the main family caregivers to motivate and supervise the patients to adhere to the behavior of rehabilitation exercises, to take care of their daily life, and to assist in their rehabilitation exercise. The level of support from the main family caregiver affects the patient’s adherence to rehabilitation exercises, and the higher the level of support, the better the patient can complete the rehabilitation exercises. (p4): My family is very helpful and caring, my daughter is very concerned about me, my daughter said that if I can’t do the rehabilitation exercises on my own, she will give me a self-funded rehab clinic number until I get good at the exercises. (p7): I feel that there is no difficulty in this rehabilitation exercise, my family understands this aspect very well, and my partner always encourages me to insist on exercising, as long as I insist on good rehabilitation shoulder function recovery is not a problem at all! (p10): “I hope that my family will be present during the rehab exercises and that they will learn to understand that they can help me with my recovery when I go home.” (p6): “The kids are busy and I’m afraid of bothering the kids, my son told me to get a good workout in and that I need to stick with it and not burden them.”
Subtheme 2: Support and Guidance From Healthcare Professionals
Most of the patients said that the knowledge of postoperative rehabilitation exercise was acquired through health education by healthcare professionals, and the professional guidance from healthcare professionals could promote the rehabilitation exercise of the patients, and they expected to receive guidance on the continuation of the rehabilitation exercise at home. (p3): After being discharged from the hospital, you need to go home and do rehabilitation exercises on your own, and you need more guidance from the doctors and nurses if you don’t understand something.(p6): “I was hospitalized for a few days and the doctors and nurses gave me a lot of knowledge about rehabilitation exercises, which I didn’t understand before, but I have to practice according to what the doctors and nurses told me.” (p12): “Worried that I can’t practice well, I want to go to an outpatient rehabilitation specialist a few times after discharge from the hospital.” (p14): I hope the doctors and nurses can do more health education, about the rehabilitation exercise knowledge a lot of don’t know, if only the discharge of the hospital can be at home to get professional guidance would be good!
Theme 3: Motivation Related Factors for Adherence to Rehabilitation Exercise Behavior
Subtheme 1: Health Beliefs
Health beliefs affect patients’ rehabilitation exercise behavior when patients have stronger self-confidence in rehabilitation exercises, their attitude towards participation in rehabilitation exercise was more positive, they could better adhere to the completion of rehabilitation exercise, and their adherence to rehabilitation exercise was higher. (p7): I had surgery on the other rotator cuff two years ago and am recovering well, just like a normal arm, and I’m confident that I’ll be able to get back to normal this time with rehab exercises. (p9): “I still have to get over my mental difficulties and grit my teeth and keep working out, I think I can do it!” (p15): “I don’t think rehab is difficult for me, I just have to be in place every day for a faster recovery.”
However, some patients expressed a lack of confidence in completing the rehabilitation exercise tasks and a fear of rehabilitation exercise in their mindset. (p4): My tolerance and willpower are so poor that I feel scared when I exercise, and I feel that I can’t keep exercising after being discharged from the hospital. (p12): “I’m a mentally fragile person who is prone to fear and anxiety, and I wonder how well the rehabilitation exercises are working out.”
Subtheme 2: Rehabilitation Expectations
Patients have different levels of rehabilitation expectations after surgery, such as recovery of shoulder joint function after surgery, improvement of quality of life, and reduction of family burden. When the expectation of rehabilitation is too high, the patients feel that the desired effect cannot be achieved, thus generating negative emotions and hindering rehabilitation exercises. However, when the expectation of rehabilitation is too low, the patient will easily become lazy and give up further rehabilitation exercise after meeting his/her expectations. (p2): I’m not asking for much, as long as I don’t have to sleep through the night in pain like I did before the surgery, I’ll work out as much as I can. (p5): I’m a farmer and I’m afraid that I won’t be able to continue farming if I don’t recover well, and I’m worried that I won’t be able to do heavy work with this arm, but I don’t feel much effect from practicing in the past few days. (p6): The burden on the family is very heavy, and I don’t know when the shoulder will be able to move normally. I’m afraid that I won’t be able to take care of myself if I don’t recover well at a later stage.
Discussion
This study explored the factors influencing rehabilitation exercise behavior of elderly rotator cuff repair patients guided by the theory of behaviour change wheel, which included capability factors, opportunity factors, and motivation factors. We found that elderly rotator cuff repair patients’ rehabilitation exercise behaviors are influenced by a variety of factors. Understanding the factors influencing rehabilitation exercise behavior can provide a valuable reference for formulating a standardized rehabilitation exercise program.
Capability‐Related Factors
Reducing Postoperative Pain and Discomfort Helps Improve Adherence to Rehabilitation Exercise
Patients with rotator cuff injuries are at risk for multiple complications immediately after surgery, with more than 50% of patients experiencing more than moderate pain.1 The level of postoperative pain and discomfort is exacerbated by the presence of frailty and inadequate nutritional status in the elderly. Most participants in this study were unwilling to perform rehabilitation exercises due to fear of pain and physical exhaustion, which seriously affects the rehabilitation exercises performed by elderly postoperative patients with ARCR. If postoperative rehabilitation is poor, the patient’s shoulder function cannot be restored. Therefore, it is particularly important to strengthen postoperative pain management, improve patients’ postoperative discomfort symptoms in a timely and effective manner, thereby reducing resistance due to pain and discomfort, and encourage patients to adhere to rehabilitation exercises. Use of hot packs before rehabilitation exercises and intermittent cold packs after rehabilitation exercises reduce the inflammatory response and help relieve pain symptoms.19 Adding instrument-assisted soft tissue mobilization to conventional rehabilitation after ARCR effectively improved pain and upper extremity function.20 Implementation of individualized phased rehabilitation exercises, when the patient’s pain and discomfort worsened, take a short break and promptly adjust the exercise intensity. Enhancing patients’ post-operative nutritional support, increasing physical strength, and reducing postoperative fatigue can help promote patients’ rehabilitation exercises.21
Expanding Access to Proactive Rehabilitation Exercise Information
Most participants indicated that they had a strong demand for rehabilitation knowledge but lack proper access to it. Due to the weak ability of elderly patients to accept new things and their low acceptance of medical treatment, a single educational approach to rehabilitation exercises can not adequately meet their needs. Even if effective rehabilitation is ensured during the postoperative stay in the hospital, the compliance and effectiveness of home rehabilitation cannot be monitored, which may lead to interruptions in rehabilitation. A study shows that remote shoulder rehabilitation has a positive effect on rehabilitation exercise behavior in patients with ARCR2.22 In the future, healthcare professionals will need to provide convenient and easy-to-understand rehabilitation knowledge resources that are tailored to the characteristics of elderly patients. For elderly patients who can use electronic products and have a strong ability to accept new things, the WeChat mobile platform, video health education, and feedback from the WeChat group can be used. Elderly patients who do not know how to use electronic devices are instructed on rehabilitation exercises using face-to-face health education and family assistance.
Opportunity‐Related Factors
Family Members and Healthcare Professionals Should Play a Supportive Role
It is worth noting that family primary caregivers and healthcare provider support may promote rehabilitation exercises in older postoperative ARCR patients. With the further development of Accelerated Rehabilitation Surgery, patients have shorter hospitalization days, faster bed turnover, and ARCR patients are facing discharge as they improve after surgery. However, the rehabilitation cycle usually takes 3–6 months, and most patients need to return to their families for at-home rehabilitation exercises, with the primary family caregiver playing an important role in assisting with rehabilitation exercises.23 Accompaniment rehabilitation exercises by family members can help patients increase the confidence to a rapid recovery and correct rehabilitation misconceptions.15 Therefore, encouraging and supporting the active participation of the family’s primary caregiver in the rehabilitation exercise process is conducive to promoting the development of rehabilitation exercise behaviors in patients. As the guides and supervisors of postoperative rehabilitation exercises, healthcare professionals play a crucial role in enabling patients to complete the exercises step by step. Managers should strengthen the training of rehabilitation knowledge of healthcare professionals. Healthcare professionals should emphasize the importance of rehabilitation exercise and give to the patient’s professional rehabilitation guidance and directions. Providing extended out-of-hospital care support and maintaining regular communication with the patient conducive to accelerate their recovery process.24
Motivation‐Related Factors
Strong Health Beliefs and Setting Reasonable Rehabilitation Expectations
Health beliefs are patients’ perceptions of the severity and susceptibility of a disease and their evaluation of preventive measures, which can directly influence patients’ health behaviors.25 The higher the patient’s level of health beliefs, the higher level of confidence in completing rehabilitation exercises, and the better compliance with functional exercises.26 The results of this study showed that the higher the patients’ self-confidence in postoperative rehabilitation exercises and the higher motivation to participate in rehabilitation exercises were important factors in promoting rehabilitation exercise in elderly postoperative ARCR patients. When patients perceive the difficulty of rehabilitation exercise, they lose confidence in adhering to rehabilitation exercise, and are prone to negative psychological states such as anxiety, depression, etc, and are unable to satisfy their expectations of rehabilitation, thus avoiding rehabilitation exercise. Healthcare professionals should pay attention to the psychological status of patients promptly, strengthen communication between doctors and patients, and use positive language to stimulate positive emotions, focus on health education during hospitalization, and improving patients’ health beliefs. On the other hand, helping patients to establish reasonable expectations for recovery is conducive to increasing self-efficacy and promoting comprehensive recovery of patients.27 Considering the patients’ situation, we will discuss with them a rehabilitation exercise plan, assist them in decomposing the rehabilitation plan into phases, and implement the rehabilitation tasks, to make the patients have a successful experience in the process of rehabilitation exercise and satisfy their reasonable expectations of rehabilitation, thus ensuring the patients’ positive state of rehabilitation exercise.
Limitations
There were two important limitations in this study. First, the research was conducted in only one hospital in China, and therefore, the results of our analysis may not be comprehensive. We have adopted the principle of maximally differentiated sampling.
Second, the findings of this study were based only on interview data from the patients potentially introducing bias. In the future, input from their family members would enhance the findings by providing additional perspectives about the rehabilitation exercise.
Conclusions
This study used the theory of behavior change wheel to analyze the factors influencing rehabilitation exercise behavior in elderly rotator cuff repair patients. Our study developed three themes: rehabilitation exercise capability-related factors, the influence of external environmental-opportunity related factors and motivation-related factors for adherence to rehabilitation exercise behavior.
The identified factors will contribute to our understanding of rehabilitation exercise behavior in elderly rotator cuff repair patients and provide a reliable basis for improving the quality of the rehabilitation exercises. We provide the following ideas for the rehabilitation exercise program suitable for elderly rotator cuff repair patients. Healthcare professionals should pay particular attention to the postoperative pain and take corresponding measures. Appropriate family and social support can stimulate the patient’s motivation to exercise. The patient’s programme for each stage of rehabilitation has clear objectives, which will help ensure the continuity of postoperative rehabilitation exercises. Future research should be to consider how to apply the identified factors to develop a comprehensive rehabilitation exercise program and expand the scope to include family members and caregivers to triangulate findings.
Relevance for Clinical Practice
Based on the findings of this study, clinical nurses can focus on factors that influence rehabilitation exercise behavior in elderly rotator cuff repair patients, and collaborate with the doctors and rehabilitators to develop a rehabilitation exercise program that is suitable for elderly rotator cuff repair patients.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article. The data is available from the corresponding author upon reasonable request.
Funding
This study was supported by the Tianjin Science and Technology Program [grant number MOST 22JCQNJC00850].
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. He L, Li Y, Liao X, et al. Effects of evidence-based nursing combined with enhanced recovery after surgery on shoulder joint function and neurological function after arthroscopic rotator cuff injury repair[J]. Medicine. 2021;100(47):27951–27953. doi:10.1097/MD.0000000000027951
2. Barnes LAF, Kim HM, Caldwell JM, et al. Satisfaction, function and repair integrity after arthroscopic versus mini‐open rotator cuff repair. Bone Joint J. 2017;99(2):245–249.
3. Greenall G, Carr A, Beard D, et al. Systematic review of the surgical management of rotator cuff repair with an augmentative patch:a feasibility study protocol. Syst Rev. 2018;7(1):187.
4. Doiron-Cadrin P, Lafrance S, Saulnier M. Shoulder rotator cuff disorders: a systematic review of clinical practice guidelines and semantic analyses of recommendations. Arch Phys Med Rehab. 2020;101(7):1233–1242.
5. National bureau of statistics. wang pingping: total population declines slightly, urbanization level continues to increase. [EB/OL]. 2023.
6. Ren YM, Duan YH, Sun YB, et al. Is arthroscopic repair superior to biceps tenotomy and tenodesis for type II SLAP lesions? A meta‐analysis of RCTS and observational studies. J Orthopaedic Surg Res. 2019;14;1:48.
7. Chang K, Hung CY, Han DS, et al. Early versus delayed passive range of motion exercise for arthroscopic rotator cuff repair:A meta-analysis of randomized controlled trials. Am J Sports Med. 2015;43(5):1265–1273.
8. Fabio VS, Daniel M, Kilian L. Current trends in rehabilitation of rotator cuff injuri-es. SICOT-J. 2023;9(14).
9. Longo UG, Risi AL, Berton A, et al. Conservative versus accelerated rehabilitation after rotator cuff repair: a systematic review and meta analysis. BMC Musculoskel-et Disord. 2021;22(1):637.
10. Mazuquin B, Moffatt M, Gill P, et al. Effectiveness of early versus delayed rehabilitation following rotator cuff repair: systematic review and meta-analyses. PLoS One. 2021;16(5):e0252137. doi:10.1371/journal.pone.0252137
11. Michie S, Van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6(1):42. doi:10.1186/1748-5908-6-42
12. Ahmadi A, Noetel M, Parker P, et al. A classification system for teachers’ motivational behaviors recommended in self-determination theory interventions. J Educ Psychol. 2023;115(8):1158–1176. doi:10.1037/edu0000783
13. Nelligan RK, Hinman RS, Atkins L, Bennell KL. A short message service intervention to support adherence to home-based strengthening exercise for people with knee osteoarthritis: intervention design applying the behavior change wheel. JMIR mHealth and uHealth. 2019;7(10):e14619. doi:10.2196/14619
14. Zhang M, Zhang H, Zheng J. Factors influencing shoulder joint function in patients with type 2 diabetes mellitus following arthroscopic rotator cuff repair: a mixed-methods study. Res Nurs Health. 2025;48(2):110–120. doi:10.1002/nur.22429
15. Ahmads S, Haber M, Bokor DJ. The influence of intraoperative factors and postoperative rehabilitation compliance on the integrity of the rotator cuff after arthroscopic repair. J Shoulder Elbow Surg. 2015;24(2):229–235. doi:10.1016/j.jse.2014.06.050
16. Shibahashi H, Murakawa M, Yuki I, et al. Patient sex is a significant factor in arm function recovery after arthroscopic rotator cuff repair. Arthrosco Sports Med Rehab. 2024;6(1):100834. doi:10.1016/j.asmr.2023.100834
17. Fitzpatrick LA, Atinga A, White L, et al. Rotator cuff injury and repa-ir. Semin Musculoskelet Radiol. 2022;26(5):585–596.
18. Ming Z, Yu Z. Motivation and barriers to postoperative rehabilitation exercise in type 2 diabetic patients with rotator cuff injuries: a qualitative study. Patient Prefer Adher. 2024;18:1483–1492.
19. Swansen T, Wright MA, Murthi AM. Postoperative rehabilitation following rotator cuff repair. Phys Med Rehabil Clin N Am. 2023;34(2):357–364.
20. Musa G, Metehan Y, Beril K, et al. Effect of instrument-assisted soft tissue mobilizat-ion in addition to conventional rehabilitation on pain, range of motion, and functional level in patients with arthroscopic rotator cuff repair: a randomized controlled trial. J Shoulder Elbow Surg. 2025;1–10.
21. Hogenbirk RNM, Van Der Plas WY, Hentzen JEKR, et al. Postope-rative muscle loss, protein intake, physical activity and outcome associations. Br J Surg. 2023;110(2):183–192.
22. Sassi M, Carnevale A, Mancuso M, et al. Machine-learning models for shoulder rehabilitation exercises classification using a wearable system. Knee Surg Sports Traumatol Arthrosc. 2024;1(1):0942–2056.
23. Toni S, Sharon L, Gary M, et al. A randomized controlled trial comparing 2 instructi-onal approaches to home exercise instruction following arthroscopic full-thickness ro-tator cuff repair. surgerY. 2022;11(32):548–559.
24. Cole BJ, Cotter EJ, Wang KC, Davey A. Patient understanding, expectations, and satisfaction regarding rotator cuff injuries and surgical management. Arthroscopy. 2017;33(8):1603–1606.
25. Chen Y, Li X, Jing G, et al. Health education interventions for older adults with h-ypertension: a systematic review and Meta-analysis[J]. Public Health Nurs. 2020;37(3):461–469.
26. Venkatachalam J, Abrahm SB, Singh Z, et al. Determinants of patient’s adherence to hypertension medications in a rural population of Kancheepuram District in Tamil Na-Du, South India. Indian J Community Med. 2015;40(1):33–37.
27. Van Zaanen Y, Siertsema T, Kievit AJ, et al. Only low patients’ expectat-ions are prognostic for dissatisfaction with performing work-related knee-straining ac-tivities after total knee arthroplasty. A prospective multicentre cohort study. Arch Phys Med Rehabil. 2023;104(12):2051–2058.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.